Abstract
Purpose: This systematic review evaluated whole-body MRI (WB-MRI) as a cancer screening tool for individuals carrying germline TP53 mutations, a population known to be at a significantly elevated risk of malignancy. The primary objective is to assess the diagnostic performance of WB-MRI in detecting cancer in this cohort. Methods: PubMed, MEDLINE, EMBASE and the Cochrane Central Registry of Controlled Trials were searched until 18 August 2023. Eligible studies were selected based on predefined inclusion criteria. The data extracted included information on study characteristics, patient demographics, and the WB-MRI diagnostic performance. Results: This systematic review identified eight eligible studies, comprising 506 TP53 mutation carriers. The mean age was 34.6 ± 16.3 (range 1–74) years. In total, 321/506 (63.4%) of the patients were female and 185/506 (36.6%) were male. In addition, 267/506 (52.8%) had a previous oncological diagnosis. Thirty-six new cancers were diagnosed with WB-MRI (36/506 (7.1%)). The overall pooled proportion of cancer detected on MRI was 7% (95% confidence interval 5–10). In total, 44 new lesions were picked up, as multiple lesions were found in some patients. Conclusion: WB-MRI is an effective cancer screening tool for TP53 mutation carriers. While these findings suggest the potential for WB-MRI to contribute to early cancer detection in this high-risk population, further research and the standardisation of protocols internationally are warranted to optimise its clinical utility.
1. Introduction
Germline TP53 mutations cause Li-Fraumeni syndrome (LFS), a rare genetically inherited autosomal dominant condition that significantly elevates the lifetime risk of developing multiple types of cancers [,,,], including breast, brain and/or sarcomatous lesions []. The reported rates of cancer development are 22% by the age of 5, 41% by age 18 and almost 100% by age 70 [,]. Unlike other hereditary cancer syndromes, in LFS, the universal radiological guidelines for cancer screening are not as clear []. Despite this, emerging data suggest that surveillance may offer benefits [,,]. Furthermore, surveillance guidelines for individuals carrying disease-causing TP53 mutations have recently been outlined through the collaborative efforts of an international consortium led by Canadian and US teams [,]. These guidelines recommend that carriers initiate annual WBMRI and annual brain MRI from the first year of life [].
Several global studies, mostly conducted without gadolinium-based contrast agents (GBCAs), have validated the effectiveness of WBMRI, showing an overall estimated detection rate of 7% for new and localised primary cancers during the initial screen [,,]. Given the potential long-term retention of GBCAs in various organs, it is recommended that caution is exercised when administering multiple GBCAs to germline TP53 variant carriers. Furthermore, only macrocyclic GBCAs, known for their apparently lower retention in the body [], should be utilised.
Research is ongoing to establish effective strategies for the early detection and surveillance of cancer in TP53 mutation carriers [,]. Traditional cancer screening paradigms have often proven inadequate for this high-risk population, necessitating a more nuanced and comprehensive approach [,]. WB-MRI, a non-invasive imaging modality, has emerged as a promising contender in this pursuit [,,]. WB-MRI can scrutinise soft tissues and organs throughout the body without the need for ionising radiation []. This non-radiating characteristic makes it an attractive option for repeated surveillance in individuals predisposed to cancer, thus mitigating the cumulative risks associated with radiation exposure from computed tomography (CT) scans [,].
The deployment of WB-MRI as a primary cancer screening tool for LFS poses several clinical, logistical, and financial implications []. Its efficacy in reliably detecting cancers at an early, treatable stage in this unique population remains controversial [,]. This systematic review aims to synthesise the existing body of literature regarding the utility of WB-MRI as a cancer screening modality for individuals with LFS.
2. Methods
2.1. Registration and Search Strategy
Our search was conducted in line with the most recent Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations []. Our study protocol was prospectively registered with PROSPERO (CRD42023400797). We conducted a search using PubMed, MEDLINE (Ovid), EMBASE and the Cochrane Central Register of Controlled Trials using a search strategy undertaken on 18 August 2023. The search pathway is illustrated in the PRISMA diagram in Figure 1. The grey literature was also searched for any relevant studies. The systematic search process with detailed search terms are outlined in Supplementary Material S1. Due to heterogeneity and the descriptive nature of the results that are presented, a narrative summary of findings is presented.
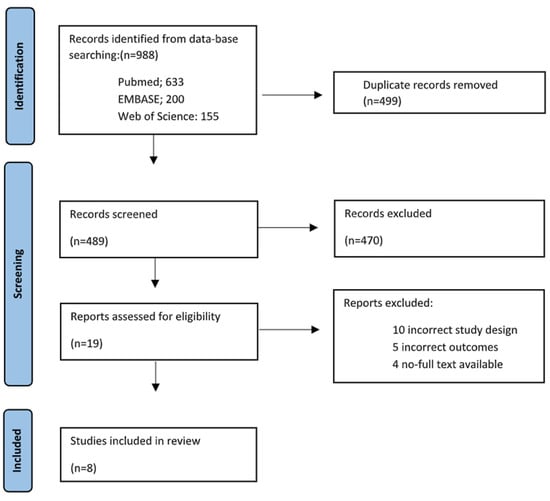
Figure 1.
PRISMA flowchart outlining the systematic search process.
2.2. Inclusion/Exclusion Criteria
2.2.1. Inclusion Criteria
For analytical inclusion, studies had to meet the following criteria:
- (a)
- Report on patients with LFS who underwent WB-MRI radiological oncological screening.
- (b)
- Report on cancers picked up on WB-MRI.
- (c)
- Report with a well-defined research methodology.
2.2.2. Exclusion Criteria
Studies were excluded from the analysis if the following were true:
- (a)
- Patients did not have a diagnosis of LFS.
- (b)
- Imaging was performed by another radiological modality, other than WB-MRI.
- (c)
- Outcomes of interest were not reported.
- (d)
- The methodology was not clearly reported.
2.3. Identification of Studies and Outcomes of Interest
Studies that satisfied the inclusion and exclusion criteria were included in our review. The information extracted was based on the PICO framework (Population,
Intervention, Comparator, and Outcomes) []. The following PICO elements were used as the basis for selecting studies:
- I.
- Population: LFS patients
- II.
- Intervention: LFS patient undergoing WB-MRI for cancer screening
- III.
- Comparison: asymptomatic non-LFS patients undergoing WB-MRI
- IV.
- Outcome:
Primary outcome: incidence of new cancer diagnosis on WB-MRI.
2.4. Study Selection, Data Extraction and Critical Appraisal
A database was created using the reference managing software EndNote X9 TM Number 21. The abstracts of articles yielded from the search were reviewed by two independent authors (HCT and NOS) based on the inclusion and exclusion criteria detailed above. Following the removal of duplicate articles, discrepancies in judgment about the relevance of articles were resolved via an open discussion between the authors and an independent third reviewer (MK). An article was excluded from the review when the three reviewers came to an agreement. Full texts of the shortlisted articles were obtained and further evaluated to ensure that they met our inclusion criteria. The references of the shortlisted articles were then searched to identify other relevant studies that may have been missed through the initial search of online databases. Data were extracted by two reviewers independently from the articles that met the inclusion criteria based on a full-text review. In order to extract and store the data efficiently, the Cochrane Collaboration screening and data extraction tool, Covidence version 2.0, was used [].
2.5. Statistical Analysis
A proportional meta-analysis was performed []. Statistical analysis was run using Stata 17 []. Proportions were pooled using the “metaprop” function within Stata; 95% confidence intervals were employed and p ≤ 0.05 was considered statistically significant. Heterogeny was reported using I2, with >−50% considered significant [].
2.6. Risk of Bias
The potential biases were assessed using the Newcastle–Ottawa scale (HT) risk of bias tool and the results were tabulated []. This assessment tool grades each study as being ‘satisfactory’ or ‘unsatisfactory’ across various categories. We assigned stars to evaluate the study quality: 7 stars—“very good”, 5–6 stars “good”, 3–4 stars “satisfactory” and 0–2 stars “unsatisfactory”. The critical appraisal was completed by two reviewers independently (HT and NOS), where once again a third reviewer (MK) was asked to arbitrate when there were discrepancies in opinion (See Supplementary Material S2).
3. Results
3.1. Search Results
In total, 988 articles were identified and 499 duplicate articles were excluded. Thereafter, the study titles and abstracts were screened, resulting in 19 studies being eligible for full-text review. Of these, eight studies met the eligibility criteria and were included [,,,,,,,]. The PRISMA flow chart is illustrated in Figure 1. Overall, six studies were prospective cohort studies [,,,,,], and the remaining two studies were retrospective cohort studies [,]. Only one study used a control group []. The primary outcome was the identification of lesions suspicious for malignancy in asymptomatic TP53 carriers in seven studies, whilst Kagami et al. defined the primary outcome as radiological findings leading to follow-up imaging or intervention in asymptomatic TP53 carriers [].
3.2. Patient Characteristics
Overall, 550 patients who had body MRI were included; of these, 506/550 (92%) of the patients had a known diagnosis of LFS, the remaining 44 being from the control group in the study by Saya et al. [] Five studies examined adults and children [,,,,], two studies examined children only [,], and one study examined adults only []. The mean age was 34.6 ± 16.3 (range 1–74) years. In total, 321/506 (63.4%) of the patients were female and 185/506 (36.6%) were male. Overall, 267/506 (52.8%) had a previous cancer diagnosis. See Table 1 for characteristics of the trials and populations.

Table 1.
Characteristics of the trials included.
3.3. MRI Protocols/Acquisition Parameters
All eight studies employed MRI as the only imaging modality for screening. Overall, four studies reported on scanning time; however, only Mai et al. reported a mean time of 45 min [], whilst the other three studies reported a scanning time range (25–150 min) [,,]. Five of the eight studies utilised an identical WB-MRI protocol in all subjects [,,,,]. In the six studies that reported it, the MRIs were reviewed by at least two or more experienced radiologists. Only two studies employed gadolinium-based contrast imaging [,]. The full acquisition parameters are illustrated in Table 2.
Table 2.
Characteristics of the MRI protocols/acquisition parameters.
3.4. Incidence of New Cancer
Overall, 44 new lesions were identified in 36 patients with WB-MRI (36/506 (7.1%)) and subsequently confirmed as cancer. The overall pooled proportion of cancer detected on MRI was 7% (95% CI 5–10) (Figure 2). The distribution of cancer diagnosis by location was as follows: 16 abdominal, 10 chest, 4 brain, 4 neck, 4 pelvis, 3 lower limb, 2 upper limb and 1 breast. Five studies specified whether the cancer was identified on the initial or follow-up WB-MRI scan [,,,,]. Nine malignant lesions (in nine patients) that were not present on the initial scan were diagnosed during follow-up WB-MRI. The most common cancers were renal cell carcinoma, osteosarcoma, colorectal adenocarcinoma and astrocytoma. The confirmation of cancer in all studies was performed through a combination of further imaging and subsequent tissue specimen for histological diagnosis. See Table 3 for lesion diagnosis by body distribution and Table 4 for a descriptive overview of the types of cancer.
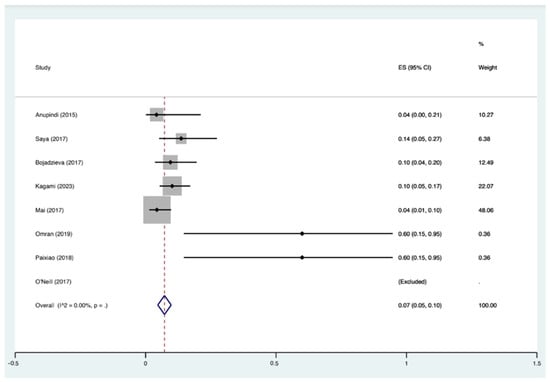
Figure 2.
Overall pooled proportion of cancer detected on MRI. ES: Effect Sizes [,,,,,,,].
Table 3.
Incidence of new cancer and critical findings.
Table 4.
Cancer location and timing of MRI.
3.5. Risk of Bias
One study was ‘very good’, seven studies were ‘good’, zero studies were ‘satisfactory’ and zero studies were ’unsatisfactory’. Supplementary Material S2 summarises the results of our risk of bias assessment and individual breakdown of included studies.
4. Discussion
The management of individuals with germline TP53 mutations presents a unique challenge to screening services due to their significant risk of developing a wide spectrum of cancers over the course of their life []. Conventional cancer screening modalities are limited in detecting the full range of malignancies associated with TP53 mutations [,,]. Whole-body MRI (WB-MRI) has emerged as a potential comprehensive tool in this context, offering a comprehensive, non-ionising radiation approach to screening for multiple cancers simultaneously [].
Our review identified eight studies encompassing 506 TP53 variant carriers who underwent WB-MRI. These studies collectively revealed several critical insights into the potential of WB-MRI in early cancer detection for high-risk individuals and detected cancer in 7% (95% CI 5–10%). This figure emphasises that WB-MRI can detect asymptomatic cancers in TP53 variant carriers before reaching a more advanced stage. One of the strengths of WB-MRI lies in its ability to identify multiple lesions in a single scan. In our review, 44 new lesions were detected, underlining the comprehensiveness of this imaging approach. For individuals with TP53 mutations who are at risk of developing cancers in various organs, WB-MRI’s capacity to visualise multiple body regions simultaneously is a valuable asset. This advantage improved the efficiency of time while also reducing the burden of multiple screening tests, which TP53 mutation carriers are often subjected to.
While the findings of our review are encouraging, several important considerations should guide the future implementation of WB-MRI in clinical practice for TP53 mutation carriers. One key aspect is the need for the standardisation of protocols. Although surveillance protocols have been reported by several international consortiums [,,], currently, there is no universally accepted WB-MRI protocol for LFS screening, and variations in scanning parameters and interpretation criteria exist [,]. Establishing standardised guidelines for image acquisition and interpretation will be crucial to ensure consistent and reliable results across different healthcare settings. Another critical point of discussion is the balance between the benefits and challenges of WB-MRI. One challenge highlighted in our review is the interpretation of MRI findings. The detection of incidental lesions can lead to unnecessary patient anxiety and invasive follow-up procedures, emphasising the importance of specialised centres employing the expertise of specialised radiologists experienced in WB-MRI screening [,]. Additionally, the cost and availability of WB-MRI should be considered, as these factors may limit its widespread adoption, particularly in resource-constrained healthcare systems [,,]. In our systematic review, none of the studies examined the cost-effectiveness of WB-MRI in this cohort.
Integrating WB-MRI into a personalised screening plan, alongside other imaging modalities and clinical assessments, can provide a more comprehensive and targeted approach to cancer surveillance []. It is also worth noting that the 7.3% rate of new cancer diagnoses in our review suggests that a significant proportion of TP53 mutation carriers are developing cancers that may have been missed by conventional screening methods. This reinforces the need for improved surveillance strategies for this vulnerable population.
In conclusion, a systematic review of the literature provides compelling evidence for the use of WB-MRI as an effective cancer screening tool for TP53 mutation carriers and its ability to detect cancers in multiple organs in a single scan setting. However, the implementation of WB-MRI in clinical practice requires further validation, and in particular, simple and reproductive standardised protocols and cost-effectiveness analyses. The findings emphasise the importance of individualised risk assessment and highlights the role of WB-MRI in early cancer detection, which may ultimately improve the outcomes of TP53 mutation carriers.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm13051223/s1. Supplementary Material S1: Search strategy. Supplementary Material S2: Risk of Bias assessment (Newcastle–Ottawa scale).
Author Contributions
Conceptualization, H.C.T., N.J.O. and M.E.K.; methodology, H.C.T.; software, N.J.O.; validation, A.M., T.S.T., J.F.M., B.M.M.C. and W.Q.; formal analysis, H.C.T.; investigation, I.B.; resources, A.C.; data curation, M.E.K.; writing—original draft preparation, H.C.T.; writing—review and editing, M.E.K.; visualization, D.G.; supervision, D.G.; project administration, H.C.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Joly Leadership Fund, Trinity St. James Cancer Institute.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pasoglou, V.; Michoux, N.; Larbi, A.; Van Nieuwenhove, S.; Lecouvet, F. Whole Body MRI and oncology: Recent major advances. Br. J. Radiol. 2018, 91, 20170664. [Google Scholar] [CrossRef]
- Guha, T.; Malkin, D. Inherited TP53 Mutations and the Li-Fraumeni Syndrome. Cold Spring Harb. Perspect. Med. 2017, 7, a026187. [Google Scholar] [CrossRef]
- Varley, J.M. Germline TP53 mutations and Li-Fraumeni syndrome. Hum. Mutat. 2003, 21, 313–320, Erratum in Hum. Mutat. 2003, 21, 551. [Google Scholar] [CrossRef]
- Malkin, D.; Li, F.P.; Strong, L.C.; Fraumeni, J.F.; Nelson, C.E.; Kim, D.H.; Kassel, J.; Gryka, M.A.; Bischoff, F.Z.; Tainsky, M.A.; et al. Germ line p53 mutations in a familial syndrome of breast cancer, sarcomas, and other neoplasms. Science 1990, 250, 1233–1238. [Google Scholar] [CrossRef]
- Correa, H. Li-Fraumeni Syndrome. J. Pediatr. Genet. 2016, 5, 84–88. [Google Scholar] [CrossRef]
- Zhou, R.; Xu, A.; Gingold, J.; Strong, L.C.; Zhao, R.; Lee, D.F. Li-Fraumeni Syndrome Disease Model: A Platform to Develop Precision Cancer Therapy Targeting Oncogenic p53. Trends Pharmacol. Sci. 2017, 38, 908–927. [Google Scholar] [CrossRef]
- Bougeard, G.; Renaux-Petel, M.; Flaman, J.; Charbonnier, C.; Fermey, P.; Belotti, M.; Gauthier-Villars, M.; Stoppa-Lyonnet, D.; Consolino, E.; Brugières, L.; et al. Revisiting Li-Fraumeni syndrome from TP53 Carriers. J. Clin. Oncol. 2015, 33, 2345–2352. [Google Scholar] [CrossRef] [PubMed]
- Mai, P.L.; Best, A.F.; Peters, J.A.; DeCastro, R.M.; Khincha, P.P.; Loud, J.T.; Bremer, R.C.; Rosenberg, P.S.; Savage, S.A. Risks of first and subsequent cancers among TP53 mutation carriers in the National Cancer Institute Li-Fraumeni syndrome cohort. Cancer 2016, 122, 3673–3681. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Shore, A.; Wasserman, J.D.; Stephens, D.; Kim, R.H.; Druker, H.; Gallinger, B.; Naumer, A.; Kohlmann, W.; Novokmet, A.; et al. Biochemical and imaging surveillance in germline TP53 mutation carriers with Li-Fraumeni syndrome: 11 year follow-up of a prospective observational study. Lancet Oncol. 2016, 17, 1295–1305. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.E.; Magoon, S.; Forghani, I.; Alessandrino, F.; D’Amato, G.; Jonczak, E.; Subhawong, T.K. Radiologic screening and surveillance in hereditary cancers. Eur. J. Radiol. Open 2022, 9, 100422. [Google Scholar] [CrossRef] [PubMed]
- Consul, N.; Amini, B.; Ibarra-Rovira, J.J.; Blair, K.J.; Moseley, T.W.; Taher, A.; Shah, K.B.; Elsayes, K.M. Li-Fraumeni Syndrome and Whole-Body MRI Screening: Screening Guidelines, Imaging Features, and Impact on Patient Management. AJR Am. J. Roentgenol. 2021, 216, 252–263. [Google Scholar] [CrossRef]
- Kratz, C.P.; Achatz, M.I.; Brugières, L.; Frebourg, T.; Garber, J.E.; Greer, M.C.; Hansford, J.R.; Janeway, K.A.; Kohlmann, W.K.; McGee, R.; et al. Cancer screening recommendations for individuals with Li-Fraumeni syndrome. Clin. Cancer Res. 2018, 23, e38–e45. [Google Scholar] [CrossRef]
- Omran, M.; Tham, E.; Brandberg, Y.; Ahlström, H.; Lundgren, C.; Paulsson-Karlsson, Y.; Kuchinskaya, E.; Silander, G.; Rosén, A.; Persson, F.; et al. Whole-Body MRI Surveillance-Baseline Findings in the Swedish Multicentre Hereditary TP53-Related Cancer Syndrome Study (SWEP53). Cancers 2022, 14, 380. [Google Scholar] [CrossRef]
- Bojadzieva, J.; Amini, B.; Day, S.F.; Jackson, T.L.; Thomas, P.S.; Willis, B.J.; Throckmorton, W.R.; Daw, N.C.; Bevers, T.B.; Strong, L.C. Whole body magnetic resonance imaging (WB-MRI) and brain MRI baseline surveillance in TP53 germline mutation carriers: Experience from the Li-Fraumeni Syndrome Education and Early Detection (LEAD) clinic. Fam. Cancer 2018, 17, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Blomqvist, L.; Nordberg, G.F.; Nurchi, V.M.; Aaseth, J.O. Gadolinium in Medical Imaging-Usefulness, Toxic Reactions and Possible Countermeasures-A Review. Biomolecules. 2022, 12, 742. [Google Scholar] [CrossRef] [PubMed]
- Sorrell, A.D.; Espenschied, C.R.; Culver, J.O.; Weitzel, J.N. Tumor protein p53 (TP53) testing and Li-Fraumeni syndrome: Current status of clinical applications and future directions. Mol. Diagn. Ther. 2013, 17, 31–47. [Google Scholar] [CrossRef] [PubMed]
- Frankenthal, I.A.; Alves, M.C.; Tak, C.; Achatz, M.I. Cancer surveillance for patients with Li-Fraumeni Syndrome in Brazil: A cost-effectiveness analysis. Lancet Reg. Health Am. 2022, 12, 100265. [Google Scholar] [CrossRef] [PubMed]
- Boyd, M.T.; Vlatkovic, N. p53: A molecular marker for the detection of cancer. Expert Opin. Med. Diagn. 2008, 2, 1013–1024. [Google Scholar] [CrossRef]
- Kumamoto, T.; Yamazaki, F.; Nakano, Y.; Tamura, C.; Tashiro, S.; Hattori, H.; Nakagawara, A.; Tsunematsu, Y. Medical guidelines for Li-Fraumeni syndrome 2019, version 1.1. Int. J. Clin. Oncol. 2021, 26, 2161–2178, Erratum in Int. J. Clin. Oncol. 2022, 27, 262–263. [Google Scholar] [CrossRef]
- Bancroft, E.K.; Saya, S.; Brown, E.; Thomas, S.; Taylor, N.; Rothwell, J.; Pope, J.; Chamberlain, A.; Page, E.; Benafif, S.; et al. Psychosocial effects of whole-body MRI screening in adult high-risk pathogenic TP53 mutation carriers: A case-controlled study (SIGNIFY). J. Med. Genet. 2020, 57, 226–236. [Google Scholar] [CrossRef]
- Anupindi, S.A.; Bedoya, M.A.; Lindell, R.B.; Rambhatla, S.J.; Zelley, K.; Nichols, K.E.; Chauvin, N.A. Diagnostic Performance of Whole-Body MRI as a Tool for Cancer Screening in Children With Genetic Cancer-Predisposing Conditions. AJR Am. J. Roentgenol. 2015, 205, 400–408. [Google Scholar] [CrossRef]
- Ballinger, M.L.; Ferris, N.J.; Moodie, K.; Mitchell, G.; Shanley, S.; James, P.A.; Thomas, D.M. Surveillance in Germline TP53 Mutation Carriers Utilizing Whole-Body Magnetic Resonance Imaging. JAMA Oncol. 2017, 3, 1735–1736. [Google Scholar] [CrossRef]
- Schmidt, G.; Dinter, D.; Reiser, M.F.; Schoenberg, S.O. The uses and limitations of whole-body magnetic resonance imaging. Dtsch. Arztebl. Int. 2010, 107, 383–389. [Google Scholar]
- Goehde, S.C.; Hunold, P.; Vogt, F.M.; Ajaj, W.; Goyen, M.; Herborn, C.U.; Forsting, M.; Debatin, J.F.; Ruehm, S.G. Full-body cardiovascular and tumor MRI for early detection of disease: Feasibility and initial experience in 298 subjects. AJR 2005, 184, 598–611. [Google Scholar] [CrossRef]
- Kramer, H.; Michaely, K.; Nikolaou, K.; Reiser, M.F.; Schoenberg, S.O. State of the art cardiovascular imaging with parallel imaging techniques on a whole body MR scanner: Experience in more than 200 individuals. Eur. Radiol. 2006, 41, 141–147. [Google Scholar]
- Paixão, D.; Guimarães, M.D.; de Andrade, K.C.; Nóbrega, A.F.; Chojniak, R.; Achatz, M.I. Whole-body magnetic resonance imaging of Li-Fraumeni syndrome patients: Observations from a two rounds screening of Brazilian patients. Cancer Imaging 2018, 18, 27. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, E.C. The well-built clinical question: The key tofinding the best evidence efficiently. World Med. J. 1999, 98, 25–28. [Google Scholar]
- Covidence Systematic Review Software, version: 2.0; Veritas Health Innovation: Melbourne, Australia, 2023.
- Barker, T.H.; Migliavaca, C.B.; Stein, C.; Colpani, V.; Falavigna, M.; Aromataris, E.; Munn, Z. Conducting proportional meta-analysis in different types of systematic reviews: A guide for synthesisers of evidence. BMC Med. Res. Methodol. 2021, 21, 189. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software; Release 17; StataCorp LLC: College Station, TX, USA, 2021. [Google Scholar]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, J.; Robertson, J.; Peterson, V.; Welch, V. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analysis. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 23 November 2023).
- Saya, S.; Killick, E.; Thomas, S.; Taylor, N.; Bancroft, E.K.; Rothwell, J.; Benafif, S.; Dias, A.; Mikropoulos, C.; Pope, J.; et al. Baseline results from the UK SIGNIFY study: A whole-body MRI screening study in TP53 mutation carriers and matched controls. Fam. Cancer 2017, 16, 433–440. [Google Scholar] [CrossRef]
- Kagami, L.A.T.; Du, Y.K.; Fernandes, C.J.; Le, A.N.; Good, M.; Duvall, M.M.; Baldino, S.E.; Powers, J.; Zelley, K.; States, L.J.; et al. Rates of Intervention and Cancer Detection on Initial versus Subsequent Whole-body MRI Screening in Li-Fraumeni Syndrome. Cancer Prev. Res. 2023, 16, 507–512. [Google Scholar] [CrossRef]
- Mai, P.L.; Khincha, P.P.; Loud, J.T.; DeCastro, R.M.; Bremer, R.C.; Peters, J.A.; Liu, C.Y.; Bluemke, D.A.; Malayeri, A.A.; Savage, S.A. Prevalence of Cancer at Baseline Screening in the National Cancer Institute Li-Fraumeni Syndrome Cohort. JAMA Oncol. 2017, 3, 1640–1645. [Google Scholar] [CrossRef]
- O’Neill, A.F.; Voss, S.D.; Jagannathan, J.P.; Kamihara, J.; Nibecker, C.; Itriago-Araujo, E.; Masciari, S.; Parker, E.; Barreto, M.; London, W.B.; et al. Screening with whole-body magnetic resonance imaging in pediatric subjects with Li-Fraumeni syndrome: A single institution pilot study. Pediatr. Blood Cancer 2018, 65, e26822. [Google Scholar] [CrossRef]
- Evans, D.G.; Woodward, E.R.; Bajalica-Lagercrantz, S.; Oliveira, C.; Frebourg, T. Germline TP53 Testing in Breast Cancers: Why, When and How? Cancers 2020, 12, 3762. [Google Scholar] [CrossRef]
- Weitzel, J.N.; Chao, E.C.; Nehoray, B.; Van Tongeren, L.R.; LaDuca, H.; Blazer, K.R.; Slavin, T.; Pesaran, T.; Rybak, C.; Solomon, I.; et al. Somatic TP53 variants frequently confound germ-line testing results. Genet. Med. 2018, 20, 809–816. [Google Scholar] [CrossRef]
- Frebourg, T.; Bajalica Lagercrantz, S.; Oliveira, C.; Magenheim, R.; Evans, D.G. Guidelines for the Li–Fraumeni and heritable TP53-related cancer syndromes. Eur. J. Hum. Genet. 2020, 28, 1379–1386. [Google Scholar] [CrossRef]
- Ballinger, M.L.; Best, A.; Mai, P.L.; Khincha, P.P.; Loud, J.T.; Peters, J.A.; Achatz, M.I.; Chojniak, R.; Balieiro da Costa, A.; Santiago, K.M.; et al. Baseline Surveillance in Li-Fraumeni Syndrome Using Whole-Body Magnetic Resonance Imaging: A Meta-analysis. JAMA Oncol. 2017, 3, 1634–1639, Erratum in JAMA Oncol. 2018, 4, 590. [Google Scholar] [CrossRef]
- Petralia, G.; Zugni, F.; Summers, P.E.; Colombo, A.; Pricolo, P.; Grazioli, L.; Colagrande, S.; Giovagnoni, A.; Padhani, A.R.; on behalf of the Italian Working Group on Magnetic Resonance. Whole-body magnetic resonance imaging (WB-MRI) for cancer screening: Recommendations for use. Radiol. Med. 2021, 126, 1434–1450. [Google Scholar] [CrossRef]
- Benusiglio, P.R.; Brugières, L.; Caron, O. Whole-body MRI screening in children with Li-Fraumeni and other cancer predisposition syndromes. AJR 2016, 206, W52. [Google Scholar] [CrossRef]
- Tak, C.R.; Biltaji, E.; Kohlmann, W.; Maese, L.; Hainaut, P.; Villani, A.; Malkin, D.; Sherwin, C.M.T.; Brixner, D.I.; Schiffman, J.D. Cost-effectiveness of early cancer surveillance for patients with Li-Fraumeni syndrome. Pediatr. Blood Cancer 2019, 66, e27629. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).