
Associations Between Upper Extremity Activity Capacity and Strength and Post-Operative Ambulation After Geriatric Hip Fracture: A Prospective Controlled Study

Abstract

1. Introduction
2. Materials and Methods
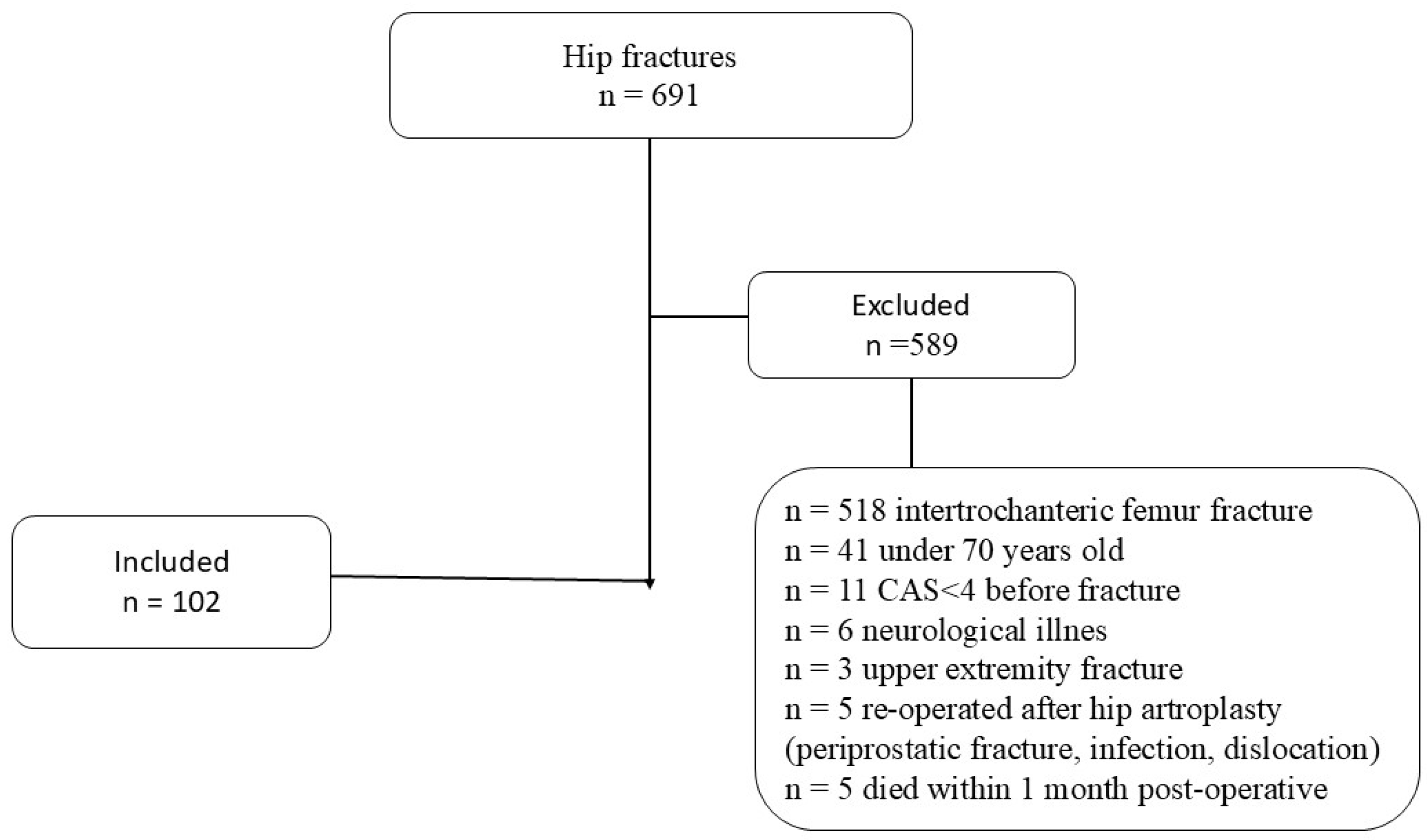
2.1. Patient Inclusion
2.2. Evaluation of Patients
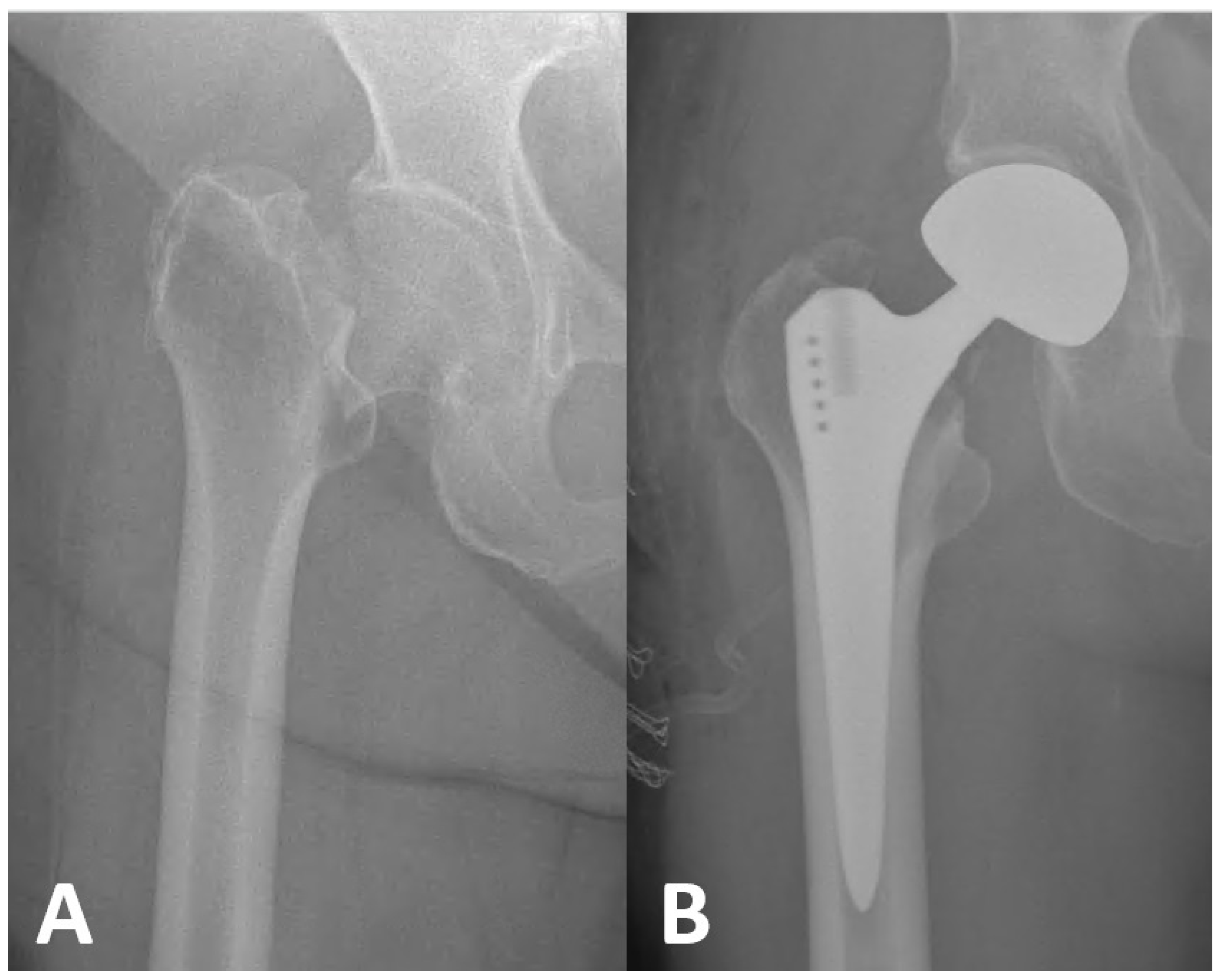
2.3. Surgical Technique and Follow-Up Protocol
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Veronese, N.; Maggi, S. Epidemiology and social costs of hip fracture. Injury 2018, 49, 1458–1460. [Google Scholar] [CrossRef]
- Tunçez, M.; Bulut, T.; Süner, U.; Önder, Y.; Kazımoğlu, C. Prognostic nutritional index (PNI) is an independent risk factor for the postoperative mortality in geriatric patients undergoing hip arthroplasty for femoral neck fracture? A prospective controlled study. Arch. Orthop. Trauma Surg. 2024, 144, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Hershkovitz, A.; Pulatov, I.; Brill, S.; Beloosesky, Y. Can hip-fractured elderly patients maintain their rehabilitation achievements after 1 year? Disabil. Rehabil. 2012, 34, 304–310. [Google Scholar] [CrossRef]
- Bozkurt, H.H.; Tokgöz, M.A.; Yapar, A.; Atik, O.Ş. What is the importance of canal-to-diaphysis ratio on osteoporosis-related hip fractures? Eklem. Hastalik. Cerrahisi. 2019, 30, 296–300. [Google Scholar] [CrossRef] [PubMed]
- McDonough, C.M.; Harris-Hayes, M.; Kristensen, M.T.; Overgaard, J.A.; Herring, T.B.; Kenny, A.M.; Mangione, K.K. Physical Therapy Management of Older Adults with Hip Fracture. J. Orthop. Sports Phys. Ther. 2021, 51, CPG1–CPG81. [Google Scholar] [CrossRef] [PubMed]
- Gleich, J.; Pfeufer, D.; Keppler, A.M.; Mehaffey, S.; Fürmetz, J.; Böcker, W.; Kammerlander, C.; Neuerburg, C. Identification of hip fracture patients at risk for postoperative mobilisation complications via handgrip strength assessment. Arch. Orthop. Trauma Surg. 2022, 142, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.T.; Andersen, L.; Bech-Jensen, R.; Moos, M.; Hovmand, B.; Ekdahl, C.; Kehlet, H. High intertester reliability of the Cumulated Ambulation Score for the evaluation of basic mobility in patients with hip fracture. Clin. Rehabil. 2009, 23, 1116–1123. [Google Scholar] [CrossRef] [PubMed]
- Min, K.; Beom, J.; Kim, B.R.; Lee, S.Y.; Lee, G.J.; Lee, J.H.; Lee, S.Y.; Won, S.J.; Ahn, S.; Bang, H.J.; et al. Clinical Practice Guideline for Postoperative Rehabilitation in Older Patients with Hip Fractures. Ann. Rehabil. Med. 2021, 45, 225–259. [Google Scholar] [CrossRef]
- Gu, Q.; Koenig, L.; Mather, R.C., 3rd; Tongue, J. Surgery for hip fracture yields societal benefits that exceed the direct medical costs. Clin. Orthop. Relat. Res. 2014, 472, 3536–3546. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.S.; Jeon, Y.S.; Ahn, C.H.; Roh, T.H. Osteosynthesis versus endoprosthesis for the treatment of femoral neck fracture in Asian elderly patients. BMC Musculoskelet. Disord. 2016, 17, 264. [Google Scholar] [CrossRef] [PubMed]
- Storr, B.; Peiris, C.L.; Snowdon, D.A. Community Reintegration After Rehabilitation for Hip Fracture: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2022, 103, 1638–1650. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.I.; Kim, J.T.; Park, C.H.; Cha, Y. Diagnosis and Management of Sarcopenia after Hip Fracture Surgery: Current Concept Review. Hip Pelvis 2022, 34, 1–9. [Google Scholar] [CrossRef]
- Conte, M.; Vasuri, F.; Trisolino, G.; Bellavista, E.; Santoro, A.; Degiovanni, A.; Martucci, E.; D’Errico-Grigioni, A.; Caporossi, D.; Capri, M.; et al. Increased Plin2 expression in human skeletal muscle is associated with sarcopenia and muscle weakness. PLoS ONE 2013, 8, e73709. [Google Scholar] [CrossRef] [PubMed]
- Savino, E.; Martini, E.; Lauretani, F.; Pioli, G.; Zagatti, A.M.; Frondini, C.; Pellicciotti, F.; Giordano, A.; Ferrari, A.; Nardelli, A.; et al. Handgrip strength predicts persistent walking recovery after hip fracture surgery. Am. J. Med. 2013, 126, 1068–1075.e1. [Google Scholar] [CrossRef] [PubMed]
- Siminiuc, D.; Gumuskaya, O.; Mitchell, R.; Bell, J.; Cameron, I.D.; Hallen, J.; Birkenhead, K.; Hurring, S.; Baxter, B.; Close, J.; et al. Rehabilitation after surgery for hip fracture—The impact of prompt, frequent and mobilisation-focused physiotherapy on discharge outcomes: An observational cohort study. BMC Geriatr. 2024, 24, 629. [Google Scholar] [CrossRef]
- Chang, C.M.; Lee, C.H.; Shih, C.M.; Wang, S.P.; Chiu, Y.C.; Hsu, C.E. Handgrip strength: A reliable predictor of postoperative early ambulation capacity for the elderly with hip fracture. BMC Musculoskelet. Disord. 2021, 22, 103. [Google Scholar] [CrossRef] [PubMed]
- Hershkovitz, A.; Yichayaou, B.; Ronen, A.; Maydan, G.; Kornyukov, N.; Burstin, A.; Brill, S. The association between hand grip HGS and rehabilitation outcome in post-acute hip fractured patients. Aging Clin. Exp. Res. 2019, 31, 1509–1516. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Kim, C.H.; Kim, J.W. Handgrip strength effectiveness and optimal measurement timing for predicting functional outcomes of a geriatric hip fracture. Sci. Rep. 2022, 12, 20600. [Google Scholar] [CrossRef] [PubMed]
- Foss, N.B.; Kristensen, M.T.; Kehlet, H. Prediction of postoperative morbidity, mortality and rehabilitation in hip fracture patients: The cumulated ambulation score. Clin. Rehabil. 2006, 20, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Grana, E.; Verzellotti, S.; Grassi, F.A.; Ferriero, G.; Kristensen, M.T.; Cisari, C.; Invernizzi, M. Cross-cultural validation of the Italian version of the Cumulated Ambulation Score. Int. J. Rehabil. Res. 2016, 39, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Wright, J.G.; Katz, J.N.; Upper Extremity Collaborative Group. Development of the QuickDASH: Comparison of three item-reduction approaches. J. Bone Jt. Surg. Am. 2005, 87, 1038–1046. [Google Scholar]
- Hillman, T.E.; Nunes, Q.M.; Hornby, S.T.; Stanga, Z.; Neal, K.R.; Rowlands, B.J.; Allison, S.P.; Lobo, D.N. A practical posture for hand grip dynamometry in the clinical setting. Clin. Nutr. 2005, 24, 224–228. [Google Scholar] [CrossRef]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Kuh, D.; Cooper, C.; Sayer, A.A. Global variation in grip strength: A systematic review and meta-analysis of normative data. Age Ageing 2016, 45, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Pallardo Rodil, B.; Gómez Pavón, J.; Menéndez Martínez, P. Hip fracture mortality: Predictive models. Med. Clin. 2020, 154, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Ortíz Martínez, J.G.; Bodu Lamberti, E.M.; Karduss Preciado, C.; Polo Miranda, M.F. Experience of a centre of excellence in hip fractures of the elderly in Colombia: Influence of time-to-surgery on inpatient mortality and complications. Int. Orthop. 2024, 48, 2499–2504. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Díaz-Guerra, G.; Hawkins Carranza, F.; Librizzi, S. Socioeconomic status, osteoporosis and fragility fractures. Rev. Española Cirugía Ortopédica Traumatol. 2024, 24, 110–113. [Google Scholar]
- Umehara, T.; Kaneguchi, A.; Watanabe, K.; Katayama, N.; Teramoto, H.; Kuwahara, D.; Kaneyashiki, R.; Mizuno, T.; Kito, N.; Kakehashi, M. Association between physical function and parameters of hip structural analysis in patients with hip fracture. Hip Int. 2024, 34, 677–683. [Google Scholar] [CrossRef]
- Krakers, S.M.; Woudsma, S.; van Dartel, D.; Vermeer, M.; Vollenbroek-Hutten, M.M.; Hegeman, J.H.; on behalf of the Up & Go after a Hip Fracture Group. Rehabilitation of Frail Older Adults after Hip Fracture Surgery: Predictors for the Length of Geriatric Rehabilitation Stay at a Skilled Nursing Home. J. Clin. Med. 2024, 13, 4547. [Google Scholar] [CrossRef]
- Handoll, H.H.; Cameron, I.D.; Mak, J.C.; Panagoda, C.E.; Finnegan, T.P. Multidisciplinary rehabilitation for older people with hip fractures. Cochrane Database Syst. Rev. 2021, 11, CD007125. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Zhong, F.; Zhan, X.; Bao, Y.; Zhu, X. Postoperative rehabilitation exercise experiences of geriatric patients with femoral neck fractures based on the perspective of medical staff: A qualitative study. BMC Geriatr. 2024, 24, 667. [Google Scholar] [CrossRef] [PubMed]
- Sieber, F.E.; Barnett, S.R. Preventing postoperative complications in the elderly. Anesth. Clin. 2011, 29, 83–97. [Google Scholar] [CrossRef]
- Rantanen, T.; Masaki, K.; He, Q.; Ross, G.W.; Willcox, B.J.; White, L. Midlife muscle strength and human longevity up to age 100 years: A 44-year prospective study among a decedent cohort. Age 2012, 34, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Deeg, D.J.; Lips, P.; Harris, T.B.; Bouter, L.M. Skeletal muscle mass and muscle strength in relation to lower-extremity performance in older men and women. J. Am. Geriatr. Soc. 2000, 48, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Beloosesky, Y.; Weiss, A.; Manasian, M.; Salai, M. Handgrip strength of the elderly after hip fracture repair correlates with functional outcome. Disabil. Rehabil. 2010, 32, 367–373. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| x ± sd | M (Min–Max) | |
|---|---|---|
| Age (year) | 78.83 ± 6.99 | 78.50 (70–93) |
| BMI | 25.48 ± 3.01 | 25.35 (19–29) |
| Female | 65 | - |
| Male | 37 | - |
| Time until surgery (day) | 3.80 ± 1.06 | 4 (1–5) |
| Time after surgery (day) | 4.17 ± 2.06 | 4 (1–8) |
| Total hospital stay (day) | 7.97 ± 2.36 | 8 (3–13) |
| Preop CAS | 5.45 ± 0.74 | 6 (4–6) |
| Postop CAS (3rd day) | 3.24 ± 1.02 | 3 (0–6) |
| Postop CAS (1st month) | 4.01 ± 1.05 | 4 (1–6) |
| Postop QDASH (3rd day) | 35.18 ± 33.02 | 35.10 (0–84.09) |
| Postop QDASH (1st month) | 36.15 ± 33.90 | 38.25 (0–96) |
| Postop HGS (kg) (3rd day) | 16.79 ± 9.99 | 15 (2.2–45) |
| Postop HGS (kg) (1st month) | 17.20 ± 10.20 | 15.2 (3–46) |
| Preop CAS | Postop CAS 3rd Day | Postop CAS 1st Month | Postop QDASH 3rd Day | Postop QDASH 1st Month | Postop HGS 3rd Day | Postop HGS 1st Month | |
|---|---|---|---|---|---|---|---|
| Age | −0.489 ** 0.001 | −0.373 ** 0.001 | −0.417 ** 0.001 | 0.530 ** 0.001 | 0.560 ** 0.001 | −0.519 ** 0.001 | −0.529 ** 0.001 |
| BMI | 0.003 0.979 | 0.156 0.118 | 0.061 0.544 | 0.087 0.386 | 0.097 0.396 | 0.040 0.689 | 0.060 0.689 |
| Time until surgery | −0.082 0.412 | −0.013 0.898 | −0.134 0.178 | 0.052 0.601 | 0.062 0.621 | −0.061 0.540 | −0.081 0.540 |
| Time after surgery | 0.002 0.988 | 0.111 0.267 | 0.082 0.413 | 0.088 0.377 | 0.098 0.377 | 0.126 0.208 | 0.156 0.208 |
| Total hospital stay | −0.010 0.921 | 0.059 0.556 | 0.012 0.907 | 0.065 0.518 | 0.075 0.538 | 0.090 0.367 | 0.190 0.367 |
| Preop CAS | x | 0.450 ** 0.001 * | 0.485 ** 0.001 | −0.532 * 0.001 | −0.532 * 0.001 | 0.483 ** 0.001 | 0.513 ** 0.001 |
| Postop CAS 3rd day | 0.450 ** 0.001 * | x | 0.699 ** 0.001 | −0.504 ** 0.001 | −0.494 ** 0.001 | 0.405 ** 0.001 | 0.415 ** 0.001 |
| Postop CAS 1st month | 0.485 ** 0.001 | 0.699 ** 0.001 | x | −0.589 0.001 | −0.579 ** 0.001 | 0.617 ** 0.001 | 0.717 ** 0.001 |
| Postop QDASH 3rd day | −0.552 * 0.001 | −0.504 ** 0.001 | −0.589 0.001 | x | 0.072 0.413 | −0.418 ** 0.001 | −0.446 ** 0.001 |
| Postop QDASH 1st month | −0.532 * 0.001 | −0.494 ** 0.001 | −0.579 0.001 | 0.072 0.413 | x | −0.518 ** 0.001 | −0.408 ** 0.001 |
| Postop HGS 3rd day | 0.483 ** 0.001 | 0.405 ** 0.001 | 0.617 ** 0.001 | −0.418 ** 0.001 | −0.518 ** 0.001 | x | 0.087 0.340 |
| Postop HGS 1st month | 0.513 ** 0.001 | 0.415 ** 0.001 | 0.717 ** 0.001 | −0.446 ** 0.001 | −0.408 ** 0.001 | 0.087 0.340 | x |
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | VIF | |
|---|---|---|---|---|---|---|
| B | Std. Error | Beta | ||||
| Constant | 3.55 | 1.10 | – | 3.209 | 0.002 | – |
| Postop QDASH 1st month | −0.01 | 0.00 | −0.365 | −4.018 | <0.001 | 1.606 |
| Postop HGS 1st month | 0.05 | 0.01 | 0.437 | 4.857 | <0.001 | 1.575 |
| Age | 0.00 | 0.01 | 0.000 | −0.005 | 0.996 | 1.528 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuncez, M.; Bulut, T.; Onder, Y.; Talar, O.R. Associations Between Upper Extremity Activity Capacity and Strength and Post-Operative Ambulation After Geriatric Hip Fracture: A Prospective Controlled Study. J. Clin. Med. 2025, 14, 1040. https://doi.org/10.3390/jcm14041040
Tuncez M, Bulut T, Onder Y, Talar OR. Associations Between Upper Extremity Activity Capacity and Strength and Post-Operative Ambulation After Geriatric Hip Fracture: A Prospective Controlled Study. Journal of Clinical Medicine. 2025; 14(4):1040. https://doi.org/10.3390/jcm14041040
Chicago/Turabian StyleTuncez, Mahmut, Tugrul Bulut, Yilmaz Onder, and Omur Rezan Talar. 2025. "Associations Between Upper Extremity Activity Capacity and Strength and Post-Operative Ambulation After Geriatric Hip Fracture: A Prospective Controlled Study" Journal of Clinical Medicine 14, no. 4: 1040. https://doi.org/10.3390/jcm14041040
APA StyleTuncez, M., Bulut, T., Onder, Y., & Talar, O. R. (2025). Associations Between Upper Extremity Activity Capacity and Strength and Post-Operative Ambulation After Geriatric Hip Fracture: A Prospective Controlled Study. Journal of Clinical Medicine, 14(4), 1040. https://doi.org/10.3390/jcm14041040