
Defining and Evaluating the Impact of Bleeding Severity on Time to Endoscopy and Mortality Risk: A Prospective Multicenter Cohort Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Definitions
2.2. Bleeding Severity Analysis
2.3. Statistical Analysis
2.4. Internal Validation
3. Results
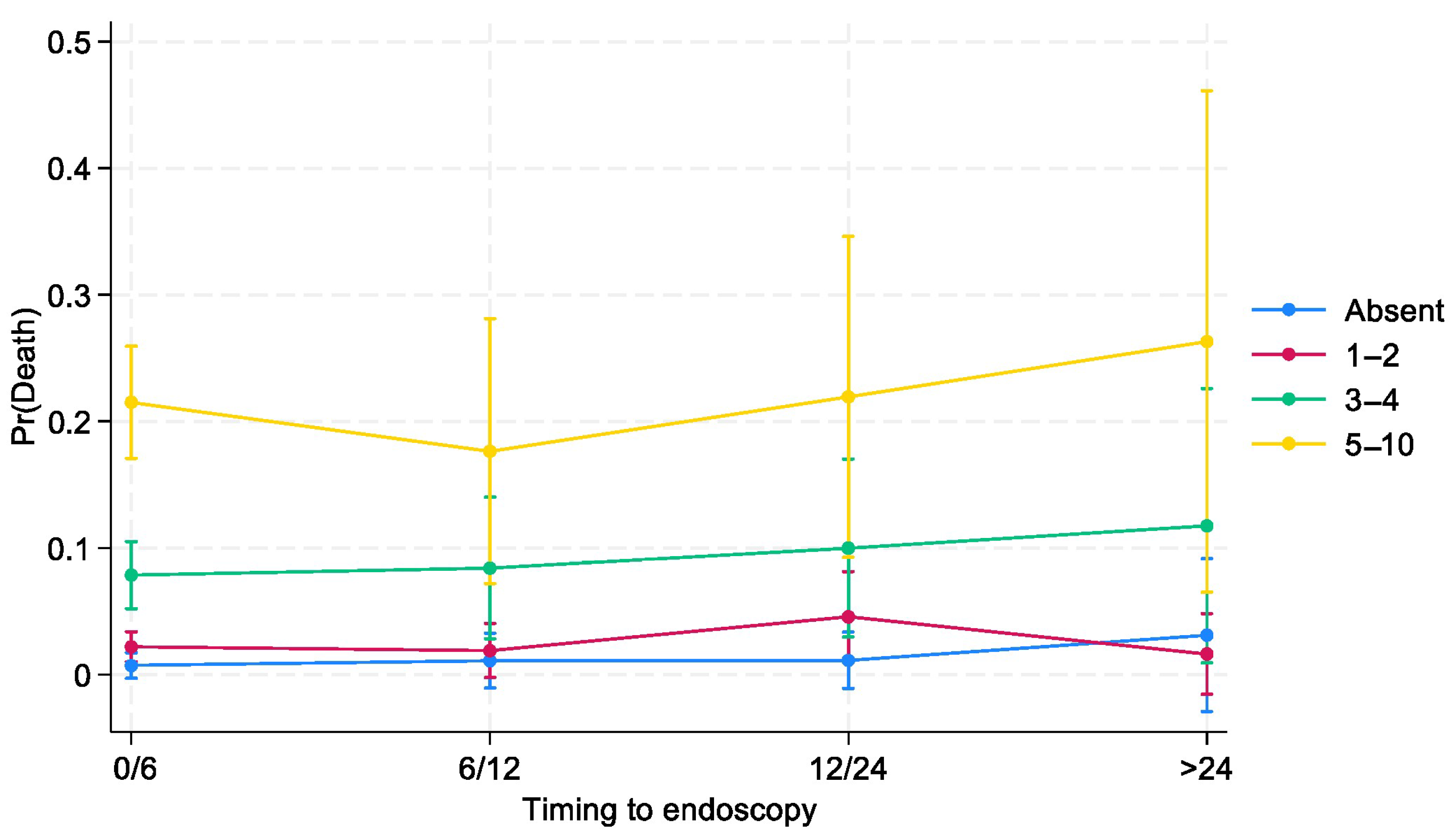
Bleeding Severity and Time to Endoscopy
4. Discussion
Perspective
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BleSev | bleeding severity |
| ASA score | American Society of Anesthesiologists physical status classification system |
| GB score | Glasgow–Blatchford score |
| Hb | hemoglobin |
| PPI | proton pump inhibitor |
| RBC | red blood cell |
| ED | emergency department |
| NSAIDs | nonsteroidal anti-inflammatory drugs |
| Bpm | beat per minute |
| SD | standard deviation |
| UGIB | upper gastrointestinal bleeding |
| 95% CI | 95% confidence interval |
References
- Laine, L.; Yang, H.; Chang, S.-C.; Datto, C. Trends for incidence of hospitalization and death due to GI complications in the United States from 2001 to 2009. Am. J. Gastroenterol. 2012, 107, 1190–1195; quiz 1196. [Google Scholar] [CrossRef] [PubMed]
- Abougergi, M.S.; Travis, A.C.; Saltzman, J.R. The in-hospital mortality rate for upper GI hemorrhage has decreased over 2 decades in the United States: A nationwide analysis. Gastrointest. Endosc. 2015, 81, 882–888. [Google Scholar] [CrossRef]
- Wuerth, B.A.; Rockey, D.C. Changing Epidemiology of Upper Gastrointestinal Hemorrhage in the Last Decade: A Nationwide Analysis. Dig. Dis. Sci. 2018, 63, 1286–1293. [Google Scholar] [CrossRef]
- Stanley, A.J.; Laine, L. Management of acute upper gastrointestinal bleeding. BMJ 2019, 364, l536. [Google Scholar] [CrossRef] [PubMed]
- Jairath, V.; Thompson, J.; Kahan, B.C.; Daniel, R.; A Hearnshaw, S.; Travis, S.P.L.; Murphy, M.F.; Palmer, K.R.; A Logan, R.F. Poor Outcomes in Hospitalized Patients With Gastrointestinal Bleeding: Impact of Baseline Risk, Bleeding Severity, and Process of Care. Am. J. Gastroenterol. 2014, 109, 1603–1612. [Google Scholar] [CrossRef]
- Guo, C.L.T.; Wong, S.H.; Lau, L.H.S.; Lui, R.N.S.; Mak, J.W.Y.; Tang, R.S.Y.; Yip, T.C.F.; Wu, W.K.K.; Wong, G.L.H.; Chan, F.K.L.; et al. Timing of endoscopy for acute upper gastrointestinal bleeding: A territory-wide cohort study. Gut 2022, 71, 1544–1550. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.Y.; Yu, Y.; Tang, R.S.; Chan, H.C.; Yip, H.-C.; Chan, S.M.; Luk, S.W.; Wong, S.H.; Lau, L.H.; Lui, R.N.; et al. Timing of Endoscopy for Acute Upper Gastrointestinal Bleeding. N. Engl. J. Med. 2020, 382, 1299–1308. [Google Scholar] [CrossRef] [PubMed]
- Laine, L.; Laursen, S.B.; Zakko, L.; Dalton, H.R.; Ngu, J.H.; Schultz, M.; Stanley, A.J. Severity and Outcomes of Upper Gastrointestinal Bleeding With Bloody Vs. Coffee-Grounds Hematemesis. Am. J. Gastroenterol. 2018, 113, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Daabiss, M. American Society of Anaesthesiologists physical status classification. Indian J. Anaesth. 2011, 55, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Gralnek, I.M.; Stanley, A.J.; Morris, A.J.; Camus, M.; Lau, J.; Lanas, A.; Laursen, S.B.; Radaelli, F.; Papanikolaou, I.S.; Gonçalves, T.C.; et al. Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2021. Endoscopy 2021, 53, 300–332. [Google Scholar] [CrossRef] [PubMed]
- Blatchford, O.; Murray, W.R.; Blatchford, M. A risk score to predict need for treatment for uppergastrointestinal haemorrhage. Lancet 2000, 356, 1318–1321. [Google Scholar] [CrossRef]
- Laine, L.; Spiegel, B.; Rostom, A.; Moayyedi, P.; Kuipers, E.J.; Bardou, M.; Sung, J.; Barkun, A.N. Methodology for Randomized Trials of Patients With Nonvariceal Upper Gastrointestinal Bleeding: Recommendations From an International Consensus Conference. Am. J. Gastroenterol. 2010, 105, 540–550. [Google Scholar] [CrossRef] [PubMed]
- De Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Abraldes, J.G.; Albillos, A.; Baiges, A.; Bajaj, J.; Bañares, R.; et al. Baveno VII—Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet Lond. Engl. 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Torres, C.M.; Kenzik, K.M.; Saillant, N.N.; Scantling, D.R.; Sanchez, S.E.; Brahmbhatt, T.S.; Dechert, T.A.; Sakran, J.V. Timing to First Whole Blood Transfusion and Survival Following Severe Hemorrhage in Trauma Patients. JAMA Surg. 2024, 159, 374. [Google Scholar] [CrossRef]
- Marmo, R.; Soncini, M.; de Franchis, R. GISED—Gruppo Italiano per lo Studio dell’Emorragia Digestiva. Patient’s performance status should dictate transfusion strategy in nonvariceal acute upper gastrointestinal bleeding (NV-AUGIB): A prospective multicenter cohort study: Transfusion strategy in NV-AUGIB. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2020, 52, 1156–1163. [Google Scholar]
- Ogundimu, E.O.; Altman, D.G.; Collins, G.S. Adequate sample size for developing prediction models is not simply related to events per variable. J. Clin. Epidemiol. 2016, 76, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): The TRIPOD Statement. Ann. Intern. Med. 2015, 162, 55. [Google Scholar] [CrossRef] [PubMed]
- Stanley, A.; Ashley, D.; Dalton, H.; Mowat, C.; Gaya, D.R.; Thompson, E.; Warshow, U.; Groome, M.; Cahill, A.; Benson, G.; et al. Outpatient management of patients with low-risk upper-gastrointestinal haemorrhage: Multicentre validation and prospective evaluation. Lancet 2009, 373, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Shung, D.L.; Au, B.; Taylor, R.A.; Tay, J.K.; Laursen, S.B.; Stanley, A.J.; Dalton, H.R.; Ngu, J.; Schultz, M.; Laine, L. Validation of a Machine Learning Model That Outperforms Clinical Risk Scoring Systems for Upper Gastrointestinal Bleeding. Gastroenterology 2020, 158, 160–167. [Google Scholar] [CrossRef]
- Bucci, C.; Marmo, C.; Soncini, M.; Riccioni, M.E.; Laursen, S.B.; Gralnek, I.M.; Marmo, R.; Amitrano, L.; Anderloni, A.; Andriulli, A.; et al. The interaction of patients’ physical status and time to endoscopy on mortality risk in patients with upper gastrointestinal bleeding: A national prospective cohort study. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2024, 56, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Merola, E.; Michielan, A.; de Pretis, G. Optimal timing of endoscopy for acute upper gastrointestinal bleeding: A systematic review and meta-analysis. Intern. Emerg. Med. 2021, 16, 1331–1340. [Google Scholar] [CrossRef] [PubMed]
- Saffouri, E.; Blackwell, C.; Laursen, S.B.; Laine, L.; Dalton, H.R.; Ngu, J.; Shultz, M.; Norton, R.; Stanley, A.J. The Shock Index is not accurate at predicting outcomes in patients with upper gastrointestinal bleeding. Aliment Pharmacol. Ther. 2020, 51, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Jiang, W.; Cheng, R.; Dang, Y.; Min, L.; Zhang, S. Does Early Endoscopy Affect the Clinical Outcomes of Patients with Acute Nonvariceal Upper Gastrointestinal Bleeding? A Systematic Review and Meta-Analysis. Gut Liver 2023, 17, 566–580. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Number of Patients out of 2525 | |
|---|---|
| Age, mean (±SD) | 68 (±15.8) |
| Male, n (%) | 1691 (67.3%) |
| Outpatients, n (%) | 2142 (84.8%) |
| Cardiac frequency, bpm mean (±SD) | 89.3 (±16.5) |
| Mean systolic blood pressure, mean (±SD)) | 115.6 (±22.6) |
| Mean diastolic blood pressure, mean (±SD) | 67.4 (±12.9) |
| Hemoglobin levels, g/dL (IQR) | 8.8 (7.4–10.7) |
| Blood urea nitrogen, mg/dL (IQR) | 58.0 (38–92) |
| Clinical presentation | |
| Syncope, n (%) | 256 (10.1%) |
| Altered mental status, n (%) | 420 (16.6%) |
| Hematemesis, n (%) | 1127 (44.6%) |
| Melena, n (%) | 1660 (65.7%) |
| Comorbidities | |
| ASA score | |
| I | 648 (25.7%) |
| II | 856 (33.9%) |
| III | 855 (33.9%) |
| IV | 166 (6.6%) |
| Renal failure | 326 (12.9%) |
| Chronic coronary artery disease, n (%) | 552 (21.9%) |
| Chronic obstructive pulmonary disease, n (%) | 284 (11.2%) |
| Neoplasia, n (%) | 408 (16.2%) |
| Cirrhosis, n (%) | 537 (21.3%) |
| CHILD score, mean (IQR) | 8 (6–10) |
| Number of patients receiving RBC transfusion before endoscopy, n (%) | 585 (23.2%) |
| Nonvariceal source of bleeding, n (%) | 2079 (82.3%) |
| Weight | |
|---|---|
| Altered mental status, yes | 3 |
| Systolic blood pressure ≤ 100 mmHg | 2 |
| Blood urea nitrogen level ≥ 130 mg/dL | 2 |
| Hemoglobin level ≤ 8 g/dL | 2 |
| Hematemesis, yes | 1 |
| Total | 10 |
| Death by Any Cause | |||
|---|---|---|---|
| Odds Ratio | p | (95% CI) | |
| No risk factors (reference) | 1 | ||
| 1–2 | 2.41 | 0.077 | 0.91–6.37 |
| 3–4 | 9.25 | 0.000 | 3.67–23.36 |
| ≥5 | 26.29 | 0.000 | 10.59–65.27 |
| Bleeding Severity Scale | ||||||
|---|---|---|---|---|---|---|
| Total | 0 | 1–2 | 3–4 | ≥5 | p-Value | |
| n = 2525 | n = 498 | n = 965 | n = 606 | n = 456 | ||
| Time lapse from the ED to endoscopy (h) | <0.001 | |||||
| 0–6, n (%) 6–12, n (%) 12–24, n (%) >24, n (%) | 1589 (64.6) 393 (16.0) 330 (13.4) 146 (5.9) | 275 (56.7) 90 (18.6) 88 (18.1) 32 (6.6) | 590 (62.8) 157 (16.7) 131 (14) 61 (6.5) | 394 (66.4) 95 (16.0) 70 (11.8) 34 (5.7) | 330 (72.3) 51 (11.6) 41 (9.3) 19 (4.3) | |
| High-risk stigmata at index endoscopy, n (%) | 771 (30.5) | 158 (31.7) | 276 (28.6) | 172 (28.4) | 165 (36.2) | 0.017 |
| Need for therapeutic endoscopy, n (%) | 1477 (58.5) | 230 (46.2) | 543 (56.3) | 387 (63.9) | 317 (69.5) | <0.001 |
| Transfusion(s), n (%) | 1554 (61.5) | 170 (34.1) | 558 (57.8) | 423 (69.8) | 403 (88.4) | <0.001 |
| Transfusion number, (IQR) | 2 (0–3) | 0 (0–2) | 1 (0–3) | 2 (0–3) | 3 (2–4) | <0.001 |
| Rebleeding, n (%) | 157 (6.2) | 13 (2.6) | 33 (3.4) | 45 (7.4) | 66 (14.5) | <0.001 |
| Need for surgery or interventional radiology, n (%) | 98 (3.9) | 15 (3) | 29 (3) | 27 (4.5) | 27 (5.9) | 0.035 |
| Death by any cause, n (%) | 176 (7) | 5 (1) | 23 (2.4) | 52 (8.6) | 96 (21.1) | <0.001 |
| Length of stay, day(s) mean (± SD) | 9.7 (± 8.8) | 7.9 (± 7.1) | 9.2 (± 8.9) | 10 (± 8.3) | 12.3 (± 10.3) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marmo, C.; Bucci, C.; Soncini, M.; Riccioni, M.E.; Marmo, R.; on behalf of the GISED Study Group. Defining and Evaluating the Impact of Bleeding Severity on Time to Endoscopy and Mortality Risk: A Prospective Multicenter Cohort Study. J. Clin. Med. 2025, 14, 1643. https://doi.org/10.3390/jcm14051643
Marmo C, Bucci C, Soncini M, Riccioni ME, Marmo R, on behalf of the GISED Study Group. Defining and Evaluating the Impact of Bleeding Severity on Time to Endoscopy and Mortality Risk: A Prospective Multicenter Cohort Study. Journal of Clinical Medicine. 2025; 14(5):1643. https://doi.org/10.3390/jcm14051643
Chicago/Turabian StyleMarmo, Clelia, Cristina Bucci, Marco Soncini, Maria Elena Riccioni, Riccardo Marmo, and on behalf of the GISED Study Group. 2025. "Defining and Evaluating the Impact of Bleeding Severity on Time to Endoscopy and Mortality Risk: A Prospective Multicenter Cohort Study" Journal of Clinical Medicine 14, no. 5: 1643. https://doi.org/10.3390/jcm14051643
APA StyleMarmo, C., Bucci, C., Soncini, M., Riccioni, M. E., Marmo, R., & on behalf of the GISED Study Group. (2025). Defining and Evaluating the Impact of Bleeding Severity on Time to Endoscopy and Mortality Risk: A Prospective Multicenter Cohort Study. Journal of Clinical Medicine, 14(5), 1643. https://doi.org/10.3390/jcm14051643