
Open vs. Robot-Assisted Artificial Urinary Sphincter Implantation in Women with Stress Urinary Incontinence: A Multicenter Comparative Study

Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Perioperative Management
2.3. Surgical Techniques
2.3.1. Robot-Assisted Laparoscopic Implantation
2.3.2. Open Implantation
2.4. Outcomes of Interest
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Perioperative Outcomes
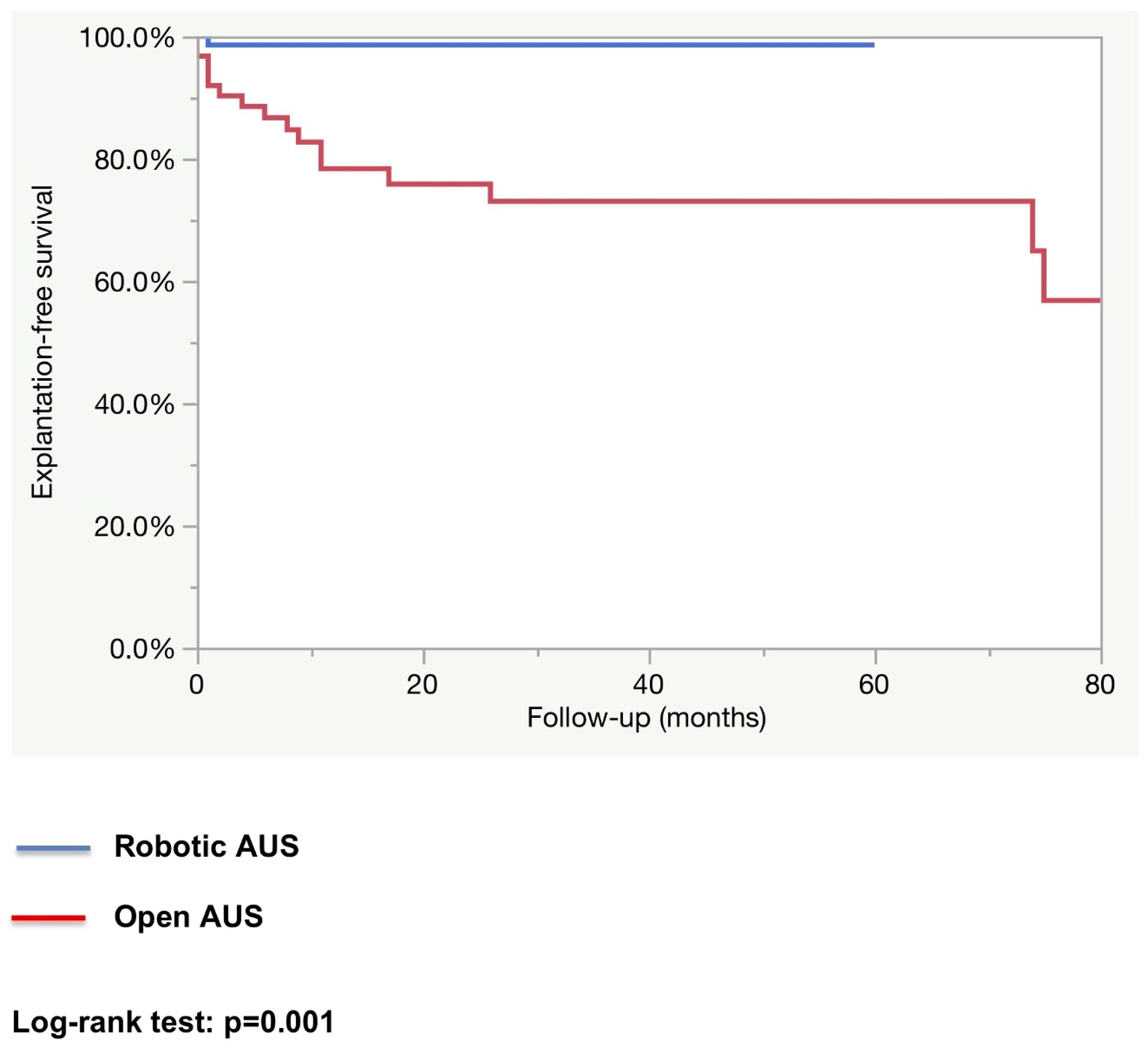
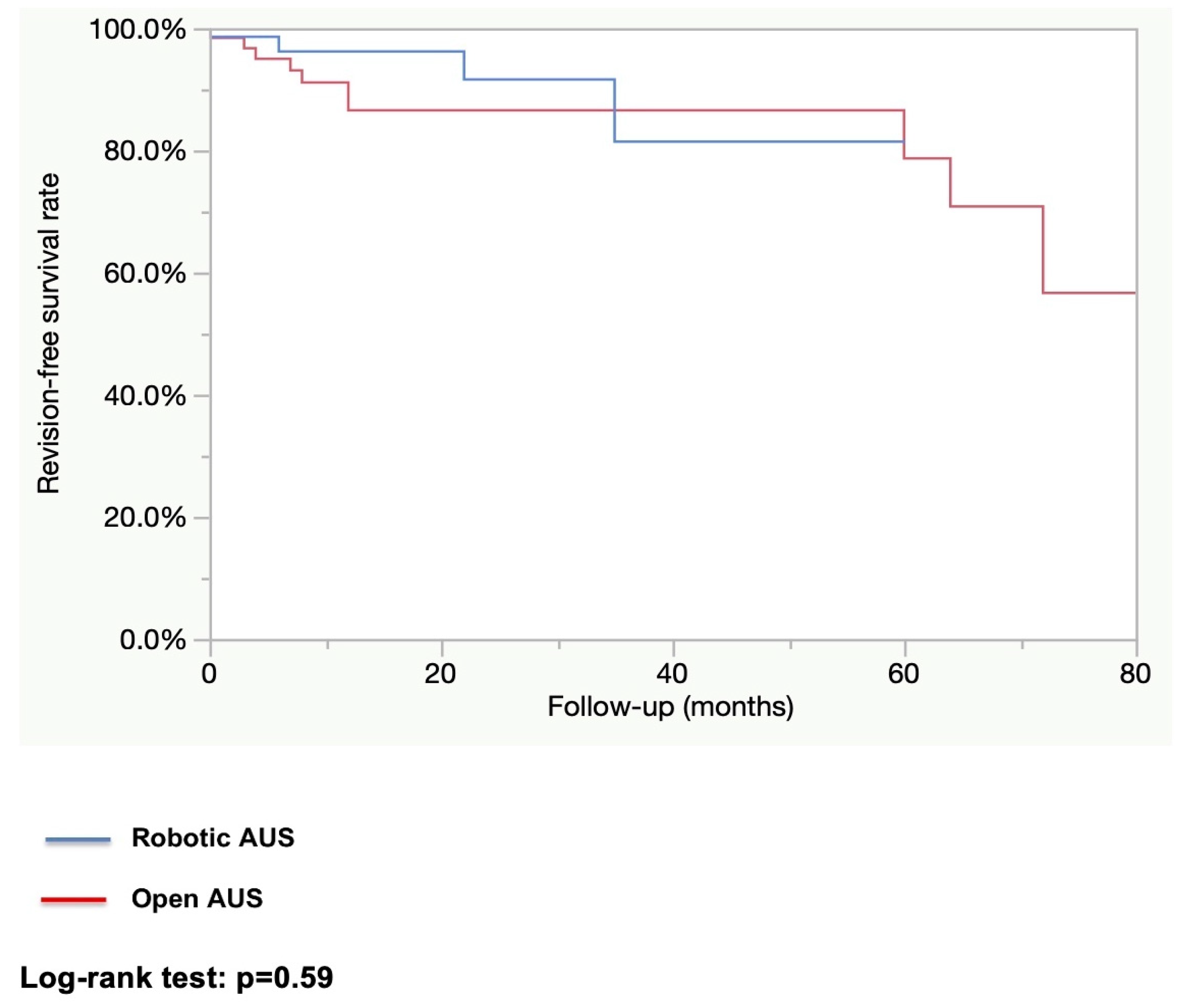
3.3. Functional Outcomes and Device Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coyne, K.S.; Sexton, C.C.; Thompson, C.L.; Milsom, I.; Irwin, D.; Kopp, Z.S.; Chapple, C.R.; Kaplan, S.; Tubaro, A.; Aiyer, L.P.; et al. The prevalence of lower urinary tract symptoms (LUTS) in the USA, the UK and Sweden: Results from the Epidemiology of LUTS (EpiLUTS) study. BJU Int. 2009, 104, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Patel, U.J.; Godecker, A.L.; Giles, D.L.; Brown, H.W. Updated Prevalence of Urinary Incontinence in Women: 2015-2018 National Population-Based Survey Data. Female Pelvic Med. Reconstr. Surg. 2022, 28, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Hunskaar, S.; Lose, G.; Sykes, D.; Voss, S. The prevalence of urinary incontinence in women in four European countries. BJU Int. 2004, 93, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Petros, P.E.; Ulmsten, U.I. An integral theory of female urinary incontinence. Experimental and clinical considerations. Acta Obstet. Gynecol. Scand. 1990, 153, 7–31. [Google Scholar] [CrossRef] [PubMed]
- DeLancey, J.O. Structural support of the urethra as it relates to stress urinary incontinence: The hammock hypothesis. Am. J. Obstet. Gynecol. 1994, 170, 1713–1720, discussion 1720–1723. [Google Scholar] [CrossRef]
- Clemons, J.L.; LaSala, C.A. The tension-free vaginal tape in women with a non-hypermobile urethra and low maximum urethral closure pressure. Int. Urogynecol. J. Pelvic Floor. Dysfunct. 2007, 18, 727–732. [Google Scholar] [CrossRef]
- Stav, K.; Dwyer, P.L.; Rosamilia, A.; Schierlitz, L.; Lim, Y.N.; Lee, J. Risk factors of treatment failure of midurethral sling procedures for women with urinary stress incontinence. Int. Urogynecol. J. 2010, 21, 149–155. [Google Scholar] [CrossRef]
- Ferreira, C.; Brychaert, P.E.; Menard, J.; Mandron, E. Laparoscopic implantation of artificial urinary sphincter in women with intrinsic sphincter deficiency: Mid-term outcomes. Int. J. Urol. Off. J. Jpn. Urol. Assoc. 2017, 24, 308–313. [Google Scholar] [CrossRef]
- Costa, P.; Poinas, G.; Ben Naoum, K.; Bouzoubaa, K.; Wagner, L.; Soustelle, L.; Boukaram, M.; Droupy, S. Long-term results of artificial urinary sphincter for women with type III stress urinary incontinence. Eur. Urol. 2013, 63, 753–758. [Google Scholar] [CrossRef]
- Fournier, G.; Callerot, P.; Thoulouzan, M.; Valeri, A.; Perrouin-Verbe, M.A. Robotic-assisted laparoscopic implantation of artificial urinary sphincter in women with intrinsic sphincter deficiency incontinence: Initial results. Urology 2014, 84, 1094–1098. [Google Scholar] [CrossRef]
- Chartier-Kastler, E.; Vaessen, C.; Rouprêt, M.; Bassi, S.; Cancrini, F.; Phé, V. Robot-assisted laparoscopic artificial urinary sphincter insertion in women with stress urinary incontinence: A pilot single-centre study. BJU Int. 2020, 126, 722–730. [Google Scholar] [CrossRef] [PubMed]
- Peyronnet, B.; Vincendeau, S.; Tondut, L.; Bensalah, K.; Damphousse, M.; Manunta, A. Artificial urinary sphincter implantation in women with stress urinary incontinence: Preliminary comparison of robot-assisted and open approaches. Int. Urogynecol. J. 2016, 27, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Cour, F.; Le Normand, L.; Lapray, J.F.; Hermieu, J.F.; Peyrat, L.; Yiou, R.; Donon, L.; Wagner, L.; Vidart, A. Intrinsic sphincter deficiency and female urinary incontinence. Progres. Urol. J. Assoc. Francaise Urol.Soc. Francaise Urol. 2015, 25, 437–454. [Google Scholar]
- Hermieu, J.F.; Conquy, S.; Leriche, B.; Debodinance, P.; Delorme, E.; Boccon Gibod, L.; Vidart, A.; Cour, F.; Richard, F.; Cardot, V.; et al. Synthesis of the guidelines for the treatment of non-neurological urinary incontinence in women. Progres. Urol. J. Assoc. Francaise Urol. Soc. Francaise Urol. 2010, 20 (Suppl. S2), S94–S99. [Google Scholar]
- Peyronnet, B.; Capon, G.; Belas, O.; Manunta, A.; Allenet, C.; Hascoet, J.; Calves, J.; Belas, M.; Callerot, P.; Robert, G.; et al. Robot-assisted AMS-800 Artificial Urinary Sphincter Bladder Neck Implantation in Female Patients with Stress Urinary Incontinence. Eur. Urol. 2019, 75, 169–175. [Google Scholar] [CrossRef]
- Costa, P.; Mottet, N.; Rabut, B.; Thuret, R.; Ben Naoum, K.; Wagner, L. The use of an artificial urinary sphincter in women with type III incontinence and a negative Marshall test. J. Urol. 2001, 165, 1172–1176. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Leal Ghezzi, T.; Campos Corleta, O. 30 Years of Robotic Surgery. World J. Surg. 2016, 40, 2550–2557. [Google Scholar] [CrossRef]
- Ahmed, K.; Khan, M.S.; Vats, A.; Nagpal, K.; Priest, O.; Patel, V.; Patel, V.; Vecht, J.A.; Ashrafian, H.; Yang, G.-Z.; et al. Current status of robotic assisted pelvic surgery and future developments. Int. J. Surg. Lond. Engl. 2009, 7, 431–440. [Google Scholar] [CrossRef]
- Palep, J.H. Robotic assisted minimally invasive surgery. J. Minimal Access Surg. 2009, 5, 1–7. [Google Scholar] [CrossRef]
- Koh, F.H.X.; Tan, K.K.; Lieske, B.; Tsang, M.L.; Tsang, C.B.; Koh, D.C. Endowrist versus wrist: A case-controlled study comparing robotic versus hand-assisted laparoscopic surgery for rectal cancer. Surg. Laparosc. Endosc. Percutan Tech. 2014, 24, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Hanly, E.J.; Miller, B.E.; Kumar, R.; Hasser, C.J.; Coste-Maniere, E.; Talamini, M.A.; Aurora, A.A.; Schenkman, N.S.; Marohn, M.R. Mentoring console improves collaboration and teaching in surgical robotics. J. Laparoendosc. Adv. Surg. Tech. 2006, 16, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.L.; Scott, E.M.; Krivak, T.C.; Olawaiye, A.B.; Chu, T.; Richard, S.D. Dual-console robotic surgery: A new teaching paradigm. J. Robot. Surg. 2013, 7, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Salkowski, M.; Checcucci, E.; Chow, A.K.; Rogers, C.C.; Adbollah, F.; Liatsikos, E.; Dasgupta, P.; Guimaraes, G.C.; Rassweiler, J.; Mottrie, A.; et al. New multiport robotic surgical systems: A comprehensive literature review of clinical outcomes in urology. Ther. Adv. Urol. 2023, 15, 17562872231177781. [Google Scholar] [CrossRef]
- Nelson, R.J.; Chavali, J.S.S.; Yerram, N.; Babbar, P.; Kaouk, J.H. Current status of robotic single-port surgery. Urol. Ann. 2017, 9, 217–222. [Google Scholar]
- Kaouk, J.; Beksac, A.T.; Abou Zeinab, M.; Duncan, A.; Schwen, Z.R.; Eltemamy, M. Single Port Transvesical Robotic Radical Prostatectomy: Initial Clinical Experience and Description of Technique. Urology 2021, 155, 130–137. [Google Scholar] [CrossRef]
- Gondran-Tellier, B.; Boissier, R.; Baboudjian, M.; Rouy, M.; Gaillet, S.; Lechevallier, E.; Michel, F.; Karsenty, G. Robot-assisted implantation of an artificial urinary sphincter, the AMS-800, via a posterior approach to the bladder neck in women with intrinsic sphincter deficiency. BJU Int. 2019, 124, 1077–1080. [Google Scholar] [CrossRef]
- Broudeur, L.; Loubersac, T.; Le Normand, L.; Karam, G.; Branchereau, J.; Rigaud, J.; Perrouin-Verbe, M.A. New technique of robot-assisted laparoscopic artificial urinary sphincter implantation in female by a posterior approach with intraoperative cystoscopic monitoring. World J. Urol. 2021, 39, 4221–4226. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Open AUS n = 64 | Robotic AUS n = 71 | p-Value | |
|---|---|---|---|
| Median age (years) | 66.5 (IQR: 59–74) | 68 (IQR: 61–74) | 0.57 |
| Mean Body Mass Index (kg/m2) | 28.5 (±4.9) | 27.2 (±4.8) | 0.13 |
| ASA score | 0.21 | ||
| 1 | 8 (12.9%) | 14 (21.2%) | |
| 2 | 36 (58.1%) | 40 (60.6%) | |
| 3 | 18 (29%) | 12 (18.2%) | |
| Neurogenic SUI | 7 (10.9%) | 4 (6%) | 0.32 |
| History of radiation therapy | 4 (6.2%) | 0 (0%) | 0.03 |
| History of previous anti-incontinence procedure | 57 (89%) | 64 (90.1%) | 0.95 |
| History of previous synthetic midurethral sling | 47 (74.6%) | 57 (80.3%) | 0.44 |
| Mean Maximum urethral closure pressure (cmH₂O) | 25.9 (±14.5) | 22.8 (±8.2) | 0.29 |
| Detrusor overactivity on preoperative urodynamics | 9 (15.5%) | 6 (8.4%) | 0.17 |
| Open AUS n = 64 | Robotic AUS n = 71 | p-Value | |
|---|---|---|---|
| Mean operative time (min) | 126.2 (±51.8) | 179.9 (±48.5) | <0.0001 |
| Intraoperative complications (Vaginal or bladder neck injury) | 17 (27.4%) | 9 (12.7%) | 0.03 |
| Mean estimated blood loss (mL) | 164.1 (±194.1) | 16.2 (±37.3) | <0.0001 |
| 30-day postoperative complications | 29 (46.8%) | 11 (15.5%) | <0.0001 |
| Major postoperative complications (Clavien ≥ 3) | 11 (17.2%) | 2 (2.8%) | 0.01 |
| Mean length of hospital stay (days) | 6.5 (±5.6) | 4.1 (±1.9) | 0.002 |
| Open AUS n = 64 | Robotic AUS n = 71 | p-Value | |
|---|---|---|---|
| Complete continence (no pad) | 40 (62.3%) | 59 (83.3%) | 0.01 |
| Explantation | 22 (27.4%) | 1 (1.4%) | <0.0001 |
| Revision | 11 (17.5%) | 4 (5.6%) | 0.02 |
| Median follow-up (months) | 25.5 (IQR: 8–55) | 12.2 (IQR: 4–22) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dubois, A.; Capon, G.; Belas, O.; Vidart, A.; Manunta, A.; Hascoet, J.; Freton, L.; Thibault, F.; Cardot, V.; Dubois, F.; et al. Open vs. Robot-Assisted Artificial Urinary Sphincter Implantation in Women with Stress Urinary Incontinence: A Multicenter Comparative Study. J. Clin. Med. 2025, 14, 284. https://doi.org/10.3390/jcm14010284
Dubois A, Capon G, Belas O, Vidart A, Manunta A, Hascoet J, Freton L, Thibault F, Cardot V, Dubois F, et al. Open vs. Robot-Assisted Artificial Urinary Sphincter Implantation in Women with Stress Urinary Incontinence: A Multicenter Comparative Study. Journal of Clinical Medicine. 2025; 14(1):284. https://doi.org/10.3390/jcm14010284
Chicago/Turabian StyleDubois, Alexandre, Grégoire Capon, Olivier Belas, Adrien Vidart, Andrea Manunta, Juliette Hascoet, Lucas Freton, Frederic Thibault, Vincent Cardot, Frédéric Dubois, and et al. 2025. "Open vs. Robot-Assisted Artificial Urinary Sphincter Implantation in Women with Stress Urinary Incontinence: A Multicenter Comparative Study" Journal of Clinical Medicine 14, no. 1: 284. https://doi.org/10.3390/jcm14010284
APA StyleDubois, A., Capon, G., Belas, O., Vidart, A., Manunta, A., Hascoet, J., Freton, L., Thibault, F., Cardot, V., Dubois, F., Corbel, L., Della Negra, E., Haab, F., Peyrat, L., Cornu, J.-N., Grise, P., Descazeaud, A., Fournier, G., & Peyronnet, B. (2025). Open vs. Robot-Assisted Artificial Urinary Sphincter Implantation in Women with Stress Urinary Incontinence: A Multicenter Comparative Study. Journal of Clinical Medicine, 14(1), 284. https://doi.org/10.3390/jcm14010284