


Association of Immune-Mediated Inflammatory Diseases and Fracture Risk in Patients with Type 2 Diabetes: A Nationwide Population-Based Study

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Methods
2.1. Data Source
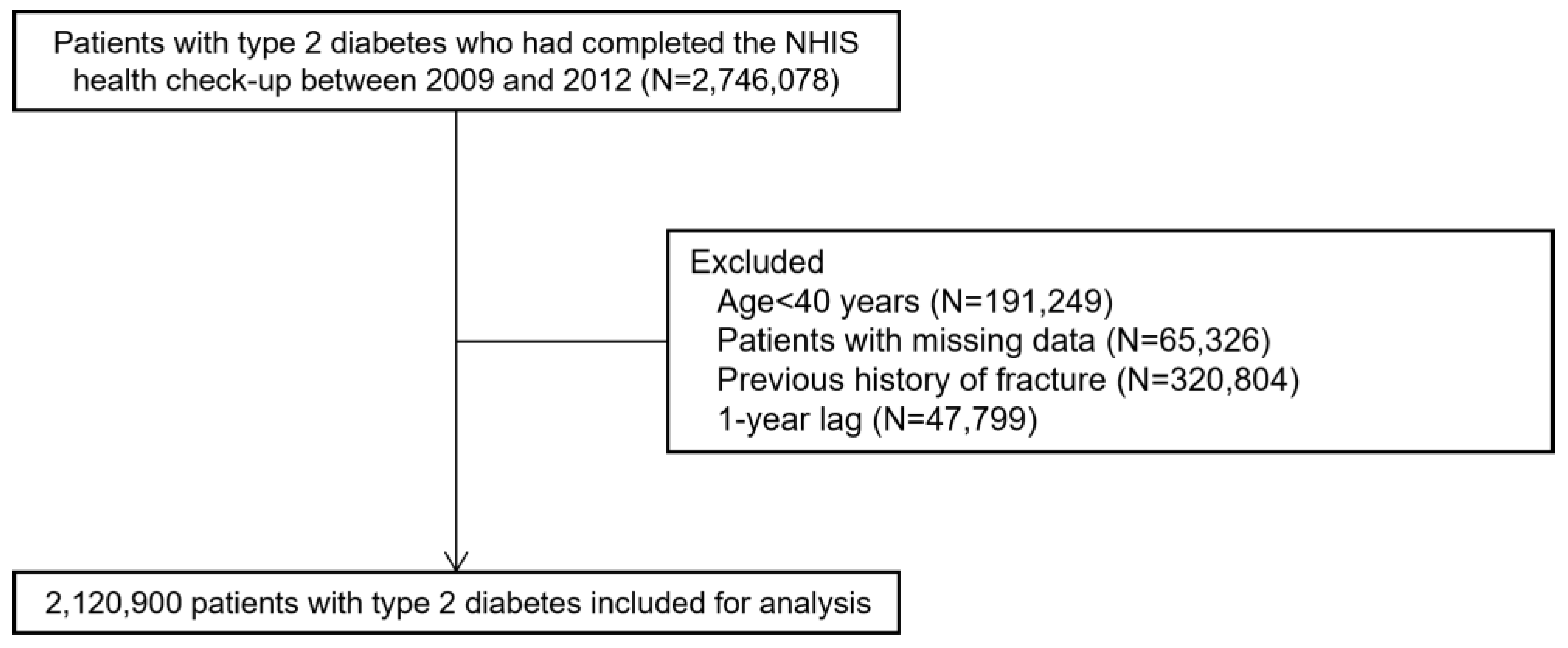
2.2. Study Cohort
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
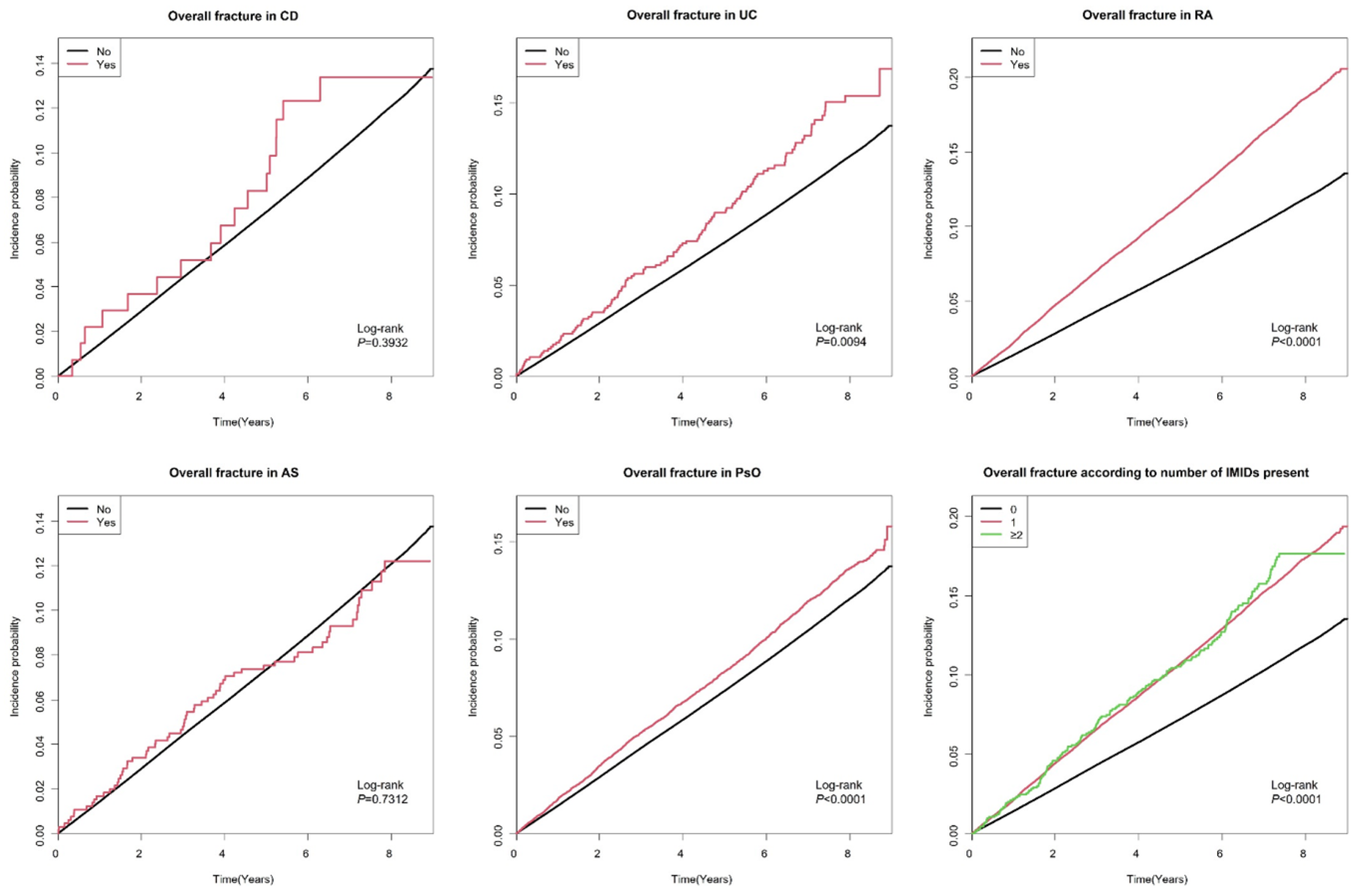
3.2. Incidence and Risk of Overall Fractures According to the Presence of IMIDs
3.3. Incidence and Risk of Osteoporotic and Non-Osteoporotic Fractures According to the Presence of IMIDs
3.4. Incidence and Risk of Vertebral and Hip Fractures According to the Presence of IMIDs
3.5. Subgroup Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Napoli, N.; Incalzi, R.A.; De Gennaro, G.; Marcocci, C.; Marfella, R.; Papalia, R.; Purrello, F.; Ruggiero, C.; Tarantino, U.; Tramontana, F.; et al. Bone fragility in patients with diabetes mellitus: A consensus statement from the working group of the Italian Diabetes Society (SID), Italian Society of Endocrinology (SIE), Italian Society of Gerontology and Geriatrics (SIGG), Italian Society of Orthopaedics and Traumatology (SIOT). Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1375–1390. [Google Scholar] [CrossRef] [PubMed]
- Oei, L.; Rivadeneira, F.; Zillikens, M.C.; Oei, E.H. Diabetes, diabetic complications, and fracture risk. Curr. Osteoporos. Rep. 2015, 13, 106–115. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Thong, E.P.; Milat, F.; Enticott, J.C.; Joham, A.E.; Ebeling, P.R.; Mishra, G.D.; Teede, H.J. The diabetes-fracture association in women with type 1 and type 2 diabetes is partially mediated by falls: A 15-year longitudinal study. Osteoporos. Int. 2021, 32, 1175–1184. [Google Scholar] [CrossRef] [PubMed]
- Dytfeld, J.; Michalak, M. Type 2 diabetes and risk of low-energy fractures in postmenopausal women: Meta-analysis of observational studies. Aging Clin. Exp. Res. 2017, 29, 301–309. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vestergaard, P. Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes--a meta-analysis. Osteoporos. Int. 2007, 18, 427–444. [Google Scholar] [CrossRef] [PubMed]
- Rathmann, W.; Kostev, K. Fracture risk in patients with newly diagnosed type 2 diabetes: A retrospective database analysis in primary care. J. Diabetes Complicat. 2015, 29, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Cavati, G.; Pirrotta, F.; Merlotti, D.; Ceccarelli, E.; Calabrese, M.; Gennari, L.; Mingiano, C. Role of Advanced Glycation End-Products and Oxidative Stress in Type-2-Diabetes-Induced Bone Fragility and Implications on Fracture Risk Stratification. Antioxidants 2023, 12, 928. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eller-Vainicher, C.; Cairoli, E.; Grassi, G.; Grassi, F.; Catalano, A.; Merlotti, D.; Falchetti, A.; Gaudio, A.; Chiodini, I.; Gennari, L. Pathophysiology and Management of Type 2 Diabetes Mellitus Bone Fragility. J. Diabetes Res. 2020, 2020, 7608964. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schett, G.; McInnes, I.B.; Neurath, M.F. Reframing Immune-Mediated Inflammatory Diseases through Signature Cytokine Hubs. N. Engl. J. Med. 2021, 385, 628–639. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, P.; Mosekilde, L. Fracture risk in patients with celiac Disease, Crohn’s disease, and ulcerative colitis: A nationwide follow-up study of 16,416 patients in Denmark. Am. J. Epidemiol. 2002, 156, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N.; Blanchard, J.F.; Leslie, W.; Wajda, A.; Yu, B.N. The incidence of fracture among patients with inflammatory bowel disease. A population-based cohort study. Ann. Intern. Med. 2000, 133, 795–799. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.J.; Wick, M.C.; Ackermann, P.W.; Montgomery, S.M. Increased fracture risk in patients with rheumatic disorders and other inflammatory diseases—A case-control study with 53,108 patients with fracture. J. Rheumatol. 2010, 37, 2247–2250. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Mahl, M.; Sachs, M.C.; Björk, J.; Michaelsson, K.; Ekbom, A.; Johan, A.; Ann-Sofie, B.; Ola, O. Fracture Risk in Patients with Inflammatory Bowel Disease: A Nationwide Population-Based Cohort Study From 1964 to 2014. Am. J. Gastroenterol. 2019, 114, 291–304. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; Hsieh, E.; Peng, L.; Yu, C.; Wang, Y.; Wu, C.; Wang, Q.; Li, M.; Zeng, X. Incidence of fractures among patients with rheumatoid arthritis: A systematic review and meta-analysis. Osteoporos. Int. 2018, 29, 1263–1275. [Google Scholar] [CrossRef] [PubMed]
- Sambrook, P.N.; Geusens, P. The epidemiology of osteoporosis and fractures in ankylosing spondylitis. Ther. Adv. Musculoskelet. Dis. 2012, 4, 287–292. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vosse, D.; Landewé, R.; van der Heijde, D.; van der Linden, S.; van Staa, T.P.; Geusens, P. Ankylosing spondylitis and the risk of fracture: Results from a large primary care-based nested case-control study. Ann. Rheum. Dis. 2009, 68, 1839–1842. [Google Scholar] [CrossRef] [PubMed]
- Ogdie, A.; Harter, L.; Shin, D.; Baker, J.; Takeshita, J.; Choi, H.K.; Jon Love, T.; Gelfand, J.M. The risk of fracture among patients with psoriatic arthritis and psoriasis: A population-based study. Ann. Rheum. Dis. 2017, 76, 882–885. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Briot, K.; Geusens, P.; Em Bultink, I.; Lems, W.; Roux, C. Inflammatory diseases and bone fragility. Osteoporos. Int. 2017, 28, 3301–3314. [Google Scholar] [CrossRef]
- Kim, J.A.; Yoon, S.; Kim, L.Y.; Kim, D.S. Towards Actualizing the Value Potential of Korea Health Insurance Review and Assessment (HIRA) Data as a Resource for Health Research: Strengths, Limitations, Applications, and Strategies for Optimal Use of HIRA Data. J. Korean Med. Sci. 2017, 32, 718–728. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Park, J.H.; Lee, J.; Yu, S.Y.; Jung, J.H.; Han, K.; Kim, D.H.; Rhee, J. Comparing proton pump inhibitors with histamin-2 receptor blockers regarding the risk of osteoporotic fractures: A nested case-control study of more than 350,000 Korean patients with GERD and peptic ulcer disease. BMC Geriatr. 2020, 20, 407. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jiao, H.; Xiao, E.; Graves, D.T. Diabetes and Its Effect on Bone and Fracture Healing. Curr. Osteoporos. Rep. 2015, 13, 327–335. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Claes, L.; Recknagel, S.; Ignatius, A. Fracture healing under healthy and inflammatory conditions. Nat. Rev. Rheumatol. 2012, 8, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Marfella, R.; Sardu, C.; D’Onofrio, N.; Prattichizzo, F.; Scisciola, L.; Messina, V.; La Grotta, L.; Balestrieri, M.L.; Maggi, P.; Napoli, C.; et al. Glycaemic control is associated with SARS-CoV-2 breakthrough infections in vaccinated patients with type 2 diabetes. Nature Commun. 2022, 13, 2318. [Google Scholar] [CrossRef] [PubMed]
- Aeberli, D.; Eser, P.; Bonel, H.; Widmer, J.; Caliezi, G.; Varisco, P.A.; Möller, B.; Villiger, P.M. Reduced trabecular bone mineral density and cortical thickness accompanied by increased outer bone circumference in metacarpal bone of rheumatoid arthritis patients: A cross-sectional study. Arthritis Res. Ther. 2010, 12, R119. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nguyen, N.D.; Eisman, J.A.; Center, J.R.; Nguyen, T.V. Risk factors for fracture in nonosteoporotic men and women. J. Clin. Endocrinol. Metab. 2007, 92, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Davey-Ranasinghe, N.; Deodhar, A. Osteoporosis and vertebral fractures in ankylosing spondylitis. Curr. Opin. Rheumatol. 2013, 25, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Tsur, A.M.; David, P.; Watad, A.; Nissan, D.; Cohen, A.D.; Amital, H. Ankylosing Spondylitis and the Risk of Hip Fractures: A Matched Cohort Study. J. Gen. Intern. Med. 2022, 37, 3283–3288. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sepehri, N.Z.; Raeisi, T.; Razi, B.; Janmohammadi, P.; Darand, M.; Alizadeh, S. The association between psoriasis and psoriatic arthritis with the risk of osteoporosis, osteopenia and bone fractures: A systematic review and meta-analysis. Int. J. Clin. Pract. 2021, 75, e14630. [Google Scholar] [CrossRef] [PubMed]
- Soare, I.; Sirbu, A.; Martin, S.; Diculescu, M.; Mateescu, B.; Tieranu, C.; Fica, S. Assessment of bone quality with trabecular bone score in patients with inflammatory bowel disease. Sci. Rep. 2021, 11, 20345. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Melton, L.J., 3rd; Leibson, C.L.; Achenbach, S.J.; Therneau, T.M.; Khosla, S. Fracture risk in type 2 diabetes: Update of a population-based study. J. Bone Miner. Res. 2008, 23, 1334–1342. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Miyoshi, A.; Kameda, H.; Nagai, S.; Nakamura, A.; Miya, A.; Takase, T.; Atsumi, T.; Miyoshi, H. Beneficial effects of switching to denosumab from bisphosphonates or selective estrogen receptor modulators in postmenopausal women with type 2 diabetes and osteopenia/osteoporosis. J. Diabetes Investig. 2021, 12, 1293–1300. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Allen, C.S.; Yeung, J.H.; Vandermeer, B.; Homik, J. Bisphosphonates for steroid-induced osteoporosis. Cochrane Database Syst. Rev. 2016, 10, Cd001347. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
| Total Population | No CD | CD | p | No UC | UC | p | No RA | RA | p | No AS | AS | p | No PsO | PsO | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of patients | 2,120,900 | 2,120,762 | 138 | 2,120,030 | 870 | 2,055,204 | 65,696 | 2,120,243 | 657 | 2,101,207 | 19,693 | |||||
| Age, years, mean ± SD | 58.47 ± 10.53 | 58.47 ± 10.53 | 57.16 ± 10.93 | 0.144 | 58.47 ± 10.53 | 59.23 ± 10.22 | 0.034 | 58.36 ± 10.54 | 61.89 ±9.8 | <0.001 | 58.47 ± 10.53 | 54.53 ± 9.98 | <0.001 | 58.46 ± 10.53 | 59.68 ± 10.32 | <0.001 |
| Age, years, n (%) | 0.535 | 0.040 | <0.001 | <0.001 | <0.001 | |||||||||||
| 40–65 | 1,495,743 (70.52) | 1,495,649 (70.52) | 94 (68.12) | 1,495,157 (70.53) | 586 (67.36) | 1,456,938 (70.89) | 38,805 (59.07) | 1,495,205 (70.52) | 538 (81.89) | 1,482,567 (70.56) | 13,176 (66.91) | |||||
| 65≤ | 625,157 (29.48) | 625,113 (29.48) | 44 (31.88) | 624,873 (29.47) | 284 (32.64) | 598,266 (29.11) | 26,891 (40.93) | 625,038 (29.48) | 119 (18.11) | 618,640 (29.44) | 6517 (33.09) | |||||
| Male sex, n (%) | 1,281,181 (60.41) | 1,281,091 (60.41) | 90 (65.22) | 0.248 | 1,280,574 (60.40) | 607 (69.77) | <0.001 | 1,257,075 (61.17) | 24,106 (36.69) | <0.001 | 1,280,645 (60.40) | 536 (81.58) | <0.001 | 1,267,810 (60.34) | 13371 (67.90) | <0.001 |
| BMI, kg/m2, Mean ± SD | 25.07 ±3.29 | 25.07 ± 3.29 | 23.78 ± 3.53 | <0.001 | 25.07 ± 3.29 | 24.4 ± 2.99 | <0.001 | 25.07 ± 3.28 | 25.1 2 ± 3.39 | <0.001 | 25.07 ± 3.29 | 25.36 ± 3.48 | 0.023 | 25.07 ± 3.29 | 25.09 ± 3.29 | 0.414 |
| Smoking, n (%) | 0.008 | <0.001 | <0.001 | <0.001 | <0.001 | |||||||||||
| Non-smoker | 1,186,168 (55.93) | 1,186,096 (55.93) | 72 (52.17) | 1,185,731 (55.93) | 437 (50.23) | 1,138,456 (55.39) | 47,712 (72.63) | 1,185,913 (55.93) | 255 (38.81) | 1,176,674 (56.00) | 9494 (48.21) | |||||
| Former smoker | 417,133 (19.67) | 417,092 (19.67) | 41 (29.71) | 4,168,02 (19.66) | 331 (38.05) | 408,065 (19.86) | 9068 (13.80) | 416,951 (19.67) | 182 (27.70) | 412,319 (19.62) | 4814 (24.45) | |||||
| Current smoker | 517,599 (24.4) | 517,574 (24.41) | 25 (18.12) | 517,497 (24.41) | 102 (11.72) | 508,683 (24.75) | 8916 (13.57) | 517,379 (24.40) | 220 (33.49) | 512,214 (24.38) | 5385 (27.34) | |||||
| Alcohol consumption, n (%) | 0.046 | <0.001 | <0.001 | 0.111 | 0.059 | |||||||||||
| None | 1,228,912 (57.94) | 1,228,819 (57.94) | 93 (67.39) | 1,228,311 (57.94) | 601 (69.08) | 1,179,667 (57.40) | 49,245 (74.96) | 1,228,556 (57.94) | 356 (54.19) | 1,217,340 (57.94) | 11,572 (58.76) | |||||
| Mild drinker | 686,373 (32.36) | 686,335 (32.36) | 38 (27.54) | 686,155 (32.37) | 218 (25.06) | 673,203 (32.76) | 13,170 (20.05) | 686,136 (32.36) | 237 (36.07) | 680,107 (32.37) | 6266 (31.82) | |||||
| Heavy drinker | 205,615 (9.69) | 205,608 (9.70) | 7 (5.07) | 205,564 (9.70) | 51 (5.86) | 202,334 (9.84) | 3281 (4.99) | 205,551 (9.69) | 64 (9.74) | 203,760 (9.70) | 1855 (9.42) | |||||
| Regular physical activity, n (%) | 458,444 (21.62) | 458,416 (21.62) | 28 (20.29) | 0.705 | 458,247 (21.62) | 197 (22.64) | 0.461 | 445,442 (21.67) | 13,002 (19.79) | <0.001 | 458,324 (21.62) | 120 (18.26) | 0.037 | 454,077 (21.61) | 4367 (22.18) | 0.055 |
| Low income, n (%) | 492,625 (23.23) | 492,595 (23.23) | 30 (21.74) | 0.679 | 492,461 (23.23) | 164 (18.85) | 0.0022 | 476,711 (23.20) | 15,914 (24.22) | <0.001 | 492,491 (23.23) | 134 (20.40) | 0.086 | 487,903 (23.22) | 4722 (23.98) | 0.012 |
| Rural residence, n (%) | 1,182,177 (55.74) | 1,182,096 (55.74) | 81 (58.70) | 0.484 | 1181725 (55.74) | 452 (51.95) | 0.025 | 1,143,587 (55.64) | 38,590 (58.74) | <0.001 | 1,181,807 (55.74) | 370 (56.32) | 0.766 | 1,170,965 (55.73) | 11,212 (56.93) | <0.001 |
| Hypertension, n (%) | 1,238,054 (58.37) | 1,237,983 (58.37) | 71 (51.45) | 0.099 | 1,237,624 (58.38) | 430 (49.43) | <0.001 | 1,195,358 (58.16) | 42,696 (64.99) | <0.001 | 1,237,659 (58.37) | 395 (60.12) | 0.363 | 1,225,861 (58.34) | 12,193 (61.92) | <0.001 |
| Dyslipidemia, n (%) | 912,871 (43.04) | 912,829 (43.04) | 42 (30.43) | 0.003 | 912,522 (43.04) | 349 (40.11) | 0.081 | 878,388 (42.74) | 34,483 (52.49) | <0.001 | 912,589 (43.04) | 282 (42.92) | 0.951 | 903,374 (42.99) | 9497 (48.23) | <0.001 |
| CKD, n (%) | 242,950 (11.46) | 242,929 (11.45) | 21 (15.22) | 0.165 | 242,863 (11.46) | 87 (10.00) | 0.178 | 232,954 (11.33) | 9996 (15.22) | <0.001 | 242,888 (11.46) | 62 (9.44) | 0.104 | 240,512 (11.45) | 2438 (12.38) | <0.001 |
| Stroke, n (%) | 103,532 (4.88) | 103,525 (4.88) | 7 (5.07) | 0.917 | 103,490 (4.88) | 42 (4.83) | 0.941 | 98,274 (4.78) | 5258 (8.00) | <0.001 | 103,505 (4.88) | 27 (4.11) | 0.358 | 102,231 (4.87) | 1301 (6.61) | <0.001 |
| Anemia, n (%) | 62,933 (2.97) | 62,921 (2.97) | 12 (8.70) | <0.001 | 62,886 (2.97) | 47 (5.40) | <0.001 | 58,900 (2.87) | 4033 (6.14) | <0.001 | 62,903 (2.97) | 30 (4.57) | 0.016 | 62,221 (2.96) | 712 (3.62) | <0.001 |
| Osteoporosis, n (%) | 196,123 (9.25) | 196,103 (9.25) | 20 (14.49) | 0.033 | 196,022 (9.25) | 101 (11.61) | 0.016 | 178,075 (8.66) | 18,048 (27.47) | <0.001 | 196,014 (9.24) | 109 (16.59) | <0.001 | 194177 (9.24) | 1946 (9.88) | 0.002 |
| Use of insulin, n (%) | 194,571 (9.17) | 194,546 (9.17) | 25 (18.12) | <0.001 | 194,441 (9.17) | 130 (14.94) | <0.001 | 184,032 (8.95) | 10,539 (16.04) | <0.001 | 194,493 (9.17) | 78 (11.87) | 0.017 | 192,037 (9.14) | 2534 (12.87) | <0.001 |
| Number of oral hypoglycemic agents used 3, n (%) | 323,566 (15.26) | 323,551 (15.26) | 15 (10.87) | 0.152 | 323,443 (15.26) | 123 (14.14) | 0.359 | 311,205 (15.14) | 12,361 (18.82) | <0.001 | 323,467 (15.26) | 99 (15.07) | 0.894 | 320,182 (15.24) | 3384 (17.18) | <0.001 |
| Duration of type 2 diabetes over 5 years, n (%) | 676,322 (31.89) | 676,287 (31.89) | 35 (25.36) | 0.100 | 676,043 (31.89) | 279 (32.07) | 0.909 | 652,060 (31.73) | 24,262 (36.93) | <0.001 | 676,111 (31.89) | 211 (32.12) | 0.901 | 669,594 (31.87) | 6728 (34.16) | <0.001 |
| No. of Participants | No. of Events | Total no. of Person-Years of Follow up | IR (Per 1000 Person-Years) | Model 1 HR (95% CI) | Model 2 HR (95% CI) | Model 3 HR (95% CI) | Model 4 HR (95% CI) | Model 5 HR (95% CI) | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall fractures | ||||||||||
| CD | ||||||||||
| No | 2,120,762 | 219,822 | 13,865,630.35 | 15.85 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.398 |
| Yes | 138 | 17 | 890.21 | 19.10 | 1.23 (0.77, 1.97) | 1.28 (0.80, 2.05) | 1.30 (0.81, 2.09) | 1.27 (0.79, 2.04) | 1.28 (0.76, 1.97) | |
| UC | ||||||||||
| No | 2,120,030 | 219,725 | 13,860,881.72 | 15.85 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.004 |
| Yes | 870 | 114 | 5638.84 | 20.22 | 1.28 (1.06, 1.53) | 1.33 (1.10, 1.59) | 1.36 (1.13, 1.64) | 1.34 (1.12, 1.62) | 1.31 (1.09, 1.57) | |
| RA | ||||||||||
| No | 2,055,204 | 209,451 | 13,454,973.84 | 15.57 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 65,696 | 10,388 | 411,546.72 | 25.24 | 1.63 (1.59, 1.66) | 1.23 (1.21, 1.26) | 1.24 (1.21, 1.26) | 1.24 (1.21, 1.26) | 1.19 (1.17, 1.22) | |
| AS | ||||||||||
| No | 2,120,243 | 219,775 | 13,862,299.67 | 15.85 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.028 |
| Yes | 657 | 64 | 4220.90 | 15.16 | 0.96 (0.75, 1.22) | 1.35 (1.06, 1.73) | 1.36 (1.06, 1.73) | 1.36 (1.07, 1.74) | 1.32 (1.03, 1.68) | |
| PsO | ||||||||||
| No | 2,101,207 | 217,572 | 1,374,0471.17 | 15.83 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 19,693 | 2267 | 126,049.39 | 17.99 | 1.14 (1.09, 1.19) | 1.16 (1.12, 1.2) | 1.16 (1.11, 1.21) | 1.16 (1.12, 1.21) | 1.14 (1.10, 1.19) | |
| Number of IMIDs | ||||||||||
| 0 | 2,035,002 | 207,159 | 13,325,369.93 | 15.55 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| 1 | 84,748 | 12,511 | 533,993.80 | 23.43 | 1.51 (1.48, 1.54) | 1.22 (1.20, 1.25) | 1.22 (1.20, 1.25) | 1.22 (1.20, 1.25) | 1.18 (1.16, 1.21) | |
| ≥2 | 1150 | 169 | 7156.83 | 23.61 | 1.52 (1.31, 1.77) | 1.36 (1.17, 1.58) | 1.36 (1.17, 1.58) | 1.36 (1.17, 1.58) | 1.29 (1.11, 1.50) | |
| No. of Participants | No. of Events | Total No. of Person-Years of Follow up | IR (Per 1000 Person-Years) | Model 1 HR (95% CI) | Model 2 HR (95% CI) | Model 3 HR (95% CI) | Model 4 HR (95% CI) | Model 5 HR (95% CI) | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Osteoporotic fracture | ||||||||||
| CD | ||||||||||
| No | 2,120,762 | 113,118 | 13,865,630.35 | 8.16 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.193 |
| Yes | 138 | 11 | 890.21 | 12.36 | 1.52 (0.85, 2.75) | 1.61 (0.89, 2.90) | 1.61 (0.89, 2.91) | 1.58 (0.87, 2.85) | 1.48 (0.82, 2.67) | |
| UC | ||||||||||
| No | 2,120,030 | 113,072 | 13,860,881.72 | 8.16 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.026 |
| Yes | 870 | 57 | 5638.84 | 10.11 | 1.24 (0.96, 1.61) | 1.41 (1.09, 1.83) | 1.42 (1.09, 1.84) | 1.39 (1.08, 1.81) | 1.34 (1.04, 1.74) | |
| RA | ||||||||||
| No | 2,055,204 | 105,778 | 13,454,973.84 | 7.86 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 65,696 | 7351 | 411,546.72 | 17.86 | 2.29 (2.23, 2.34) | 1.45 (1.41, 1.48) | 1.45 (1.41, 1.48) | 1.45 (1.41, 1.48) | 1.38 (1.35, 1.41) | |
| AS | ||||||||||
| No | 2,120,243 | 113,093 | 13,862,299.67 | 8.16 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 657 | 36 | 4220.90 | 8.53 | 1.05 (0.76, 1.45) | 2.05 (1.48, 2.84) | 2.04 (1.47, 2.83) | 2.05 (1.48, 2.84) | 1.95 (1.41, 2.70) | |
| PsO | ||||||||||
| No | 2,101,207 | 111,976 | 137,40471.17 | 8.15 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 19,693 | 1153 | 126,049.39 | 9.15 | 1.13 (1.06, 1.19) | 1.25 (1.18, 1.32) | 1.25 (1.18, 1.32) | 1.25 (1.18, 1.32) | 1.22 (1.15, 1.29) | |
| Number of IMIDs | ||||||||||
| 0 | 2,035,002 | 104,629 | 13,325,369.93 | 7.85 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| 1 | 84,748 | 8392 | 533,993.80 | 15.72 | 2.01 (1.97, 2.06) | 1.42 (1.39, 1.45) | 1.42 (1.39, 1.45) | 1.42 (1.39, 1.45) | 1.36 (1.33, 1.39) | |
| ≥2 | 1150 | 108 | 7156.83 | 15.09 | 1.94 (1.61, 2.34) | 1.63 (1.35, 1.97) | 1.63 (1.35, 1.97) | 1.62 (1.34, 1.96) | 1.54 (1.26, 1.84) | |
| Non-osteoporotic fracture | ||||||||||
| CD | ||||||||||
| No | 2,120,762 | 106,704 | 13,865,630.35 | 7.70 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.754 |
| Yes | 138 | 6 | 890.21 | 6.74 | 0.88 (0.40, 1.96) | 0.89 (0.40, 1.98) | 0.91 (0.41, 2.03) | 0.89 (0.40, 1.98) | 0.88 (0.40, 1.96) | |
| UC | ||||||||||
| No | 2,120,030 | 106,653 | 13,860,881.72 | 7.69 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.052 |
| Yes | 870 | 57 | 5638.84 | 10.11 | 1.32 (1.01, 1.71) | 1.29 (0.99, 1.67) | 1.33 (1.02, 1.72) | 1.32 (1.01, 1.71) | 1.29 (1.00, 1.68) | |
| RA | ||||||||||
| No | 2,055,204 | 103,673 | 13,454,973.84 | 7.71 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 65696 | 3037 | 411,546.72 | 7.38 | 0.96 (0.92, 0.99) | 0.93 (0.90, 0.97) | 0.94 (0.90, 0.97) | 0.94 (0.90, 0.97) | 0.92 (0.88, 0.95) | |
| AS | ||||||||||
| No | 2,120,243 | 106,682 | 13,862,299.67 | 7.70 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.534 |
| Yes | 657 | 28 | 4220.90 | 6.63 | 0.87 (0.60, 1.26) | 0.90 (0.62, 1.30) | 0.90 (0.62, 1.31) | 0.91 (0.63, 1.31) | 0.90 (0.61, 1.29) | |
| PsO | ||||||||||
| No | 2,101,207 | 105,596 | 13,740,471.17 | 7.69 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 19,693 | 1114 | 126,049.39 | 8.84 | 1.15 (1.08, 1.22) | 1.12 (1.06, 1.19) | 1.12 (1.06, 1.19) | 1.13 (1.06, 1.20) | 1.11 (1.05, 1.18) | |
| Number of IMIDs | ||||||||||
| 0 | 2,035,002 | 102,530 | 13,325,369.93 | 7.69 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.050 |
| 1 | 84,748 | 4119 | 533,993.80 | 7.71 | 1 (0.97, 1.03) | 0.98 (0.95, 1.01) | 0.98 (0.95, 1.01) | 0.98 (0.95, 1.01) | 0.96 (0.93, 0.99) | |
| ≥2 | 1150 | 61 | 7156.83 | 8.52 | 1.11 (0.86, 1.43) | 1.08 (0.84, 1.39) | 1.09 (0.85, 1.40) | 1.09 (0.85, 1.40) | 1.06 (0.82, 1.36) | |
| No. of Participants | No. of Events | Total No. of Person-Years of Follow up | IR (per 1000 Person-Years) | Model 1 HR (95% CI) | Model 2 HR (95% CI) | Model 3 HR (95% CI) | Model 4 HR (95% CI) | Model 5 HR (95% CI) | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Vertebral fracture | ||||||||||
| CD | ||||||||||
| No | 2,120,762 | 65,675 | 14,416,786.45 | 4.56 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.531 |
| Yes | 138 | 3 | 931.72 | 3.22 | 0.75 (0.25, 2.24) | 0.74 (0.24,2.28) | 0.74 (0.24, 2.29) | 0.73 (0.24, 2.27) | 0.70 (0.23, 2.16) | |
| UC | ||||||||||
| No | 2,120,030 | 65,642 | 1,441,1796.77 | 4.55 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.047 |
| Yes | 870 | 36 | 5921.40 | 6.08 | 1.33 (0.96, 1.85) | 1.42 (1.02, 1.97) | 1.44 (1.04, 2.00) | 1.43 (1.03, 1.99) | 1.39 (1.00, 1.93) | |
| RA | ||||||||||
| No | 2,055,204 | 61,953 | 13,982,052.26 | 4.43 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 65,696 | 3725 | 435,665.90 | 8.55 | 1.93 (1.87, 2.00) | 1.35 (1.31, 1.39) | 1.35 (1.31, 1.40) | 1.35 (1.31, 1.40) | 1.30 (1.26, 1.34) | |
| AS | ||||||||||
| No | 2,120,243 | 65,652 | 14,413,340.35 | 4.55 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.001 |
| Yes | 657 | 26 | 4377.81 | 5.94 | 1.31 (0.89, 1.92) | 2.19 (1.49, 3.21) | 2.18 (1.49, 3.21) | 2.19 (1.49, 3.21) | 2.11 (1.44, 3.11) | |
| PsO | ||||||||||
| No | 2,101,207 | 64,926 | 14,286,224.00 | 4.54 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 19,693 | 752 | 131,494.16 | 5.72 | 1.26 (1.17, 1.36) | 1.31 (1.22, 1.41) | 1.31 (1.22, 1.41) | 1.31 (1.22, 1.41) | 1.29 (1.20, 1.38) | |
| Number of IMIDs | ||||||||||
| 0 | 2,035,002 | 61,197 | 13,846,883.08 | 4.42 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| 1 | 84,748 | 4420 | 563,318.69 | 7.85 | 1.78 (1.73, 1.83) | 1.35 (1.31, 1.39) | 1.35 (1.31, 1.39) | 1.35 (1.31, 1.39) | 1.30 (1.26, 1.34) | |
| ≥2 | 1150 | 61 | 7516.40 | 8.12 | 1.85 (1.44, 2.37) | 1.60 (1.24, 2.05) | 1.59 (1.24, 2.05) | 1.59 (1.24, 2.05) | 1.51 (1.18, 1.94) | |
| Hip fracture | ||||||||||
| CD | ||||||||||
| No | 2,120,762 | 26,086 | 14,566,878.07 | 1.79 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.316 |
| Yes | 138 | 3 | 939.61 | 3.19 | 1.81 (0.59, 5.57) | 2.01 (0.65, 6.22) | 2.04 (0.66, 6.34) | 1.83 (0.59, 5.66) | 1.78 (0.58, 5.53) | |
| UC | ||||||||||
| No | 2,120,030 | 26,077 | 14,561,834.62 | 1.79 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.687 |
| Yes | 870 | 12 | 5983.06 | 2.01 | 1.12 (0.64, 1.98) | 1.17 (0.66, 2.05) | 1.22 (0.69, 2.14) | 1.18 (0.67, 2.08) | 1.12 (0.64, 1.98) | |
| RA | ||||||||||
| No | 2,055,204 | 24,684 | 14,123,511.73 | 1.75 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| Yes | 65,696 | 1405 | 444,305.95 | 3.16 | 1.82 (1.72, 1.92) | 1.26 (1.20, 1.33) | 1.27 (1.20, 1.34) | 1.27 (1.21, 1.34) | 1.19 (1.13, 1.26) | |
| AS | ||||||||||
| No | 2,120,243 | 26,080 | 14,563,367.88 | 1.79 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.030 |
| Yes | 657 | 9 | 4449.80 | 2.02 | 1.14 (0.60, 2.19) | 2.11 (1.10, 4.05) | 2.11 (1.10, 4.05) | 2.14 (1.12, 4.12) | 2.06 (1.07, 3.96) | |
| PsO | ||||||||||
| No | 2,101,207 | 25,801 | 14,434,581.39 | 1.79 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 0.011 |
| Yes | 19,693 | 288 | 133,236.29 | 2.16 | 1.21 (1.08, 1.36) | 1.21 (1.08, 1.36) | 1.20 (1.07, 1.35) | 1.21 (1.08, 1.36) | 1.16 (1.03, 1.31) | |
| Number of IMIDs | ||||||||||
| 0 | 2,035,002 | 24,395 | 13,986,649.78 | 1.74 | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | 1 (Ref.) | <0.001 |
| 1 | 84,748 | 1672 | 573,459.70 | 2.92 | 1.68 (1.60, 1.76) | 1.26 (1.20, 1.32) | 1.26 (1.20, 1.33) | 1.27 (1.21, 1.33) | 1.19 (1.13, 1.25) | |
| ≥2 | 1150 | 22 | 7708.20 | 2.85 | 1.65 (1.09, 2.50) | 1.43 (0.94, 2.17) | 1.41 (0.93, 2.14) | 1.41 (0.93, 2.14) | 1.31 (0.86, 1.98) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Kwon, O.C.; Kim, R.; Kim, J.H.; Kim, M.-J.; Park, M.-C.; Kim, J.-H.; Youn, Y.H.; Park, H.; Han, K.; et al. Association of Immune-Mediated Inflammatory Diseases and Fracture Risk in Patients with Type 2 Diabetes: A Nationwide Population-Based Study. J. Clin. Med. 2025, 14, 795. https://doi.org/10.3390/jcm14030795
Kim Y, Kwon OC, Kim R, Kim JH, Kim M-J, Park M-C, Kim J-H, Youn YH, Park H, Han K, et al. Association of Immune-Mediated Inflammatory Diseases and Fracture Risk in Patients with Type 2 Diabetes: A Nationwide Population-Based Study. Journal of Clinical Medicine. 2025; 14(3):795. https://doi.org/10.3390/jcm14030795
Chicago/Turabian StyleKim, Yuna, Oh Chan Kwon, Ryul Kim, Jong Hoon Kim, Min-Jae Kim, Min-Chan Park, Jie-Hyun Kim, Young Hoon Youn, Hyojin Park, Kyungdo Han, and et al. 2025. "Association of Immune-Mediated Inflammatory Diseases and Fracture Risk in Patients with Type 2 Diabetes: A Nationwide Population-Based Study" Journal of Clinical Medicine 14, no. 3: 795. https://doi.org/10.3390/jcm14030795
APA StyleKim, Y., Kwon, O. C., Kim, R., Kim, J. H., Kim, M.-J., Park, M.-C., Kim, J.-H., Youn, Y. H., Park, H., Han, K., & Chun, J. (2025). Association of Immune-Mediated Inflammatory Diseases and Fracture Risk in Patients with Type 2 Diabetes: A Nationwide Population-Based Study. Journal of Clinical Medicine, 14(3), 795. https://doi.org/10.3390/jcm14030795