
Complications and Outcomes in 39,864 Patients Receiving Standard Care Plus Mechanical Circulatory Support or Standard Care Alone for Infarct-Associated Cardiogenic Shock

 , , , , , , , ,
, , , , , , , ,
Abstract
1. Introduction
2. Methods
2.1. Data Source and Patient Selection
2.2. In-Hospital Treatment, Outcome, and Follow-Up
2.3. Endpoints
2.4. Statistical Methods
3. Results
3.1. In-Hospital Treatments and Complications
3.2. Length of Stay and In-Hospital Outcome
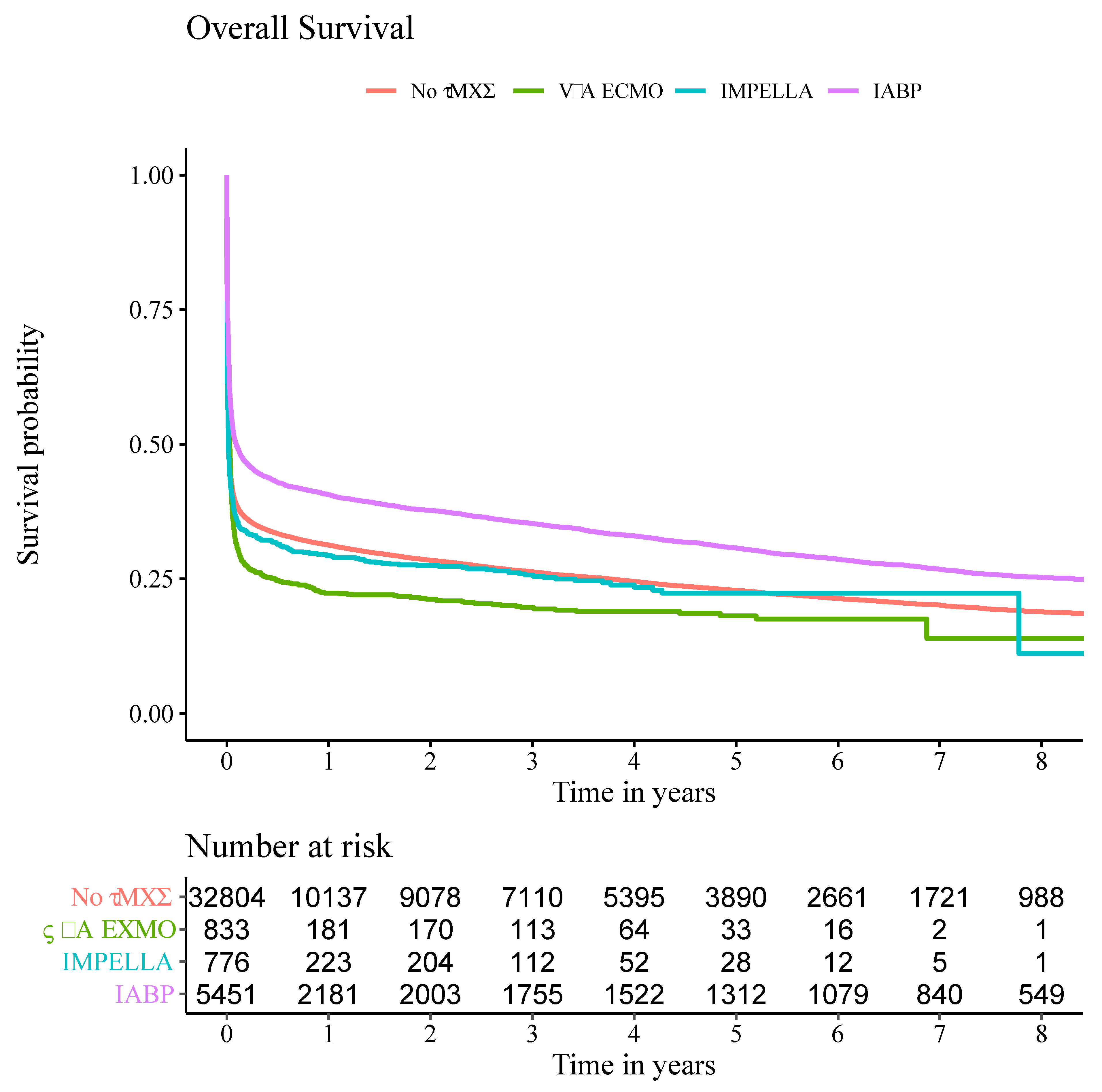
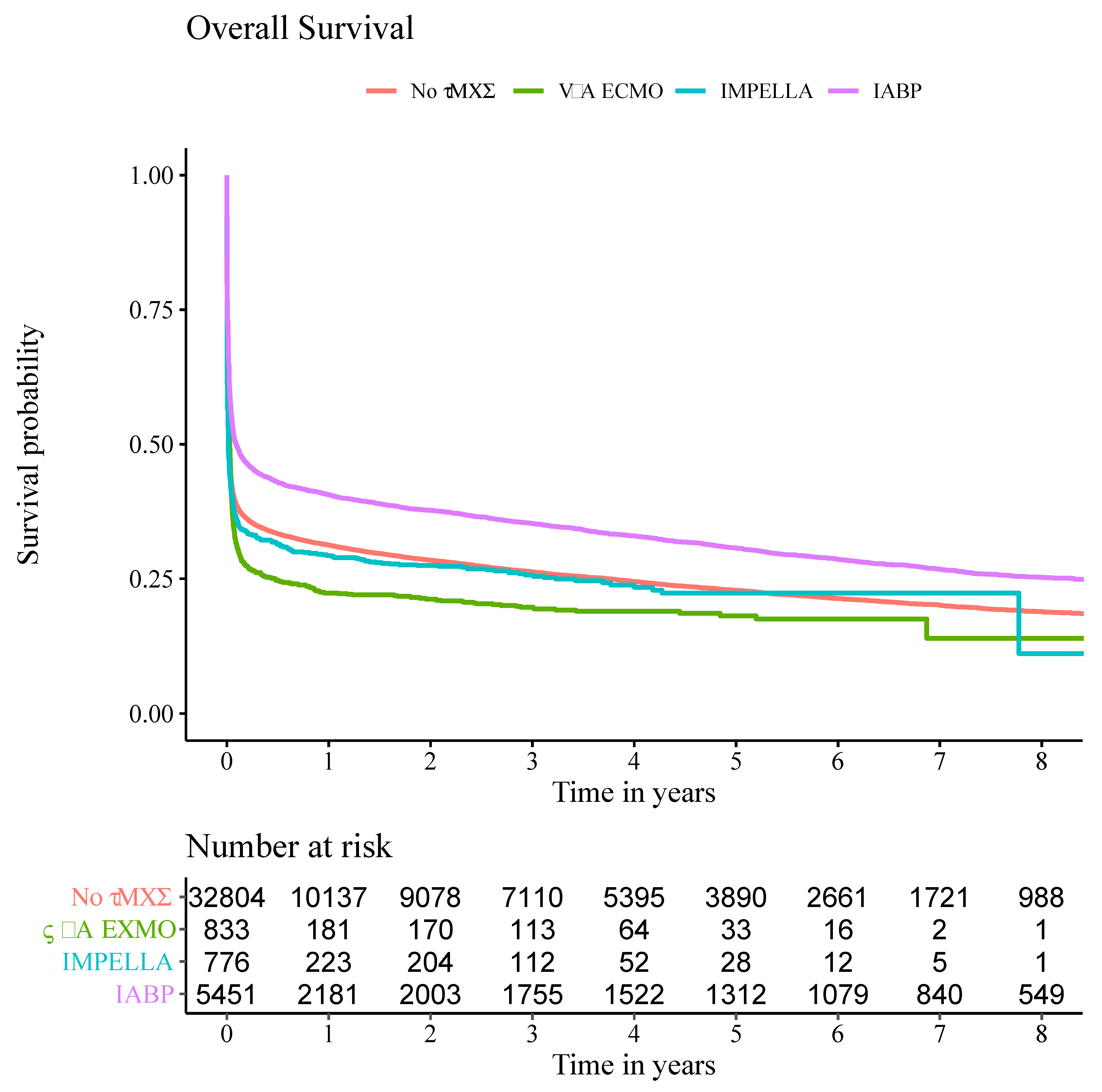
3.3. Overall Survival
4. Discussion
4.1. Overall Survival
4.2. Treatment Modalities and Complications
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pepe, M.; Bortone, A.S.; Giordano, A.; Cecere, A.; Burattini, O.; Nestola, P.L.; Patti, G.; Di Cillo, O.; Signore, N.; Forleo, C.; et al. Cardiogenic Shock Following Acute Myocardial Infarction: What’s New? Shock 2020, 53, 391–399. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation 2017, 136, e232–e268. [Google Scholar] [CrossRef] [PubMed]
- Babaev, A.; Frederick, P.D.; Pasta, D.J.; Every, N.; Sichrovsky, T.; Hochman, J.S.; Investigators, N. Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. JAMA 2005, 294, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Radovanovic, D.; Nallamothu, B.K.; Seifert, B.; Bertel, O.; Eberli, F.; Urban, P.; Pedrazzini, G.; Rickli, H.; Stauffer, J.C.; Windecker, S.; et al. Temporal trends in treatment of ST-elevation myocardial infarction among men and women in Switzerland between 1997 and 2011. Eur. Heart J. Acute Cardiovasc. Care 2012, 1, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Jeger, R.V.; Radovanovic, D.; Hunziker, P.R.; Pfisterer, M.E.; Stauffer, J.C.; Erne, P.; Urban, P.; Investigators, A.P.R. Ten-year trends in the incidence and treatment of cardiogenic shock. Ann. Intern. Med. 2008, 149, 618–626. [Google Scholar] [CrossRef]
- Sjauw, K.D.; Engstrom, A.E.; Vis, M.M.; van der Schaaf, R.J.; Baan, J., Jr.; Koch, K.T.; de Winter, R.J.; Piek, J.J.; Tijssen, J.G.; Henriques, J.P. A systematic review and meta-analysis of intra-aortic balloon pump therapy in ST-elevation myocardial infarction: Should we change the guidelines? Eur. Heart J. 2009, 30, 459–468. [Google Scholar] [CrossRef]
- Goldberg, R.J.; Spencer, F.A.; Gore, J.M.; Lessard, D.; Yarzebski, J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: A population-based perspective. Circulation 2009, 119, 1211–1219. [Google Scholar] [CrossRef]
- Hochman, J.S.; Buller, C.E.; Sleeper, L.A.; Boland, J.; Dzavik, V.; Sanborn, T.A.; Godfrey, E.; White, H.D.; Lim, J.; LeJemtel, T. Cardiogenic shock complicating acute myocardial infarction—Etiologies, management and outcome: A report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK? J. Am. Coll. Cardiol. 2000, 36, 1063–1070. [Google Scholar] [CrossRef]
- Lauridsen, M.D.; Rorth, R.; Lindholm, M.G.; Kjaergaard, J.; Schmidt, M.; Moller, J.E.; Hassager, C.; Torp-Pedersen, C.; Gislason, G.; Kober, L.; et al. Trends in first-time hospitalization, management, and short-term mortality in acute myocardial infarction-related cardiogenic shock from 2005 to 2017: A nationwide cohort study. Am. Heart J. 2020, 229, 127–137. [Google Scholar] [CrossRef]
- Hochman, J.S.; Sleeper, L.A.; Webb, J.G.; Sanborn, T.A.; White, H.D.; Talley, J.D.; Buller, C.E.; Jacobs, A.K.; Slater, J.N.; Col, J.; et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N. Engl. J. Med. 1999, 341, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Zeymer, U.; Neumann, F.J.; Ferenc, M.; Olbrich, H.G.; Hausleiter, J.; de Waha, A.; Richardt, G.; Hennersdorf, M.; Empen, K.; et al. Intra-aortic balloon counterpulsation in acute myocardial infarction complicated by cardiogenic shock (IABP-SHOCK II): Final 12 month results of a randomised, open-label trial. Lancet 2013, 382, 1638–1645. [Google Scholar] [CrossRef] [PubMed]
- Unverzagt, S.; Buerke, M.; de Waha, A.; Haerting, J.; Pietzner, D.; Seyfarth, M.; Thiele, H.; Werdan, K.; Zeymer, U.; Prondzinsky, R. Intra-aortic balloon pump counterpulsation (IABP) for myocardial infarction complicated by cardiogenic shock. Cochrane Database Syst. Rev. 2015, CD007398. [Google Scholar] [CrossRef]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Schrage, B.; Becher, P.M.; Bernhardt, A.; Bezerra, H.; Blankenberg, S.; Brunner, S.; Colson, P.; Cudemus Deseda, G.; Dabboura, S.; Eckner, D.; et al. Left Ventricular Unloading Is Associated With Lower Mortality in Patients With Cardiogenic Shock Treated With Venoarterial Extracorporeal Membrane Oxygenation: Results From an International, Multicenter Cohort Study. Circulation 2020, 142, 2095–2106. [Google Scholar] [CrossRef]
- Smith, M.; Vukomanovic, A.; Brodie, D.; Thiagarajan, R.; Rycus, P.; Buscher, H. Duration of veno-arterial extracorporeal life support (VA ECMO) and outcome: An analysis of the Extracorporeal Life Support Organization (ELSO) registry. Crit. Care 2017, 21, 45. [Google Scholar] [CrossRef]
- Seyfarth, M.; Sibbing, D.; Bauer, I.; Frohlich, G.; Bott-Flugel, L.; Byrne, R.; Dirschinger, J.; Kastrati, A.; Schomig, A. A randomized clinical trial to evaluate the safety and efficacy of a percutaneous left ventricular assist device versus intra-aortic balloon pumping for treatment of cardiogenic shock caused by myocardial infarction. J. Am. Coll. Cardiol. 2008, 52, 1584–1588. [Google Scholar] [CrossRef]
- Ouweneel, D.M.; Eriksen, E.; Seyfarth, M.; Henriques, J.P. Percutaneous Mechanical Circulatory Support Versus Intra-Aortic Balloon Pump for Treating Cardiogenic Shock: Meta-Analysis. J. Am. Coll. Cardiol. 2017, 69, 358–360. [Google Scholar] [CrossRef]
- Tsao, N.W.; Shih, C.M.; Yeh, J.S.; Kao, Y.T.; Hsieh, M.H.; Ou, K.L.; Chen, J.W.; Shyu, K.G.; Weng, Z.C.; Chang, N.C.; et al. Extracorporeal membrane oxygenation-assisted primary percutaneous coronary intervention may improve survival of patients with acute myocardial infarction complicated by profound cardiogenic shock. J. Crit. Care 2012, 27, 530.e1–530.e11. [Google Scholar] [CrossRef]
- Schrage, B.; Ibrahim, K.; Loehn, T.; Werner, N.; Sinning, J.M.; Pappalardo, F.; Pieri, M.; Skurk, C.; Lauten, A.; Landmesser, U.; et al. Impella Support for Acute Myocardial Infarction Complicated by Cardiogenic Shock. Circulation 2019, 139, 1249–1258. [Google Scholar] [CrossRef]
- Authors/Task Force Members; Windecker, S.; Kolh, P.; Alfonso, F.; Collet, J.P.; Cremer, J.; Falk, V.; Filippatos, G.; Hamm, C.; Head, S.J.; et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 2014, 35, 2541–2619. [Google Scholar] [CrossRef] [PubMed]
- Mehta, L.S.; Beckie, T.M.; DeVon, H.A.; Grines, C.L.; Krumholz, H.M.; Johnson, M.N.; Lindley, K.J.; Vaccarino, V.; Wang, T.Y.; Watson, K.E.; et al. Acute Myocardial Infarction in Women: A Scientific Statement From the American Heart Association. Circulation 2016, 133, 916–947. [Google Scholar] [CrossRef] [PubMed]
- Cenko, E.; Yoon, J.; Kedev, S.; Stankovic, G.; Vasiljevic, Z.; Krljanac, G.; Kalpak, O.; Ricci, B.; Milicic, D.; Manfrini, O.; et al. Sex Differences in Outcomes After STEMI: Effect Modification by Treatment Strategy and Age. JAMA Intern. Med. 2018, 178, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Kuehnemund, L.; Koeppe, J.; Feld, J.; Wiederhold, A.; Illner, J.; Makowski, L.; Gerss, J.; Reinecke, H.; Freisinger, E. Gender differences in acute myocardial infarction-A nationwide German real-life analysis from 2014 to 2017. Clin. Cardiol. 2021, 44, 890–898. [Google Scholar] [CrossRef]
- Lee, J.H.; Park, J.H.; Jang, J.H.; Kim, S.H.; Hong, S.Y.; Heo, W.; Lee, D.H.; Choi, H.S.; Kim, K.H.; Jang, H.J. The role of nafamostat mesilate as a regional anticoagulant during extracorporeal membrane oxygenation. Acute Crit. Care 2022, 37, 177–184. [Google Scholar] [CrossRef]
- Li, D.H.; Sun, M.W.; Zhang, J.C.; Zhang, C.; Deng, L.; Jiang, H. Is bivalirudin an alternative anticoagulant for extracorporeal membrane oxygenation (ECMO) patients? A systematic review and meta-analysis. Thromb. Res. 2022, 210, 53–62. [Google Scholar] [CrossRef]
- Sanfilippo, F.; La Via, L.; Murabito, P.; Pappalardo, F.; Astuto, M. More evidence available for the use of Bivalirudin in patients supported by extracorporeal membrane oxygenation. Thromb. Res. 2022, 211, 148–149. [Google Scholar] [CrossRef]
- Sheu, J.J.; Tsai, T.H.; Lee, F.Y.; Fang, H.Y.; Sun, C.K.; Leu, S.; Yang, C.H.; Chen, S.M.; Hang, C.L.; Hsieh, Y.K.; et al. Early extracorporeal membrane oxygenator-assisted primary percutaneous coronary intervention improved 30-day clinical outcomes in patients with ST-segment elevation myocardial infarction complicated with profound cardiogenic shock. Crit. Care Med. 2010, 38, 1810–1817. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| No tMCS (n = 32,804) | IABP (n = 5451) | Impella (n = 776) | V-A ECMO (n = 833) | p-Value | |
|---|---|---|---|---|---|
| Male, n (%) | 19,615 (59.8) | 3676 (67.4) | 541 (69.7) | 638 (76.6) | <0.001 |
| Age, median (IQR) | 75.64 (17.0) | 71.61 (16.8) | 70.61 (17.3) | 63.68 (16.9) | <0.001 |
| No of diseased coronary vessels: 0, n (%) | 7308 (22.3) | 283 (5.19) | 50 (6.44) | 63 (7.56) | <0.001 |
| No of diseased coronary vessels: 1, n (%) | 4056 (12.4) | 586 (10.8) | 86 (11.1) | 72 (8.64) | <0.001 |
| No of diseased coronary vessels: 2, n (%) | 5922 (18.1) | 938 (17.2) | 145 (18.7) | 145 (17.4) | <0.001 |
| No of diseased coronary vessels: 3, n (%) | 15,518 (47.3) | 3644 (66.9) | 495 (63.8) | 553 (66.4) | <0.001 |
| Arterial hypertension, n (%) | 28,907 (88.1) | 4680 (85.9) | 654 (84.3) | 675 (81.0) | <0.001 |
| Diabetes, n (%) | 17,073 (52.1) | 2820 (51.7) | 405 (52.2) | 425 (51.0) | 0.917 |
| Dyslipidemia, n (%) | 21,893 (66.7) | 3866 (70.9) | 544 (70.1) | 544 (65.3) | <0.001 |
| Obesitas, n (%) | 8850 (27.0) | 1587 (29.1) | 225 (29.0) | 249 (29.9) | 0.002 |
| Smoking, n (%) | 6522 (19.9) | 1223 (22.4) | 197 (25.4) | 265 (31.8) | <0.001 |
| Previous myocardial infarction, n (%) | 9653 (29.4) | 1883 (34.5) | 252 (32.5) | 261 (31.3) | <0.001 |
| Previous stroke, n (%) | 5097 (15.5) | 662 (12.1) | 92 (11.9) | 78 (9.36) | <0.001 |
| Previous PCI, n (%) | 2356 (7.18) | 449 (8.24) | 68 (8.76) | 76 (9.12) | 0.004 |
| Previous CABG, n (%) | 2728 (8.32) | 418 (7.67) | 58 (7.47) | 50 (6.00) | 0.037 |
| Previous valve replacement, n (%) | 429 (1.31) | 40 (0.73) | 0 (0) | 13 (1.56) | <0.001 |
| Chronic heart failure, n (%) | 23,244 (70.9) | 4187 (76.8) | 606 (78.09) | 670 (80.4) | <0.001 |
| Chronic kidney disease, n (%) | 14,090 (43.0) | 2187 (40.1) | 294 (37.9) | 307 (36.9) | <0.001 |
| Chronic kidney disease with dialysis, n (%) | 6340 (19.3) | 873 (16.0) | 136 (17.5) | 114 (13.7) | <0.001 |
| No tMCS (n = 32,804) | IABP (n = 5451) | Impella (n = 776) | V-A ECMO (n = 833) | p-Value | |
|---|---|---|---|---|---|
| PCI, n (%) | 21,460 (65.4) | 4070 (74.7) | 734 (94.6) | 659 (79.1) | <0.001 |
| CABG, n (%) | 1519 (4.63) | 1723 (31.6) | 18 (2.32) | 221 (26.5) | <0.001 |
| In-hospital resuscitation, n (%) | 13,769 (42.0) | 2298 (42.2) | 416 (53.6) | 537 (64.5) | <0.001 |
| Mechanical ventilation, n (%) | 20,975 (63.9) | 4345 (79.7) | 648 (83.5) | 757 (90.9) | <0.001 |
| Ventilation, median hours (IQR) | 32 (126) | 81 (200) | 41.5 (144) | 93 (281) | <0.001 |
| Acute kidney injury, n (%) | 8835 (26.9) | 1732 (31.8) | 341 (43.9) | 440 (52.8) | <0.001 |
| Renal replacement therapy, n (%) | 3975 (12.1) | 1590 (29.2) | 237 (30.5) | 419 (50.3) | <0.001 |
| Bleeding, n (%) | 3058 (9.32) | 980 (18.0) | 162 (20.9) | 317 (38.1) | <0.001 |
| Red blood cell transfusion, n (%) | 7131 (21.7) | 2954 (54.2) | 401 (51.7) | 736 (88.4) | <0.001 |
| Hemorrhagic stroke, n (%) | 249 (0.76) | 53 (0.97) | 12 (1.55) | 26 (3.12) | <0.001 |
| Ischemic stroke, n (%) | 1347 (4.11) | 289 (5.30) | 31 (3.99) | 80 (9.60) | <0.001 |
| Sepsis, n (%) | 3034 (9.25) | 757 (13.9) | 123 (15.9) | 187 (22.5) | <0.001 |
| Length of stay, median days (IQR) | 7 (16) | 13 (24) | 6 (22) | 12 (30) | <0.001 |
| Death (during index case), n (%) | 19,367 (59.0) | 2569 (47.1) | 482 (62.1) | 488 (58.6) | <0.001 |
| Death (after index case within case chain), n (%) | 969 (7.21) | 339 (11.8) | 35 (11.9) | 132 (38.3) | <0.001 |
| Total Death (within case chain), n (%) | 20,336 (62.0) | 2908 (53.4) | 517 (66.6) | 620 (74.4) | <0.001 |
| Comparison | Death (During Index Case) | Death (After Index Case) | Total Death (Within Case Chain) |
|---|---|---|---|
| No tMCS vs. tMCS | <0.001 | <0.001 | <0.001 |
| No tMCS vs. IABP | <0.001 | <0.001 | <0.001 |
| No tMCS vs. Impella | 0.09 | 0.002 | 0.009 |
| No tMCS vs. V-A ECMO | 0.79 | <0.001 | <0.001 |
| IABP vs. Impella | <0.001 | 0.94 | <0.001 |
| IABP vs. V-A ECMO | <0.001 | <0.001 | <0.001 |
| Impella vs. V-A ECMO | 0.15 | <0.001 | <0.001 |
| No tMCS | IABP | Impella | V-A ECMO | |
|---|---|---|---|---|
| 1 year estimators, % (95% CI) | 31.3 (30.8–31.8) | 40.6 (39.3–41.9) | 29.3 (26.1–32.5) | 22.4 (19.5–25.2) |
| 2 years estimators, % (95% CI) | 28.4 (28.0–28.9) | 37.7 (36.4–39.0) | 27.5 (24.3–30.6) | 21.3 (18.5–24.0) |
| 5 years estimators, % (95% CI) | 22.9 (22.4–23.4) | 30.7 (29.5–32.0) | 22.4 (18.9–25.8) | 18.1 (15.3–21.0) |
| 8 years estimators, % (95% CI) | 18.9 (18.4–19.4) | 25.3 (24.1–26.6) | 11.2 (0–26.8) | 14.0 (7.43–20.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padberg, J.-S.; Feld, J.; Padberg, L.; Köppe, J.; Makowski, L.; Gerß, J.; Dröge, P.; Ruhnke, T.; Günster, C.; Lange, S.A.; et al. Complications and Outcomes in 39,864 Patients Receiving Standard Care Plus Mechanical Circulatory Support or Standard Care Alone for Infarct-Associated Cardiogenic Shock. J. Clin. Med. 2024, 13, 1167. https://doi.org/10.3390/jcm13041167
Padberg J-S, Feld J, Padberg L, Köppe J, Makowski L, Gerß J, Dröge P, Ruhnke T, Günster C, Lange SA, et al. Complications and Outcomes in 39,864 Patients Receiving Standard Care Plus Mechanical Circulatory Support or Standard Care Alone for Infarct-Associated Cardiogenic Shock. Journal of Clinical Medicine. 2024; 13(4):1167. https://doi.org/10.3390/jcm13041167
Chicago/Turabian StylePadberg, Jan-Sören, Jannik Feld, Leonie Padberg, Jeanette Köppe, Lena Makowski, Joachim Gerß, Patrik Dröge, Thomas Ruhnke, Christian Günster, Stefan Andreas Lange, and et al. 2024. "Complications and Outcomes in 39,864 Patients Receiving Standard Care Plus Mechanical Circulatory Support or Standard Care Alone for Infarct-Associated Cardiogenic Shock" Journal of Clinical Medicine 13, no. 4: 1167. https://doi.org/10.3390/jcm13041167
APA StylePadberg, J.-S., Feld, J., Padberg, L., Köppe, J., Makowski, L., Gerß, J., Dröge, P., Ruhnke, T., Günster, C., Lange, S. A., & Reinecke, H. (2024). Complications and Outcomes in 39,864 Patients Receiving Standard Care Plus Mechanical Circulatory Support or Standard Care Alone for Infarct-Associated Cardiogenic Shock. Journal of Clinical Medicine, 13(4), 1167. https://doi.org/10.3390/jcm13041167