


Intraventricular Thrombosis After Myocardial Infarction: Prognostic Evaluation in Relation to Microvascular Obstruction Extent by CMR
 , , ,
, , ,  , and
, and
Abstract

1. Introduction
2. Materials and Methods
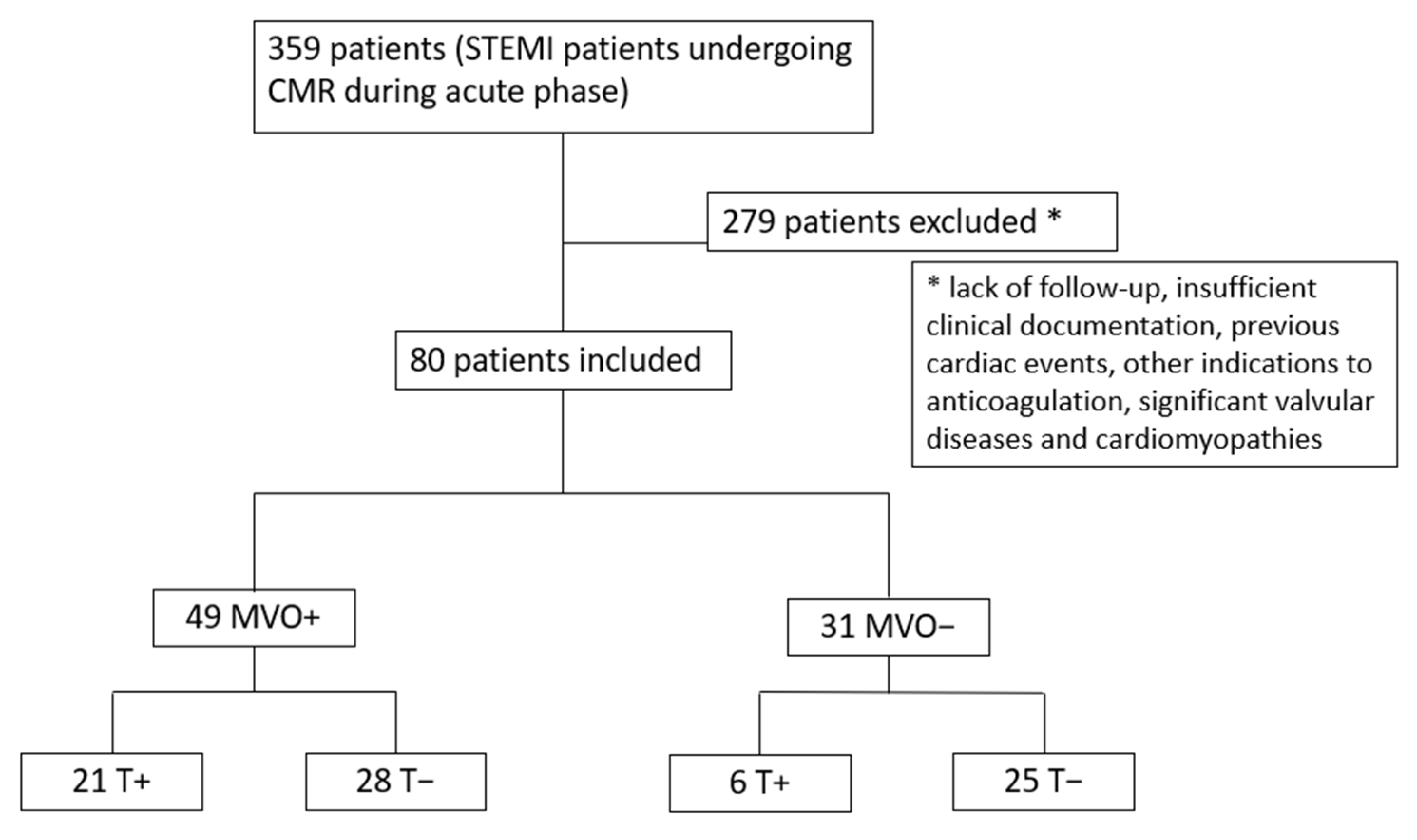
2.1. Patients and Study Design
2.2. CMR Acquisition Protocol and Analysis
2.3. Statistical Analysis
3. Results
3.1. Population During Hospitalization
3.2. Predictors of Major Cardiovascular Events
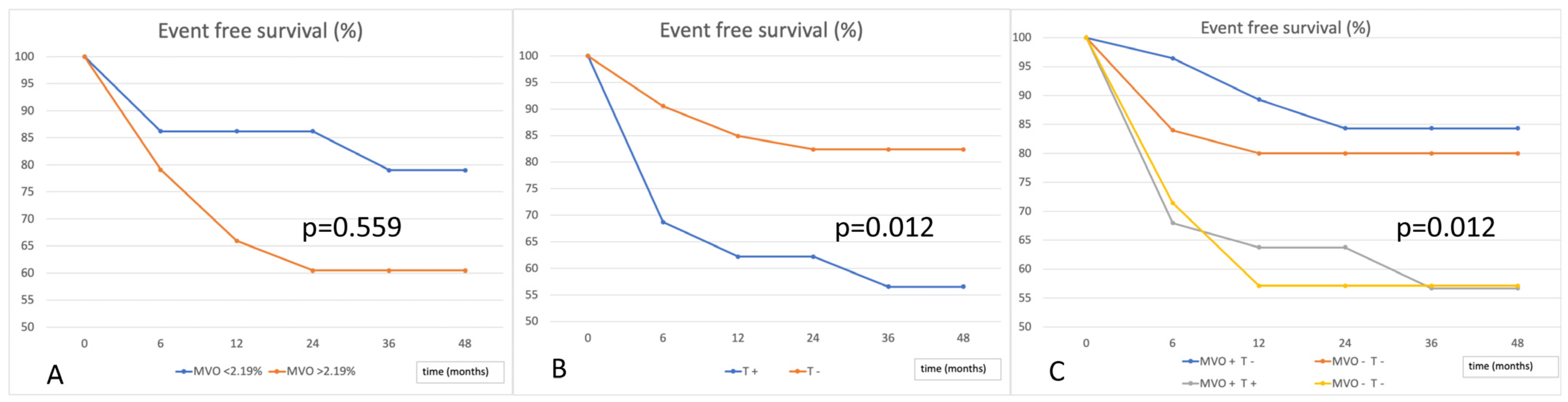
3.3. Event-Free Survival According to MVO and LV Thrombosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phan, J.; Nguyen, T.; French, J.; Moses, D.; Schlaphoff, G.; Lo, S.; Juergens, C.; Richards, D.; Thomas, L. Incidence and predictors of left ventricular thrombus formation following acute ST-segment elevation myocardial infarction: A serial cardiac MRI study. Int. J. Cardiol. Heart Vasc. 2019, 24, 100395. [Google Scholar] [CrossRef] [PubMed]
- Pöss, J.; Desch, S.; Eitel, C.; de Waha, S.; Thiele, H.; Eitel, I. Left Ventricular Thrombus Formation After ST-Segment–Elevation Myocardial Infarction Insights From a Cardiac Magnetic Resonance Multicenter Study. Circ. Cardiovasc. Imaging 2015, 8, e003417. [Google Scholar] [CrossRef] [PubMed]
- Weir, R.A.; Murphy, C.A.; Petrie, C.J.; Martin, T.N.; Balmain, S.; Clements, S.; Steedman, T.; Wagner, G.S.; Dargie, H.J.; McMurray, J.J.V. Microvascular obstruction remains a portent of adverse remodeling in optimally treated patients with left ventricular systolic dysfunction after acute myocardial infarction. Circ. Cardiovasc. Imaging 2010, 3, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Niccoli, G.; Scalone, G.; Lerman, A.; Crea, F. Coronary microvascular obstruction in acute myocardial infarction. Eur. Heart J. 2016, 37, 1024–1033. [Google Scholar] [CrossRef]
- Niccoli, G.; Burzotta, F.; Galiuto, L.; Crea, F. Myocardial no-reflow in humans. J. Am. Coll. Cardiol. 2009, 54, 281–292. [Google Scholar] [CrossRef]
- Konijnenberg, L.S.A.; Damman, P.; Duncker, D.J.; Kloner, R.A.; Nijveldt, R.; van Geuns, R.M.; Berry, C.; Riksen, N.P.; Escaned, J.; van Royen, N. Pathophysiology and diagnosis of coronary microvascular dysfunction in ST-elevation myocardial infarction. Cardiovasc. Res. 2020, 116, 787–805. [Google Scholar] [CrossRef]
- Fishbein, M.C.; Y-Rit, J.; Lando, U.; Kanmatsuse, K.; Mercier, J.C.; Gantz, W. The relationship of vascular injury and myocardial hemorrhage to necrosis after reperfusion. Circulation 1980, 62, 1274–1279. [Google Scholar] [CrossRef]
- Lombardo, A.; Niccoli, G.; Natale, L.; Bernardini, A.; Cosentino, N.; Bonomo, L.; Crea, F. Impact of microvascular obstruction and infarct size on left ventricular remodeling in reperfused myocardial infarction: A contrast-enhanced cardiac magnetic resonance imaging study. Int. J. Cardiovasc. Imaging 2012, 28, 835–842. [Google Scholar] [PubMed]
- De Waha, S.; Desch, S.; Eitel, I.; Fuernau, G.; Zachrau, J.; Leuschner, A.; Gutberlet, M.; Schuler, G.; Thiele, H. Impact of early vs. late microvascular obstruction assessed by magnetic resonance on long-term outcome after ST-elevation myocardial infarction: A comparison with traditional prognostic markers. Eur. Heart J. 2010, 31, 2660–2668. [Google Scholar] [PubMed]
- Bodi, B.; Gavara, J.; Lopez-Lereu, M.P.; Monmeneu, J.V.; de Dios, E.; Perez-Sole, N.; Bonanad, C.; Marcos-Garces, V.; Canoves, J.; Minana, J.; et al. Impact of Persistent Microvascular Obstruction Late After STEMI on Adverse LV Remodeling: A CMR Study. JACC Cardiovasc. Imaging 2023, 16, 919–930. [Google Scholar]
- Ito, H.; Maruyama, A.; Iwakura, K.; Takiuchi, S.; Masuyama, T.; Hori, M.; Higashino, Y.; Fujii, K.; Minamino, T. Clinical implications of the ‘no reflow’ phenomenon. A predictor of complications and left ventricular remodeling in reperfused anterior wall myocardial infarction. Circulation 1996, 93, 223–228. [Google Scholar] [PubMed]
- Baks, T.; van Geuns, R.J.; Biagini, E.; Wielopolski, P.; Mollet, N.R.; Cademartiri, F.; van der Giessen, W.J.; Krestin, G.P.; Serruys, P.W.; Duncker, D.J.; et al. Effects of primary angioplasty for acute myocardial infarction on early and late infarct size and left ventricular wall characteristics. J. Am. Coll. Cardiol. 2006, 47, 40–44. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [PubMed]
- Cruz Rodriguez, J.B.; Okajima, K.; Greenberg, B.K. Management of left ventricular thrombus: A narrative review. Ann. Transl. Med. 2021, 9, 520. [Google Scholar]
- Sørensen, R.; Hansen, M.L.; Abildstrom, S.Z.; Hvelplund, A.; Andersson, C.; Jørgensen, C.; Madsen, J.K.; Hansen, P.R.; Køber, L.; Torp-Pedersen, C.; et al. Risk of bleeding in patients with acute myocardial infarction treated with different combinations of aspirin, clopidogrel, and vitamin K antagonists in Denmark: A retrospective analysis of nationwide registry data. Lancet 2009, 374, 1967–1974. [Google Scholar] [CrossRef] [PubMed]
- Bulluck, H.; Chan, M.H.H.; Paradies, V.; Yellon, R.L.; Ho, H.H.; Chan, M.Y.; Chin, C.W.L.; Tan, J.W.; Hausenloy, D.J. Incidence and predictors of left ventricular thrombus by cardiovascular magnetic resonance in acute ST-segment elevation myocardial infarction treated by primary percutaneous coronary intervention: A meta-analysis. J. Cardiovas. Magn. Reson. 2018, 20, 72. [Google Scholar]
- Qian, G.; Liu, H.; Wang, J.; Wu, C.; Chen, Y. Risk of cardiac rupture after acute myocardial infarction is related to a risk of hemorrhage. J. Zhejiang Univ.-Sci. B (Biomed. Biotechnol.) 2013, 14, 736–742. [Google Scholar]
- Rickham, P.P. Human Experimentation: Code of Ethics of the World Medical Association. Br. Med. J. 1964, 2, 177. [Google Scholar] [CrossRef]
- Wu, K.C.; Zerhouni, E.A.; Judd, R.M.; Lugo-Olivieri, C.H.; Barouch, L.A.; Schulman, S.P.; Blumenthal, R.S.; Lima, J.A.C. Prognostic Significance of Microvascular Obstruction by Magnetic Resonance Imaging in Patients With Acute Myocardial Infarction. Circulation 1998, 97, 765–772. [Google Scholar]
- Hamirani, Y.S.; Wong, A.; Kramer, C.M.; Salerno, M. Effect of Microvascular Obstruction and Intramyocardial Hemorrhage by CMR on LV Remodeling and Outcomes After Myocardial Infarction. JACC Cardiovasc. Imaging 2014, 7, 940–952. [Google Scholar] [CrossRef]
- Marcos-Garcés, V.; Perez, N.; Gavara, J.; Lopez-Lereu, M.P.; Monmeneu, J.V.; Rios-Navarro, C.; de Dios, E.; Merenciano-González, H.; Gabaldon-Pérez, A.; Cànoves, J.; et al. Risk score for early risk prediction by cardiac magnetic resonance after acute myocardial infarction. Int. J. Cardiol. 2022, 349, 150–154. [Google Scholar] [PubMed]
- Cochet, A.; Lalande, A.; Lorgis, L. Prognostic value of microvascular damage determined by cardiac magnetic resonance in non ST-segment elevation myocardial infarction: Comparison between first-pass and late gadolinium-enhanced images. Investig. Radiol. 2010, 45, 725–732. [Google Scholar] [CrossRef]
- Cochet, A.A.; Lorgis, L.; Lalande, A. Prognostic impact of persistent microvascular obstruction as assessed by contrast-enhanced cardiac magnetic resonance in reperfused acute myocardial infarction. Eur. Radiol. 2009, 19, 2117–2126. [Google Scholar] [CrossRef] [PubMed]
- van Kranenburg, M.; Magro, M.; Thiele, H.; de Waha, S.; Eitel, I.; Cochet, A.; Cottin, Y.; Atar, D.; Buser, P.; Wu, E.; et al. Prognostic Value of Microvascular Obstruction and Infarct Size, as Measured by CMR in STEMI Patients. JACC Cardiovasc. Imaging 2014, 7, 930–939. [Google Scholar] [CrossRef] [PubMed]
- Bodi, V.; Sanchis, J.; Nunez, J. Prognostic value of a comprehensive cardiac magnetic resonance assessment soon after a first ST-segment elevation myocardial infarction. J. Am. Coll. Cardiol. Imaging 2009, 2, 835–842. [Google Scholar] [CrossRef]
- Eitel, I.; Blase, P.; Adams, V. Growth-differentiation factor 15 as predictor of mortality in acute reperfused ST-elevation myocardial infarction: Insights from cardiovascular magnetic resonance. Heart 2011, 97, 632–640. [Google Scholar] [CrossRef]
- Eitel, I.; Wöhrle, J.; Suenkel, H. Intracoronary compared with intravenous bolus abciximab application during primary percutaneous coronary intervention in ST-segment elevation myocardial infarction: Cardiac magnetic resonance substudy of the AIDA STEMI trial. J. Am. Coll. Cardiol. 2013, 61, 1447–1454. [Google Scholar] [CrossRef]
- de Waha, S.; Patel, M.; Granger, C.B.; Ohman, E.M.; Maehara, A.; Eitel, I.; Ben-Yehuda, O.; Jenkins, P.; Thiele, H.; Stone, G.W. Relationship between microvascular obstruction and adverse events following primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: An individual patient data pooled analysis from seven randomized trials. Eur. Heart J. 2017, 38, 3502–3510. [Google Scholar] [CrossRef]
- Eitel, I.; de Waha, S.; Wöhrle, J. Comprehensive prognosis assessment by CMR imaging after ST-segment elevation myocardial infarction. J. Am. Coll. Cardiol. 2014, 64, 1217–1226. [Google Scholar] [CrossRef]
- Symons, R.; Pontone, G.; Schwitter, J.; Francone, M.; Iglesias, J.F.; Barison, A.; Zalewski, J.; De Luca, L.; Degrauwe, S.; Claus, P.; et al. Long-Term Incremental Prognostic Value of Cardiovascular Magnetic Resonance After ST-Segment Elevation Myocardial Infarction: A Study of the Collaborative Registry on CMR in STEMI. JACC Cardiovasc. Imaging 2018, 11, 813–825. [Google Scholar] [CrossRef]
- Galea, N.; Dacquino, G.M.; Ammendola, R.M.; Coco, S.; Agati, L.; De Luca, L.; Carbone, I.; Fedele, F.; Catalano, C.; Francone, M. Microvascular obstruction extent predicts major adverse cardiovascular events in patients with acute myocardial infarction and preserved ejection fraction. Eur. Radiol. 2019, 29, 2369–2377. [Google Scholar]
- Khafagy, R.T.M.; El Mozy, W.; Hamed, E.; ElKhalek, Y.I.A.; Tantawy, W. Prognostic value of microvascular occlusion MRI quantification in assessment of reperfused myocardial infarction. Egypt. J. Radiol. Nucl. Med. 2020, 51, 86. [Google Scholar]
- Bruder, O.; Breuckmann, F.; Jensen, C.; Jochims, M.; Naber, C.K.; Barkhausen, J.; Erbel, R.; Sabin, G.V.; Essen, H. Prognostic impact of contrast-enhanced CMR early after acute ST segment elevation myocardial infarction (STEMI) in a regional STEMI network: Results of the “Herzinfarktverbund Essen”. HERZ 2008, 33, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Larose, E.; Rodes-Cabau, J.; Pibarot, P.; Rinfret, S.; Proulx, G.; Nguyen, C.M.; Dery, J.P.; Gleeton, O.; Roy, L.; Noel, B. Predicting late myocardial recovery and outcomes in the early hours of ST-segment elevation myocardial infarction traditional measures compared with microvascular obstruction, salvaged myocardium, and necrosis characteristics by cardiovascular magnetic resonance. J. Am. Coll. Cardiol. 2010, 55, 2459–2469. [Google Scholar]
- Dall’Armellina, E.; Karia, N.; Lindsay, A.C.; Karamitsos, T.D.; Ferreira, V.; Robson, M.D.; Kellman, P.; Francis, J.M.; Forfar, C.; Prendergast, B.D. Dynamic changes of edema and late gadolinium enhancement after acute myocardial infarction and their relationship to functional recovery and salvage index. Circ. Cardiovasc. Imaging 2011, 4, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.; Ortiz, J.T.; Tejedor, P. Infarct size by contrast enhanced cardiac magnetic resonance is a stronger predictor of outcomes than left ventricular ejection fraction or end-systolic volume index: Prospective cohort study. Heart 2008, 94, 730–736. [Google Scholar]
- Reindl, M.; Holzknecht, M.; Tiller, C.; Lechner, I.; Schiestl, M.; Simma, F.; Pamminger, M.; Henninger, B.; Mayr, A.; Klug, G.; et al. Impact of infarct location and size on clinical outcome after ST-elevation myocardial infarction treated by primary percutaneous coronary intervention. Int. J. Cardiol. 2020, 301, 14–20. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients (n = 80) | MVO + T+ (n = 21) | MVO + T− (n = 28) | MVO − T+ (n = 6) | MVO − T– (n = 25) | p | |
|---|---|---|---|---|---|---|
| CV risk factors, n (%) | ||||||
| Hypertension | 44 (55) | 15 (71) | 17 (61) | 3 (5) | 9 (36) | 0.121 |
| Dyslipidemia | 60 (75) | 20 (95) | 20 (71) | 4 (67) | 16 (64) | 0.345 |
| Smoke | 42 (53) | 16 (57) | 13 (46) | 2 (33) | 11 (44) | 0.457 |
| Diabetes | 3 (4) | 2 (10) | 1 (4) | 0 | 0 | 0.091 |
| CAD family history | 24 (30) | 7 (33) | 9 (32) | 2 (33) | 6 (24) | 0.874 |
| eGFR ml/min/1.73 m2 median IQR (range) | 79 (67–92) | 70 (67–89) | 78 (75–92) | 79 (70–85) | 80 (67–93) | 0.786 |
| Culprit lesion, n (%) | ||||||
| LAD | 40 (50) | 20 (95) | 10 (36) | 6 (100) | 4 (16) | 0.091 |
| LCX | 23 (28) | 0 | 10 (36) | 0 | 11 (44) | 0.237 |
| RCA | 17 (21) | 1 (5) | 8 (29) | 0 | 10 (40) | 0.670 |
| Patients (n = 80) Median IQR (Range) | MVO + T+ (n = 21) Median IQR (Range) | MVO + T− (n = 28) Median IQR (Range) | MVO − T+ (n = 6) Median IQR (Range) | MVO − T− (n = 25) Median IQR (Range) | p | |
|---|---|---|---|---|---|---|
| CMR parameters | ||||||
| LVEDV ml/m2 | 94 (81–110) | 94 (81–109) | 94 (86–108) | 108 (81–125) | 94 (78–106) | 0.789 |
| LVESV ml/m2 | 56 (43–68) | 56 (49–69) | 59 (48–67) | 50 (41–79) | 46 (39–58) | 0.896 |
| EF% | 43 (33–51) | 40 (36–47) | 40 (34–48) | 41 (34–52) | 47 (40–51) | 0.444 |
| IS mass g | 39 (25–58) | 46 (28–60) | 47 (38–60) | 23 (16–40) | 24 (15–29) | 0.676 |
| IS mass/LV mass% | 33 (23–42) | 37 (27–44) | 39 (29–46) | 26 (14–36) | 22 (14–32) | 0.569 |
| MVO mass g | 0.53 (0.01–4.47) | 3.25 (0.43–9.08) | 1.84 (0.68–5.73) | 0 | 0 | 0.095 |
| MVO mass/LV mass % | 0.45 (0.01–2.84) | 2.58 (0.04–3.56) | 1.46 (0.03–2.89) | 0 | 0 | 0.085 |
| Echo parameters | ||||||
| LVEDV ml/m2 | 68 (56–81) | 67 (56–79) | 69 (60–79) | 69 (59–93) | 62 (52–72) | 0.433 |
| LVESV ml/m2 | 39 (29–49) | 40 (33–47) | 43 (32–50) | 44 (29–59) | 33 (28–44) | 0.326 |
| EF% | 43 (35–49) | 40 (36–47) | 40 (35–48) | 41 (33–51) | 47 (42–52) | 0.685 |
| Baseline Characteristics | Absence of MACE n = 58 | Presence of MACE n = 22 | p |
|---|---|---|---|
| CMR LVEF% median IQR (range) | 43 (35–53) | 35 (30–48) | 0.048 |
| Echo LVEF% median IQR (range) | 43 (36–49) | 39 (29–50) | 0.094 |
| CMR LVEDV mL/m2 median IQR (range) | 94 (82–109) | 95 (79–127) | 0.476 |
| CMR LVESV mL/m2 median IQR (range) | 56 (42–65) | 59 (47–86) | 0.276 |
| Echo LVEDV mL/m2 median IQR (range) | 68 (54–78) | 66 (60–82) | 0.443 |
| Echo LVESV mL/m2 median IQR (range) | 38 (28–46) | 42 (32–59) | 0.194 |
| IS mass g median IQR (range) | 34 (19–53) | 45 (28–70) | 0.027 |
| IS mass (%LV) median IQR (range) | 32 (17–40) | 39 (28–53) | 0.031 |
| MVO mass g median IQR (range) | 0.43 (0.01–3.14) | 0.43 (0.01–5.51) | 0.594 |
| MVO mass (%LV) median IQR (range) | 0.21 (0.01–2.22) | 0.38 (0.01–3.82) | 0.467 |
| eGFR mL/min/1.73 m2 median IQR (range) | 80 (68–91) | 66 (52–89) | 0.038 |
| LV thrombus treated with anticoagulation (%) | 30 | 59 | 0.016 |
| Baseline Characteristics | Univariate Analysis | ||
|---|---|---|---|
| HR | CI | p | |
| CMR LVEF% | 0.96 | 0.93–0.99 | 0.032 |
| Echo LVEF% | 0.95 | 0.91–1.00 | 0.050 |
| Echo LVEDV ml/m2 | 1.01 | 0.99–1.02 | 0.690 |
| Echo LVESV ml/m2 | 1.02 | 1.00–1.04 | 0.032 |
| IS mass g | 1.02 | 1.00–1.04 | 0.013 |
| IS mass (%LV) | 1.04 | 1.01–1.07 | 0.008 |
| IS mass > 18% | 3.49 | 0.82–14.97 | 0.092 |
| MVO presence | 1.09 | 0.46–2.59 | 0.854 |
| MVO mass | 1.06 | 0.99–1.13 | 0.086 |
| MVO mass (%LV) | 1.09 | 0.99–1.21 | 0.079 |
| MVO mass > 2.19% | 1.64 | 0.70–3.83 | 0.257 |
| eGFR | 0.98 | 0.96–1.00 | 0.016 |
| LV thrombus treated with anticoagulation | 2.83 | 1.21–6.64 | 0.017 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cecchetto, A.; Zupa, F.; De Lazzari, M.; Bolis, A.; Baritussio, A.; Nistri, S.; De Conti, G.; Perazzolo Marra, M. Intraventricular Thrombosis After Myocardial Infarction: Prognostic Evaluation in Relation to Microvascular Obstruction Extent by CMR. J. Clin. Med. 2025, 14, 2658. https://doi.org/10.3390/jcm14082658
Cecchetto A, Zupa F, De Lazzari M, Bolis A, Baritussio A, Nistri S, De Conti G, Perazzolo Marra M. Intraventricular Thrombosis After Myocardial Infarction: Prognostic Evaluation in Relation to Microvascular Obstruction Extent by CMR. Journal of Clinical Medicine. 2025; 14(8):2658. https://doi.org/10.3390/jcm14082658
Chicago/Turabian StyleCecchetto, Antonella, Francesco Zupa, Manuel De Lazzari, Angiola Bolis, Anna Baritussio, Stefano Nistri, Giorgio De Conti, and Martina Perazzolo Marra. 2025. "Intraventricular Thrombosis After Myocardial Infarction: Prognostic Evaluation in Relation to Microvascular Obstruction Extent by CMR" Journal of Clinical Medicine 14, no. 8: 2658. https://doi.org/10.3390/jcm14082658
APA StyleCecchetto, A., Zupa, F., De Lazzari, M., Bolis, A., Baritussio, A., Nistri, S., De Conti, G., & Perazzolo Marra, M. (2025). Intraventricular Thrombosis After Myocardial Infarction: Prognostic Evaluation in Relation to Microvascular Obstruction Extent by CMR. Journal of Clinical Medicine, 14(8), 2658. https://doi.org/10.3390/jcm14082658