
Efficacy and Complication Rates of Percutaneous Vertebroplasty and Kyphoplasty in the Treatment of Vertebral Compression Fractures: A Retrospective Analysis of 280 Patients



Abstract
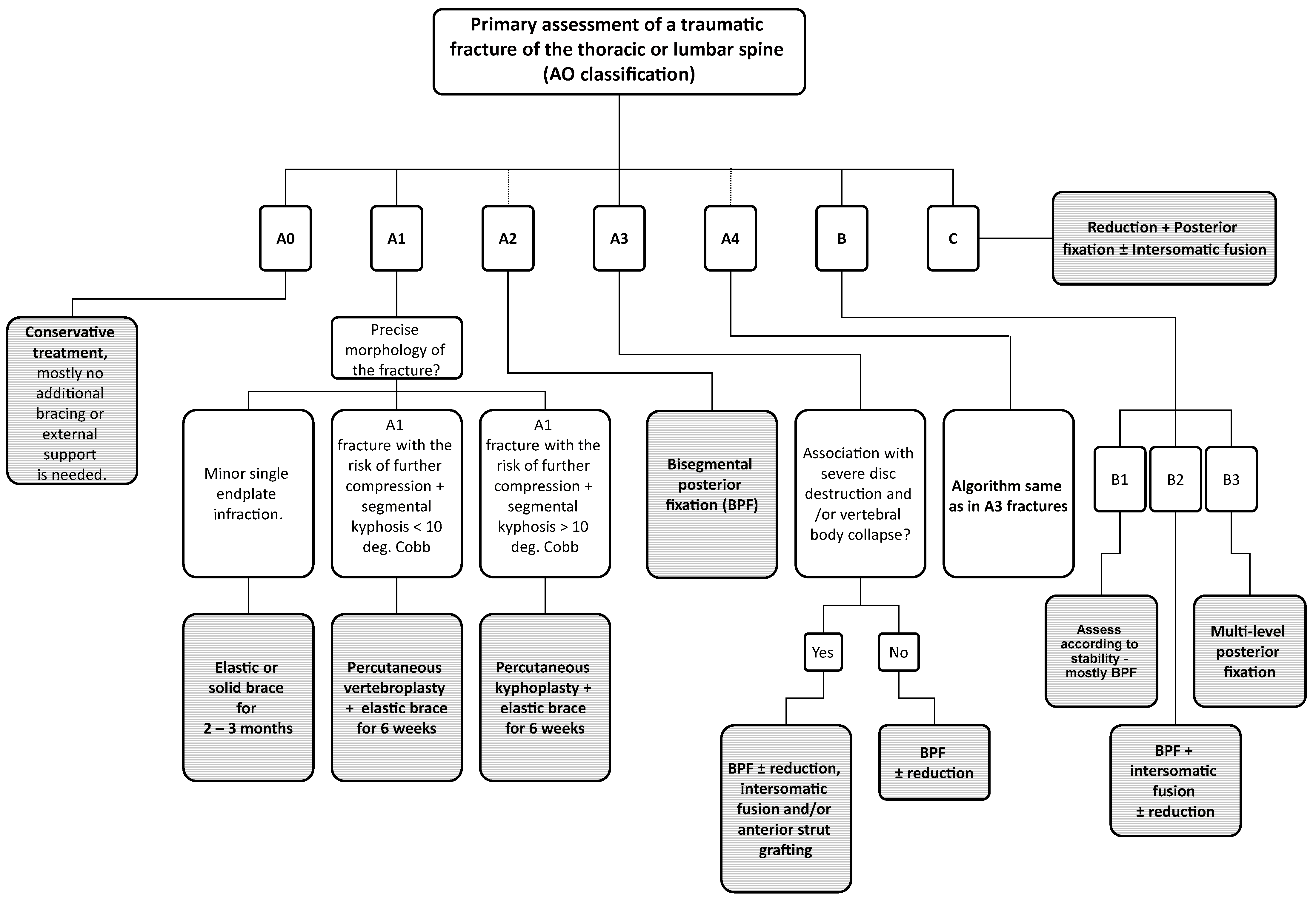
1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
2.2. Surgical Technique
2.3. Statistical Analysis
2.4. Follow-Up
3. Results
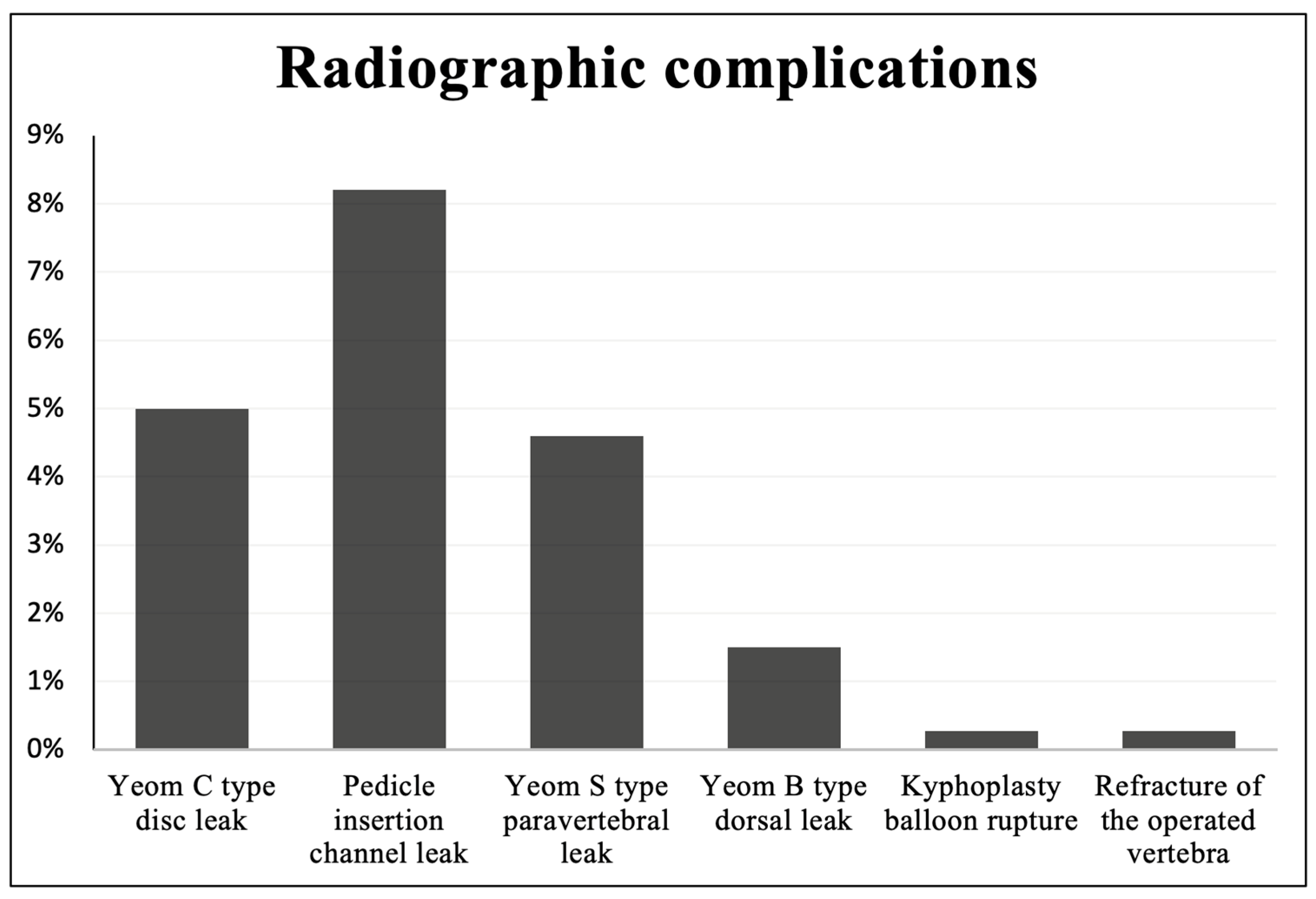
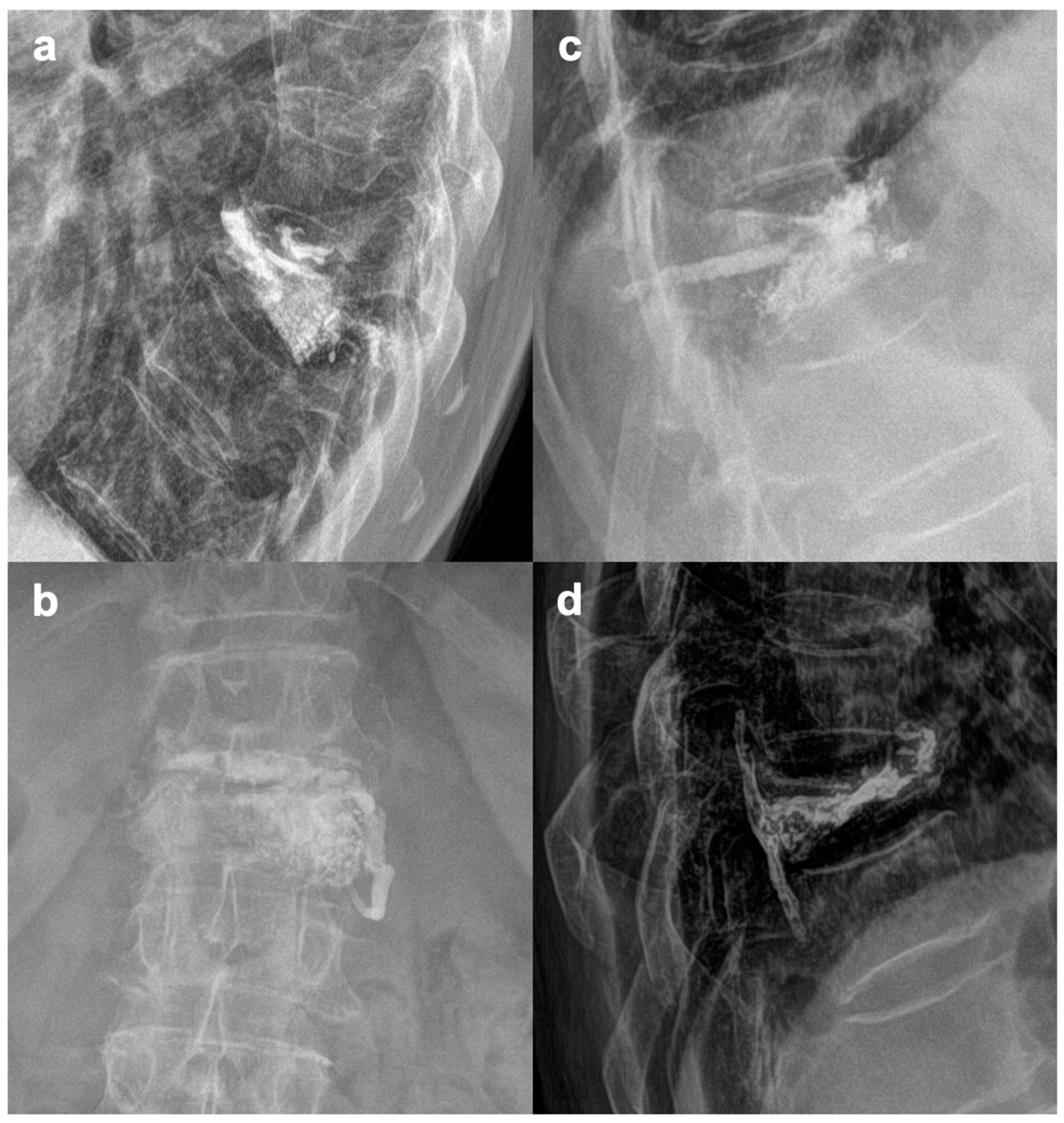
3.1. Spectrum of Registered Complications
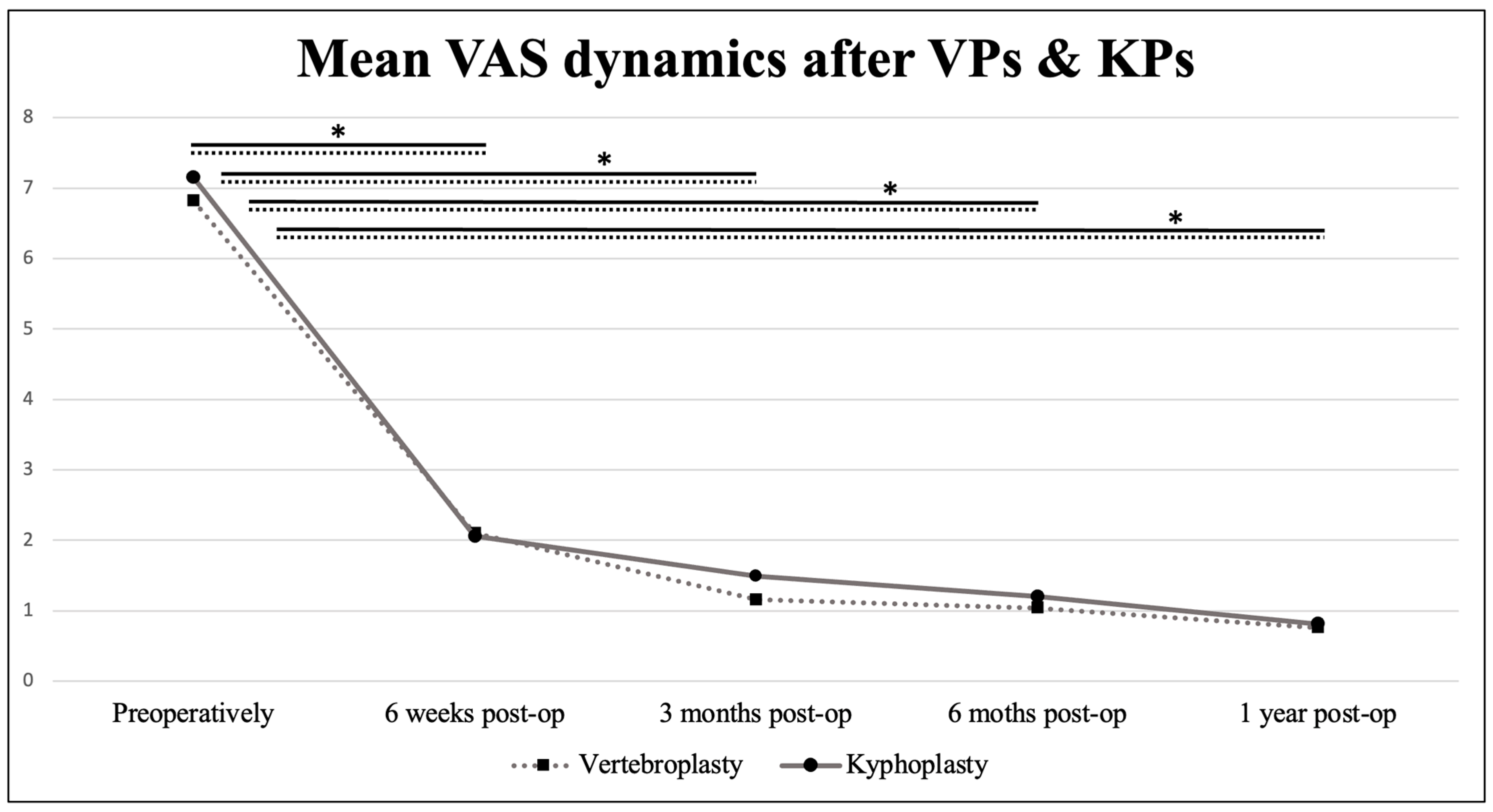
3.2. VAS Scores and Clinical Outcomes
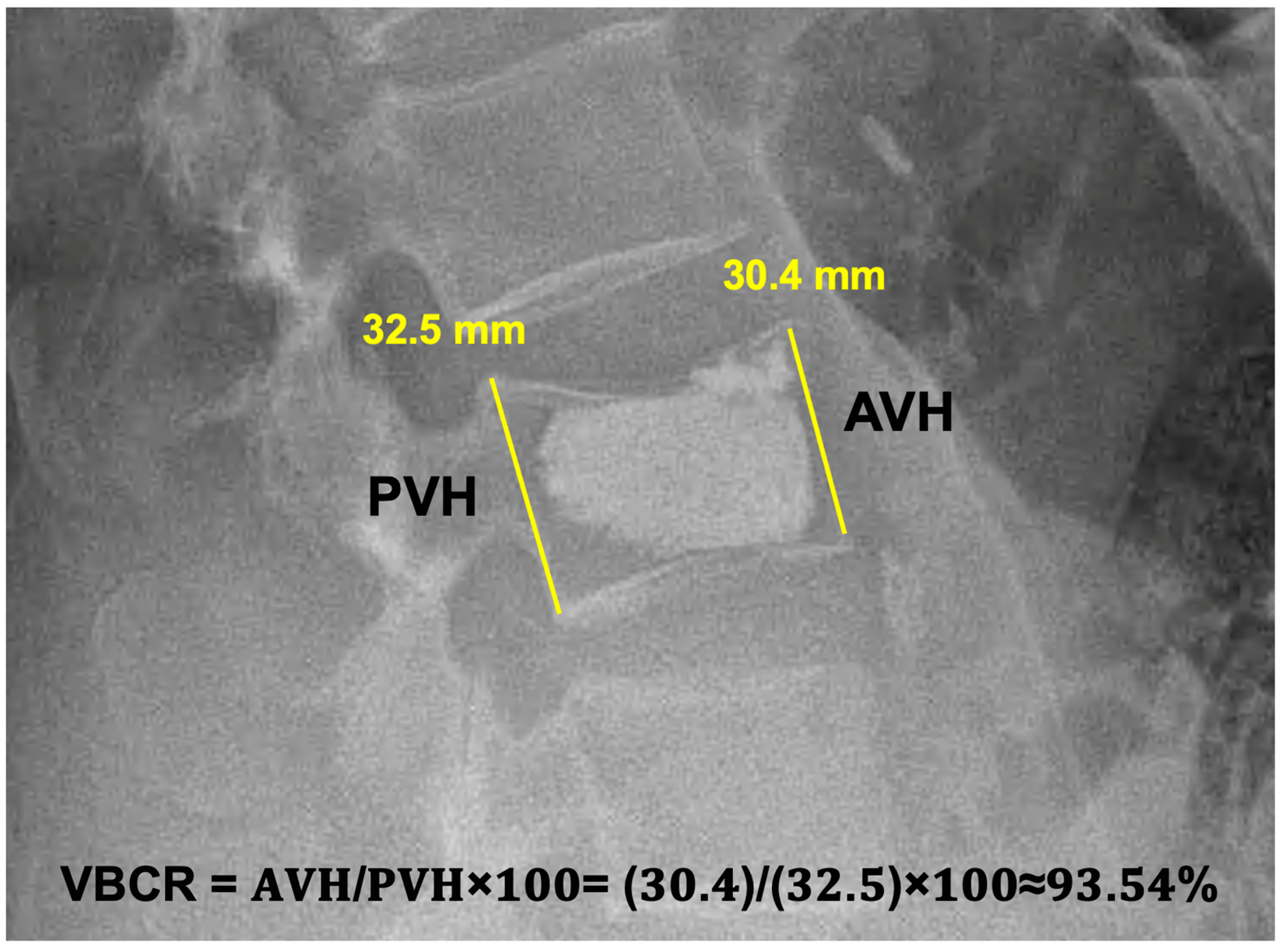
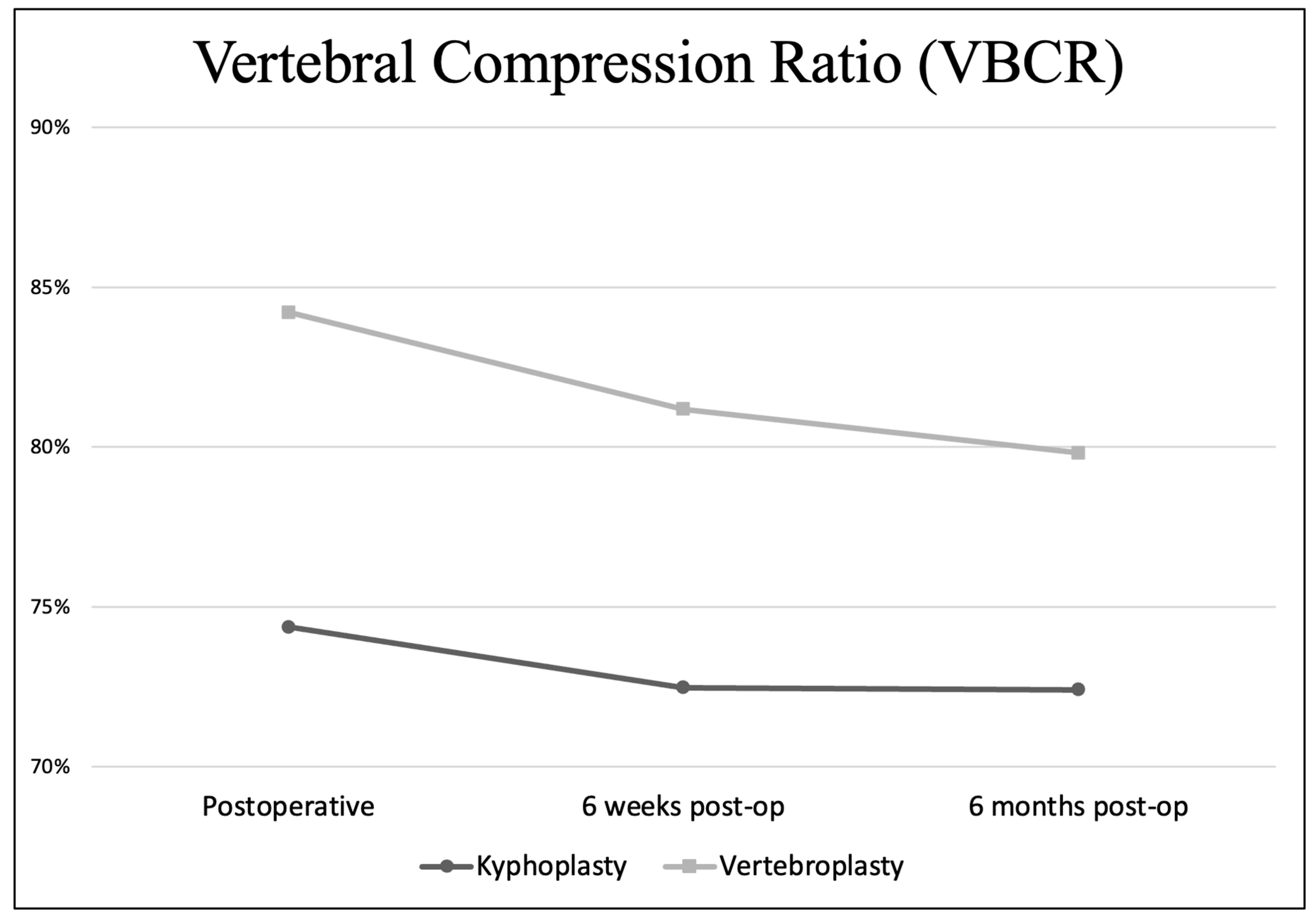
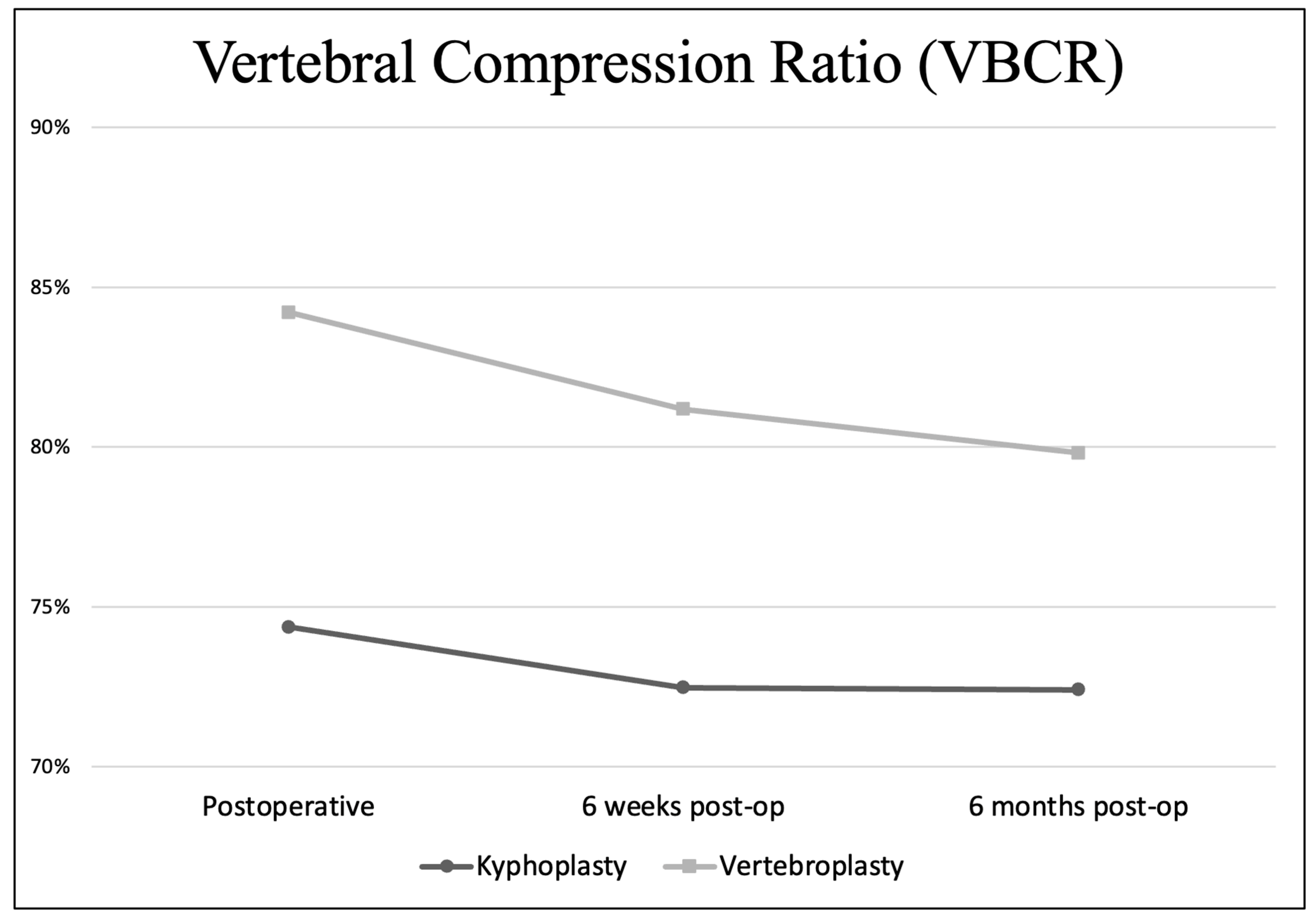
3.3. Development of VBCR through the Follow-Up
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Divi, S.N.; Schroeder, G.D.; Oner, F.C.; Kandziora, F.; Schnake, K.J.; Dvorak, M.F.; Benneker, L.M.; Chapman, J.R.; Vaccaro, A.R. AO Spine-Spine Trauma Classification System: The Value of Modifiers: A Narrative Review with Commentary on Evolving Descriptive Principles. Glob. Spine J. 2019, 9 (Suppl. S1), 77S–88S. [Google Scholar] [CrossRef]
- Kushchayev, S.V.; Wiener, P.C.; Teytelboym, O.M.; Arrington, J.A.; Khan, M.; Preul, M.C. Percutaneous Vertebroplasty: A History of Procedure, Technology, Culture, Specialty, and Economics. Neuroimaging Clin. N. Am. 2019, 29, 481–494. [Google Scholar] [CrossRef] [PubMed]
- Tomé-Bermejo, F.; Piñera, A.R.; Duran-Álvarez, C.; Román, B.L.; Mahillo, I.; Alvarez, L.; Pérez-Higueras, A. Identification of Risk Factors for the Occurrence of Cement Leakage During Percutaneous Vertebroplasty for Painful Osteoporotic or Malignant Vertebral Fracture. Spine 2014, 39, E693–E700. [Google Scholar] [CrossRef] [PubMed]
- Filippiadis, D.K.; Marcia, S.; Masala, S.; Deschamps, F.; Kelekis, A. Percutaneous Vertebroplasty and Kyphoplasty: Current Status, New Developments and Old Controversies. Cardiovasc. Interv. Radiol. 2017, 40, 1815–1823. [Google Scholar] [CrossRef]
- Noguchi, T.; Yamashita, K.; Kamei, R.; Maehara, J. Current status and challenges of percutaneous vertebroplasty (PVP). Jpn. J. Radiol. 2023, 41, 1–13. [Google Scholar] [CrossRef]
- Cao, J.; Kong, L.; Meng, F.; Zhang, Y.; Shen, Y. Risk factors for new vertebral compression fractures after vertebroplasty: A meta-analysis. ANZ J. Surg. 2016, 86, 549–554. [Google Scholar] [CrossRef]
- Telera, S.; Raus, L.; Pipola, V.; De Iure, F.; Gasbarrini, A. Vertebral Body Augmentation, Vertebroplasty and Kyphoplasty in Spine Surgery; Springer: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Hsu, W.E.; Su, K.C.; Chen, K.H.; Pan, C.C.; Lu, W.H.; Lee, C.H. The Evaluation of Different Radiological Measurement Parameters of the Degree of Collapse of the Vertebral Body in Vertebral Compression Fractures. Appl. Bionics Biomech. 2019, 2019, 4021640. [Google Scholar] [CrossRef] [PubMed]
- Rebolledo, B.J.; Gladnick, B.P.; Unnanuntana, A.; Nguyen, J.T.; Kepler, C.K.; Lane, J.M. Comparison of unipedicular and bipedicular balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Bone Jt. J. 2013, 95, 401–406. [Google Scholar] [CrossRef]
- Lee, C.H.; Kim, H.J.; Lee, M.K.; Kim, H.S.; Choi, S.S. Comparison of efficacies of unipedicular kyphoplasty and bipedicular kyphoplasty for treatment of single-level osteoporotic vertebral compression fractures. Medicine 2020, 99, e22046. [Google Scholar] [CrossRef]
- Yan, L.; Jiang, R.; He, B.; Liu, T.; Hao, D. A Comparison Between Unilateral Transverse Process-Pedicle and Bilateral Puncture Techniques in Percutaneous Kyphoplasty. Spine 2014, 39, B19–B26. [Google Scholar] [CrossRef]
- Son, S.; Lee, S.G.; Kim, W.K.; Park, C.W.; Yoo, C.J. Early Vertebroplasty versus Delayed Vertebroplasty for Acute Osteoporotic Compression Fracture: Are the Results of the Two Surgical Strategies the Same? J. Korean Neurosurg. Soc. 2014, 56, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Xu, J.; Wang, Q. Timing of Percutaneous Balloon Kyphoplasty for Osteoporotic Vertebral Compression Fractures. Pain Physician 2023, 26, 231–243. [Google Scholar] [PubMed]
- Zhang, J.; Fan, Y.; He, X.; Du, J.; Hao, D. Bracing after percutaneous vertebroplasty for thoracolumbar osteoporotic vertebral compression fractures was not effective. Clin. Interv. Aging 2019, 14, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Zhu, N.; Zhang, H.; Hao, D. Vertebral refracture after percutaneous vertebroplasty for osteoporotic vertebral compression fractures with and without brace wearing: A retrospective study of 300 patients. Front. Surg. 2023, 9, 1056729. [Google Scholar] [CrossRef]
- Kato, T.; Inose, H.; Ichimura, S.; Tokuhashi, Y.; Nakamura, H.; Hoshino, M.; Togawa, D.; Hirano, T.; Haro, H.; Ohba, T.; et al. Comparison of Rigid and Soft-Brace Treatments for Acute Osteoporotic Vertebral Compression Fracture: A Prospective, Randomized, Multicenter Study. J. Clin. Med. 2019, 8, 198. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Liu, T.; Yin, P.; Wang, Y.; Liao, S.; Zhang, S.; Su, Q.; Hai, Y. The therapeutic effects of percutaneous kyphoplasty on osteoporotic vertebral compression fractures with or without intravertebral cleft. Int. Orthop. 2019, 43, 359–365. [Google Scholar] [CrossRef]
- Zhu, S.Y.; Zhong, Z.M.; Wu, Q.; Chen, J.T. Risk factors for bone cement leakage in percutaneous vertebroplasty: A retrospective study of four hundred and eighty five patients. Int. Orthop. 2016, 40, 1205–1210. [Google Scholar] [CrossRef]
- Liu, J.T.; Li, C.; Chang, C.S.; Liao, W.J. Long-term follow-up study of osteoporotic vertebral compression fracture treated using balloon kyphoplasty and vertebroplasty. J. Neurosurg. Spine 2015, 23, 94–98. [Google Scholar] [CrossRef]
- de Falco, R.; Bocchetti, A. Balloon kyphoplasty for pure traumatic thoracolumbar fractures: Retrospective analysis of 61 cases focusing on restoration of vertebral height. Eur. Spine J. 2014, 23 (Suppl. S6), 664–670. [Google Scholar] [CrossRef]
- Bonnard, E.; Foti, P.; Kastler, A.; Amoretti, N. Percutaneous vertebroplasty under local anaesthesia: Feasibility regarding patients’ experience. Eur. Radiol. 2017, 27, 1512–1516. [Google Scholar] [CrossRef]
- Li, Y.X.; Guo, D.Q.; Zhang, S.C.; Liang, D.; Yuan, K.; Mo, G.Y.; Li, D.X.; Guo, H.Z.; Tang, Y.; Luo, P.J. Risk factor analysis for re-collapse of cemented vertebrae after percutaneous vertebroplasty (PVP) or percutaneous kyphoplasty (PKP). Int. Orthop. 2018, 42, 2131–2139. [Google Scholar] [CrossRef] [PubMed]
- Seuvic, F.M.; Gillet, R.; Louis, M.; Germain, É.; Lombard, C.; Blum, A.; Gondim Teixeira, P.A. Association between opportunistic vertebral bone density measurements and new vertebral fractures after percutaneous vertebral cementoplasty: A case-control study. Eur. Radiol. 2023, 33, 106–115. [Google Scholar] [CrossRef]
- Schousboe, J.T.; Lix, L.M.; Morin, S.N.; Derkatch, S.; Bryanton, M.; Alhrbi, M.; Leslie, W.D. Prevalent vertebral fracture on bone density lateral spine (VFA) images in routine clinical practice predict incident fractures. Bone 2019, 121, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Saracen, A.; Kotwica, Z. Complications of percutaneous vertebroplasty. Medicine 2016, 95, e3850. [Google Scholar] [CrossRef]
- Wang, C.H.; Ma, J.Z.; Zhang, C.C.; Nie, L. Comparison of high-viscosity cement vertebroplasty and balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Pain Physician 2015, 18, E187–E194. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level Distribution of the Operated Fractures | Type of Fracture (AO Classification) | ||
|---|---|---|---|
| Th8 Th9 Th10 Th11 Th12 L1 L2 L3 L4 | 3 cases (1%) 1 case (0.4%) 4 cases (2%) 20 cases (7%) 71 cases (25%) 100 cases (36%) 47 cases (17%) 25 cases (9%) 9 cases (3%) | A1 | 228 cases (82%) |
| A3 | 50 cases (18%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerny, J.; Soukup, J.; Petrosian, K.; Loukotova, L.; Novotny, T. Efficacy and Complication Rates of Percutaneous Vertebroplasty and Kyphoplasty in the Treatment of Vertebral Compression Fractures: A Retrospective Analysis of 280 Patients. J. Clin. Med. 2024, 13, 1495. https://doi.org/10.3390/jcm13051495
Cerny J, Soukup J, Petrosian K, Loukotova L, Novotny T. Efficacy and Complication Rates of Percutaneous Vertebroplasty and Kyphoplasty in the Treatment of Vertebral Compression Fractures: A Retrospective Analysis of 280 Patients. Journal of Clinical Medicine. 2024; 13(5):1495. https://doi.org/10.3390/jcm13051495
Chicago/Turabian StyleCerny, Jan, Jan Soukup, Kadzhik Petrosian, Lucie Loukotova, and Tomas Novotny. 2024. "Efficacy and Complication Rates of Percutaneous Vertebroplasty and Kyphoplasty in the Treatment of Vertebral Compression Fractures: A Retrospective Analysis of 280 Patients" Journal of Clinical Medicine 13, no. 5: 1495. https://doi.org/10.3390/jcm13051495
APA StyleCerny, J., Soukup, J., Petrosian, K., Loukotova, L., & Novotny, T. (2024). Efficacy and Complication Rates of Percutaneous Vertebroplasty and Kyphoplasty in the Treatment of Vertebral Compression Fractures: A Retrospective Analysis of 280 Patients. Journal of Clinical Medicine, 13(5), 1495. https://doi.org/10.3390/jcm13051495