
Effect of Mirror Therapy on Post-Needling Pain Following Deep Dry Needling of Myofascial Trigger Point in Lateral Elbow Pain: Prospective Controlled Pilot Trial
 ,
,  , , , ,
, , , ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
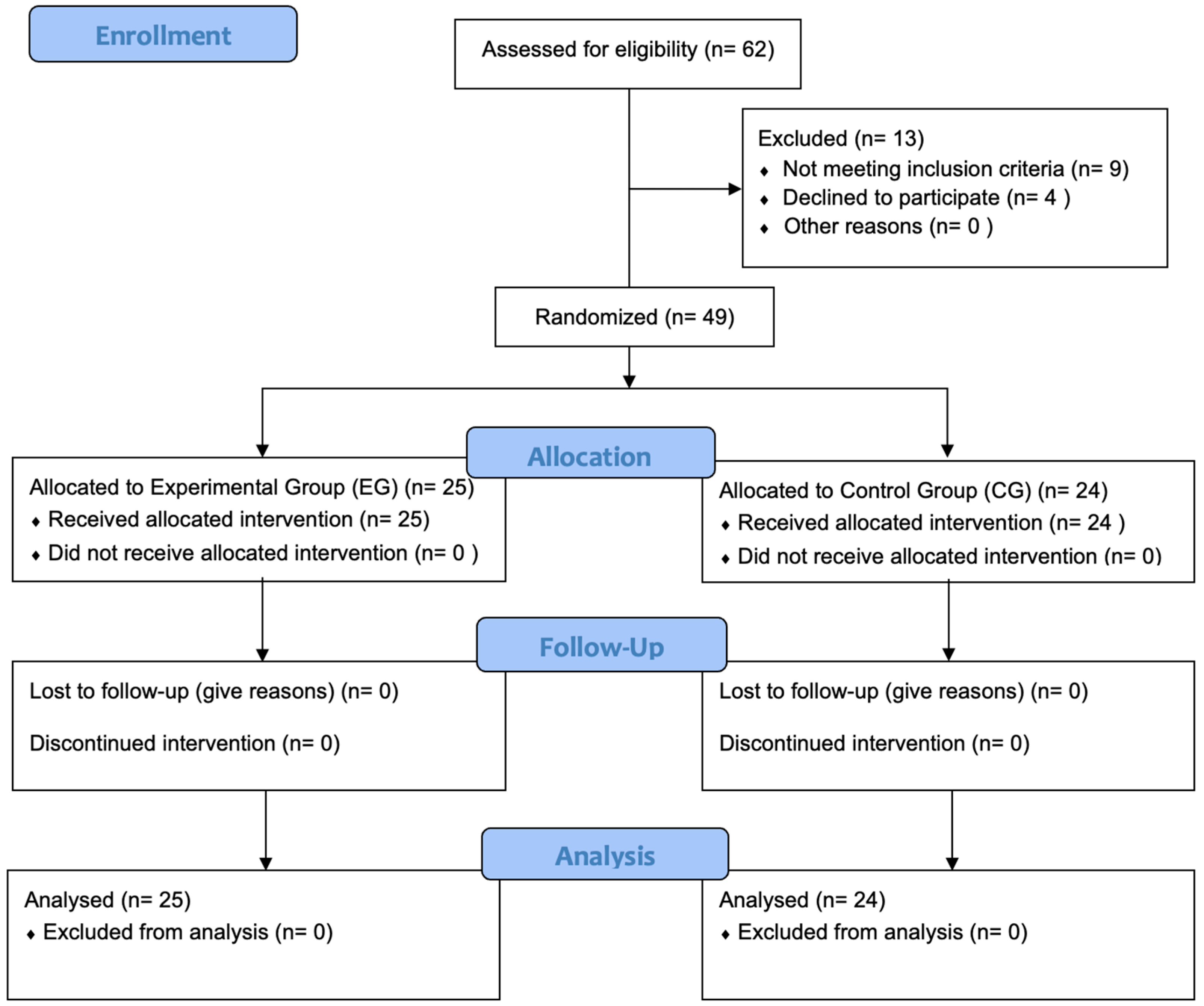
2.1. Study Design
2.2. Participants
2.3. Sample Size Determination
2.4. Randomized Allocation
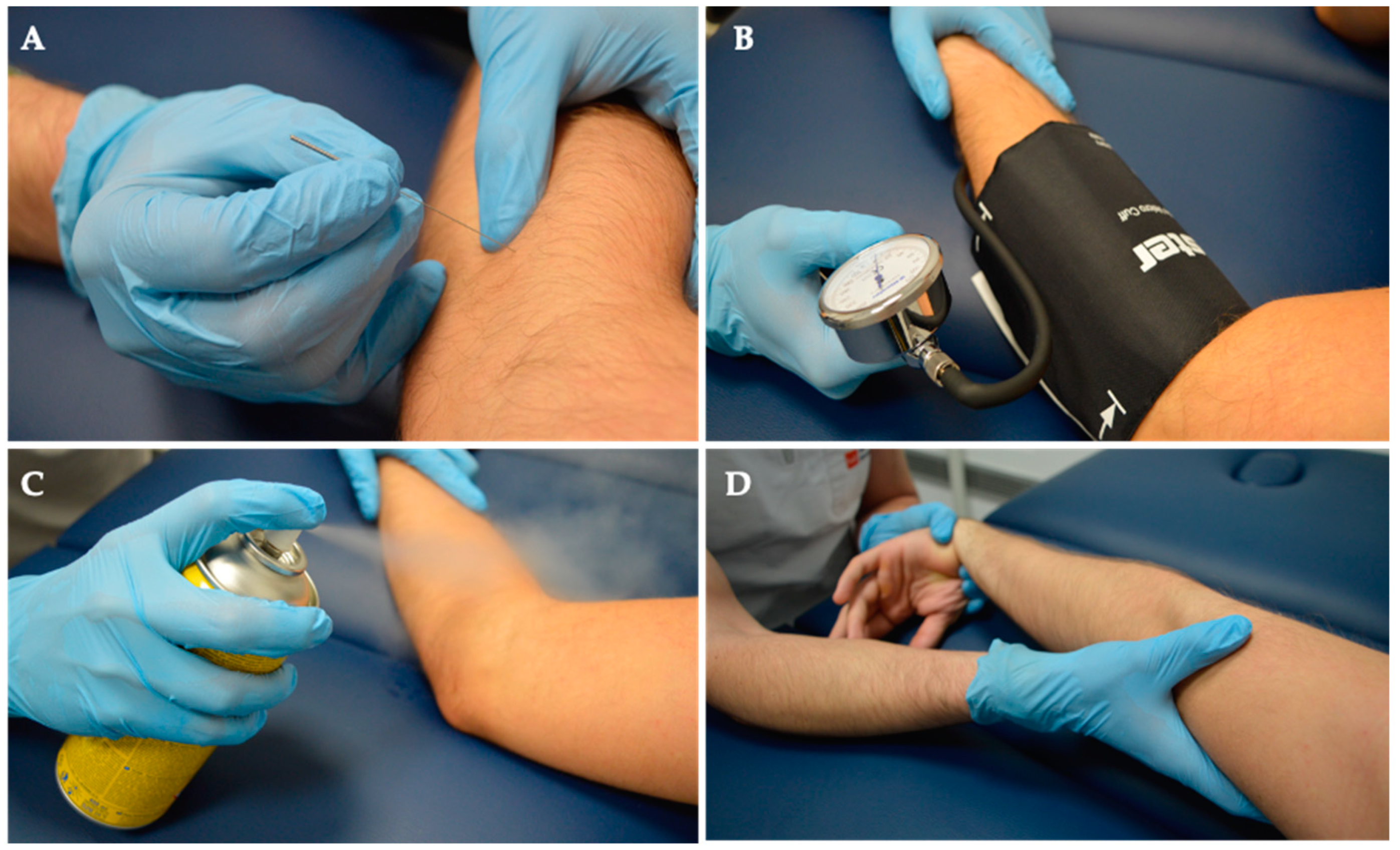
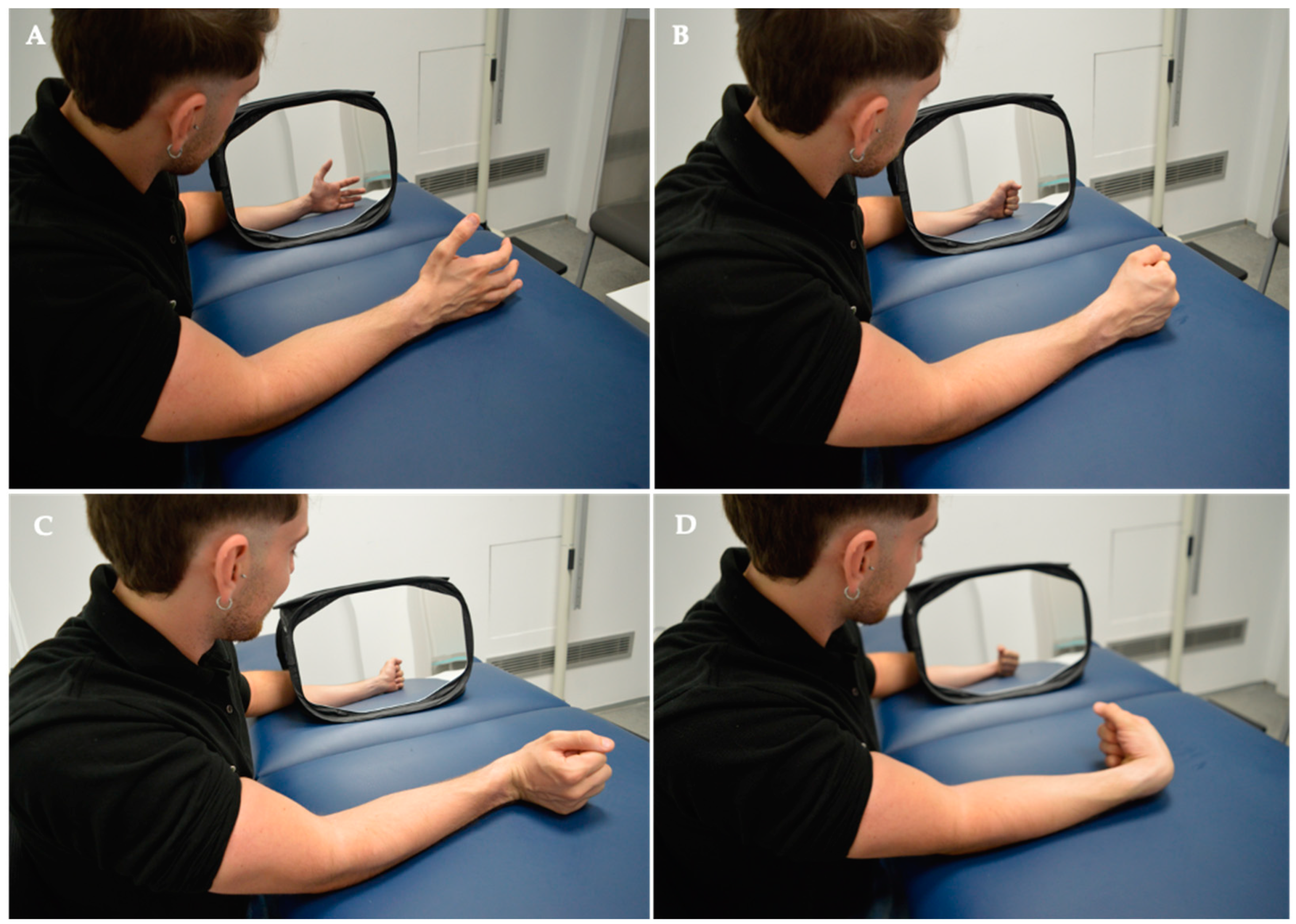
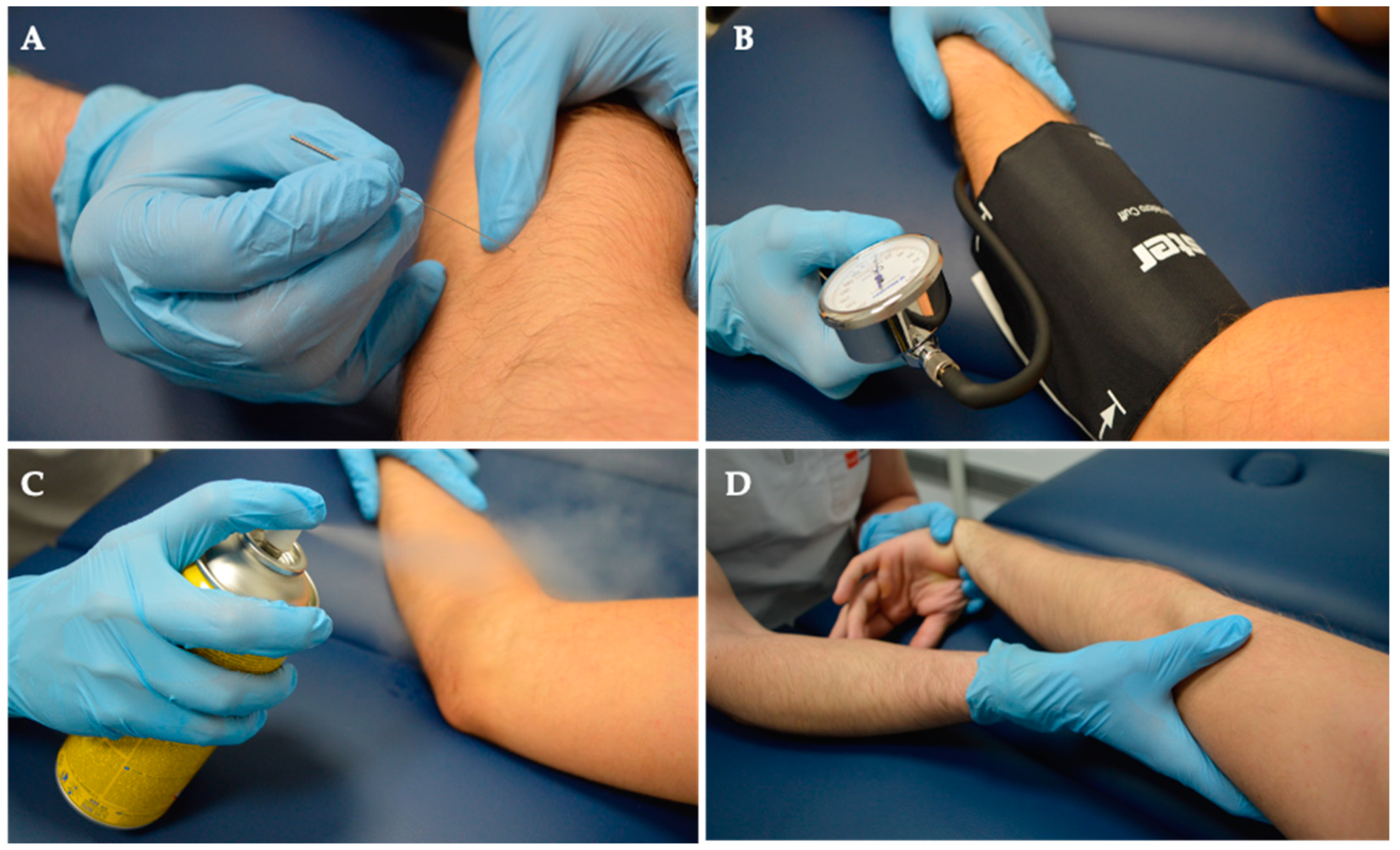
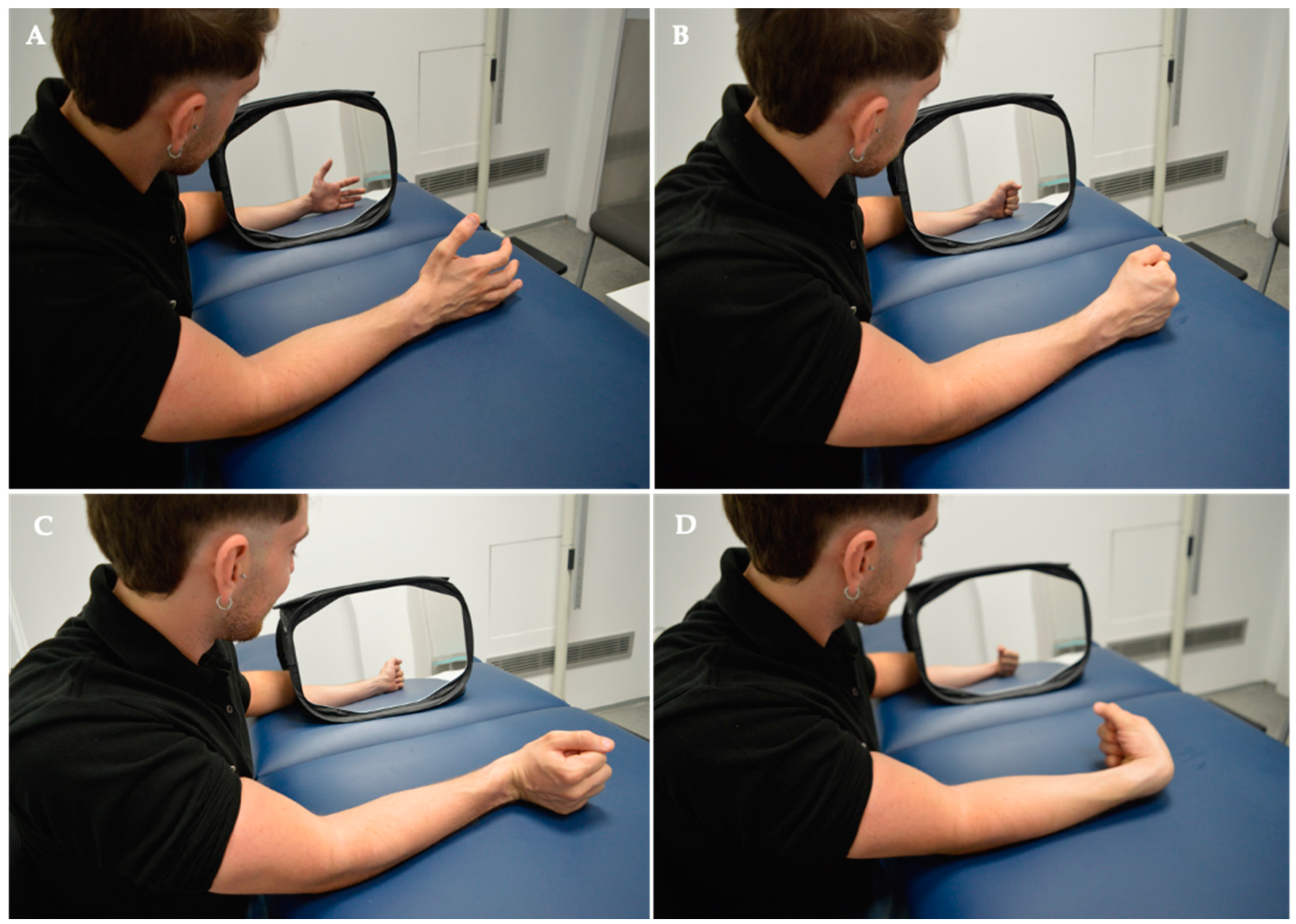
2.5. Intervention
2.6. Outcome Measures
2.7. Statistical Analysis
3. Results
3.1. Demographic Description of the Sample
3.2. Description of Study Variables
3.3. Main Findings
3.3.1. Intra-Group Differences
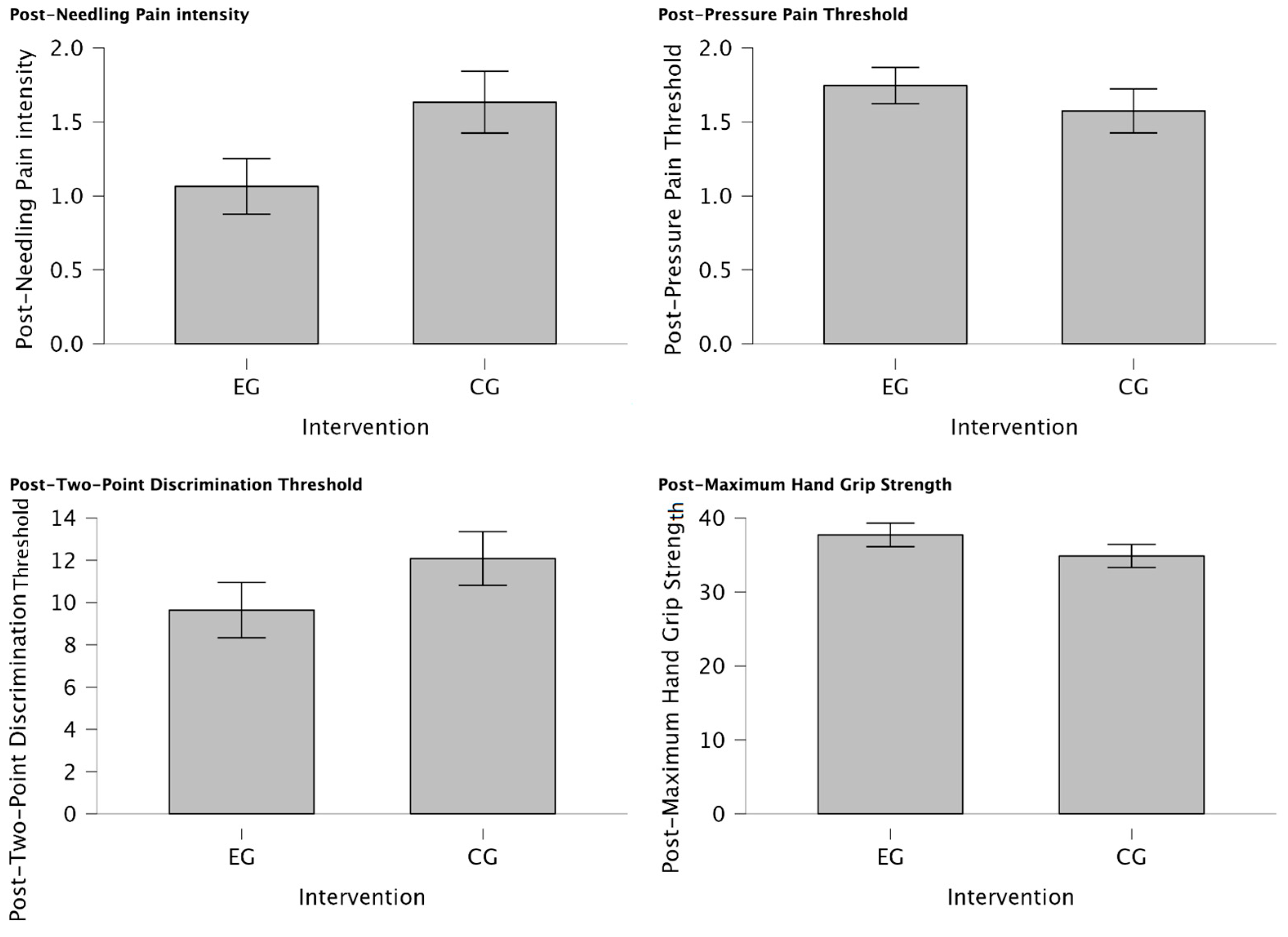
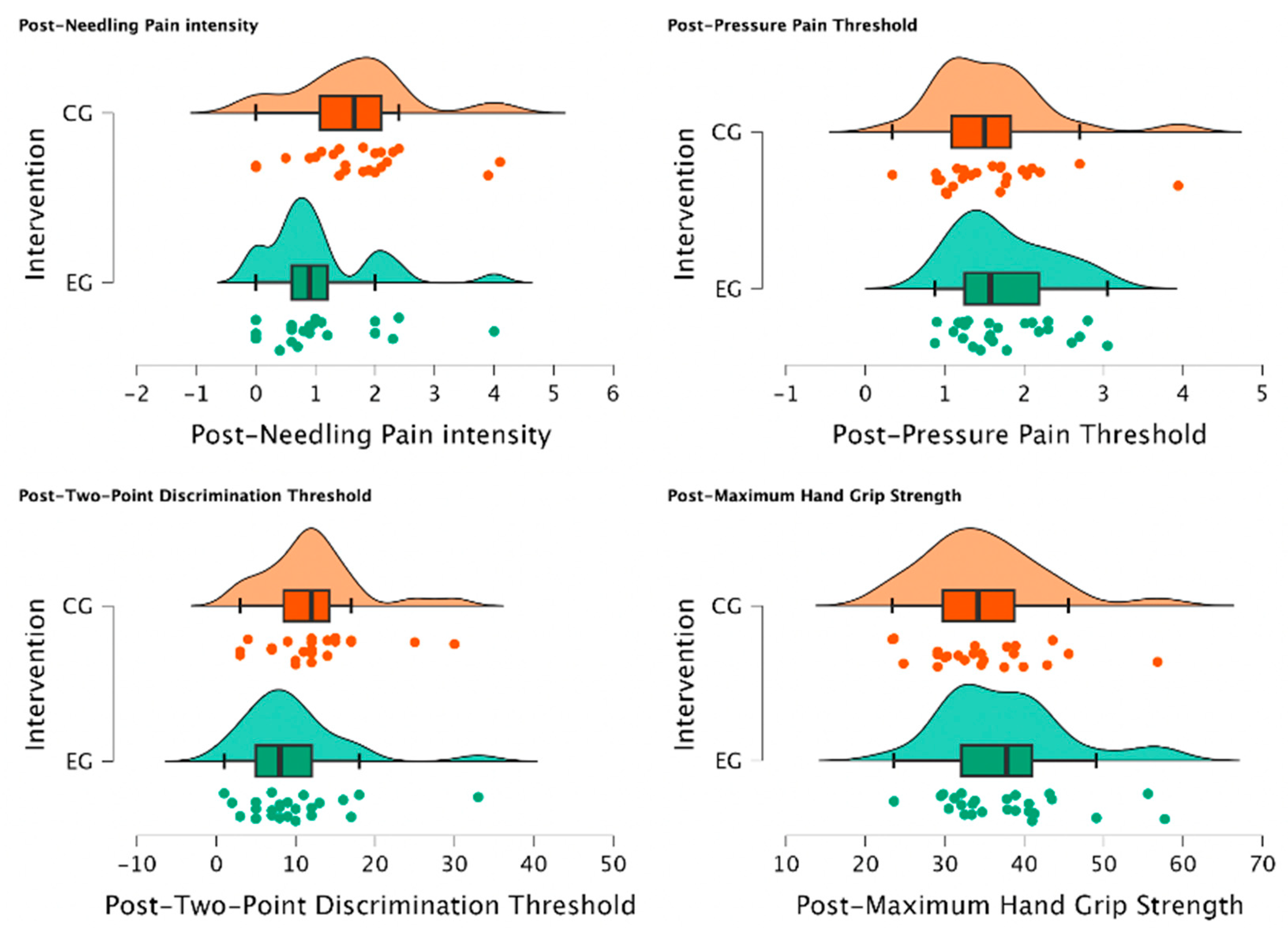
3.3.2. Inter-Group Differences
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martín-Pintado-Zugasti, A.; Pecos-Martin, D.; Rodríguez-Fernández, Á.L.; Alguacil-Diego, I.M.; Portillo-Aceituno, A.; Gallego-Izquierdo, T.; Fernandez-Carnero, J. Ischemic Compression After Dry Needling of a Latent Myofascial Trigger Point Reduces Post-Needling Soreness Intensity and Duration. PM&R 2015, 7, 1026–1034. [Google Scholar] [CrossRef]
- Dommerholt, J. Dry needling–peripheral and central considerations. J. Man. Manip. Ther. 2011, 19, 223–227. [Google Scholar] [CrossRef]
- Simons, D.G. Symptomatology and clinical pathophysiology of myofascial pain. Schmerz 1991, 5, 29–37. [Google Scholar] [CrossRef]
- Shushkevich, Y.; Kalichman, L. Myofascial pain in lateral epicondylalgia: A review. J. Bodyw. Mov. Ther. 2013, 17, 434–439. [Google Scholar] [CrossRef]
- Kuan, T.S.; Hong, C.Z.; Chen, J.T.; Chen, S.M.; Chien, C.H. The spinal cord connections of the myofascial trigger spots. Eur. J. Pain 2007, 11, 624–634. [Google Scholar] [CrossRef]
- Borg-Stein, J.; Iaccarino, M.A. Myofascial pain syndrome treatments. Phys. Med. Rehabil. Clin. N. Am. 2014, 25, 357–374. [Google Scholar] [CrossRef]
- Urits, I.; Charipova, K.; Gress, K.; Schaaf, A.L.; Gupta, S.; Kiernan, H.C.; Choi, P.E.; Jung, J.W.; Cornett, E.; Kaye, A.D.; et al. Treatment and management of myofascial pain syndrome. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 427–448. [Google Scholar] [CrossRef]
- Cagnie, B.; Dewitte, V.; Barbe, T.; Timmermans, F.; Delrue, N.; Meeus, M. Physiologic effects of dry needling. Curr. Pain Headache Rep. 2013, 17, 348. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.Z.; Simons, D.G. Pathophysiologic and electrophysiologic mechanisms of myofascial trigger points. Arch. Phys. Med. Rehabil. 1998, 79, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Chou, L.W.; Hsieh, Y.L.; Kuan, T.S.; Hong, C.Z. Needling therapy for myofascial pain: Recommended technique with multiple rapid needle insertions. Biomedicine 2014, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Dommerholt, J. Myofascial trigger points: Peripheral or central phenomenon? Curr. Rheumatol. Rep. 2014, 16, 395. [Google Scholar] [CrossRef] [PubMed]
- Malanga, G.A.; Yan, N.; Stark, J. Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury. Postgrad. Med. 2015, 127, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Li, J.; Tian, Y.; Lu, X. Effect of ischemic compression on myofascial pain syndrome: A systematic review and meta-analysis. Chiropr. Man. Therap. 2022, 30, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Mense, S. How Do Muscle Lesions such as Latent and Active Trigger Points Influence Central Nociceptive Neurons? J. Musculoskelet. Pain. 2010, 18, 348–353. [Google Scholar] [CrossRef]
- Walder, R.Y.; Rasmussen, L.A.; Rainier, J.D.; Light, A.R.; Wemmie, J.A.; Sluka, K.A. ASIC1 and ASIC3 play different roles in the development of Hyperalgesia after inflammatory muscle injury. J. Pain 2010, 11, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Wemmie, J.A.; Taugher, R.J.; Kreple, C.J. Acid-sensing ion channels in pain and disease. Nat. Rev. Neurosci. 2013, 14, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Lázaro-Navas, I.; Lorenzo-Sánchez-Aguilera, C.; Pecos-Martín, D.; Jiménez-Rejano, J.J.; Navarro-Santana, M.J.; Fernández-Carnero, J.; Gallego-Izquierdo, T. Immediate Effects of Dry Needling on the Autonomic Nervous System and Mechanical Hyperalgesia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 6018. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Carnero, J.; Gilarranz-de-Frutos, L.; León-Hernández, J.V.; Pecos-Martin, D.; Alguacil-Diego, I.; Gallego-Izquierdo, T.; Martín-Pintado-Zugasti, A. Effectiveness of Different Deep Dry Needling Dosages in the Treatment of Patients with Cervical Myofascial Pain: A Pilot RCT. Am. J. Phys. Med. Rehabil. 2017, 96, 726–733. [Google Scholar] [CrossRef]
- Chys, M.; De Meulemeester, K.; De Greef, I.; Murillo, C.; Kindt, W.; Kouzouz, Y.; Lescroart, B.; Cagnie, B. Clinical Effectiveness of Dry Needling in Patients with Musculoskeletal Pain-An Umbrella Review. J. Clin. Med. 2023, 12, 1205. [Google Scholar] [CrossRef]
- Chou, L.W.; Kao, M.J.; Lin, J.G. Probable mechanisms of needling therapies for myofascial pain control. Evid. Based Complement. Alternat. Med. 2012, 2012, 705327. [Google Scholar] [CrossRef]
- Hsieh, Y.L.; Yang, S.A.; Yang, C.C.; Chou, L.W. Dry needling at myofascial trigger spots of rabbit skeletal muscles modulates the biochemicals associated with pain, inflammation, and hypoxia. Evid. Based Complement. Alternat. Med. 2012, 2012, 342165. [Google Scholar] [CrossRef]
- Korkmaz, M.D.; Medin Ceylan, C. Effect of dry-needling and exercise treatment on myofascial trigger point: A single-blind randomized controlled trial. Complement Ther Clin Pract. 2022, 47, 101571. [Google Scholar] [CrossRef]
- Perreault, T.; Dunning, J.; Butts, R. The local twitch response during trigger point dry needling: Is it necessary for successful outcomes? J. Bodyw. Mov. Ther. 2017, 21, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Gilliams, E.A. Uncovering the biochemical milieu of myofascial trigger points using in vivo microdialysis: An application of muscle pain concepts to myofascial pain syndrome. J. Bodyw. Mov. Ther. 2008, 12, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Myburgh, C.; Hartvigsen, J.; Aagaard, P.; Holsgaard-Larsen, A. Skeletal muscle contractility, self-reported pain and tissue sensitivity in females with neck/shoulder pain and upper Trapezius myofascial trigger points- a randomized intervention study. Chiropr Man Therap. 2012, 20, 36. [Google Scholar] [CrossRef] [PubMed]
- León-Hernández, J.V.; Martín-Pintado-Zugasti, A.; Frutos, L.G.; Alguacil-Diego, I.M.; de la Llave-Rincón, A.I.; Fernandez-Carnero, J. Immediate and short-term effects of the combination of dry needling and percutaneous TENS on post-needling soreness in patients with chronic myofascial neck pain. Braz. J. Phys. Ther. 2016, 20, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Vorawanthanachai, T. Factors Associated with Immediate Post-needling Soreness after Dry Needling at Upper Trapezius Muscle in Patients with Myofascial Pain syndrome. ASEAN J. Rehabil. Med. 2023, 33, 23–27. [Google Scholar]
- Martín-Pintado-Zugasti, A.; Mayoral Del Moral, O.; Gerwin, R.D.; Fernández-Carnero, J. Post-needling soreness after myofascial trigger point dry needling: Current status and future research. J. Bodyw. Mov. Ther. 2018, 22, 941–946. [Google Scholar] [CrossRef]
- Cheng, H.T. Spinal cord mechanisms of chronic pain and clinical implications. Curr. Pain Headache Rep. 2010, 14, 213–220. [Google Scholar] [CrossRef]
- Comitato, A.; Bardoni, R. Presynaptic Inhibition of Pain and Touch in the Spinal Cord: From Receptors to Circuits. Int. J. Mol. Sci. 2021, 22, 414. [Google Scholar] [CrossRef]
- López-Royo, M.P.; Pedersini, P.; Cantero-Téllez, R.; Valdes, K.; Doménech-García, V.; Herrero, P.; Villafañe, J.H. Effects of Ischemic Compression on Trigger Points in the First Dorsal Interosseous Muscle in Patients with Thumb Carpometacarpal Osteoarthritis. Int. J. Environ. Res. Public Health 2021, 18, 2961. [Google Scholar] [CrossRef] [PubMed]
- Martín-Pintado Zugasti, A.; Rodríguez-Fernández, Á.L.; García-Muro, F.; López-López, A.; Mayoral, O.; Mesa-Jiménez, J.; Fernández-Carnero, J. Effects of spray and stretch on postneedling soreness and sensitivity after dry needling of a latent myofascial trigger point. Arch. Phys. Med. Rehabil. 2014, 95, 1925–1932.e1. [Google Scholar] [CrossRef] [PubMed]
- McCabe, C. Mirror visual feedback therapy. A practical approach. J. Hand Ther. 2011, 24, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Rjosk, V.; Kaminski, E.; Hoff, M.; Sehm, B.; Steele, C.J.; Villringer, A.; Ragert, P. Mirror Visual Feedback-Induced Performance Improvement and the Influence of Hand Dominance. Front. Hum. Neurosci. 2016, 9, 702. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, Y.; Kodaka, K. Vision-Driven Kinesthetic Illusion in Mirror Visual Feedback. i-Perception 2018, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Huang, P.C.; Chen, Y.T.; Lin, K.C.; Yang, H.W. Effects of mirror therapy on motor and sensory recovery in chronic stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2013, 94, 1023–1030. [Google Scholar] [CrossRef]
- Tracey, I.; Mantyh, P.W. The cerebral signature for pain perception and its modulation. Neuron 2007, 55, 377–391. [Google Scholar] [CrossRef]
- Thieme, H.; Morkisch, N.; Rietz, C.; Dohle, C.; Borgetto, B. The Efficacy of Movement Representation Techniques for Treatment of Limb Pain--A Systematic Review and Meta-Analysis. J. Pain. 2016, 17, 167–180. [Google Scholar] [CrossRef]
- Deconinck, F.J.A.; Smorenburg, A.R.P.; Benham, A.; Ledebt, A.; Feltham, M.G.; Savelsbergh, G.J.P. Reflections on mirror therapy: A systematic review of the effect of mirror visual feedback on the brain. Neurorehabil. Neural. Repair. 2015, 29, 349–361. [Google Scholar] [CrossRef]
- Zhang, Y.; Xing, Y.; Li, C.; Hua, Y.; Hu, J.; Wang, Y.; Ya, R.; Meng, Q.; Bai, Y. Mirror therapy for unilateral neglect after stroke: A systematic review. Eur. J. Neurol. 2022, 29, 358–371. [Google Scholar] [CrossRef]
- Xie, H.M.; Zhang, K.X.; Wang, S.; Wang, N.; Wang, N.; Li, X.; Huang, L.P. Effectiveness of Mirror Therapy for Phantom Limb Pain: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2022, 103, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Ol, H.; Van Heng, Y.; Danielsson, L.; Husum, H. Mirror therapy for phantom limb and stump pain: A randomized controlled clinical trial in landmine amputees in Cambodia. Scand. J. Pain 2018, 18, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.; Shamseer, L.; Altman, D.G.; Weeks, L.; Peters, J.; Kober, T.; Dias, S.; Schulz, K.F.; Plint, A.C.; Moher, D. Consolidated standards of reporting trials (CONSORT) and the completeness of reporting of randomised controlled trials (RCTs) published in medical journals. Cochrane Database Syst. Rev. 2012, 11, MR000030. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Lee, J.S.; Hobden, E.; Stiell, I.G.; Wells, G.A. Clinically important change in the visual analog scale after adequate pain control. Acad. Emerg. Med. 2003, 10, 1128–1130. [Google Scholar] [CrossRef]
- Liu, Y.; Lin, L.; Xiong, Q.; Zeng, W.; Yu, L.; Hou, Y. Effect of mirror therapy on recovery of stroke survivors: A systematic review and network meta-analysis. Neurosci. Lett. 2018, 662, 292–300. [Google Scholar] [CrossRef]
- Mirela Cristina, L.; Matei, D.; Ignat, B.; Popescu, C.D. Mirror therapy enhances upper extremity motor recovery in stroke patients. Acta Neurol Belg. 2015, 15, 597–603. [Google Scholar] [CrossRef]
- Mulder, T. Motor imagery and action observation: Cognitive tools for rehabilitation. J. Neural. Transm. 2007, 114, 1265–1278. [Google Scholar] [CrossRef]
- Garry, M.I.; Loftus, A.; Summers, J.J. Mirror, mirror on the wall: Viewing a mirror reflection of unilateral hand movements facilitates ipsilateral M1 excitability. Exp. Brain Res. 2005, 163, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Watanabe, T.; Kuwabara, T.; Yunoki, K.; Chen, X.; Kubo, N.; Kirimoto, H. Excitability of the Ipsilateral Primary Motor Cortex During Unilateral Goal-Directed Movement. Front. Hum. Neurosci. 2021, 15, 617146. [Google Scholar] [CrossRef] [PubMed]
- Volz, M.S.; Suarez-Contreras, V.; Portilla, A.L.S.; Illigens, B.; Bermpohl, F.; Fregni, F. Movement observation-induced modulation of pain perception and motor cortex excitability. Clin. Neurophysiol. 2015, 126, 1204–1211. [Google Scholar] [CrossRef] [PubMed]
- Vidor, L.P.; Torres, I.L.; Medeiros, L.F.; Dussán-Sarria, J.A.; Dall’agnol, L.; Deitos, A.; Brietzke, A.; Laste, G.; Rozisky, J.R.; Fregni, F.; et al. Association of anxiety with intracortical inhibition and descending pain modulation in chronic myofascial pain syndrome. BMC Neurosci. 2014, 15, 42. [Google Scholar] [CrossRef] [PubMed]
- Iwanami, J.; Mutai, H.; Sagari, A.; Sato, M.; Kobayashi, M. Relationship between Corticospinal Excitability While Gazing at the Mirror and Motor Imagery Ability. Brain Sci. 2023, 13, 463. [Google Scholar] [CrossRef] [PubMed]
- Do, A.T.L.; Enax-Krumova, E.K.; Özgül, Ö.; Eitner, L.B.; Heba, S.; Tegenthoff, M.; Maier, C.; Höffken, O. Distraction by a cognitive task has a higher impact on electrophysiological measures compared with conditioned pain modulation. BMC Neurosci. 2020, 21, 53. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, P.; Petersson, K.M.; Ghatan, P.H.; Stone-Elander, S.; Ingvar, M. Pain-related cerebral activation is altered by a distracting cognitive task. Pain 2000, 85, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Moont, R.; Pud, D.; Sprecher, E.; Sharvit, G.; Yarnitsky, D. ‘Pain inhibits pain’ mechanisms: Is pain modulation simply due to distraction? Pain 2010, 150, 113–120. [Google Scholar] [CrossRef]
- Asefi Rad, A.; Wippert, P.M. Insights into pain distraction and the impact of pain catastrophizing on pain perception during different types of distraction tasks. Front. Pain Res. 2024, 5, 1266974. [Google Scholar] [CrossRef]
- Bisio, A.; Biggio, M.; Avanzino, L.; Ruggeri, P.; Bove, M. Kinaesthetic illusion shapes the cortical plasticity evoked by action observation. J. Physiol. 2019, 597, 3233–3245. [Google Scholar] [CrossRef]
- Bello, U.M.; Kranz, G.S.; Winser, S.J.; Chan, C.C.H. Neural Processes Underlying Mirror-Induced Visual Illusion: An Activation Likelihood Estimation Meta-Analysis. Front. Hum. Neurosci. 2020, 14, 276. [Google Scholar] [CrossRef]
- Puledda, F.; Bruchhage, M.; O’Daly, O.; Ffytche, D.; Williams, S.C.R.; Goadsby, P.J. Occipital cortex and cerebellum gray matter changes in visual snow syndrome. Neurology 2020, 95, e1792–e1799. [Google Scholar] [CrossRef]
- Lee, J.; Ahn, S.W.; Wachholtz, A.; Lee, J.H. Attentional Patterns Toward Pain-Related Information: Comparison Between Chronic Pain Patients and Non-pain Control Group. Front. Psychol. 2020, 11, 1990. [Google Scholar] [CrossRef] [PubMed]
- Ruf, S.P.; Hetterich, L.; Mazurak, N.; Rometsch, C.; Jurjut, A.M.; Ott, S.; Herrmann-Werner, A.; Zipfel, S.; Stengel, A. Mirror Therapy in Patients with Somatoform Pain Disorders—A Pilot Study. Behav. Sci. 2023, 13, 432. [Google Scholar] [CrossRef] [PubMed]
- Samuelkamaleshkumar, S.; Reethajanetsureka, S.; Pauljebaraj, P.; Benshamir, B.; Padankatti, S.M.; David, J.A. Mirror therapy enhances motor performance in the paretic upper limb after stroke: A pilot randomized controlled trial. Arch. Phys. Med. Rehabil. 2014, 95, 2000–2005. [Google Scholar] [CrossRef] [PubMed]
- Koenigs, M.; Barbey, A.K.; Postle, B.R.; Grafman, J. Superior parietal cortex is critical for the manipulation of information in working memory. J. Neurosci. 2009, 29, 14980–14986. [Google Scholar] [CrossRef]
- Balslev, D.; Cole, J.; Miall, R.C. Proprioception contributes to the sense of agency during visual observation of hand movements: Evidence from temporal judgments of action. J. Cogn. Neurosci. 2007, 19, 1535–1541. [Google Scholar] [CrossRef]
- Imaizumi, S.; Asai, T.; Koyama, S. Agency over Phantom Limb Enhanced by Short-Term Mirror Therapy. Front. Hum. Neurosci. 2017, 11, 483. [Google Scholar] [CrossRef]
- Ben Shalom, D. The amygdala-insula-medial prefrontal cortex-lateral prefrontal cortex pathway and its disorders. Front. Neuroanat. 2022, 16, 1028546. [Google Scholar] [CrossRef]
- Ferrari, C.; Lega, C.; Vernice, M.; Tamietto, M.; Mende-Siedlecki, P.; Vecchi, T.; Todorov, A.; Cattaneo, Z. The Dorsomedial Prefrontal Cortex Plays a Causal Role in Integrating Social Impressions from Faces and Verbal Descriptions. Cereb. Cortex. 2016, 26, 156–165. [Google Scholar] [CrossRef]
- Powers, K.E.; Chavez, R.S.; Heatherton, T.F. Individual differences in response of dorsomedial prefrontal cortex predict daily social behavior. Soc. Cogn. Affect. Neurosci. 2016, 11, 121–126. [Google Scholar] [CrossRef]
- Michielsen, M.E.; Selles, R.W.; van der Geest, J.N.; Eckhardt, M.; Yavuzer, G.; Stam, H.J.; Smits, M.; Ribbers, G.M.; Bussmann, J.B. Motor recovery and cortical reorganization after mirror therapy in chronic stroke patients: A phase II randomized controlled trial. Neurorehabil. Neural. Repair. 2011, 25, 223–233. [Google Scholar] [CrossRef]
- Canlı, K.; Van Oijen, J.; Van Oosterwijck, J.; Meeus, M.; Van Oosterwijck, S.; De Meulemeester, K. Influence of Sensory Re-training on Cortical Reorganization in Peripheral Neuropathy: A Systematic Review. PM&R, 2023; online ahead of print. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcomes | Group | Mean | SD | T-Student | p |
|---|---|---|---|---|---|
| Age (years) | EG | 24.9 | 10.9 | ||
| CG | 24.9 | 9.5 | −0.002 | 0.998 | |
| Weight (Kg) | EG | 75.8 | 5.7 | ||
| CG | 73.4 | 10.6 | 0.629 | 0.538 | |
| Height (m) | EG | 1.77 | 0.06 | ||
| CG | 1.72 | 0.08 | 1.261 | 0.224 | |
| BMI (Kg/m2) | EG | 24.3 | 1.7 | ||
| CG | 24.7 | 3.5 | −0.337 | 0.740 |
| Outcomes | Group | Mean | SD | Shapiro–Wilk W | p |
|---|---|---|---|---|---|
| Pre-Pain intensity | EG | 1.416 | 1.269 | 0.898 | 0.017 ** |
| (VAS 0-10) | CG | 1.150 | 0.955 | 0.861 | 0.004 ** |
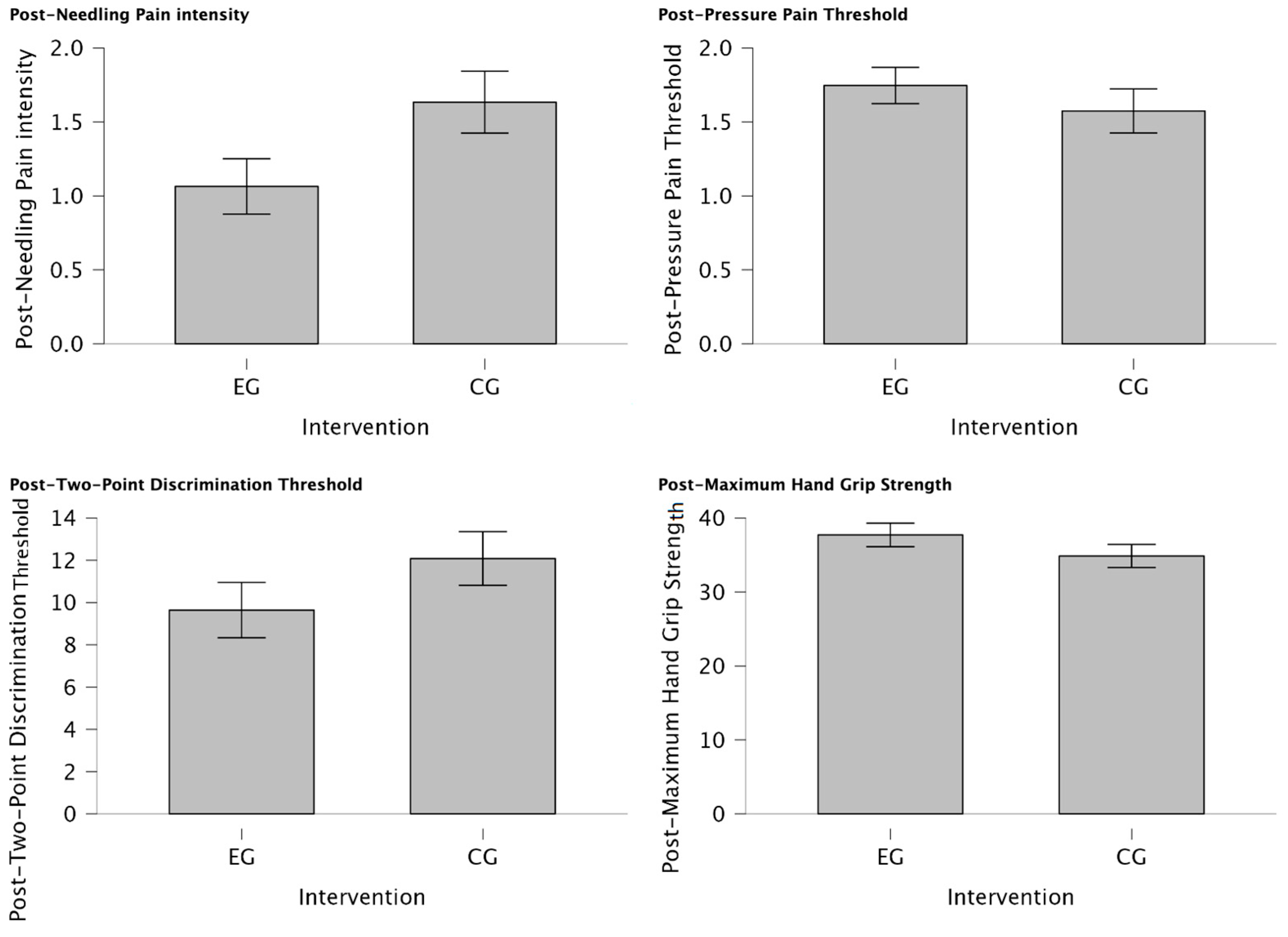
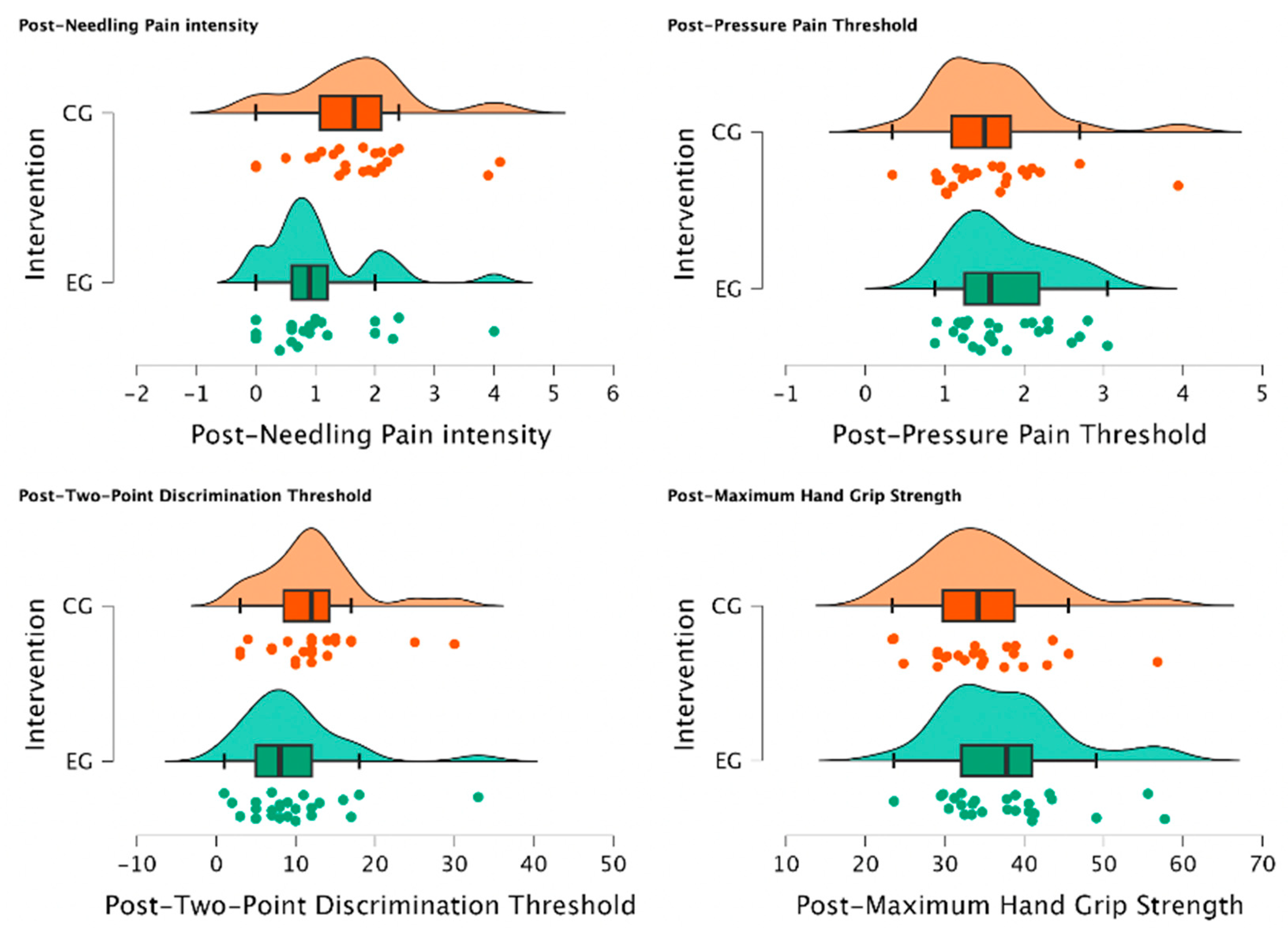
| Post-Pain intensity | EG | 1.064 | 0.934 | 0.857 | 0.002 ** |
| (VAS 0-10) | CG | 1.633 | 1.025 | 0.927 | 0.085 |
| Pre-PPT | EG | 1.909 | 0.672 | 0.911 | 0.033 * |
| (Kg/cm2) | CG | 1.640 | 0.683 | 0.862 | 0.004 ** |
| Post-PPT | EG | 1.746 | 0.613 | 0.938 | 0.135 |
| (Kg/cm2) | CG | 1.574 | 0.729 | 0.895 | 0.017 |
| Pre-TPDT | EG | 9.320 | 5.872 | 0.826 | <0.001 *** |
| (mm) | CG | 13.500 | 6.871 | 0.947 | 0.232 |
| Post-TPDT | EG | 9.640 | 6.544 | 0.840 | 0.001 ** |
| (mm) | CG | 12.083 | 6.213 | 0.903 | 0.025 ** |
| Pre-MHGS | EG | 37.96 | 8.032 | 0.911 | 0.033 * |
| (Kg/F) | CG | 34.04 | 7.386 | 0.924 | 0.073 |
| Post-MHGS | EG | 37.712 | 7.986 | 0.928 | 0.077 |
| (Kg/F) | CG | 34.867 | 7.609 | 0.944 | 0.204 |
| CI [95%] | ES | |||||||
|---|---|---|---|---|---|---|---|---|
| Outcomes | Test | Statistic | p | MD | SEM | Inf. | Sup. | Rank–Biserial |
| Pain intensity (VAS 0-10) | Wilcoxon W | 137.00 | 0.047 * | 0.400 | 0.271 | 0.000 | Inf. | 0.442 |
| PPT (Kg/cm2) | Wilcoxon W | 262.00 | <0.001 *** | 0.148 | 0.038 | 0.071 | Inf. | 0.747 |
| TPDT (mm) | Wilcoxon W | 121.00 | 0.711 | −0.000 | 0.674 | −1.500 | Inf. | −0.127 |
| MHGS (Kg/F) | Wilcoxon W | 177.00 | 0.224 | 0.200 | 0.199 | −0.150 | Inf. | 0.180 |
| CI [95%] | ES | |||||||
|---|---|---|---|---|---|---|---|---|
| Outcomes | Test | Statistic | p | MD | SEM | Inf. | Sup. | Rank–Biserial |
| Pain intensity | Wilcoxon W | 105.50 | 0.643 | −0.400 | 0.247 | −0.899 | −Inf. | −0.086 |
| (VAS 0-10) | ||||||||
| PPT (Kg/cm2) | Wilcoxon W | 163.00 | 0.648 | 0.029 | 0.073 | −Inf. | 0.166 | 0.086 |
| TPDT (mm) | Wilcoxon W | 207.00 | 0.983 | 1.999 | 1.047 | −Inf. | 3.000 | 0.496 |
| MHGS (Kg/F) | Wilcoxon W | 83.00 | 0.081 | −0.799 | 1.051 | −Inf. | 0.200 | −0.343 |
| ES | |||||
|---|---|---|---|---|---|
| Outcomes | Test | Statistic | p | Rank–Biserial Correlation | Rank–Biserial Correlation |
| Pain intensity (VAS 0-10) | Mann–Whitney U | 188.000 | 0.034 * | −0.373 | 0.165 |
| Post-PPT (Kg/cm2) | Mann–Whitney U | 354.000 | 0.862 | 0.180 | 0.165 |
| Post-TPDT (mm) | Mann–Whitney U | 212.000 | 0.079 | −0.293 | 0.165 |
| Post-MHGS (Kg/F) | Mann–Whitney U | 365.000 | 0.905 | 0.217 | 0.165 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín Pérez, S.E.; Rodríguez, J.D.; Kalitovics, A.; de Miguel Rodríguez, P.; Bortolussi Cegarra, D.S.; Rodríguez Villanueva, I.; García Molina, Á.; Ruiz Rodríguez, I.; Montaño Ocaña, J.; Martín Pérez, I.M.; et al. Effect of Mirror Therapy on Post-Needling Pain Following Deep Dry Needling of Myofascial Trigger Point in Lateral Elbow Pain: Prospective Controlled Pilot Trial. J. Clin. Med. 2024, 13, 1490. https://doi.org/10.3390/jcm13051490
Martín Pérez SE, Rodríguez JD, Kalitovics A, de Miguel Rodríguez P, Bortolussi Cegarra DS, Rodríguez Villanueva I, García Molina Á, Ruiz Rodríguez I, Montaño Ocaña J, Martín Pérez IM, et al. Effect of Mirror Therapy on Post-Needling Pain Following Deep Dry Needling of Myofascial Trigger Point in Lateral Elbow Pain: Prospective Controlled Pilot Trial. Journal of Clinical Medicine. 2024; 13(5):1490. https://doi.org/10.3390/jcm13051490
Chicago/Turabian StyleMartín Pérez, Sebastián Eustaquio, Jhoselyn Delgado Rodríguez, Alejandro Kalitovics, Pablo de Miguel Rodríguez, Daniela Sabrina Bortolussi Cegarra, Iremar Rodríguez Villanueva, Álvaro García Molina, Iván Ruiz Rodríguez, Juan Montaño Ocaña, Isidro Miguel Martín Pérez, and et al. 2024. "Effect of Mirror Therapy on Post-Needling Pain Following Deep Dry Needling of Myofascial Trigger Point in Lateral Elbow Pain: Prospective Controlled Pilot Trial" Journal of Clinical Medicine 13, no. 5: 1490. https://doi.org/10.3390/jcm13051490
APA StyleMartín Pérez, S. E., Rodríguez, J. D., Kalitovics, A., de Miguel Rodríguez, P., Bortolussi Cegarra, D. S., Rodríguez Villanueva, I., García Molina, Á., Ruiz Rodríguez, I., Montaño Ocaña, J., Martín Pérez, I. M., Sosa Reina, M. D., Villafañe, J. H., & Alonso Pérez, J. L. (2024). Effect of Mirror Therapy on Post-Needling Pain Following Deep Dry Needling of Myofascial Trigger Point in Lateral Elbow Pain: Prospective Controlled Pilot Trial. Journal of Clinical Medicine, 13(5), 1490. https://doi.org/10.3390/jcm13051490