
Practical Considerations for Odevixibat Treatment in Patients with Progressive Familial Intrahepatic Cholestasis: A Single-Center Case Series

 ,
,  ,
,
Abstract
1. Introduction
2. Methods
Patients
3. Results
3.1. Patient Characteristics and Medical History
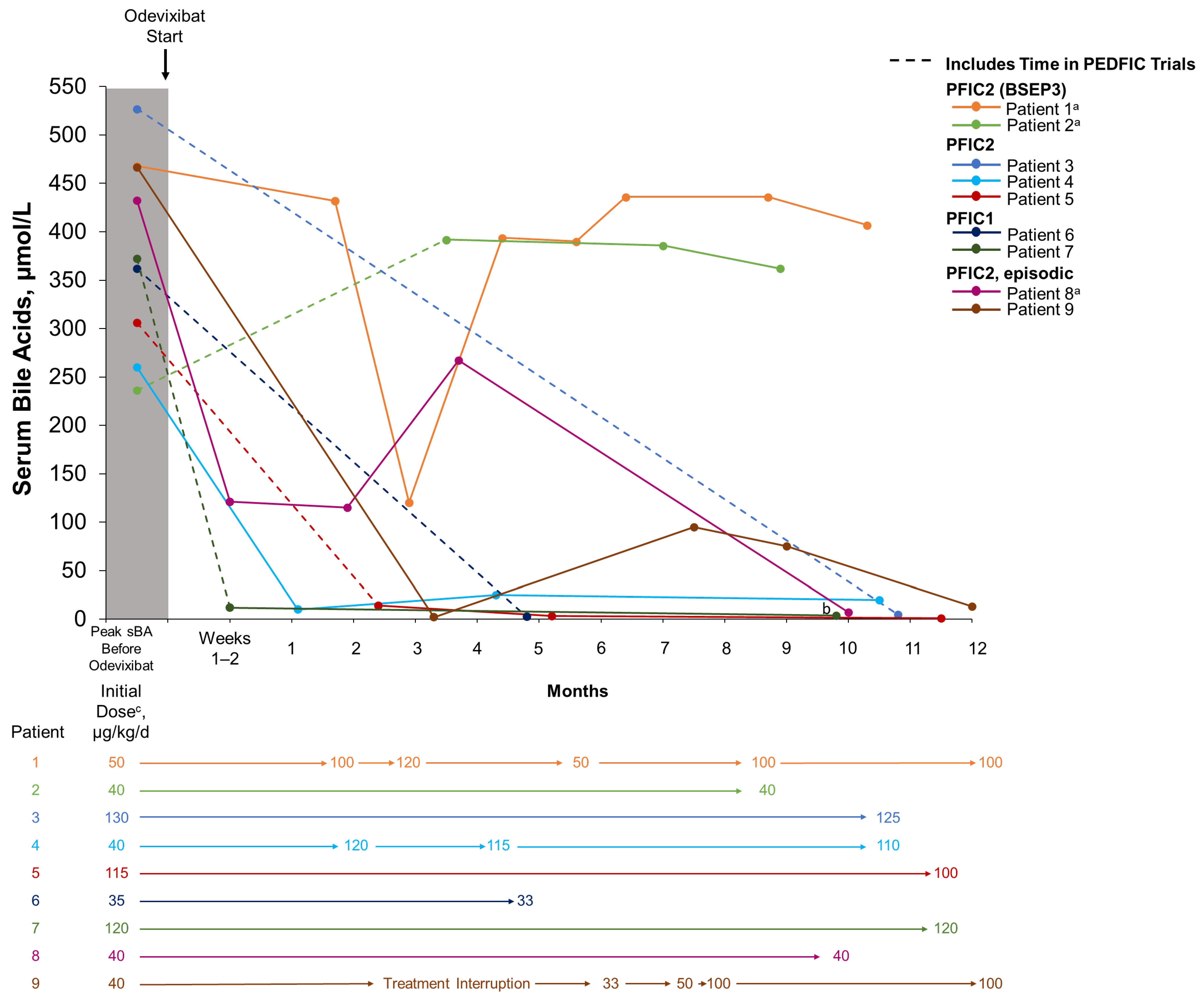
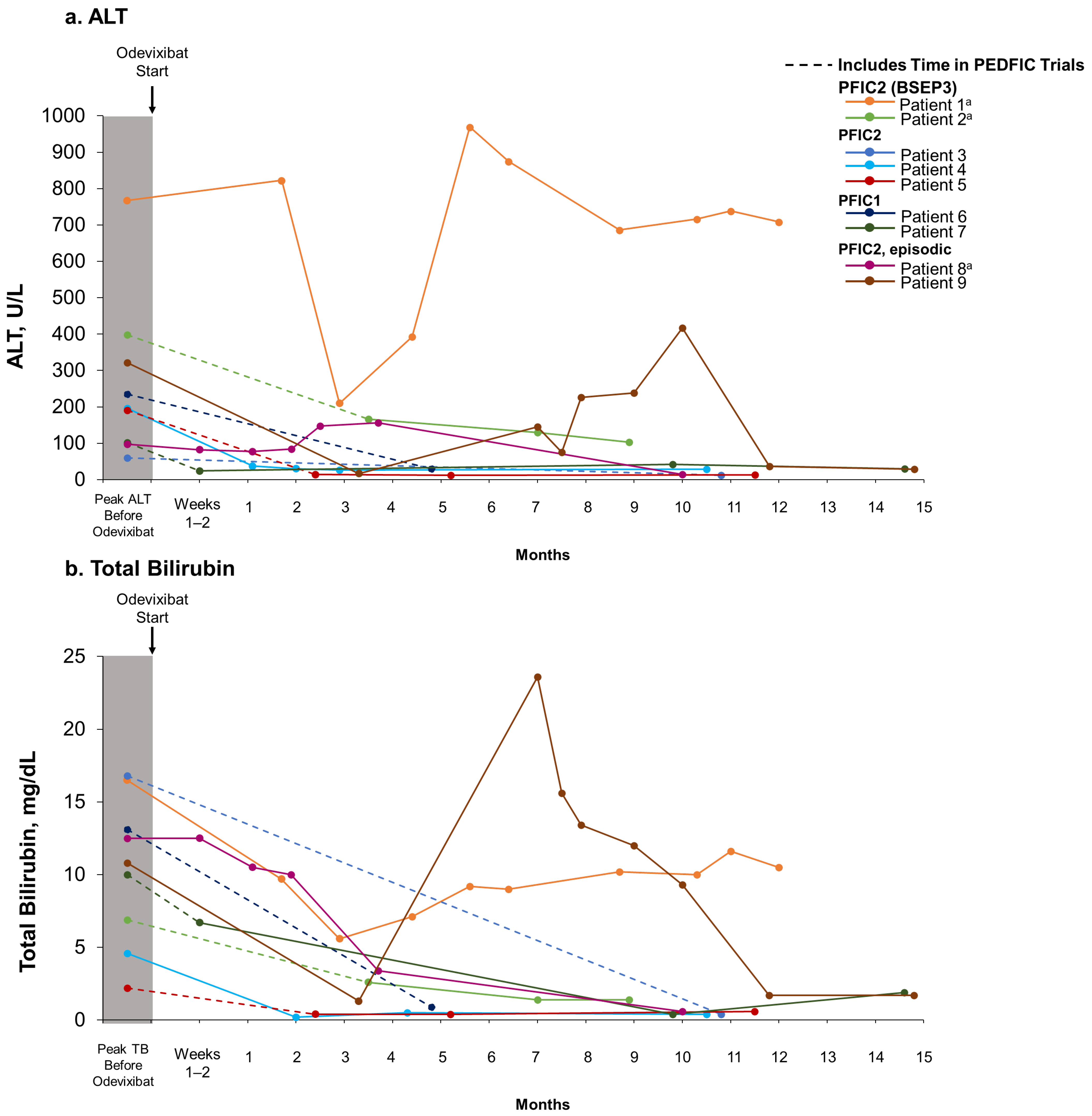
3.2. Odevixibat Treatment
3.3. Effectiveness and Safety with Odevixibat
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bull, L.N.; Thompson, R.J. Progressive familial intrahepatic cholestasis. Clin. Liver Dis. 2018, 22, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Henkel, S.A.; Squires, J.H.; Ayers, M.; Ganoza, A.; McKiernan, P.; Squires, J.E. Expanding etiology of progressive familial intrahepatic cholestasis. World J. Hepatol. 2019, 11, 450–463. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.; Kerkar, N.; Todorova, L.; Kamath, B.M.; Houwen, R.H.J. Systematic review of progressive familial intrahepatic cholestasis. Clin. Res. Hepatol. Gastroenterol. 2019, 43, 20–36. [Google Scholar] [CrossRef] [PubMed]
- van Wessel, D.B.E.; Thompson, R.J.; Gonzales, E.; Jankowska, I.; Sokal, E.; Grammatikopoulos, T.; Kadaristiana, A.; Jacquemin, E.; Spraul, A.; Lipiński, P.; et al. Genotype correlates with the natural history of severe bile salt export pump deficiency. J. Hepatol. 2020, 73, 84–93. [Google Scholar] [CrossRef]
- Amirneni, S.; Haep, N.; Gad, M.A.; Soto-Gutierrez, A.; Squires, J.E.; Florentino, R.M. Molecular overview of progressive familial intrahepatic cholestasis. World J. Gastroenterol. 2020, 26, 7470–7484. [Google Scholar] [CrossRef]
- van Wessel, D.B.E.; Thompson, R.J.; Gonzales, E.; Jankowska, I.; Shneider, B.L.; Sokal, E.; Grammatikopoulos, T.; Kadaristiana, A.; Jacquemin, E.; Spraul, A.; et al. Impact of genotype, serum bile acids, and surgical biliary diversion on native liver survival in FIC1 deficiency. Hepatology 2021, 74, 892–906. [Google Scholar] [CrossRef]
- Karpen, S.J.; Kelly, D.; Mack, C.; Stein, P. Ileal bile acid transporter inhibition as an anticholestatic therapeutic target in biliary atresia and other cholestatic disorders. Hepatol. Int. 2020, 14, 677–689. [Google Scholar] [CrossRef]
- Thebaut, A.; Debray, D.; Gonzales, E. An update on the physiopathology and therapeutic management of cholestatic pruritus in children. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 103–109. [Google Scholar] [CrossRef]
- Kamath, B.M.; Stein, P.; Houwen, R.H.J.; Verkade, H.J. Potential of ileal bile acid transporter inhibition as a therapeutic target in Alagille syndrome and progressive familial intrahepatic cholestasis. Liver Int. 2020, 40, 1812–1822. [Google Scholar] [CrossRef]
- Stapelbroek, J.M.; van Erpecum, K.J.; Klomp, L.W.; Houwen, R.H. Liver disease associated with canalicular transport defects: Current and future therapies. J. Hepatol. 2010, 52, 258–271. [Google Scholar] [CrossRef]
- van der Woerd, W.L.; Houwen, R.H.; van de Graaf, S.F. Current and future therapies for inherited cholestatic liver diseases. World J. Gastroenterol. 2017, 23, 763–775. [Google Scholar] [CrossRef] [PubMed]
- Graffner, H.; Gillberg, P.G.; Rikner, L.; Marschall, H.U. The ileal bile acid transporter inhibitor A4250 decreases serum bile acids by interrupting the enterohepatic circulation. Aliment. Pharmacol. Ther. 2016, 43, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Bylvay [Summary of Product Characteristics]; Ipsen Pharma: Boulogne-Billancourt, France, 2024.
- Bylvay [Package Insert]; Ipsen Biopharmaceuticals, Inc.: Cambridge, MA, USA, 2024.
- Kayfanda [Summary of Product Characteristics]; Ipsen Pharma: Boulogne-Billancourt, France, 2024.
- Thompson, R.J.; Arnell, H.; Artan, R.; Baumann, U.; Calvo, P.L.; Czubkowski, P.; Dalgic, B.; D’Antiga, L.; Durmaz, Ö.; Fischler, B.; et al. Odevixibat treatment in progressive familial intrahepatic cholestasis: A randomised, placebo-controlled, phase 3 trial. Lancet Gastroenterol. Hepatol. 2022, 7, 830–842. [Google Scholar] [CrossRef]
- Thompson, R.J.; Artan, R.; Baumann, U.; Calvo, P.L.; Czubkowski, P.; Dalgic, B.; D’antiga, L.; Di Giorgio, A.; Durmaz, Ö.; Gonzalès, E.; et al. Interim results from an ongoing, open-label, single-arm trial of odevixibat in progressive familial intrahepatic cholestasis. JHEP Rep. 2023, 5, 100782. [Google Scholar] [CrossRef] [PubMed]
- Slavetinsky, C.; Sturm, E. Odevixibat and partial external biliary diversion showed equal improvement of cholestasis in a patient with progressive familial intrahepatic cholestasis. BMJ Case Rep. 2020, 13, e234185. [Google Scholar] [CrossRef] [PubMed]
- Ohlendorf, J.; Goldschmidt, I.; Junge, N.; Laue, T.; Nasser, H.; Jäckel, E.; Mutschler, F.; Pfister, E.-D.; Herebian, D.; Keitel, V.; et al. Ileal bile acid transporter inhibition reduces post-transplant diarrhea and growth failure in FIC1 disease—A case report. Children 2022, 9, 669. [Google Scholar] [CrossRef]
- Pepe, A.; Colucci, A.; Carucci, M.; Nazzaro, L.; Bucci, C.; Ranucci, G.; Di Giorgio, A.; Vajro, P.; Mandato, C. Case Report: Add-on treatment with odevixibat in a new subtype of progressive familial intrahepatic cholestasis broadens the therapeutic horizon of genetic cholestasis. Front. Pediatr. 2023, 11, 1061535. [Google Scholar] [CrossRef]
- Di Giorgio, A.; Sciveres, M.; Fuoti, M.; Sonzogni, A.; Mandato, C.; D’Antiga, L. Treatment with an ileal bile acid transporter inhibitor in patients with TJP2 deficiency. Clin. Res. Hepatol. Gastroenterol. 2023, 47, 102185. [Google Scholar] [CrossRef]
- Nomden, M.; Kuipers, F.; Hulscher, J.B.F.; Lindström, E.; Valcheva, V.; Verkade, H.J. Odevixibat treatment induced biliary bile acid secretion in responsive patients with bile salt export pump deficiency. Gastroenterology 2023, 165, 496–498. [Google Scholar] [CrossRef]
- Flattmann, F.E.; Mohiuddin, F.S.; Singh, A.; Tandon, A.; Lockett, S.J.; Hirsch, J.D.; Mosieri, C.N.; Kaye, A.M.; Varrassi, G.; Ahmadzadeh, S.; et al. Odevixibat: A Novel Bile Salt Inhibitor Treatment for Pruritus in Progressive Familial Intrahepatic Cholestasis. Cureus 2024, 16, e56886. [Google Scholar] [CrossRef]
- Thompson, R.; Baumann, U.; Calvo, P.L.; D’Antiga, L.; Di Giorgio, A.; Gonzalès, E.; Grammatikopoulos, T.; Gupte, G.; Hardikar, W.; Kamath, B.M.; et al. Sustained long-term efficacy and safety of odevixibat in patients with progressive familial intrahepatic cholestasis: Results from the PEDFIC 2 phase III, open-label extension study [poster]. In Proceedings of the Annual Meeting of the American Association for the Study of Liver Diseases, San Diego, CA, USA, 15–19 November 2024. [Google Scholar]
- Sticova, E.; Jirsa, M.; Pawłowska, J. New insights in genetic cholestasis: From molecular mechanisms to clinical implications. Can. J. Gastroenterol. Hepatol. 2018, 2018, 2313675. [Google Scholar] [CrossRef] [PubMed]
- Di Giorgio, A.; Blokzijl, H.; Gonzales, E.M.; Salcedo, M.; Van Der Woerd, W.; Clemson, C.; Thevathasan, L.; Valcheva, V.; Valzasina, B.; Verkade, H.J. Odevixibat treatment in patients with recurrent episodic cholestasis and biallelic mutations in ATP8B1: A retrospective case series. Hepatology 2022, 76, S1551–S1552. [Google Scholar]
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age at Last Assessment, Years | Age at Genetic Diagnosis, Years | Diagnosis | Gene (DNA Mutations) | Medical History, Leading Signs and Symptoms, and Procedures | Maximum Symptom Severity Before Odevixibat a | Peak a sBA, μmol/L | Peak a TB, mg/dL | Peak a ALT/ AST, U/L | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pruritus | Sleep Disturbance | ||||||||||
| 1 | M | 1.8 | 0.1 | PFIC2 (BSEP3) b | ABCB11 (c.1966_1967delTT; c.3722T>C) | Neonatal cholestasis; jaundice, failure to thrive; PEG c | Severe | Mild | 468 | 16.5 | 768/ 938 |
| 2 | F | 6.4 | 0.5 | PFIC2 (BSEP3) b | ABCB11 (c.1966_1967delTT; c.3722T>C) | Vitamin K deficiency hemorrhage; apathetic, vomiting, failure to thrive; PEG c | Severe | Severe | 236 | 6.9 | 398/ 538 |
| 3 | M | 5.3 | 1.1 | PFIC2 | ABCB11 (c.992C>T; c.640G>A) | Jaundice | Severe | Severe | 527 | 16.8 | 60/ 135 |
| 4 | M | 1.3 | 0.3 | PFIC2 | ABCB11 (c.409G>A; c.833G>A) | Neonatal cholestasis; intermittent discolored stools, jaundice | Severe | Severe | 260 | 4.6 | 196/ 191 |
| 5 | M | 4.9 | 0.7 | PFIC2 | ABCB11 d (c.1445A>G; c.3083C>T) | Vitamin K deficiency hemorrhage; transaminase elevation | Severe | Severe | 306 | 2.2 | 191/ 144 |
| 6 | M | 18.8 | 15.1 | PFIC1 | ATP8B1 e (c.1982T>C; c.2097+2T>C) | Cholestasis with low GGT; jaundice, fatigue, vomiting, not able to perform; nasobiliary tube f | Severe | Severe | 362 | 13.1 | 235/ 158 |
| 7 | F | 6.6 | 0.6 | PFIC1 | ATP8B1 (c.2854C>T; c.2600G>A) | Jaundice | Severe | Severe | 373 | 10 | 102/ 120 |
| 8 | M | 15.8 | ~1 | PFIC2 b | ABCB11 (c.278A>C; c.463A>C) | Neonatal cholestasis; jaundice | Severe g | Severe g | 433 | 12.5 | 97/ 57 |
| 9 | M | 22.9 | 9.2 | PFIC2 | ABCB11 (c.278A>C; c.463A>C) | Transient neonatal cholestasis, coagulation disorder; jaundice; nasobiliary tube h | Severe g | Severe g | 467 | 10.8 | 322/ 186 |
| Patient | Observation Time Before Starting Odevixibat or Entering into the PEDFIC Trials, Years | Time in PEDFIC Trials, Months | Age at Start of Real-World Odevixibat, Years | Odevixibat Treatment Duration Outside of PEDFIC Trials a, Months | Starting Dose b, µg/kg/d | Current Dose a, µg/kg/d |
|---|---|---|---|---|---|---|
| 1 | 0.9 | − | 1 | 12 | 50 | 100 c |
| 2 | 1.8 | 5 (PEDFIC 1) 22 (PEDFIC 2) | 5.7 | 9 | 40 | 40 |
| 3 | 0.5 | 31 (PEDFIC 1 + 2) | 4.1 | 11 | 130 | 125 |
| 4 | 0.3 | − | 0.5 | 11 | 40 | 120 |
| 5 | 1.1 | 30 (PEDFIC 1 + 2) | 3.8 | 12 | 115 | 100 |
| 6 | 2.3 | 17 (PEDFIC 2) | 18.2 | 5 | 40 | 33 |
| 7 | 1.8 | 41 (PEDFIC 2) | 5.5 | 14 | 120 | 120 |
| 8 | 14.4 | − | 15 | 10 | 40 | 40 |
| 9 | 13.1 | − | 21.7 | 15 d | 40 | 100 e |
| Patient | Physician-Reported Change in Signs and Symptoms After Odevixibat | Physician and/or Caregiver-Reported Adverse Events or Side Effects | Caregiver-Reported Outcomes | Caregiver-Reported Ease of Administration | ||
|---|---|---|---|---|---|---|
| Global Satisfaction (0–4) a | Current Pruritus Assessment (VAS 0–10) b | Current Sleep Disturbance | ||||
| 1 | Consistent pruritus improvement Stools a little more fluid Liver transplantation c | None | 3 | 3–4 | From time to time | Easy |
| 2 | No consistent pruritus improvement Liver transplantation d | None | 1 | 6–8 | Yes | Difficult e |
| 3 | Completely resolved symptoms Normal everyday life | Slightly more liquid stool 1–2×/day | 4 | 0 | No | Very easy |
| 4 | Significant reduction in pruritus | None | 4 | 0 | No | Very easy |
| 5 | Pruritus and sleep disturbance absent No evidence of GI side effects | None | 4 | 0 | No | Easy |
| 6 | All symptoms f completely gone | Diarrhea 1–2×/day | 4 | 0 | No | Very easy |
| 7 | No pruritus Good thriving Softer stool consistency | Softer stool consistency Stool 2–3×/day | 4 | 0 | No | Easy |
| 8 | No pruritus Protracted hyperbilirubinemia (3–10 mg/dL) Infection-triggered relapses | None | 4 | 0 | No | Very easy |
| 9 | Pruritus and sleep disturbance absent Diarrhea 1–2× daily Infection-triggered relapses | Transient abdominal cramps and watery stools; no complaints after introductory phase | 4 | 0 | No | Very easy |
| Patient | Vitamin Supplements Before Starting Any Odevixibat Treatment | Vitamin Supplements During Odevixibat Treatment | ||
|---|---|---|---|---|
| Vitamin | Dose | Vitamin | Dose | |
| 1 | DEKAs Vitamin Essential a | 1 × 1 mL | DEKAs Vitamin Essential a | 1 × 0.5 mL |
| 2 | Vitamin D | 1000 IE | Vitamin D | 1000 IE |
| Vitamin E | 111 IE | Vitamin E | 111 IE | |
| Vitamin K | 3 mg 3×/week | Vitamin K | 3 mg 3×/week | |
| 3 | Vitamin A | 3 × 4000 IE | None | NA |
| Vitamin D | 500 IE | |||
| Vitamin E | 3 × 111 IE | |||
| Vitamin K | 2 mg 1×/week | |||
| 4 | Vitamin A | 7500 IE | None | NA |
| Vitamin D | 3000 IE | |||
| Vitamin E | 105 IE | |||
| Vitamin K | 3 mg | |||
| 5 | Vitamin A | 1 × 20,000 IE | Vitamin A Vitamin D Vitamin K | 1 × 20,000 IE 1 × 2000 IE 2 mg 3×/week |
| Vitamin D | 3000 IE daily | |||
| Vitamin E | 1 × 225 IE | |||
| Vitamin K | 2 mg 3×/week | |||
| 6 | Vitamin D | 2000 IE | Vitamin D | 2000 IE |
| Vitamin K | 5 mg | |||
| 7 | Vitamin D | 2000 IE | None | NA |
| 8 | None | NA | Vitamin K | 1 × 10 mg |
| 9 | None | NA | None | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marx, M.; Hartleif, S.; Hilberath, J.; Berg, C.P.; Tsiflikas, I.; Singer, S.; Sturm, E. Practical Considerations for Odevixibat Treatment in Patients with Progressive Familial Intrahepatic Cholestasis: A Single-Center Case Series. J. Clin. Med. 2024, 13, 7508. https://doi.org/10.3390/jcm13247508
Marx M, Hartleif S, Hilberath J, Berg CP, Tsiflikas I, Singer S, Sturm E. Practical Considerations for Odevixibat Treatment in Patients with Progressive Familial Intrahepatic Cholestasis: A Single-Center Case Series. Journal of Clinical Medicine. 2024; 13(24):7508. https://doi.org/10.3390/jcm13247508
Chicago/Turabian StyleMarx, Milena, Steffen Hartleif, Johannes Hilberath, Christoph P. Berg, Ilias Tsiflikas, Stephan Singer, and Ekkehard Sturm. 2024. "Practical Considerations for Odevixibat Treatment in Patients with Progressive Familial Intrahepatic Cholestasis: A Single-Center Case Series" Journal of Clinical Medicine 13, no. 24: 7508. https://doi.org/10.3390/jcm13247508
APA StyleMarx, M., Hartleif, S., Hilberath, J., Berg, C. P., Tsiflikas, I., Singer, S., & Sturm, E. (2024). Practical Considerations for Odevixibat Treatment in Patients with Progressive Familial Intrahepatic Cholestasis: A Single-Center Case Series. Journal of Clinical Medicine, 13(24), 7508. https://doi.org/10.3390/jcm13247508