
Comparison of Dexmedetomidine and Remifentanil on Adropin Expression in Unilateral Lumbar Microdiscectomy: A Prospective Active Controlled Randomized Trial Study

Abstract
1. Introduction
2. Materials and Methods
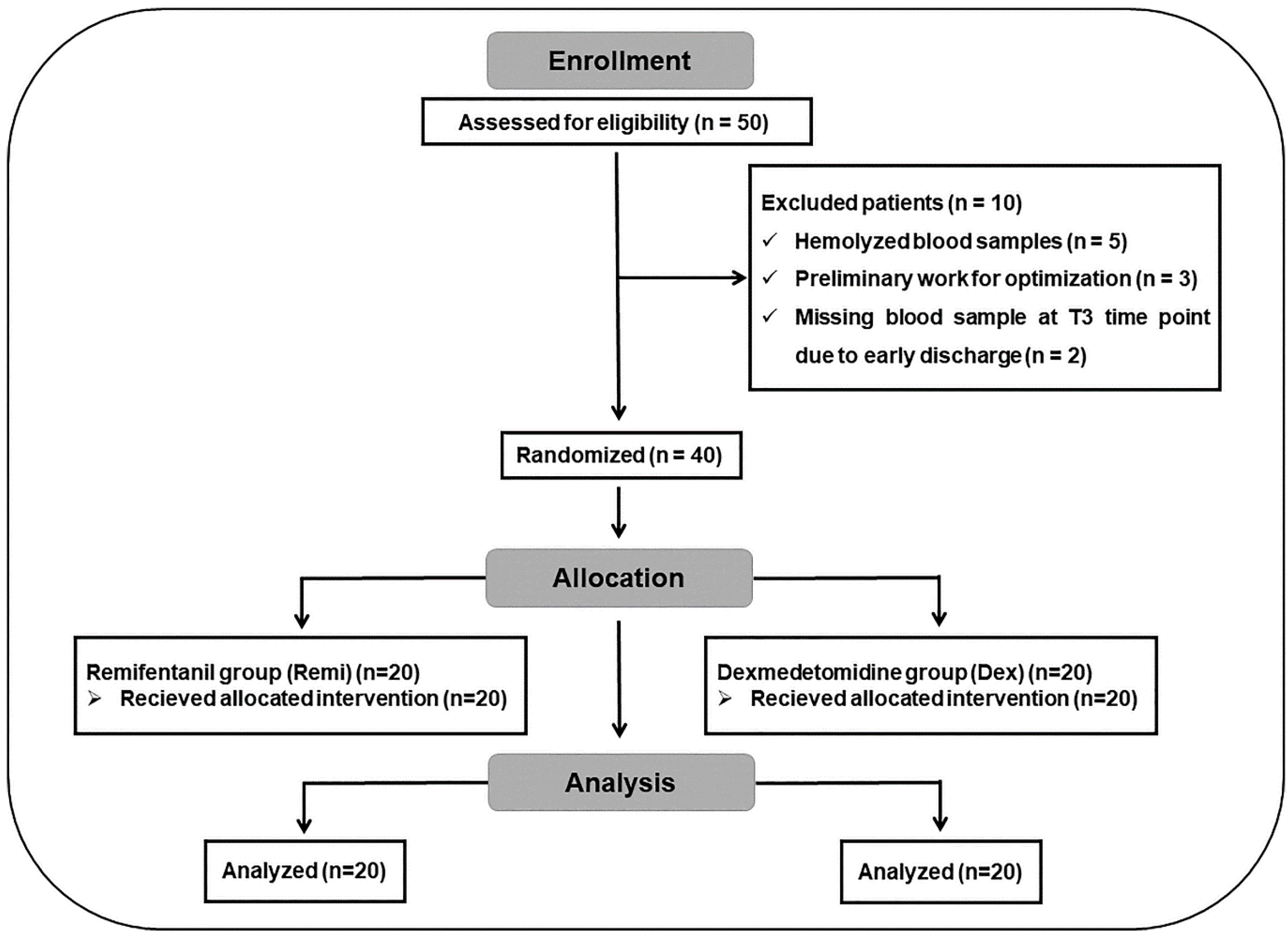
2.1. Participants and Ethical Statement
2.2. Anesthesia Protocols
2.3. Surgical Protocols
2.4. Blood Sample Collection
2.5. Enzyme-Linked Immunosorbent Assay (ELISA) Analyses
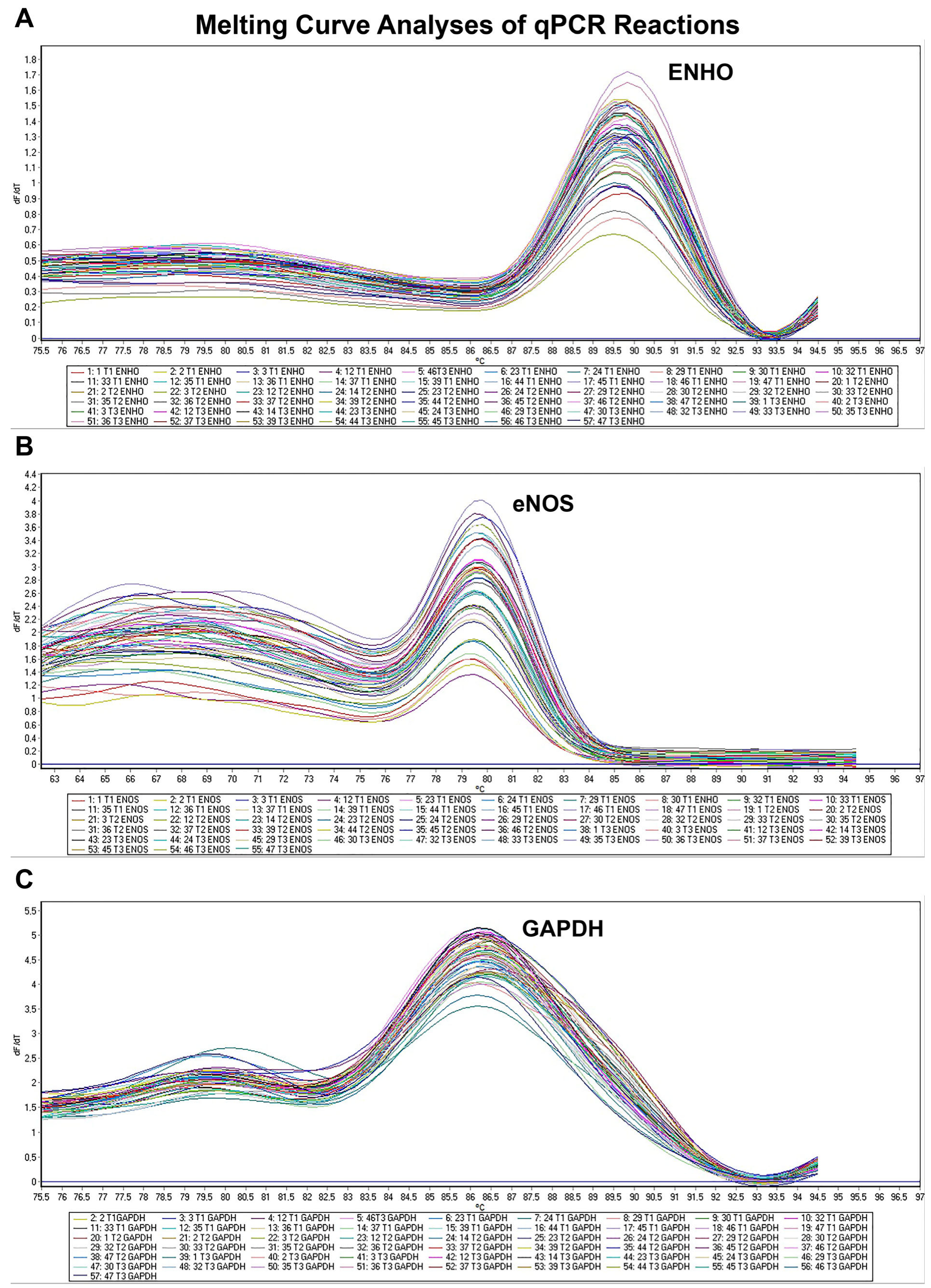
2.6. Relative mRNA Expression Analysis
2.7. Statistical Analysis
3. Results
3.1. Demographic and Clinical Parameters of Subjects
3.2. Adropin and eNOS Expression Levels
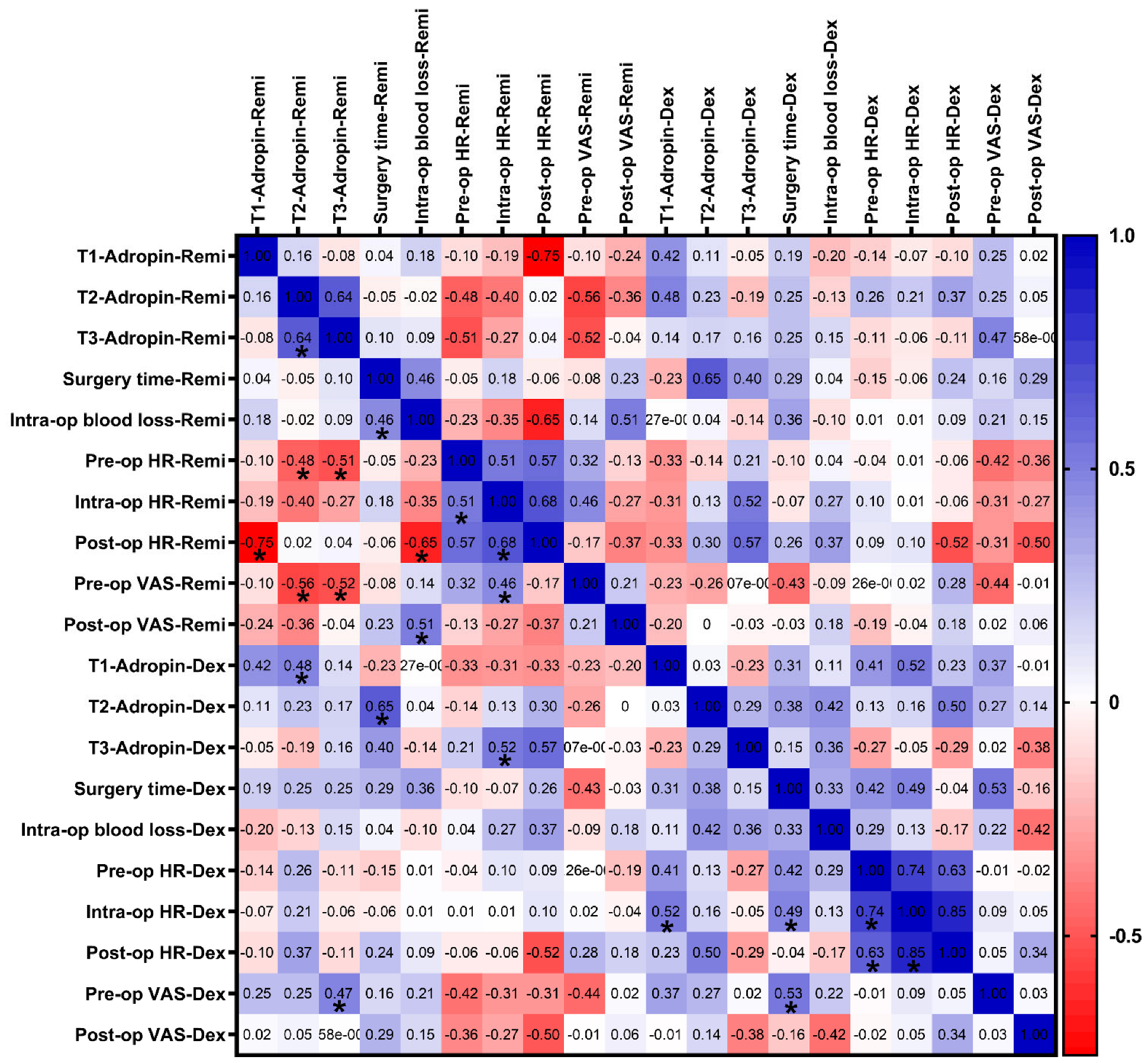
3.3. Correlation Analyses of Serum Adropin Levels with Clinical Parameters
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologists |
| BMI | Body Mass Index |
| BPH | Benign prostatic hyperplasia |
| cGMP | Cyclic guanosine monophosphate |
| CNS | Central nervous system |
| COPD | Chronic obstructive pulmonary disease |
| Ct | Cycle threshold |
| Dex | Dexmedetomidine |
| DM | Diabetes mellitus |
| EDTA | Ethylenediaminetetraacetic acid |
| ELISA | Enzyme-Linked ImmunoSorbent Assay |
| ENHO | Energy homeostasis associated |
| eNOS | Endothelial nitric oxide synthase |
| GAPDH | Glyceraldehyde-3-phosphate dehydrogenase |
| HT | Hypertension |
| LDH | Lumbar disc herniation |
| MAP | Mean arterial pressure |
| MRI | Magnetic resonance imaging |
| NSAID | Non-steroid anti-inflamatory drug |
| NO | Nitric oxide |
| PACU | Post-anesthesia care unit |
| pre-op | Preoperative |
| post-op | Postoperative |
| Remi | Remifentanil |
| RT-qPCR | Quantitative reverse transcription polymerase chain reaktion |
| SBP | Systolic blood pressure |
| VAS | Visual analogue scale |
References
- Fjeld, O.R.; Grovle, L.; Helgeland, J.; Smastuen, M.C.; Solberg, T.K.; Zwart, J.A.; Grotle, M. Complications, reoperations, readmissions, and length of hospital stay in 34,639 surgical cases of lumbar disc herniation. Bone Jt. J. 2019, 101-B, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Shakya, A.; Sharma, A.; Singh, V.; Rathore, A.; Garje, V.; Wadgave, V.; Kakadiya, G.; Marathe, N. Preoperative Lumbar Epidural Steroid Injection Increases the Risk of a Dural Tear During Minimally Invasive Lumbar Discectomy. Int. J. Spine Surg. 2022, 16, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Kreiner, D.S.; Hwang, S.W.; Easa, J.E.; Resnick, D.K.; Baisden, J.L.; Bess, S.; Cho, C.H.; DePalma, M.J.; Dougherty, P., 2nd; Fernand, R.; et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014, 14, 180–191. [Google Scholar] [CrossRef]
- Gunraj, R.E.; Yang, C.; Liu, L.; Larochelle, J.; Candelario-Jalil, E. Protective roles of adropin in neurological disease. Am. J. Physiol. Cell Physiol. 2023, 324, C674–C678. [Google Scholar] [CrossRef] [PubMed]
- Shahjouei, S.; Ansari, S.; Pourmotabbed, T.; Zand, R. Potential Roles of Adropin in Central Nervous System: Review of Current Literature. Front. Mol. Biosci. 2016, 3, 25. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.G.; Trevaskis, J.L.; Lam, D.D.; Sutton, G.M.; Koza, R.A.; Chouljenko, V.N.; Kousoulas, K.G.; Rogers, P.M.; Kesterson, R.A.; Thearle, M.; et al. Identification of adropin as a secreted factor linking dietary macronutrient intake with energy homeostasis and lipid metabolism. Cell Metab. 2008, 8, 468–481. [Google Scholar] [CrossRef]
- Aydin, S.; Kuloglu, T.; Aydin, S.; Eren, M.N.; Yilmaz, M.; Kalayci, M.; Sahin, I.; Kocaman, N.; Citil, C.; Kendir, Y. Expression of adropin in rat brain, cerebellum, kidneys, heart, liver, and pancreas in streptozotocin-induced diabetes. Mol. Cell. Biochem. 2013, 380, 73–81. [Google Scholar] [CrossRef]
- Lovren, F.; Pan, Y.; Quan, A.; Singh, K.K.; Shukla, P.C.; Gupta, M.; Al-Omran, M.; Teoh, H.; Verma, S. Adropin is a novel regulator of endothelial function. Circulation 2010, 122, S185–S192. [Google Scholar] [CrossRef]
- Aydin, S. Three new players in energy regulation: Preptin, adropin and irisin. Peptides 2014, 56, 94–110. [Google Scholar] [CrossRef]
- Kwon, O.S.; Andtbacka, R.H.I.; Hyngstrom, J.R.; Richardson, R.S. Vasodilatory function in human skeletal muscle feed arteries with advancing age: The role of adropin. J. Physiol. 2019, 597, 1791–1804. [Google Scholar] [CrossRef]
- Monsalve-Naharro, J.A.; Domingo-Chiva, E.; Garcia Castillo, S.; Cuesta-Montero, P.; Jimenez-Vizuete, J.M. Inhaled nitric oxide in adult patients with acute respiratory distress syndrome. Farm. Hosp. 2017, 41, 292–312. [Google Scholar] [CrossRef] [PubMed]
- Lopez, B.L.; Davis-Moon, L.; Ballas, S.K.; Ma, X.L. Sequential nitric oxide measurements during the emergency department treatment of acute vasoocclusive sickle cell crisis. Am. J. Hematol. 2000, 64, 15–19. [Google Scholar] [CrossRef]
- Ma, P.; Zeng, H. Effects of epidural anesthesia combined with dexmedetomidine on blood pressure, sedation, analgesia and serum beta-endorphin levels in patients with hip fractures. Am. J. Transl. Res. 2021, 13, 6457–6467. [Google Scholar]
- Wallace, J.L. Nitric oxide, aspirin-triggered lipoxins and NO-aspirin in gastric protection. Inflamm. Allergy Drug Targets 2006, 5, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Birgenheier, N.M.; Stuart, A.R.; Egan, T.D. Soft drugs in anesthesia: Remifentanil as prototype to modern anesthetic drug development. Curr. Opin. Anaesthesiol. 2020, 33, 499–505. [Google Scholar] [CrossRef]
- Janipour, M.; Bastaninejad, S.; Mohebbi, A.; Amali, A.; Owji, S.H.; Jazi, K.; Mirali, R.A.; Moshfeghinia, R. Dexmedetomidine versus remifentanil in nasal surgery: A systematic review and meta-analysis. BMC Anesthesiol. 2024, 24, 194. [Google Scholar] [CrossRef]
- Komatsu, R.; Turan, A.M.; Orhan-Sungur, M.; McGuire, J.; Radke, O.C.; Apfel, C.C. Remifentanil for general anaesthesia: A systematic review. Anaesthesia 2007, 62, 1266–1280. [Google Scholar] [CrossRef]
- Al-Hassan, A.; Weissman, B.; Chowdhury, S.; Sawires, J.; Soti, V. Comparative Efficacy of Dexmedetomidine and Remifentanil in Reducing Postoperative Pain and Opioid Use: A Systematic Review. Cureus 2025, 17, e79759. [Google Scholar] [CrossRef]
- Lee, S. Dexmedetomidine: Present and future directions. Korean J. Anesthesiol. 2019, 72, 323–330. [Google Scholar] [CrossRef]
- Ebert, T.J.; Hall, J.E.; Barney, J.A.; Uhrich, T.D.; Colinco, M.D. The effects of increasing plasma concentrations of dexmedetomidine in humans. Anesthesiology 2000, 93, 382–394. [Google Scholar] [CrossRef]
- Liu, F.; Cui, B.; Zhao, X.; Wu, Y.; Qin, H.; Guo, Y.; Wang, H.; Lu, M.; Zhang, S.; Shen, J.; et al. Correlation of Serum Adropin Levels with Risk Factors of Cardiovascular Disease in Hemodialysis Patients. Metab. Syndr. Relat. Disord. 2021, 19, 401–408. [Google Scholar] [CrossRef]
- Saklad, M. Grading of patients for surgical procedures. Anesthesiology 1941, 2, 281–284. [Google Scholar] [CrossRef]
- Aldrete, J.A. The post-anesthesia recovery score revisited. J. Clin. Anesth. 1995, 7, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Dutton, R.P. Controlled hypotension for spinal surgery. Eur. Spine J. 2004, 13 (Suppl. S1), S66–S71. [Google Scholar] [CrossRef] [PubMed]
- Huskisson, E.C. Measurement of pain. Lancet 1974, 2, 1127–1131. [Google Scholar] [CrossRef]
- Terzi, M.Y.; Ozcan, O.; Kimyon, G.; Okuyan, H.M.; Arpaci, A.; Dogan, S. miR-451a and IL18 can differentiate familial Mediterranean fever patients in attack and remission periods: A prospective cross-sectional study. Clin. Rheumatol. 2025, 44, 1691–1704. [Google Scholar] [CrossRef]
- Altamimi, T.R.; Gao, S.; Karwi, Q.G.; Fukushima, A.; Rawat, S.; Wagg, C.S.; Zhang, L.; Lopaschuk, G.D. Adropin regulates cardiac energy metabolism and improves cardiac function and efficiency. Metabolism 2019, 98, 37–48. [Google Scholar] [CrossRef]
- Mocnik, M.; Marcun Varda, N. Current Knowledge of Selected Cardiovascular Biomarkers in Pediatrics: Kidney Injury Molecule-1, Salusin-alpha and -beta, Uromodulin, and Adropin. Children 2022, 9, 102. [Google Scholar] [CrossRef]
- Degoute, C.S. Controlled hypotension: A guide to drug choice. Drugs 2007, 67, 1053–1076. [Google Scholar] [CrossRef]
- Fujie, S.; Hasegawa, N.; Horii, N.; Uchida, M.; Sanada, K.; Hamaoka, T.; Padilla, J.; Martinez-Lemus, L.A.; Maeda, S.; Iemitsu, M. Aerobic Exercise Restores Aging-Associated Reductions in Arterial Adropin Levels and Improves Adropin-Induced Nitric Oxide-Dependent Vasorelaxation. J. Am. Heart Assoc. 2021, 10, e020641. [Google Scholar] [CrossRef]
- Huang, S.T.; Lei, Y.Q.; Xie, W.P.; Zheng, Y.R.; Chen, Q.; Cao, H. Effect of postoperative administration of inhaled nitric oxide combined with high-frequency oscillatory ventilation in infants with acute hypoxemic respiratory failure and pulmonary hypertension after congenital heart surgery: A retrospective cohort study. J. Card. Surg. 2022, 37, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Javaherforooshzadeh, F.; Monajemzadeh, S.A.; Soltanzadeh, M.; Janatmakan, F.; Salari, A.; Saeed, H. A Comparative Study of the Amount of Bleeding and Hemodynamic Changes between Dexmedetomidine Infusion and Remifentanil Infusion for Controlled Hypotensive Anesthesia in Lumbar Discopathy Surgery: A Double-Blind, Randomized, Clinical Trial. Anesth. Pain. Med. 2018, 8, e66959. [Google Scholar] [CrossRef]
- Mantz, J. Dexmedetomidine. Drugs Today 1999, 35, 151–157. [Google Scholar] [CrossRef]
- Beers, R.; Camporesi, E. Remifentanil update: Clinical science and utility. CNS Drugs 2004, 18, 1085–1104. [Google Scholar] [CrossRef]
- Patel, S.S.; Spencer, C.M. Remifentanil. Drugs 1996, 52, 417–427, discussion 428. [Google Scholar] [CrossRef] [PubMed]
- Richa, F.; Yazigi, A.; Sleilaty, G.; Yazbeck, P. Comparison between dexmedetomidine and remifentanil for controlled hypotension during tympanoplasty. Eur. J. Anaesthesiol. 2008, 25, 369–374. [Google Scholar] [CrossRef]
- Fan, X.; Cai, H.; Pan, B.; Xie, Y. Comparison of dexmedetomidine and remifentanil on reducing coughing during emergence from anesthesia with tracheal intubation: A meta-analysis. Front. Pharmacol. 2022, 13, 993239. [Google Scholar] [CrossRef] [PubMed]
- Beloeil, H.; Garot, M.; Lebuffe, G.; Gerbaud, A.; Bila, J.; Cuvillon, P.; Dubout, E.; Oger, S.; Nadaud, J.; Becret, A.; et al. Balanced Opioid-free Anesthesia with Dexmedetomidine versus Balanced Anesthesia with Remifentanil for Major or Intermediate Noncardiac Surgery. Anesthesiology 2021, 134, 541–551. [Google Scholar] [CrossRef]
- Zhang, Y.; Jiang, W.; Luo, X. Remifentanil combined with dexmedetomidine on the analgesic effect of breast cancer patients undergoing modified radical mastectomy and the influence of perioperative T lymphocyte subsets. Front. Surg. 2022, 9, 1016690. [Google Scholar] [CrossRef]
- Naik, B.I.; Nemergut, E.C.; Kazemi, A.; Fernandez, L.; Cederholm, S.K.; McMurry, T.L.; Durieux, M.E. The Effect of Dexmedetomidine on Postoperative Opioid Consumption and Pain After Major Spine Surgery. Anesth. Analg. 2016, 122, 1646–1653. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Symbol | Primer Sequence | Amplicon (bp) | Anneal. (°C), Cycle | Ref. Seq. |
|---|---|---|---|---|
| ENHO | F: 5′-CTCAACTCAGGCTCAGGACT-3′ R: 5′-GACAGTGGAGCTGCCTCAAT-3′ | 144 | 65, 40× | NM_198573.3 |
| eNOS | F: 5′-GAAGGCGACAATCCTGTATGGC-3′ R: 5′-TGTTCGAGGGACACCACGTCAT-3′ | 135 | 65, 40× | NM_000603.5 |
| GAPDH | F: 5′-GTCTCCTCTGACTTCAACAGCG-3′ R: 5′- ACCACCCTGTTGCTGTAGCCAA -3′ | 131 | 65, 40× | NM_002046.7 |
| Remi (n = 20) | Dex (n = 20) | p-Value | |
|---|---|---|---|
| Age, year | 46.3 (12.6) | 42.4 (10.9) | 0.295 a |
| Sex | 0.320 b | ||
| Female | 11/20 (55%) | 15/20 (75%) | |
| Male | 9/20 (45%) | 5/20 (25%) | |
| BMI, kg/m2 | 24.8 (2.2) | 24.1 (2.4) | 0.405 a |
| Diseases | |||
| BPH | 1/20 (5%) | - | |
| Thyroid surgery | 1/20 (5%) | - | |
| HT | 4/20 (20%) | 3/20 (15%) | |
| DM | 4/20 (20%) | 2/20 (10%) | |
| COPD | - | 1/20 (5%) | |
| Surgery time, min | 100.0 (77.5–120.0) | 120.0 (96.3–120.0) | 0.468 c |
| Extubation time, min | 9.0 (7.3–10.0) | 6.0 (3.0–9.3) | 0.002 c |
| Intra-op blood loss, mL | 120.0 (80.0–150.0) | 110.0 (62.5–187.5) | 0.929 c |
| VAS | |||
| Pre-op VAS | 9.0 (8.3–9.8) | 9.5 (9.0–10.0) | 0.198 c |
| Post-op VAS | 1.5 (0.3–3.0) | 1.00 (1.0–2.0) | 0.548 c |
| p-value | <0.0001 d | <0.0001 d | |
| Heart rate, beats/min | |||
| Pre-op | 90.0 (78.5–100.8) | 91.5 (79.8–98.0) | 0.680 a |
| Intra-op | 75.0 (59.8–80.8) | 69.0 (60.0–77.0) | 0.287 a |
| Post-op | 69.5 (58.8–85.0) | 65.5 (59.0–74.0) | 0.377 a |
| p-value | <0.0001 e1 0.0052 e2 0.804 e3 | <0.0001 e1 <0.0001 e2 0.456 e3 | |
| SBP, mm Hg | |||
| Pre-op | 128.5 (120.0–140.0) | 127.5 (111.3–135.8) | 0.249 c |
| Intra-op | 103.0 (96.3–111.5) | 100.0 (94.8–106.8) | 0.343 a |
| Post-op | 102.0 (92.5–114.0) | 96.0 (90.0–99.0) | 0.093 c |
| p-value | <0.0001 e1 0.0006 e2 0.999 e3 | 0.011 e1 0.009 e2 0.010 e3 | |
| DBP, mm Hg | |||
| Pre-op | 80.0 (74.3–84.0) | 81.0 (75.0–88.0) | 0.511 a |
| Intra-op | 69.5 (53.0–74.0) | 63.0 (58.0–65.8) | 0.343 c |
| Post-op | 60.0 (51.0–76.0) | 59.0 (56.3–60.0) | 0.316 a |
| p-value | <0.0001 e1 0.002 e2 0.788 e3 | <0.0001 e1 <0.0001 e2 0.011 e3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gülbol-Duran, G.; Urfalı, S.; Urfalı, B. Comparison of Dexmedetomidine and Remifentanil on Adropin Expression in Unilateral Lumbar Microdiscectomy: A Prospective Active Controlled Randomized Trial Study. J. Clin. Med. 2025, 14, 3711. https://doi.org/10.3390/jcm14113711
Gülbol-Duran G, Urfalı S, Urfalı B. Comparison of Dexmedetomidine and Remifentanil on Adropin Expression in Unilateral Lumbar Microdiscectomy: A Prospective Active Controlled Randomized Trial Study. Journal of Clinical Medicine. 2025; 14(11):3711. https://doi.org/10.3390/jcm14113711
Chicago/Turabian StyleGülbol-Duran, Gülay, Senem Urfalı, and Boran Urfalı. 2025. "Comparison of Dexmedetomidine and Remifentanil on Adropin Expression in Unilateral Lumbar Microdiscectomy: A Prospective Active Controlled Randomized Trial Study" Journal of Clinical Medicine 14, no. 11: 3711. https://doi.org/10.3390/jcm14113711
APA StyleGülbol-Duran, G., Urfalı, S., & Urfalı, B. (2025). Comparison of Dexmedetomidine and Remifentanil on Adropin Expression in Unilateral Lumbar Microdiscectomy: A Prospective Active Controlled Randomized Trial Study. Journal of Clinical Medicine, 14(11), 3711. https://doi.org/10.3390/jcm14113711