
“Add More Arrows to Your Quiver”: The Role of Adding Another Chemotherapy Drug to Fluoropyrimidine and Long Term Radiotherapy in Locally Advanced Rectal Cancer: A Systematic Review and Meta-Analysis

 ,
, 
 , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
- We estimated the pooled actuarial probabilities of disease-free survival, overall survival, local recurrence and distant metastases in LARC patients treated in these RCTs;
- We analysed variabilities in OS by considering the heterogeneity between studies;
- We identified factors associated with the risk of recurrence and survival.
2. Materials and Methods
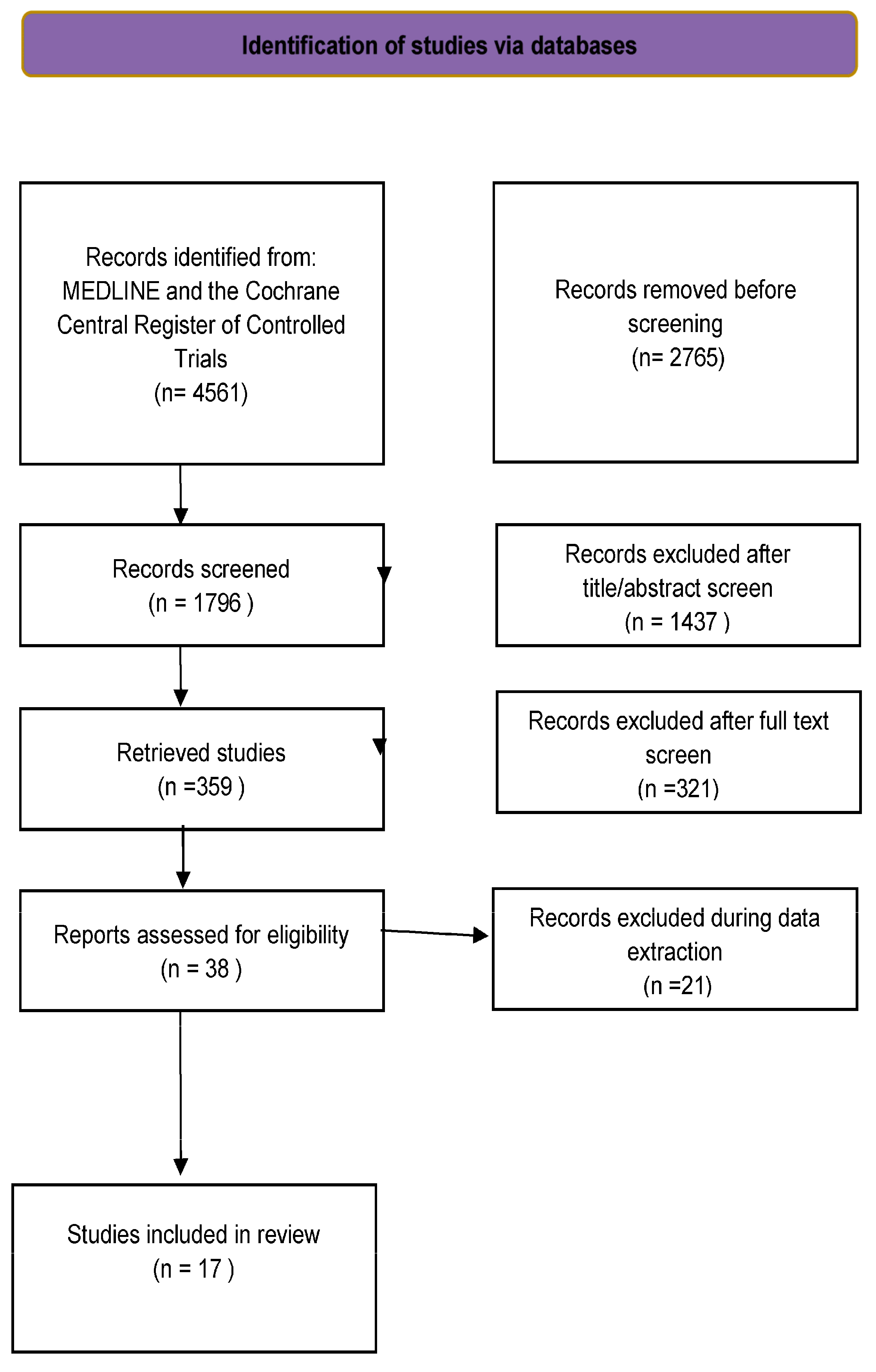
2.1. Selection of Trials
2.2. Review of Studies
2.3. Statistical Analyses
3. Results
3.1. Characteristics of the Studies
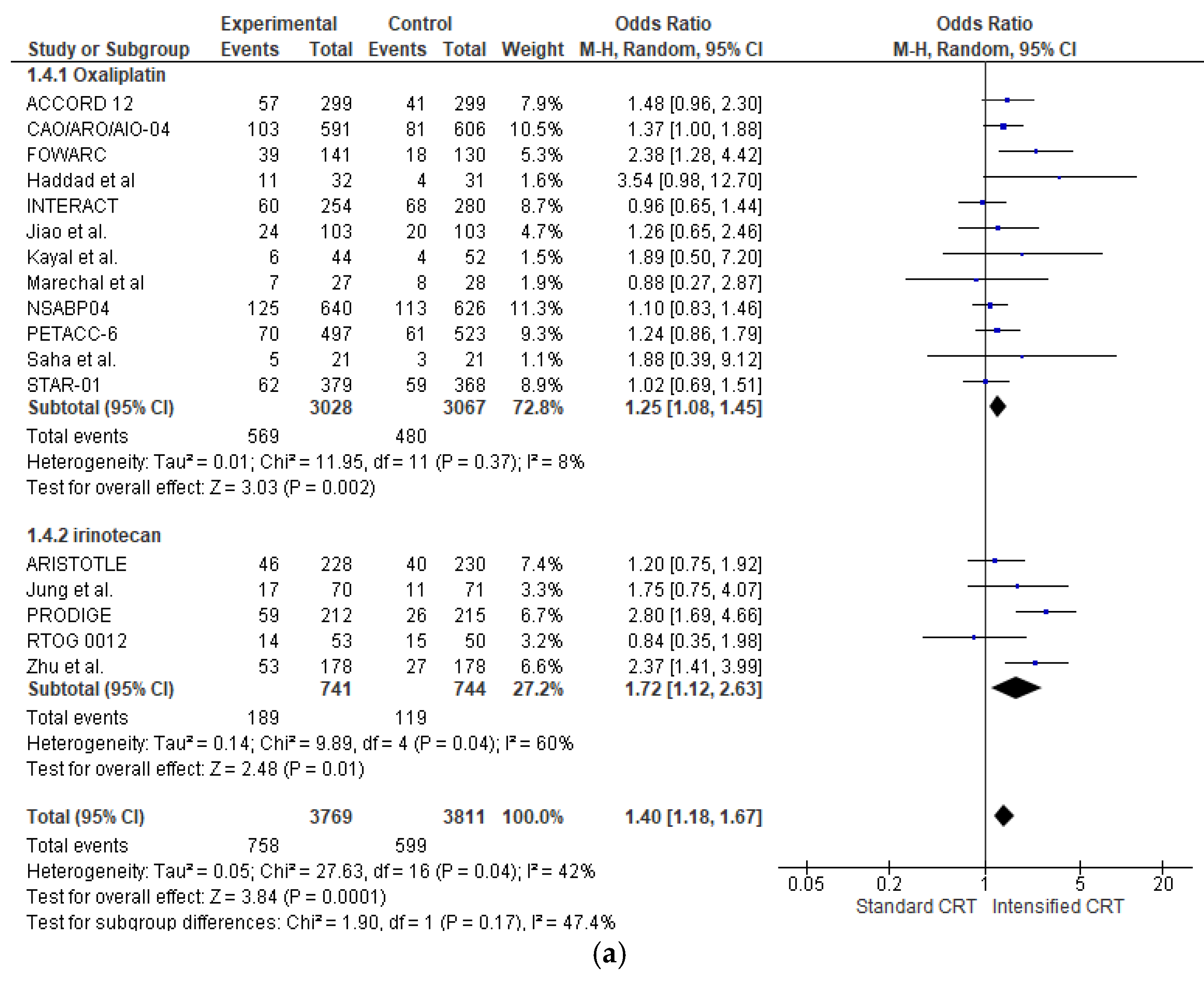
3.2. Pathological Response
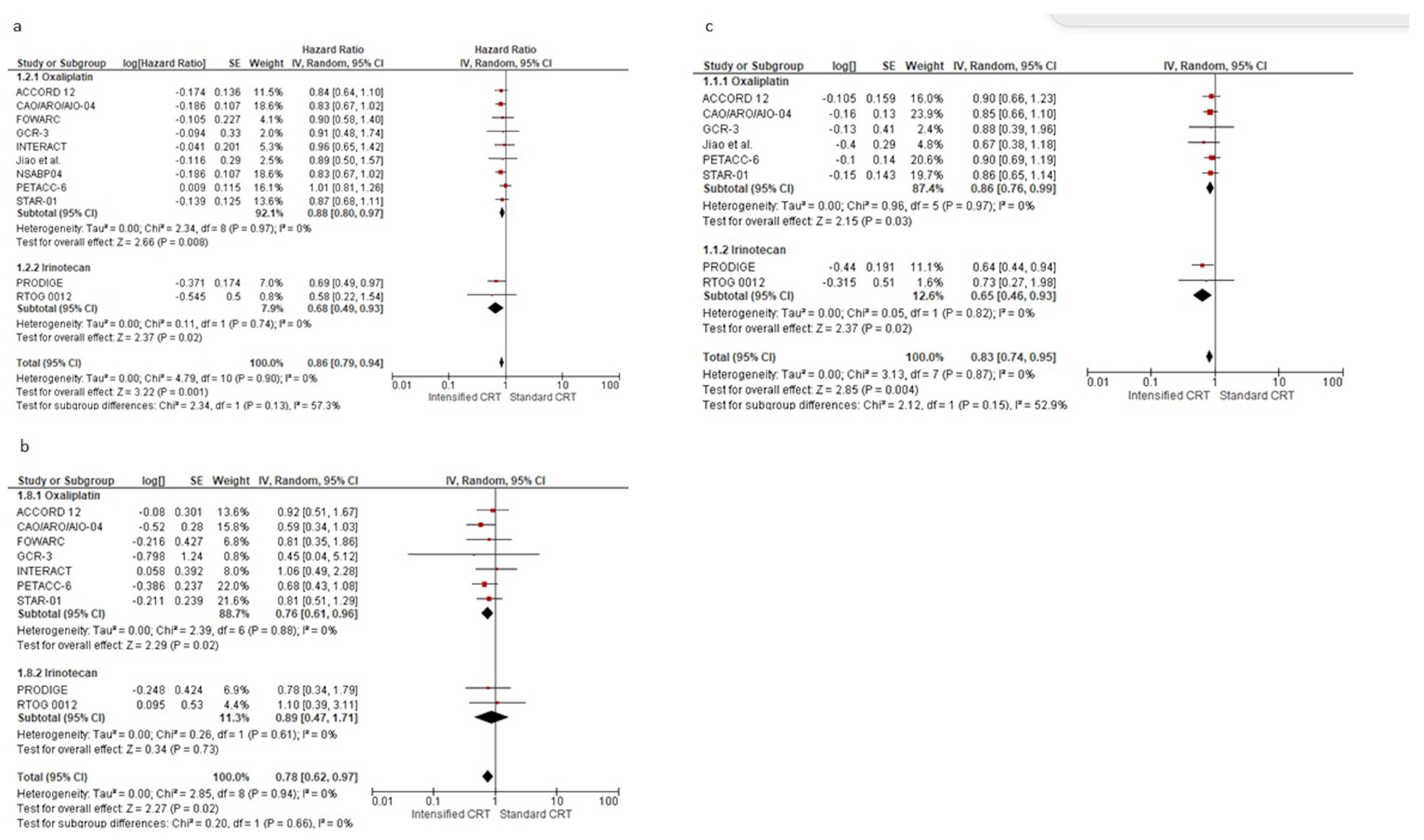
3.3. Disease-Free Survival
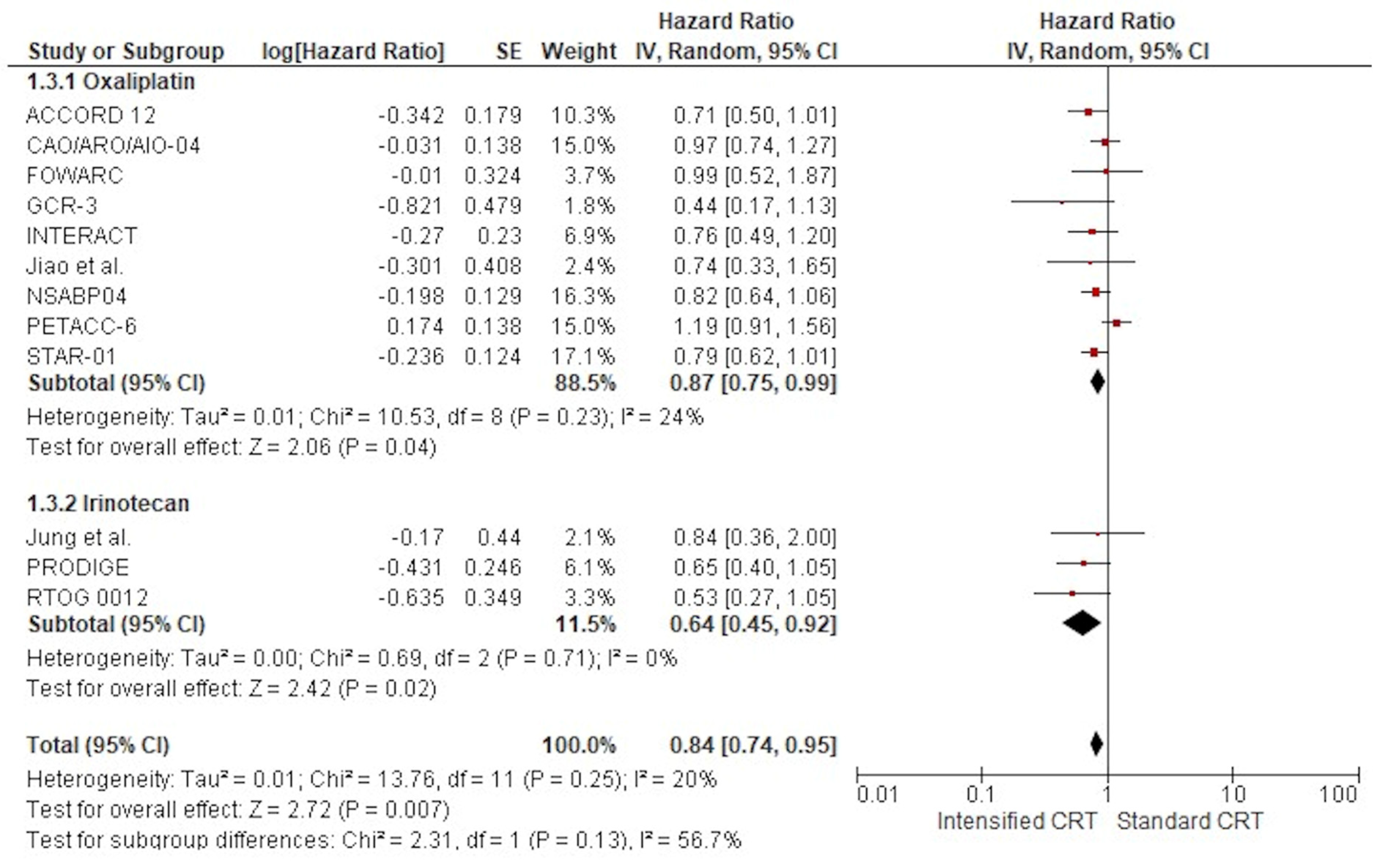
3.4. Survival
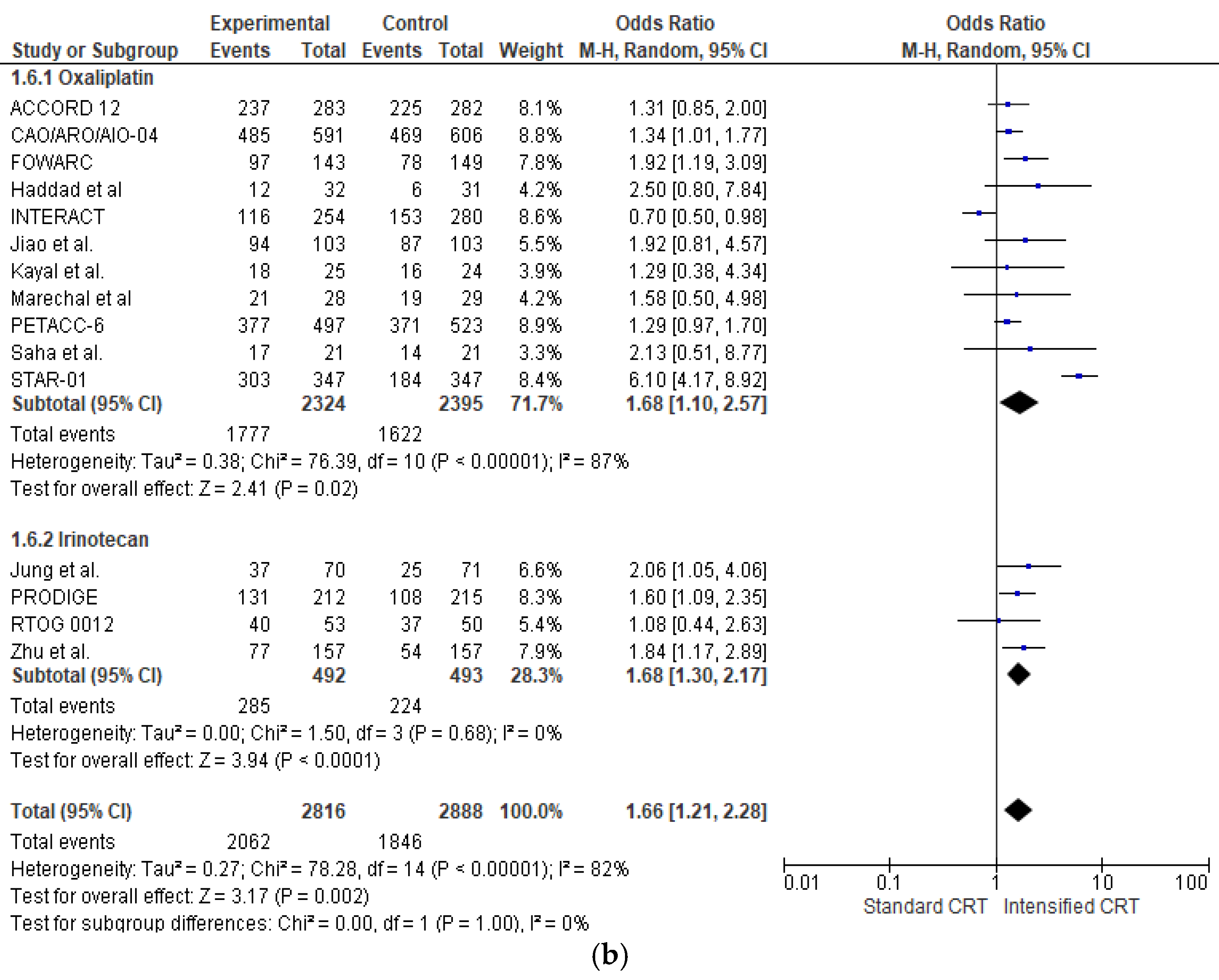
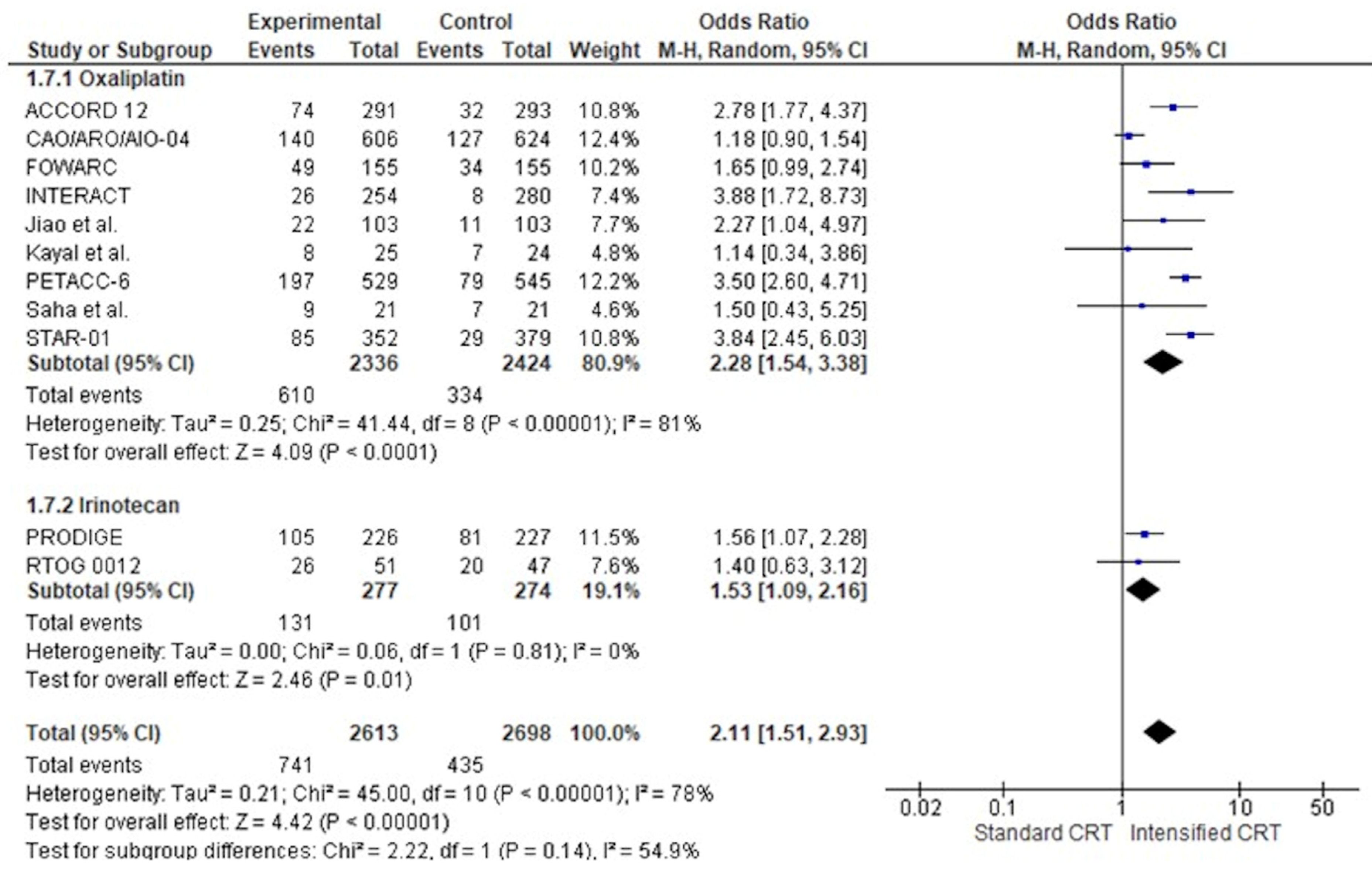
3.5. Toxicity
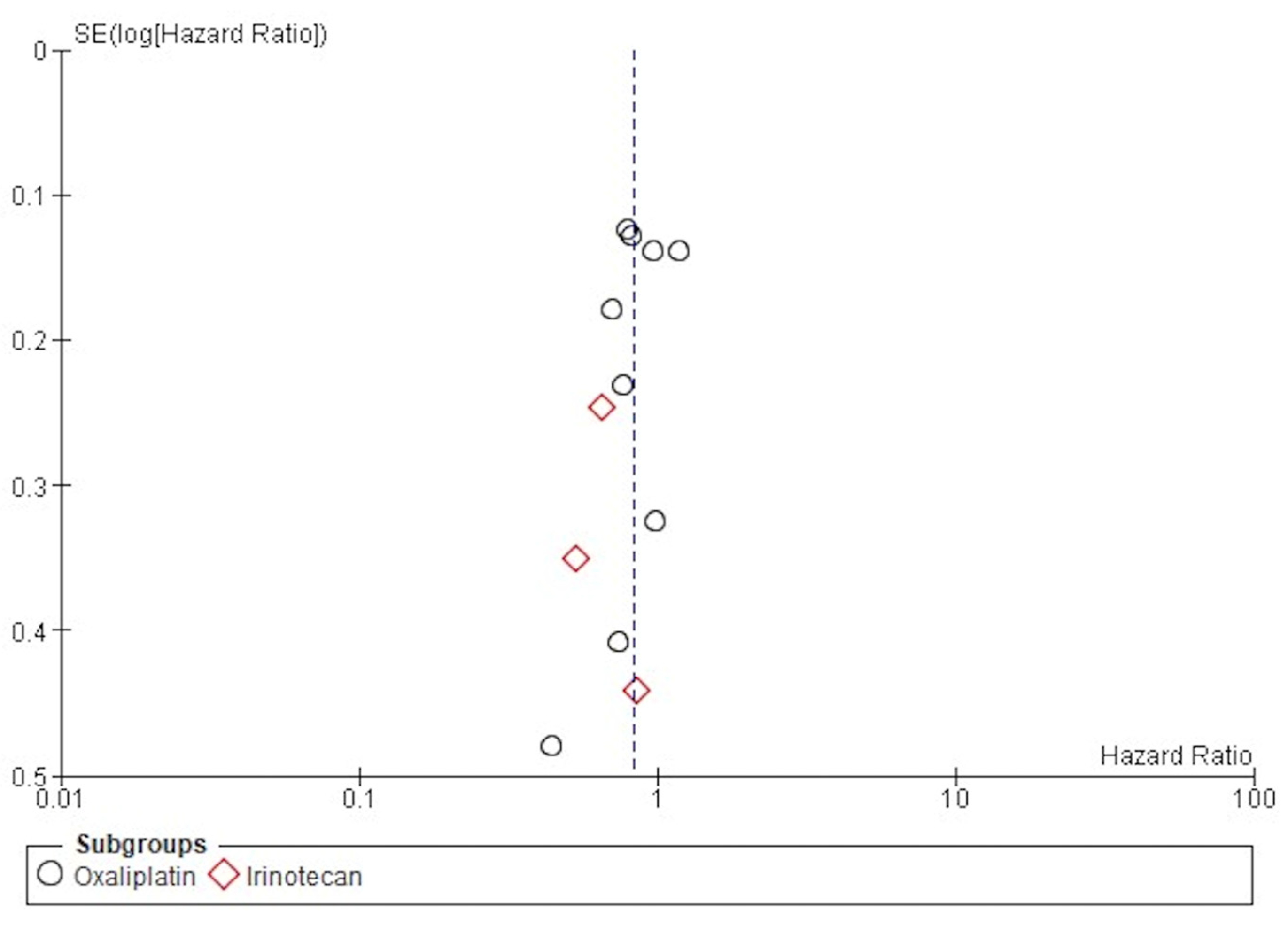
3.6. Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Morgan, E.; Arnold, M.; Gini, A.; Lorenzoni, V.; Cabasag, C.J.; Laversanne, M.; Vignat, J.; Ferlay, J.; Murphy, N.; Bray, F. Global burden of colorectal cancer in 2020 and 2040: Incidence and mortality estimates from GLOBOCAN. Gut 2023, 72, 338–344. [Google Scholar] [CrossRef]
- Cammà, C.; Giunta, M.; Fiorica, F.; Pagliaro, L.; Craxì, A.; Cottone, M. Preoperative radiotherapy for resectable rectal cancer: A meta-analysis. JAMA 2000, 284, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Heald, R.J.; Ryall, R.D. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986, 1, 1479–1482. [Google Scholar] [CrossRef] [PubMed]
- van Gijn, W.; Marijnen, C.A.; Nagtegaal, I.D.; Kranenbarg, E.M.; Putter, H.; Wiggers, T.; Rutten, H.J.; Påhlman, L.; Glimelius, B.; van de Velde, C.J. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011, 12, 575–582. [Google Scholar] [CrossRef]
- Kapiteijn, E.; Marijnen, C.A.; Nagtegaal, I.D.; Putter, H.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Pahlman, L.; Glimelius, B.; van Krieken, J.H.; et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 2001, 345, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Fiorica, F.; Cartei, F.; Carau, B.; Berretta, S.; Spartà, D.; Tirelli, U.; Santangelo, A.; Maugeri, D.; Luca, S.; Leotta, C.; et al. Adjuvant radiotherapy on older and oldest elderly rectal cancer patients. Arch. Gerontol. Geriatr. 2009, 49, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.D.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef] [PubMed]
- Fiorica, F.; Cartei, F.; Licata, A.; Enea, M.; Ursino, S.; Colosimo, C.; Cammà, C. Can chemotherapy concomitantly delivered with radiotherapy improve survival of patients with resectable rectal cancer? A meta-analysis of literature data. Cancer Treat. Rev. 2010, 36, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; the PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 2015, 349, 7647. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Gérard, J.P.; Azria, D.; Gourgou-Bourgade, S.; Martel-Laffay, I.; Hennequin, C.; Etienne, P.L.; Vendrely, V.; François, E.; de La Roche, G.; Bouché, O.; et al. Comparison of two neoadjuvant chemoradiotherapy regimens for locally advanced rectal cancer: Results of the phase III trial ACCORD 12/0405-Prodige 2. J. Clin. Oncol. 2010, 28, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Gérard, J.P.; Azria, D.; Gourgou-Bourgade, S.; Martel-Lafay, I.; Hennequin, C.; Etienne, P.L.; Vendrely, V.; François, E.; de La Roche, G.; Bouché, O.; et al. Clinical outcome of the ACCORD 12/0405 PRODIGE 2 randomized trial in rectal cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 4558–4565. [Google Scholar] [CrossRef]
- Rödel, C.; Liersch, T.; Becker, H.; Fietkau, R.; Hohenberger, W.; Hothorn, T.; Graeven, U.; Arnold, D.; Lang-Welzenbach, M.; Raab, H.R.; et al. Preoperative chemoradiotherapy and postoperative chemotherapy with fluorouracil and oxaliplatin versus fluorouracil alone in locally advanced rectal cancer: Initial results of the German CAO/ARO/AIO-04 randomised phase 3 trial. Lancet Oncol. 2012, 13, 679–687. [Google Scholar] [CrossRef]
- Maréchal, R.; Vos, B.; Polus, M.; Delaunoit, T.; Peeters, M.; Demetter, P.; Hendlisz, A.; Demols, A.; Franchimont, D.; Verset, G.; et al. Short course chemotherapy followed by concomitant chemoradiotherapy and surgery in locally advanced rectal cancer: A randomized multicentric phase II study. Ann. Oncol. 2012, 23, 1525–1530. [Google Scholar] [CrossRef]
- Schmoll, H.-J.; Stein, A.; Van Cutsem, E.; Price, T.; Hofheinz, R.D.; Nordlinger, B.; Daisne, J.-F.; Janssens, J.; Brenner, B.; Reinel, H.; et al. Pre- and Postoperative Capecitabine Without or with Oxaliplatin in Locally Advanced Rectal Cancer: PETACC 6 Trial by EORTC GITCG and ROG, AIO, AGITG, BGDO, and FFCD. J. Clin. Oncol. 2021, 39, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Aschele, C.; Cionini, L.; Lonardi, S.; Pinto, C.; Cordio, S.; Rosati, G.; Artale, S.; Tagliagambe, A.; Ambrosini, G.; Rosetti, P.; et al. Primary Tumor Response to Preoperative Chemoradiation with or Without Oxaliplatin in Locally Advanced Rectal Cancer: Pathologic Results of the STAR-01 Randomized Phase III Trial. J. Clin. Oncol. 2011, 29, 2773–2780. [Google Scholar] [CrossRef]
- Aschele, C.; Lonardi, S.; Cionini, L.; Pinto, C.; Cordio, S.S.; Rosati, G.; Bianchi, A.S.; Tagliagambe, A.; Frisinghelli, M.; Zagonel, V.; et al. Final Results of STAR-01: A Randomized Phase III Trial Comparing Preoperative Chemoradiation with or without Oxaliplatin in Locally Advanced Rectal Cancer. J. Clin. Oncol. 2016, 34, 3521. [Google Scholar] [CrossRef]
- Valentini, V.; Gambacorta, M.A.; Cellini, F.; Aristei, C.; Coco, C.; Barbaro, B.; Alfieri, S.; D’Ugo, D.; Persiani, R.; Deodato, F.; et al. The INTERACT Trial: Long-term results of a randomised trial on preoperative capecitabine-based radiochemotherapy intensified by concomitant boost or oxaliplatin, for cT2 (distal)–c3 rectal cancer. Radiother. Oncol. 2019, 134, 110–118. [Google Scholar] [CrossRef]
- Sebag-Montefiore, D.; Adams, R.; Gollins, S.; Samuel, L.M.; Glynne-Jones, R.; Harte, R.; West, N.; Quirke, P.; Myint, A.S.; Bach, S.P.; et al. ARISTOTLE: A phase III trial comparing concurrent capecitabine with capecitabine and irinotecan (Ir) chemoradiation as preoperative treatment for MRI-defined locally advanced rectal cancer (LARC). J. Clin. Oncol. 2020, 38, 4101. [Google Scholar] [CrossRef]
- Conroy, T.; Bosset, J.-F.; Etienne, P.-L.; Rio, E.; François, E.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Chi, P.; Lan, P.; Wang, L.; Chen, W.; Cui, L.; Chen, D.; Cao, J.; Wei, H.; Peng, X.; et al. Modified FOLFOX6 with or Without Radiation Versus Fluorouracil and Leucovorin with Radiation in Neoadjuvant Treatment of Locally Advanced Rectal Cancer: Initial Results of the Chinese FOWARC Multicenter, Open-Label, Randomized Three-Arm Phase III Trial. J. Clin. Oncol. 2016, 34, 3300–3307. [Google Scholar] [CrossRef]
- Deng, Y.; Chi, P.; Lan, P.; Wang, L.; Chen, W.; Cui, L.; Chen, D.; Cao, J.; Wei, H.; Peng, X.; et al. Neoadjuvant Modified FOLFOX6 with or Without Radiation Versus Fluorouracil Plus Radiation for Locally Advanced Rectal Cancer: Final Results of the Chinese FOWARC Trial. J. Clin. Oncol. 2019, 37, 3223–3233. [Google Scholar] [CrossRef]
- Jiao, D.; Zhang, R.; Gong, Z.; Liu, F.; Chen, Y.; Yu, Q.; Sun, L.; Duan, H.; Zhu, S.; Liu, F.; et al. Fluorouracil-based preoperative chemoradiotherapy with or without oxaliplatin for stage II/III rectal cancer: A 3-year follow-up study. Chin. J. Cancer Res. 2015, 27, 9. [Google Scholar]
- Iyer, L.; Das, S.; Janisch, L.; Wen, M.; Ramírez, J.; Karrison, T.; Fleming, G.F.; Vokes, E.E.; Schilsky, R.L.; Ratain, M.J. UGT1A1*28 polymorphism as a determinant of irinotecan disposition and toxicity. Pharmacogenom. J. 2002, 2, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Allegra, C.J.; Yothers, G.; O’Connell, M.J.; Beart, R.W.; Wozniak, T.F.; Pitot, H.C.; Shields, A.F.; Landry, J.C.; Ryan, D.P.; Arora, A.; et al. Neoadjuvant 5-FU or Capecitabine Plus Radiation with or Without Oxaliplatin in Rectal Cancer Patients: A Phase III Randomized Clinical Trial. JNCI J. Natl. Cancer Inst. 2015, 107, djv248. [Google Scholar] [CrossRef]
- O’Connell, M.J.; Colangelo, L.H.; Beart, R.W.; Petrelli, N.J.; Allegra, C.J.; Sharif, S.; Pitot, H.C.; Shields, A.F.; Landry, J.C.; Ryan, D.P.; et al. Capecitabine and Oxaliplatin in the Preoperative Multimodality Treatment of Rectal Cancer: Surgical End Points From National Surgical Adjuvant Breast and Bowel Project Trial R-04. J. Clin. Oncol. 2014, 32, 1927–1934. [Google Scholar] [CrossRef]
- Mohiuddin, M.; Paulus, R.; Mitchell, E.; Hanna, N.; Yuen, A.; Nichols, R.; Yalavarthi, S.; Hayostek, C.; Willett, C. 5-Year Updated Results of Rtog-0012 Randomized Phase II Study Of Neoadjuvant Combined Modality Chemoradiation for Distal Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Saha, A.; Dastidar, A.; Mahata, A.; Das, A.; Sarkar, R.; Kayal, P. A Randomized Comparative Study between Neoadjuvant 5-Fluorouracil and Leukovorin versus 5-Fluorouracil and Cisplatin along with Concurrent Radiation in Locally Advanced Carcinoma Rectum. Clin. Cancer Investig. J. 2014, 4, 32. [Google Scholar] [CrossRef]
- Saha, A.; Ghosh, S.K.; Roy, C.; Saha MLChoudhury, K.B.; Chatterjee, K. A Randomized Controlled Pilot Study to Compare Capecitabine-Oxaliplatin with 5-FU-Leucovorin as Neoadjuvant Concurrent Chemoradiation in Locally Advanced Adenocarcinoma of Rectum. J. Cancer Res. Ther. 2015, 11, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Haddad, P.; Miraie, M.; Farhan, F.; Fazeli, M.S.; Alikhassi, A.; Maddah-Safaei, A.; Aghili, M.; Kalaghchi, B.; Babaei, M. Addition of oxaliplatin to neoadjuvant radiochemotherapy in MRI-defined T3, T4 or N+ rectal cancer: A randomized clinical trial. Asia Pac. J. Clin. Oncol. 2017, 13, 416–422. [Google Scholar] [CrossRef]
- Jung, M.; Shin, S.J.; Koom, W.S.; Jung, I.; Keum, K.C.; Hur, H.; Min, B.S.; Baik, S.H.; Kim, N.K.; Kim, H.; et al. A Randomized Phase 2 Study of Neoadjuvant Chemoradiaton Therapy with 5-Fluorouracil/Leucovorin or Irinotecan/S-1 in Patients with Locally Advanced Rectal Cancer. Int. J. Radiat. Oncol. 2015, 93, 1015–1022. [Google Scholar] [CrossRef]
- Kim, C.W.; Kang, B.M.; Kim, I.Y.; Kim, J.Y.; Park, S.J.; Park, W.C.; Bae, K.B.; Bae, B.-N.; Baek, S.K.; Baik, S.H.; et al. Korean Society of Coloproctology (KSCP) trial of cONsolidation Chemotherapy for Locally advanced mid or low rectal cancer after neoadjUvant concurrent chemoraDiothErapy: A multicenter, randomized controlled trial (KONCLUDE). BMC Cancer 2018, 18, 538. [Google Scholar] [CrossRef] [PubMed]
- Fu, X.-L.; Fang, Z.; Shu, L.-H.; Tao, G.-Q.; Wang, J.-Q.; Rui, Z.-L.; Zhang, Y.-J.; Tian, Z.-Q. Meta-analysis of oxaliplatin-based versus fluorouracil-based neoadjuvant chemoradiotherapy and adjuvant chemotherapy for locally advanced rectal cancer. Oncotarget 2017, 8, 34340–34351. [Google Scholar] [CrossRef]
- Hüttner, F.J.; Probst, P.; Kalkum, E.; Hackbusch, M.; Jensen, K.; Ulrich, A.; Debus, J.; Jäger, D.; Diener, M.K. Addition of Platinum Derivatives to Fluoropyrimidine-Based Neoadjuvant Chemoradiotherapy for Stage II/III Rectal Cancer: Systematic Review and Meta-Analysis. JNCI J. Natl. Cancer Inst. 2019, 111, 887–902. [Google Scholar] [CrossRef]
- Des Guetz, G.; Landre, T.; Bollet, M.A.; Mathonnet, M.; Quéro, L. Is There a Benefit of Oxaliplatin in Combination with Neoadjuvant Chemoradiotherapy for Locally Advanced Rectal Cancer? An Updated Meta-Analysis. Cancers 2021, 13, 6035. [Google Scholar] [CrossRef]
- Siddiqui, M.R.S.; Simillis, C.; Hunter, C.; Chand, M.; Bhoday, J.; Garant, A.; Vuong, T.; Artho, G.; Rasheed, S.; Tekkis, P.; et al. A Meta-Analysis Comparing the Risk of Metastases in Patients with Rectal Cancer and MRI-Detected Extramural Vascular Invasion (MrEMVI) vs MrEMVI-Negative Cases. Br. J. Cancer 2017, 116, 1513–1519. [Google Scholar] [CrossRef]
- Battersby, N.J.; How, P.; Moran, B.; Stelzner, S.; West, N.P.; Branagan, G.; Strassburg, J.; Quirke, P.; Tekkis, P.; Pedersen, B.G.; et al. Prospective Validation of a Low Rectal Cancer Magnetic Resonance Imaging Staging System and Development of a Local Recurrence Risk Stratification Model: The MERCURY II Study. Ann. Surg. 2016, 263, 751–760. [Google Scholar] [CrossRef]
- Lord, A.C.; Corr, A.; Chandramohan, A.; Hodges, N.; Pring, E.; Airo-Farulla, C.; Moran, B.; Jenkins, J.T.; Di Fabio, F.; Brown, G. Assessment of the 2020 NICE Criteria for Preoperative Radiotherapy in Patients with Rectal Cancer Treated by Surgery Alone in Comparison with Proven MRI Prognostic Factors: A Retrospective Cohort Study. Lancet Oncol. 2022, 23, 793–801. [Google Scholar] [CrossRef]
- Meng, X.; Sun, X.; Liu, Z.; He, Y. A Novel Era of Cancer/Testis Antigen in Cancer Immunotherapy. Int. Immunopharmacol. 2021, 98, 107889. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Nishimura, S.; Ito, T.; Akagi, M. Clinicopathological Assessment of Cancer/Testis Antigens NY-ESO-1 and MAGE-A4 in Highly Aggressive Soft Tissue Sarcomas. Diagnostics 2022, 12, 733. [Google Scholar] [CrossRef]
- Ishihara, M.; Kageyama, S.; Miyahara, Y.; Ishikawa, T.; Ueda, S.; Soga, N.; Naota, H.; Mukai, K.; Harada, N.; Ikeda, H.; et al. MAGE-A4, NY-ESO-1 and SAGE MRNA Expression Rates and Co-Expression Relationships in Solid Tumours. BMC Cancer 2020, 20, 606. [Google Scholar] [CrossRef]
- Cercek, A.; Lumish, M.; Sinopoli, J.; Weiss, J.; Shia, J.; Lamendola-Essel, M.; El Dika, I.H.; Segal, N.; Shcherba, M.; Sugarman, R.; et al. PD-1 Blockade in Mismatch Repair–Deficient, Locally Advanced Rectal Cancer. N. Engl. J. Med. 2022, 386, 2363–2376. [Google Scholar] [CrossRef]
- Galluzzi, L.; Buqué, A.; Kepp, O.; Zitvogel, L.; Kroemer, G. Immunological Effects of Conventional Chemotherapy and Targeted Anticancer Agents. Cancer Cell 2015, 28, 690–714. [Google Scholar] [CrossRef] [PubMed]
- Martins, I.; Kepp, O.; Schlemmer, F.; Adjemian, S.; Tailler, M.; Shen, S.; Michaud, M.; Menger, L.; Gdoura, A.; Tajeddine, N.; et al. Restoration of the immunogenicity of cisplatin-induced cancer cell death by endoplasmic reticulum stress. Oncogene 2011, 30, 1147–1158. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Aparicio, M.; Alzuguren, P.; Mauleon, I.; Medina-Echeverz, J.; Hervas-Stubbs, S.; Mancheno, U.; Berraondo, P.; Crettaz, J.; Gonzalez-Aseguinolaza, G.; Prieto, J.; et al. Oxaliplatin in combination with liver-specific expression of interleukin 12 reduces the immunosuppressive microenvironment of tumours and eradicates metastatic colorectal cancer in mice. Gut 2011, 60, 341–349. [Google Scholar] [CrossRef]
- Kanterman, J.; Sade-Feldman, M.; Biton, M.; Ish-Shalom, E.; Lasry, A.; Goldshtein, A.; Hubert, A.; Baniyash, M. Adverse immunoregulatory effects of 5FU and CPT11 chemotherapy on myeloid-derived suppressor cells and colorectal cancer outcomes. Cancer Res. 2014, 74, 6022–6035. [Google Scholar] [CrossRef]
- Kim, H.-S.; Park, H.-M.; Park, J.-S.; Sohn, H.-J.; Kim, S.-G.; Kim, H.-J.; Oh, S.-T.; Kim, T.-G. Dendritic cell vaccine in addition to FOLFIRI regimen improve antitumor effects through the inhibition of immunosuppressive cells in murine colorectal cancer model. Vaccine 2010, 28, 7787–7796. [Google Scholar] [CrossRef]
- Kalanxhi, E.; Meltzer, S.; Schou, J.V.; Larsen, F.O.; Dueland, S.; Flatmark, K.; Jensen, B.V.; Hole, K.H.; Seierstad, T.; Redalen, K.R.; et al. Systemic immune response induced by oxaliplatin-based neoadjuvant therapy favours survival without metastatic progression in high-risk rectal cancer. Br. J. Cancer 2018, 118, 1322–1328. [Google Scholar] [CrossRef]
- Wang, L.; Dou, X.; Chen, S.; Yu, X.; Huang, X.; Zhang, L.; Chen, Y.; Wang, J.; Yang, K.; Bugno, J.; et al. YTHDF2 inhibition potentiates radiotherapy antitumor efficacy. Cancer Cell 2023, 41, 1294–1308.e8. [Google Scholar] [CrossRef]
- Fiorica, F.; Tebano, U.; Gabbani, M.; Perrone, M.; Missiroli, S.; Berretta, M.; Giuliani, J.; Bonetti, A.; Remo, A.; Pigozzi, E.; et al. Beyond Abscopal Effect: A Meta-Analysis of Immune Checkpoint Inhibitors and Radiotherapy in Advanced Non-Small Cell Lung Cancer. Cancers 2021, 13, 2352. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Simple Size | Mean Age | Male (%) | ECOG 0–1 (%) | cT3 (%) | cT4 (%) | cN+ (%) | Sphincter- Saving Surgery (%) | Definitive Stoma (%) | pCR (%) | ypT0 (%) | ypN0 (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Platin-derived/based | ||||||||||||
| ACCORD12 [12,13] | 598 | 62 | 57 | 94 | 87 | 5 | 71 | 69 | 22 | 28 | 17 | 70 |
| CAO/ARO/AIO-04 [14] | 1197 | 62 | 71 | 82 | 87 | 7 | 72 | 67 | 25 | 16 | 16 | 69 |
| FOWARC [22,23] | 271 | 53 | 64 | - | 62 | 34 | 80 | - | - | 21 | - | 74 |
| Haddad et al. [31] | 63 | 57 | 68 | - | 86 | 6 | 89 | - | - | 24 | - | - |
| INTERACT [19] | 534 | 59 | 68 | - | 90 | 0 | 77 | 71 | 15 | 29 | - | - |
| Jiao et al. [24] | 206 | 63 | 62 | 95 | 62 | 36 | 78 | 82 | 18 | 21 | 21 | 67 |
| Kayal et al. [29] | 49 | - | 73 | 87 | 31 | 69 | - | 71 | 29 | 31 | - | - |
| Marechal et al. [15] | 57 | 62 | 65 | 100 | 89 | 9 | 90 | 82 | 14 | 26 | 26 | 51 |
| NSABP04 [26,27] | 1608 | - | 68 | - | - | - | 41 | 74 | 26 | 19 | - | - |
| PETACC-6 [16] | 1094 | 62 | 71 | 99 | 85 | 8 | 71 | 67 | 25 | 12 | - | - |
| Saha et al. [30] | 49 | - | 73 | 96 | 31 | 69 | - | - | 28 | 18 | - | - |
| STAR-01 [17,18] | 747 | 62 | 67 | 99 | 81 | <1 | 65 | 76 | 18 | - | 17 | 68 |
| Irinotecan-based | ||||||||||||
| ARISTOTLE [20] | 564 | 61 | 66 | - | 77 | 16 | - | 42 | 55 | 20 | - | - |
| Jung et al. [32] | 141 | 57 | 68 | 100 | 79 | 21 | 89 | 95 | 4 | 20 | 20 | 68 |
| PRODIGE [21] | 461 | 61 | 66 | 98 | 78 | 16 | 88 | 79 | 13 | 18 | 18 | 69 |
| RTOG 0012 [28] | 103 | 57 | 65 | 100 | 72 | 30 | 38 | - | - | 15 | 28 | - |
| Zhu et al. [25] | 356 | 55 | 82 | 100 | 80 | 17 | 94 | 56 | 30 | 24 | 25 | 64 |
| Details of Neoadjuvant Radiation | Details of Neoadjuvant CT | Compliance (%) | ≥G3 (%) | Details of Adjuvant CT | ||
|---|---|---|---|---|---|---|
| Platin-derived/based | ||||||
| experimental | control | |||||
| ACCORD12 [12,13] | 1.8 Gy/25 daily fractions 45 Gy Total | CAPE 800 mg/m2 bid × 5 d + OXA 50 mg/m2 once per wk | CAPE 800 mg/m2 bid × 5 days | 94 | 19 | No specific recommendation |
| CAO/ARO/AIO-0414 [14] | 1.8 Gy/28 daily fractions 50.4 Gy Total | 5-FU 250 mg/m2 per day CVI × d 1–14 and d 22–35 + OXA 50 mg/m2 × d 1, 8, 22, and 29 | 5-FU 1000 mg/m2 per day CVI over 5 d × d 1–5 and d 29–33 | 75 | 23 | 5-FU/LV/OX: OXA 100 mg/m2 × d 1 and 15 + LV 400 mg/m2 × d 1 and 15 + 5-FU 2.4 g/m2 over 46 h CVI d 1–2 and d 15–16 |
| FOWARC [22,23] | 1.8 Gy/28 daily fractions 50.4 Gy Total | 5-FU 225 mg/m2 per d × 5 days CVI + OXA 60 mg/m2 per wk | 5-FU 225 mg/m2 per d × 5 days CVI | 90 | 27 | Fluorouracil-based adjuvant chemotherapy |
| Haddad et al. [31] | 1.8 Gy/25 daily fractions + boost of 5.4 Gy/3 fractions 50.4 Gy Total | CAPE 825 mg/m2 bid × 5 d + OXA 60 mg/m2 once per wk × 5–6 cycles | CAPE 825 mg/m2 bid × 5 days | 100 | 13 | No specific recommendation |
| INTERACT [19] | 1.8 Gy/25 daily fractions + boost of 5.4 Gy/3 fractions 50.4 Gy Total | CAPE 1300 mg/m2 in three time/day × 7 days + OXA 130 mg/m2 d 1, 19, and 38 | CAPE 1650 mg/m2 in three time/day × 7 days | 96 | 6 | 5-FU-based |
| Jiao et al. [24] | 2 Gy/25 daily fractions 50 Gy Total | CAPE 800 mg/m2 bid × d 1– 14 and d 22– 25 + OXA 60 mg/m2 d 1, 8, 22, and 29 | CAPE 800 mg/m2 bid. × d 1–14 and d 22–25 | 83 | 16 | mFOLFOX6: OXA 85 mg/m2 + LV 400 mg/m2 + 5-FU 400 mg/m2 bolus+ 5-FU 2.4 g/m2 over 46–48 h CVI every 2 wk × 6–8 cycles |
| Kayal et al. [29] | 1.8 Gy/28 daily fractions 50.4 Gy Total | 5-FU 350 mg/m2 CVI × d 1–5 and d 29–33 + CIS 100 mg/m2 × d 1 and 29 | 5-FU 350 mg/m2 CVI × d 1–5 and d 29 + LV 20 mg/m2 | - | 29 | mFOLFOX6: OXA 85 mg/m2 + LV 400 mg/m2 + 5-FU 400 mg/m2 bolus + 5-FU 2.4 g/m2 over 46–48 h CVI every 2 wk× 4 |
| Marechal et al. [15] | 1.8 Gy/25 daily fractions 45 Gy Total | day 1 and 14: 5-FU 400 mg/m2 on day 1 with folinic acid 400 mg/m2 on day 1, 5-FU 2000 mg/m2 CVI over a 46 h period CVI + OXA 100 mg/m2 i.v. over 2 h | 5-FU 225 mg/m2 per d × 5 days CVI | 97 | 21 | No specific recommendation |
| NSABP04 [26,27] | 1.8 Gy/25 daily fractions/5 wk + boost of 5.4 Gy/3 fractions (boost of 10.8 Gy/3 fractions for T4 or fixed distal tumours) 50.4 Gy (55.8 Gy) Total | 5-FU 225 mg/m2 per d × 5 days CVI + OXA 50 mg/m2 once per week or CAPE 825 mg/m2 bid × 5 days + OXA 50 mg/m2 once per week | 5-FU 225 mg/m2 per d × 5 days CVI or CAPE 825 mg/m2 bid × 5 days | - | 33 | No specific recommendation |
| PETACC-6 [16] | 1.8 Gy/25 daily fractions + optional boost of 5.4 Gy/3 fractions (d 36–38) 45 Gy/50.4 Gy | CAPE 825 mg/m2 bid × d 1–33 w/o weekends + OX 50 mg/m2 × d 1, 8, 15, 22, and 29 | CAPE (825 mg/m2 bid × d 1–33 w/o weekends) | 92 | 48 | CAPOX: CAPE 1000 mg/m2 bid × d 1–15 + OXA 130 mg/m2 × d 1 every 3 wk for 6 cycles |
| Saha et al. [30] | 1.8 Gy/28 daily fractions 50.4 Gy Total | CAPE 1000 mg/m2 bid × d 1–14 and d 25–38 + OXA 85 mg/m2 × d 1 and 29 | 5-FU 350 mg/m2 CVI × d 1–5 and d 29 + LV 20 mg/m2 | - | 43 | mFOLFOX6: OXA 85 mg/m2 + LV 400 mg/m2 + 5-FU 400 mg/m2 bolus + 5-FU 2.4 g/m2 over 46–48 h CVI every 2 wk × 4 |
| STAR-01 [17,18] | 1.8 Gy/28 daily fractions 50.4 Gy Total | 5-FU 225 mg/m2 per d × 5 days CVI + OXA 60 mg/m2 per wk | 5-FU 225 mg/m2 per d × 5 days CVI | 83 | 15 | Fluorouracil-based adjuvant chemotherapy |
| Irinotecan-based | ||||||
| ARISTOTLE [20] | 1.8 Gy/25 daily fractions 45 Gy Total | CAPE 650 mg/m2 bid + weekly Irinotecan 60 mg/m2 weeks 1–4 | CAPE 900 mg/m2 bid × 5 days | 72 | 16 | No specific recommendation |
| Jung et al. [32] | 1.8 Gy/28 daily fractions 50.4 Gy Total | Irinotecan 40 mg/m2 on days 1, 8, 15, 22, and 29 + S-1 70 mg/m2 on the day of irradiation | 5-FU (400 mg/m2/day)+ LV 20 mg/m2/day for 3 consecutive days every 4 weeks for 2 cycles | 86 | 6 | Fluorouracil-based adjuvant chemotherapy |
| PRODIGE [21] | 2 Gy/25 daily fractions 50 Gy Total | OXA 85 mg/m2 + LV 400 mg/m2 (2 h ev) followed by Irinotecan 180 mg/m2 (90 min ev) and 5-FU 2400 mg/m2 CVI over 46 h. FOLFIRINOX was given every 14 days for six cycles. | CAPE 800 mg/m2 bid × 5 days | 89 | 60 | mFOLFOX6: OXA 85 mg/m2 + LV 400 mg/m2 + 5-FU 400 mg/m2 bolus + 5-FU 2.4 g/m2 over 46–48 h CVI every 2 wk × 4 |
| RTOG 0012 [28] | 1.8 Gy/25 daily fractions (+boost 5.4 T3 and 10.8 T4) 50.4–60.4 Gy Total | 5-FU 225 mg/m2 per d × 5 days CVI and weekly 50 mg/m2 Irinotecan | 5-FU (225 mg/m2 per d × 5 days CVI) | 100 | 13 | no specific recommendation |
| Zhu et al. [25] | 2 Gy/25 daily fractions 50 Gy Total | CAPE 625 mg/m2 bid 5 d/wk and weekly 80 mg/m2 Irinotecan, followed by a cycle of CAPE 1000 mg/m2 bid plus Irinotecan 200 mg/m2 (XELIRI) 2 weeks after CRT | CAPE (825 mg/m2 bid × 5 days) | 99 | 22 | CAPOX (CAPE 1000 mg/m2 bid × d 1–15 + OXA 130 mg/m2 × d 1 every 3 wk for 6 cycles) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giuliani, J.; Tebano, U.; Mandarà, M.; Franceschetto, A.; Giorgi, C.; Missiroli, S.; Gabbani, M.; Napoli, G.; Luca, N.; Mangiola, D.; et al. “Add More Arrows to Your Quiver”: The Role of Adding Another Chemotherapy Drug to Fluoropyrimidine and Long Term Radiotherapy in Locally Advanced Rectal Cancer: A Systematic Review and Meta-Analysis. J. Clin. Med. 2025, 14, 345. https://doi.org/10.3390/jcm14020345
Giuliani J, Tebano U, Mandarà M, Franceschetto A, Giorgi C, Missiroli S, Gabbani M, Napoli G, Luca N, Mangiola D, et al. “Add More Arrows to Your Quiver”: The Role of Adding Another Chemotherapy Drug to Fluoropyrimidine and Long Term Radiotherapy in Locally Advanced Rectal Cancer: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2025; 14(2):345. https://doi.org/10.3390/jcm14020345
Chicago/Turabian StyleGiuliani, Jacopo, Umberto Tebano, Marta Mandarà, Antonella Franceschetto, Carlotta Giorgi, Sonia Missiroli, Milena Gabbani, Giuseppe Napoli, Nicoletta Luca, Daniela Mangiola, and et al. 2025. "“Add More Arrows to Your Quiver”: The Role of Adding Another Chemotherapy Drug to Fluoropyrimidine and Long Term Radiotherapy in Locally Advanced Rectal Cancer: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 14, no. 2: 345. https://doi.org/10.3390/jcm14020345
APA StyleGiuliani, J., Tebano, U., Mandarà, M., Franceschetto, A., Giorgi, C., Missiroli, S., Gabbani, M., Napoli, G., Luca, N., Mangiola, D., Muraro, M., Perrone, M., Pinton, P., & Fiorica, F. (2025). “Add More Arrows to Your Quiver”: The Role of Adding Another Chemotherapy Drug to Fluoropyrimidine and Long Term Radiotherapy in Locally Advanced Rectal Cancer: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 14(2), 345. https://doi.org/10.3390/jcm14020345