Plasma pS129-α-Synuclein Is a Surrogate Biofluid Marker of Motor Severity and Progression in Parkinson’s Disease

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Participants
2.2. Evaluation of Motor and Cognitive Symptoms
2.3. Measurement of Plasma Totalα-Synuclein and pS129-α-Synuclein
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Participants
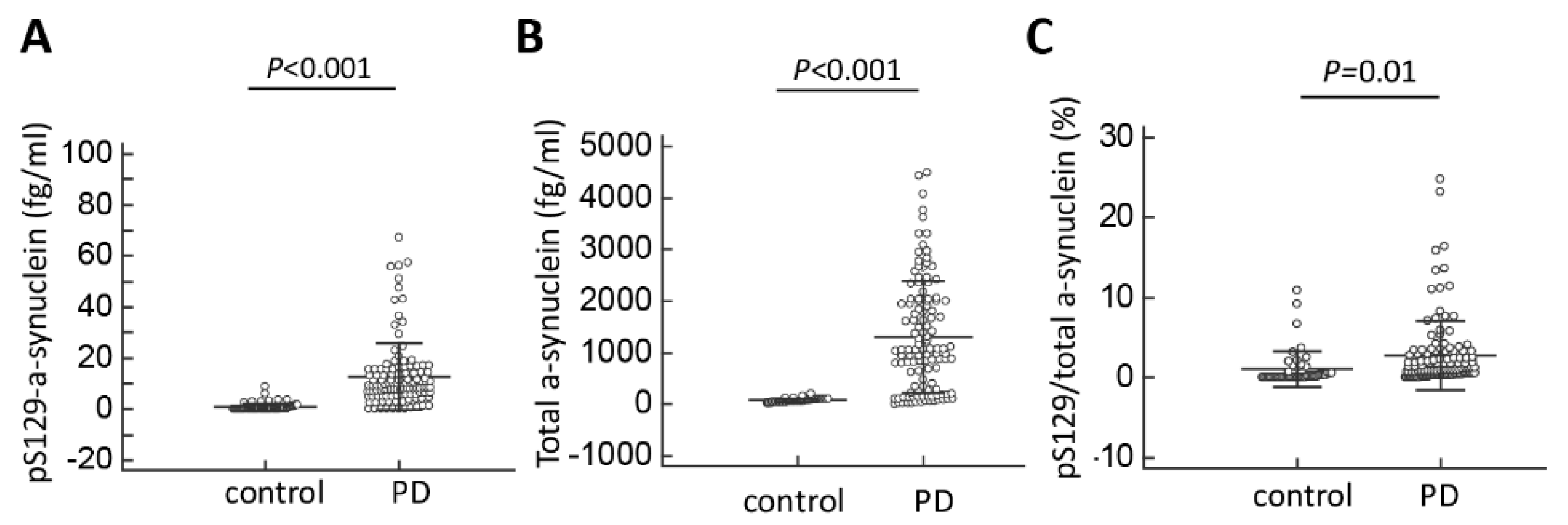
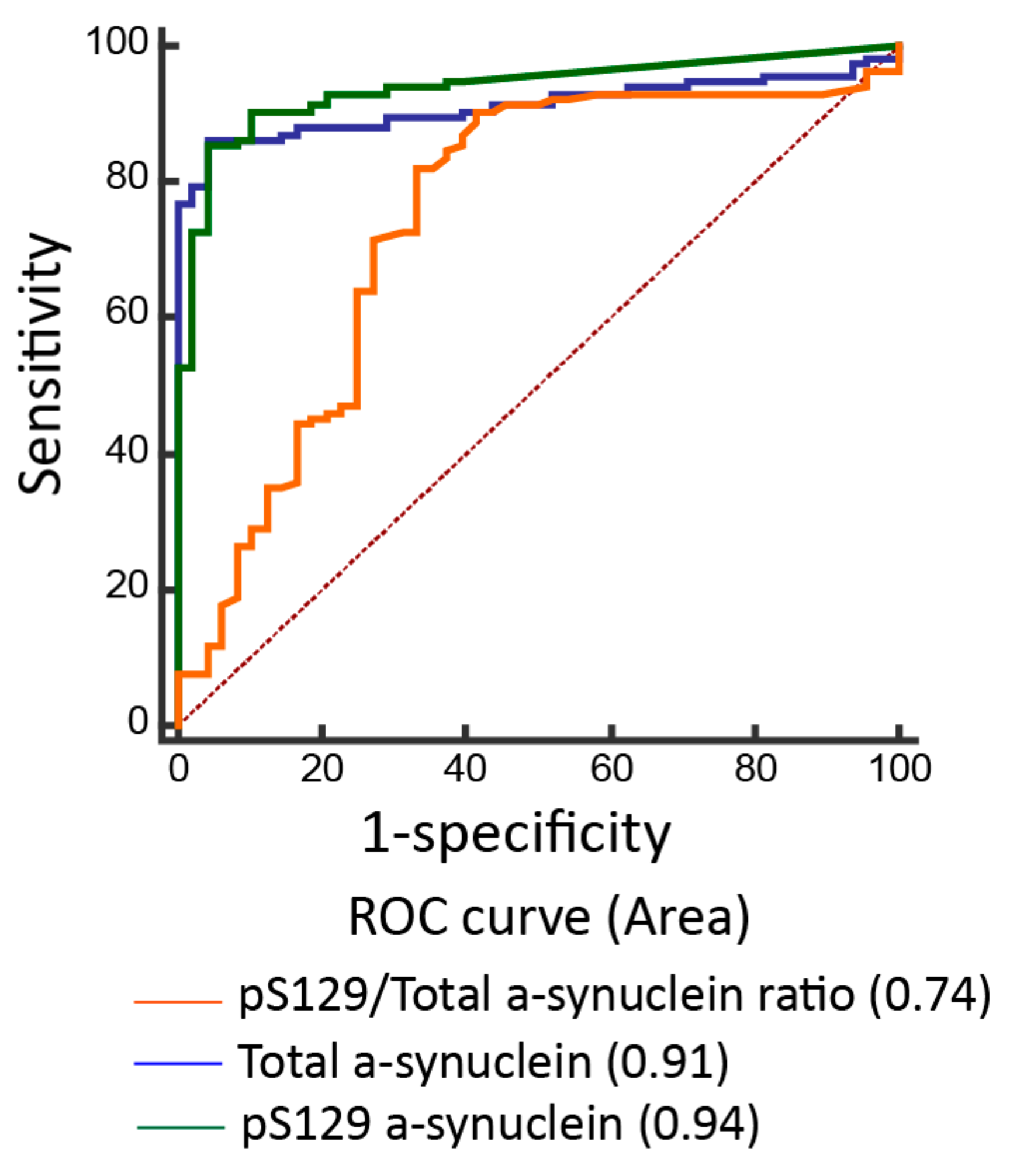
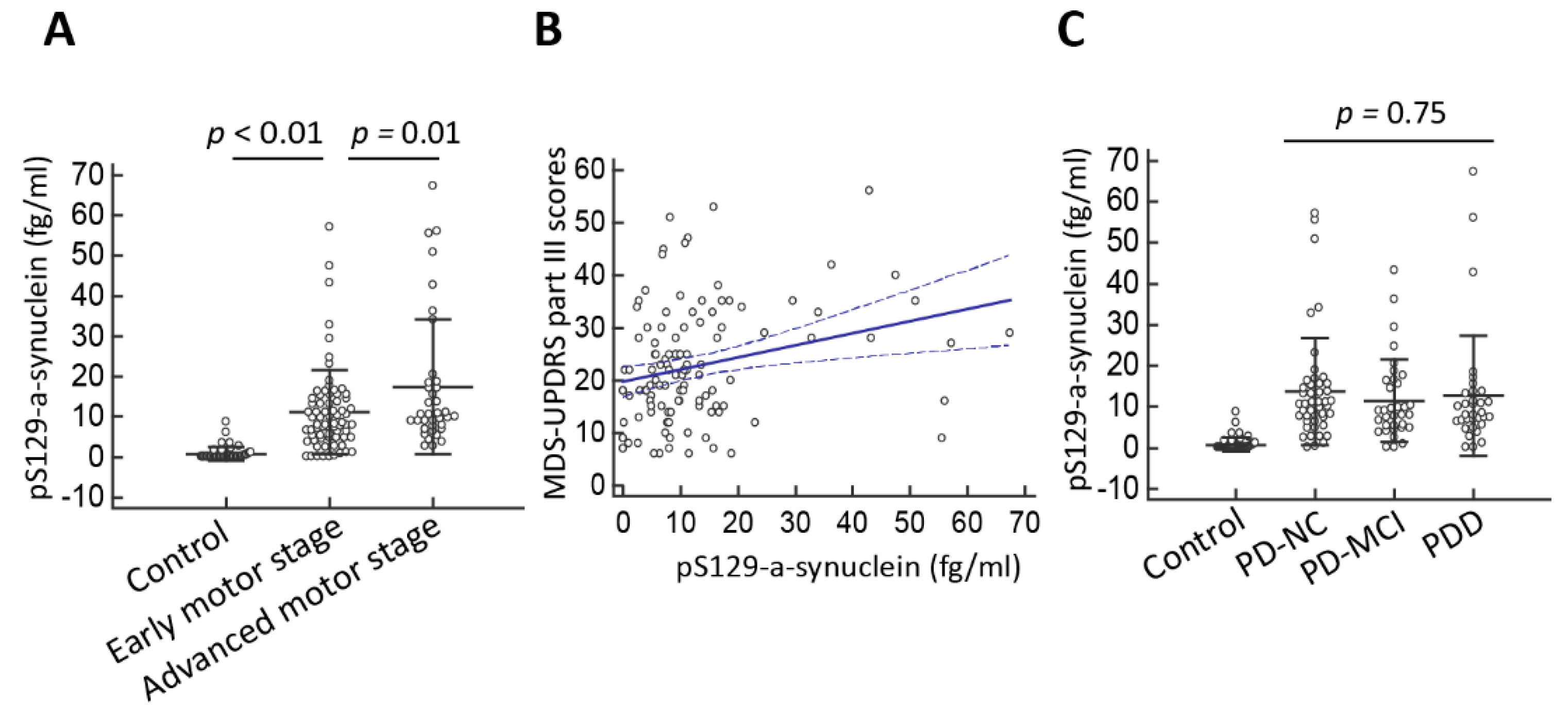
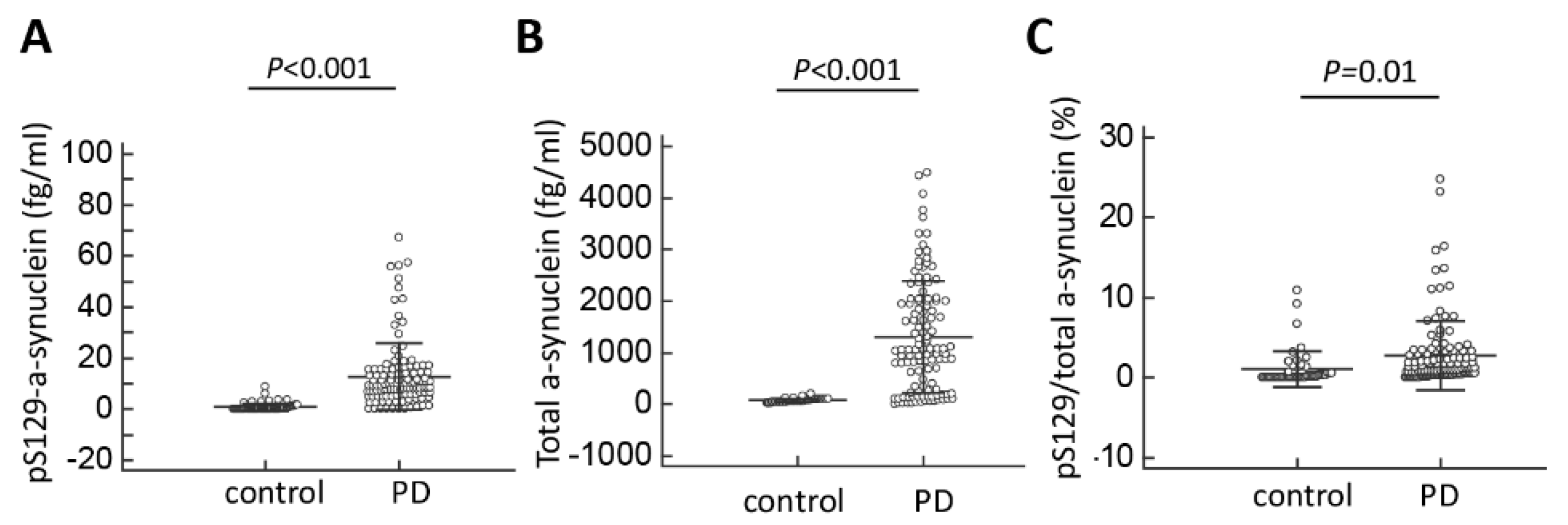
3.2. Cross-Sectional Analyses of pS129-α-Synuclein Levels and Motor and Cognitive Severity
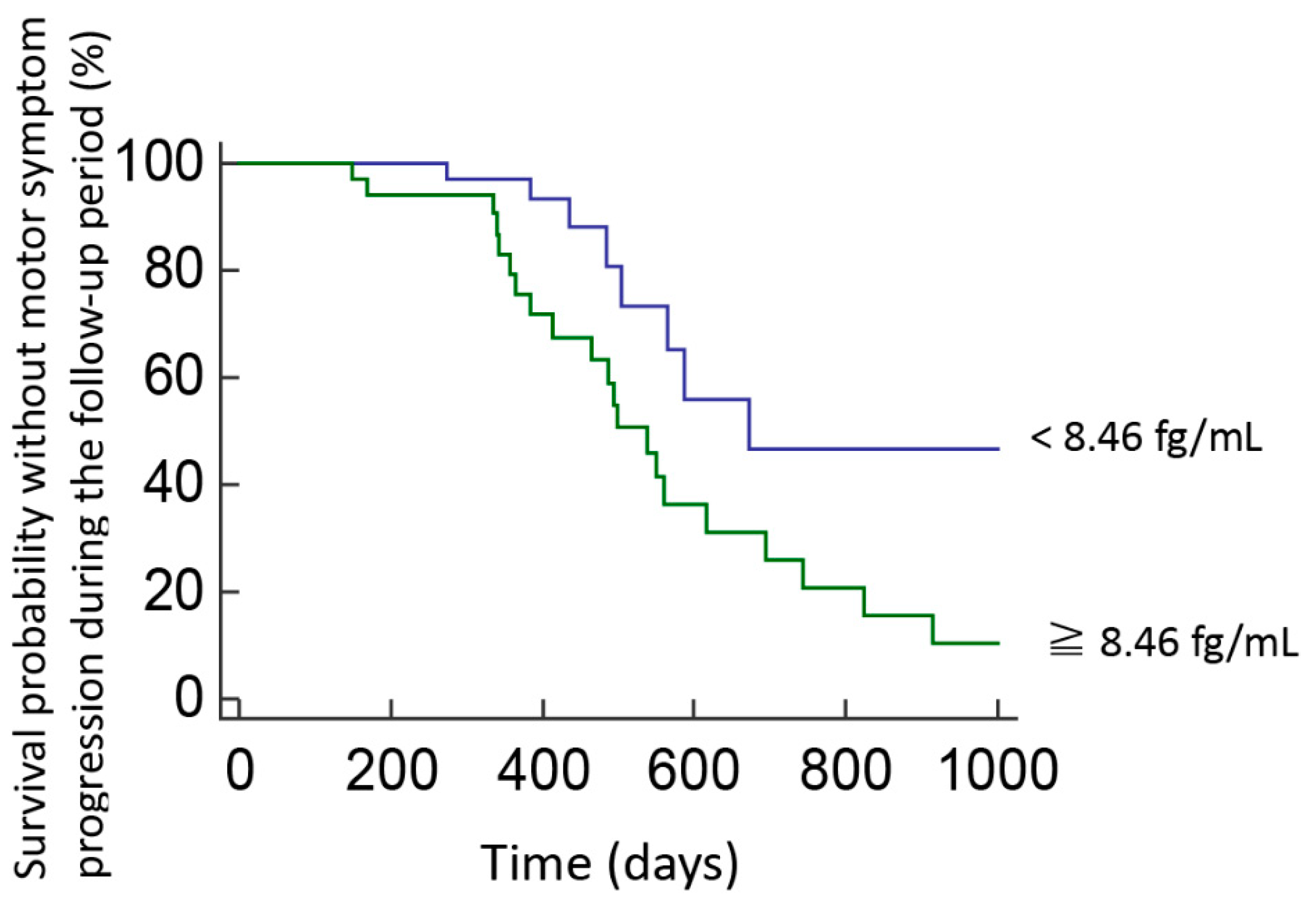
3.3. Longitudinal Follow-Up Analyses of Motor and Cognition Progression
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Luk, K.C.; Kehm, V.; Carroll, J.; Zhang, B.; O’Brien, P.; Trojanowski, J.Q.; Lee, V.M. Pathological alpha-synuclein transmission initiates Parkinson-like neurodegeneration in nontransgenic mice. Science 2012, 338, 949–953. [Google Scholar] [CrossRef] [PubMed]
- Spillantini, M.G.; Schmidt, M.L.; Lee, V.M.; Trojanowski, J.Q.; Jakes, R.; Goedert, M. Alpha-synuclein in Lewy bodies. Nature 1997, 388, 839–840. [Google Scholar] [CrossRef] [PubMed]
- Macleod, A.D.; Taylor, K.S.; Counsell, C.E. Mortality in Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2014, 29, 1615–1622. [Google Scholar] [CrossRef] [PubMed]
- Mandler, M.; Valera, E.; Rockenstein, E.; Weninger, H.; Patrick, C.; Adame, A.; Santic, R.; Meindl, S.; Vigl, B.; Smrzka, O.; et al. Next-generation active immunization approach for synucleinopathies: Implications for Parkinson’s disease clinical trials. Acta Neuropathol. 2014, 127, 861–879. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, H.; Hasegawa, M.; Dohmae, N.; Kawashima, A.; Masliah, E.; Goldberg, M.S.; Shen, J.; Takio, K.; Iwatsubo, T. alpha-Synuclein is phosphorylated in synucleinopathy lesions. Nat. Cell Biol. 2002, 4, 160–164. [Google Scholar] [CrossRef]
- Anderson, J.P.; Walker, D.E.; Goldstein, J.M.; de Laat, R.; Banducci, K.; Caccavello, R.J.; Barbour, R.; Huang, J.; Kling, K.; Lee, M.; et al. Phosphorylation of Ser-129 is the dominant pathological modification of alpha-synuclein in familial and sporadic Lewy body disease. J. Biol. Chem. 2006, 281, 29739–29752. [Google Scholar] [CrossRef] [PubMed]
- Parnetti, L.; Gaetani, L.; Eusebi, P.; Paciotti, S.; Hansson, O.; El-Agnaf, O.; Mollenhauer, B.; Blennow, K.; Calabresi, P. CSF and blood biomarkers for Parkinson’s disease. Lancet Neurol. 2019, 18, 573–586. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, M.; Chung, K.A.; Zabetian, C.P.; Leverenz, J.B.; Berg, D.; Srulijes, K.; Trojanowski, J.Q.; Lee, V.M.; Siderowf, A.D.; et al. Phosphorylated alpha-synuclein in Parkinson’s disease. Sci. Transl. Med. 2012, 4, 121ra20. [Google Scholar] [CrossRef] [PubMed]
- Besong-Agbo, D.; Wolf, E.; Jessen, F.; Oechsner, M.; Hametner, E.; Poewe, W.; Reindl, M.; Oertel, W.H.; Noelker, C.; Bacher, M.; et al. Naturally occurring alpha-synuclein autoantibody levels are lower in patients with Parkinson disease. Neurology 2013, 80, 169–175. [Google Scholar] [CrossRef]
- Lin, C.H.; Yang, S.Y.; Horng, H.E.; Yang, C.C.; Chieh, J.J.; Chen, H.H.; Liu, B.H.; Chiu, M.J. Plasma alpha-synuclein predicts cognitive decline in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2017, 88, 818–824. [Google Scholar] [CrossRef]
- Ding, J.; Zhang, J.; Wang, X.; Zhang, L.; Jiang, S.; Yuan, Y.; Li, J.; Zhu, L.; Zhang, K. Relationship between the plasma levels of neurodegenerative proteins and motor subtypes of Parkinson’s disease. J. Neural Transm. (Vienna) 2017, 124, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Emre, M.; Aarsland, D.; Brown, R.; Burn, D.J.; Duyckaerts, C.; Mizuno, Y.; Broe, G.A.; Cummings, J.; Dickson, D.W.; Gauthier, S.; et al. Clinical diagnostic criteria for dementia associated with Parkinson’s disease. Mov. Disord. 2007, 22, 1689–1707; quiz 1837. [Google Scholar] [CrossRef]
- Berg, L. Clinical Dementia Rating (CDR). Psychopharmacol. Bull. 1988, 24, 637–639. [Google Scholar] [PubMed]
- Litvan, I.; Goldman, J.G.; Troster, A.I.; Schmand, B.A.; Weintraub, D.; Petersen, R.C.; Mollenhauer, B.; Adler, C.H.; Marder, K.; Williams-Gray, C.H.; et al. Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: Movement Disorder Society Task Force guidelines. Mov. Disord. 2012, 27, 349–356. [Google Scholar] [CrossRef]
- Hoops, S.; Nazem, S.; Siderowf, A.D.; Duda, J.E.; Xie, S.X.; Stern, M.B.; Weintraub, D. Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology 2009, 73, 1738–1745. [Google Scholar] [CrossRef]
- Lin, C.H.; Yang, S.Y.; Horng, H.E.; Yang, C.C.; Chieh, J.J.; Chen, H.H.; Liu, B.H.; Chiu, M.J. Plasma Biomarkers Differentiate Parkinson’s Disease from Atypical Parkinsonism Syndromes. Front. Aging Neurosci. 2018, 10, 123. [Google Scholar] [CrossRef]
- Yang, C.C.; Yang, S.Y.; Chieh, J.J.; Horng, H.E.; Hong, C.Y.; Yang, H.C.; Chen, K.H.; Shih, B.Y.; Chen, T.F.; Chiu, M.J. Biofunctionalized magnetic nanoparticles for specifically detecting biomarkers of Alzheimer’s disease in vitro. ACS Chem. Neurosci. 2011, 2, 500–505. [Google Scholar] [CrossRef]
- Yang, S.Y.; Chiu, M.J.; Lin, C.H.; Horng, H.E.; Yang, C.C.; Chieh, J.J.; Chen, H.H.; Liu, B.H. Development of an ultra-high sensitive immunoassay with plasma biomarker for differentiating Parkinson disease dementia from Parkinson disease using antibody functionalized magnetic nanoparticles. J. Nanobiotechnol. 2016, 14, 41. [Google Scholar] [CrossRef] [PubMed]
- Polymeropoulos, M.H.; Lavedan, C.; Leroy, E.; Ide, S.E.; Dehejia, A.; Dutra, A.; Pike, B.; Root, H.; Rubenstein, J.; Boyer, R.; et al. Mutation in the alpha-synuclein gene identified in families with Parkinson’s disease. Science 1997, 276, 2045–2047. [Google Scholar] [CrossRef] [PubMed]
- Simon-Sanchez, J.; Schulte, C.; Bras, J.M.; Sharma, M.; Gibbs, J.R.; Berg, D.; Paisan-Ruiz, C.; Lichtner, P.; Scholz, S.W.; Hernandez, D.G.; et al. Genome-wide association study reveals genetic risk underlying Parkinson’s disease. Nat. Genet. 2009, 41, 1308–1312. [Google Scholar] [CrossRef] [PubMed]
- Barbour, R.; Kling, K.; Anderson, J.P.; Banducci, K.; Cole, T.; Diep, L.; Fox, M.; Goldstein, J.M.; Soriano, F.; Seubert, P.; et al. Red blood cells are the major source of alpha-synuclein in blood. Neurodegener. Dis. 2008, 5, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Foulds, P.G.; Diggle, P.; Mitchell, J.D.; Parker, A.; Hasegawa, M.; Masuda-Suzukake, M.; Mann, D.M.; Allsop, D. A longitudinal study on alpha-synuclein in blood plasma as a biomarker for Parkinson’s disease. Sci. Rep. 2013, 3, 2540. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, N. CSF biomarkers in neurodegenerative diseases. Clin. Chem. Lab. Med. 2011, 49, 345–352. [Google Scholar] [CrossRef]
- Zhou, J.; Broe, M.; Huang, Y.; Anderson, J.P.; Gai, W.P.; Milward, E.A.; Porritt, M.; Howells, D.; Hughes, A.J.; Wang, X.; et al. Changes in the solubility and phosphorylation of alpha-synuclein over the course of Parkinson’s disease. Acta Neuropathol. 2011, 121, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Del Tredici, K.; Rub, U.; de Vos, R.A.; Jansen Steur, E.N.; Braak, E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Ross, G.W.; Petrovitch, H.; Abbott, R.D.; Nelson, J.; Markesbery, W.; Davis, D.; Hardman, J.; Launer, L.; Masaki, K.; Tanner, C.M.; et al. Parkinsonian signs and substantia nigra neuron density in decendents elders without PD. Ann. Neurol. 2004, 56, 532–539. [Google Scholar] [CrossRef]
- Marsden, C.D. Parkinson’s disease. Lancet 1990, 335, 948–952. [Google Scholar] [CrossRef]
- Dijkstra, A.A.; Voorn, P.; Berendse, H.W.; Groenewegen, H.J.; Netherlands Brain, B.; Rozemuller, A.J.; van de Berg, W.D. Stage-dependent nigral neuronal loss in incidental Lewy body and Parkinson’s disease. Mov. Disord. 2014, 29, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Shulman, J.M.; Nag, S.; Leurgans, S.E.; Arnold, S.E.; Morris, M.C.; Schneider, J.A.; Bennett, D.A. Nigral pathology and parkinsonian signs in elders without Parkinson disease. Ann. Neurol. 2012, 71, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B. Fundamentals of Biostatistics, 7th ed.; Brooks/Cole: Boston, MA, USA, 2011. [Google Scholar]
- Irwin, D.J.; Lee, V.M.; Trojanowski, J.Q. Parkinson’s disease dementia: Convergence of alpha-synuclein, tau and amyloid-beta pathologies. Nat. Rev. Neurosci. 2013, 14, 626–636. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Controls (n = 68) | PD (n = 122) | p Value |
|---|---|---|---|
| Age, years | 68.3 ± 9.3 | 69.3 ± 10.1 | 0.32 |
| Sex, male | 44.1% | 46.7% | 0.72 |
| Education, years | 12.9 ± 4.2 | 11.7 ± 3.8 | 0.72 |
| Disease duration, years | N.A. | 6.9 ± 3.7 | N.A. |
| MMSE | 29.3 ± 1.2 | 26.4 ± 2.3 | <0.01 |
| Hoehn–Yahr stages, on | N.A. | 2.2 ± 0.9 | N.A. |
| Hoehn–Yahr stages, off | N.A. | 3.2 ± 1.8 | N.A. |
| MDS-UPDRS part III scores, on | N.A. | 16.8 ± 8.3 | N.A. |
| MDS-UPDRS part III scores, off | N.A. | 32.2 ± 10.8 | N.A. |
| Normal Controls (n = 68) | PD Patients (n = 122) | p Value | |
|---|---|---|---|
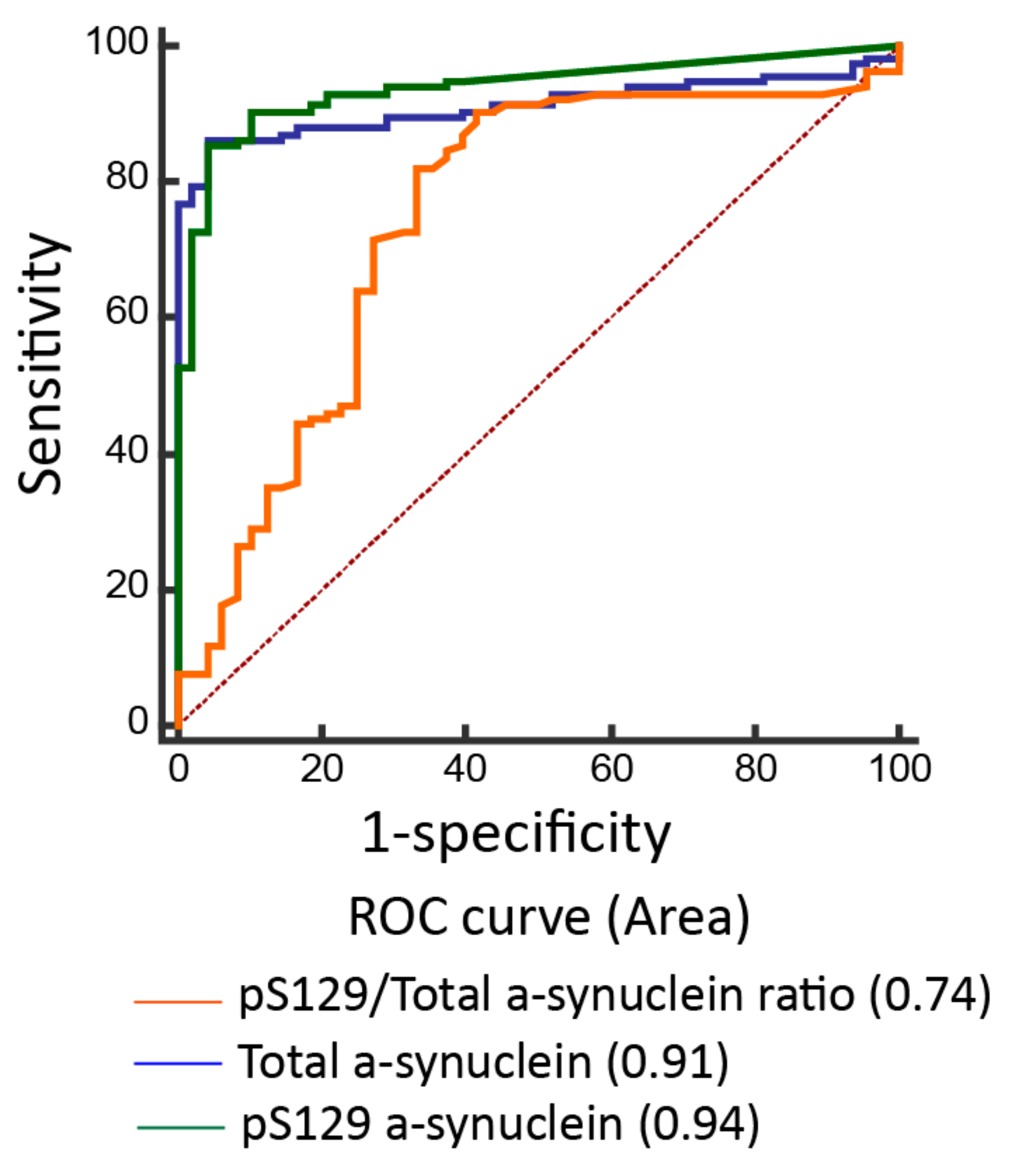
| Total α-synuclein, fg/mL (minimal–maximal values) | 76.4 ± 33.5 (21.0–211.5) | 1302.3 ± 886.6 (5.7–4477.9) | p < 0.01 ** |
| pS129-α-synuclein, fg/mL (minimal–maximal values) | 0.8 ± 0.7 (0.03–8.7) | 12.9 ± 8.7 (0.1–67.4) | p < 0.01 ** |
| pS129-α-synuclein/total α-synuclein ratio | 1.1 ± 0.6% (0.01–10.8) | 2.8 ± 1.1% (0.01–24.8) | p = 0.01 * |
| PD (n = 122) | p Value | PD (n = 122) | p Value | ||||
|---|---|---|---|---|---|---|---|
| Early Motor Stage (n = 76) | Advanced Motor Stage (n = 46) | PD-NC (n = 51) | PD-MCI (n = 35) | PDD (n = 36) | |||
| Age (years) | 67.4 ± 10.2 | 73.1 ± 8.7 | p = 0.02 | 64.3 ± 10.9 | 70.3 ± 6.4 | 79.9 ± 8.3 | p < 0.01 ** |
| Gender (M, %) | 46.1% | 50.0% | p = 0.12 | 47.1% | 48.5% | 50.3% | p = 0.21 |
| Disease duration (years) | 4.9 ± 3.5 | 8.0 ± 4.6 | p = 0.02 | 4.9 ± 2.6 | 6.1 ± 4.2 | 6.7 ± 3.3 | p = 0.04 * |
| MMSE | 26.8 ± 3.1 | 22.7 ± 3.6 | p = 0.03 | 28.8 ± 0.8 | 26.3 ± 0.9 | 18.8 ± 4.5 | p < 0.01 ** |
| Hoehn–Yahr stage (on) | 1.5 ± 0.5 | 3.0 ± 0.9 | P < 0.01 ** | 1.5 ± 0.9 | 2.1 ± 0.7 | 2.7 ± 1.3 | p = 0.06 |
| Hoehn–Yahr stage (off) | 1.9 ± 0.9 | 3.3 ± 1.2 | p = 0.02 | 1.8 ± 1.3 | 2.5 ± 0.9 | 3.2 ± 1.2 | p = 0.07 |
| UPDRS part III (on) | 19.1 ± 8.5 | 30.5 ± 12.1 | p < 0.01 * | 18.8 ± 8.5 | 23.6 ± 9.7 | 27.6 ± 10.2 | p = 0.04 * |
| UPDRS part III (off) | 28.8 ± 10.8 | 42.6 ± 13.4 | p < 0.01 * | 30.0 ± 7.4 | 32.5 ± 6.2 | 37.1 ± 14.3 | p = 0.09 |
| Total α–synuclein, fg/mL (minimal–maximal values) | 1322.8 ± 1136.6 (19.5–4427.8) | 1423.2 ± 1023.8 (32.7–4477.9) | p = 0.57 | 1181.7 ± 1115.6 (34.8–4477.9) | 1417.7 ± 1174.6 (32.7–4427.8) | 1371.6 ± 929.4 (5.6–3762.4) | p = 0.68 |
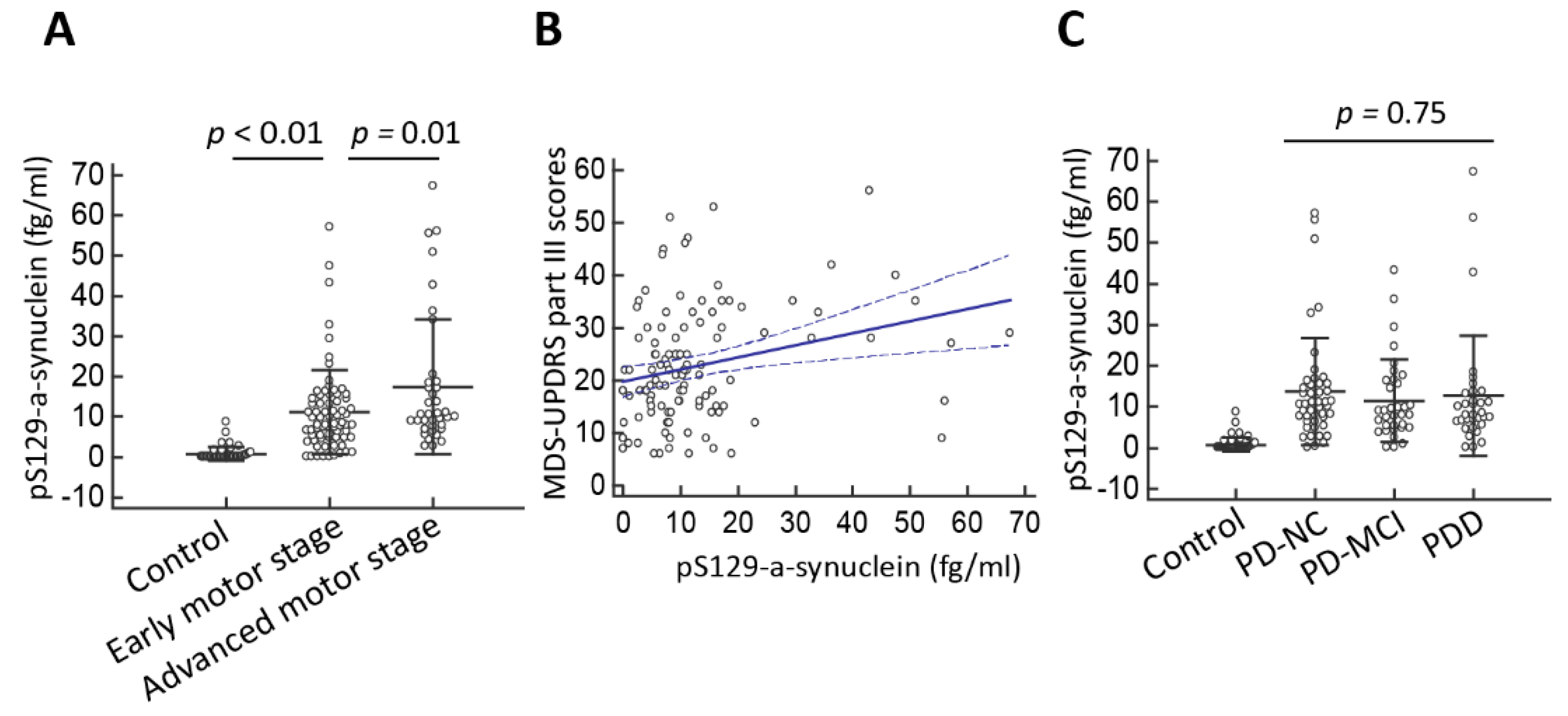
| pS129–α–synuclein, fg/mL (minimal–maximal values) | 11.1 ± 8.9 (0.1–56.2) | 17.6 ± 10.2 (2.8–67.4) | p = 0.01 * | 13.7 ± 6.8 (0.2–56.2) | 11.5 ± 7.5 (0.1–43.3) | 12.8 ± 7.1 (0.1–67.4) | p = 0.75 |
| pS129–α–synuclein/total α–synuclein ratio | 2.3 ± 1.5% (0.01–16.2) | 3.6 ± 1.9% (0.02–21.2) | p = 0.05 | 2.9 ± 1.6% (0.01–21.2) | 2.2 ± 1.4% (0.01–16.2) | 2.7 ± 1.8% (0.02–17.4) | p = 0.90 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-H.; Liu, H.-C.; Yang, S.-Y.; Yang, K.-C.; Wu, C.-C.; Chiu, M.-J. Plasma pS129-α-Synuclein Is a Surrogate Biofluid Marker of Motor Severity and Progression in Parkinson’s Disease. J. Clin. Med. 2019, 8, 1601. https://doi.org/10.3390/jcm8101601
Lin C-H, Liu H-C, Yang S-Y, Yang K-C, Wu C-C, Chiu M-J. Plasma pS129-α-Synuclein Is a Surrogate Biofluid Marker of Motor Severity and Progression in Parkinson’s Disease. Journal of Clinical Medicine. 2019; 8(10):1601. https://doi.org/10.3390/jcm8101601
Chicago/Turabian StyleLin, Chin-Hsien, Huei-Chun Liu, Shieh-Yueh Yang, Kai-Chien Yang, Chau-Chung Wu, and Ming-Jang Chiu. 2019. "Plasma pS129-α-Synuclein Is a Surrogate Biofluid Marker of Motor Severity and Progression in Parkinson’s Disease" Journal of Clinical Medicine 8, no. 10: 1601. https://doi.org/10.3390/jcm8101601
APA StyleLin, C.-H., Liu, H.-C., Yang, S.-Y., Yang, K.-C., Wu, C.-C., & Chiu, M.-J. (2019). Plasma pS129-α-Synuclein Is a Surrogate Biofluid Marker of Motor Severity and Progression in Parkinson’s Disease. Journal of Clinical Medicine, 8(10), 1601. https://doi.org/10.3390/jcm8101601