
Lactate to Albumin Ratio and Mortality in Patients with Severe Coronavirus Disease-2019 Admitted to an Intensive Care Unit

 , , , ,
, , , ,  , and
, and 
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
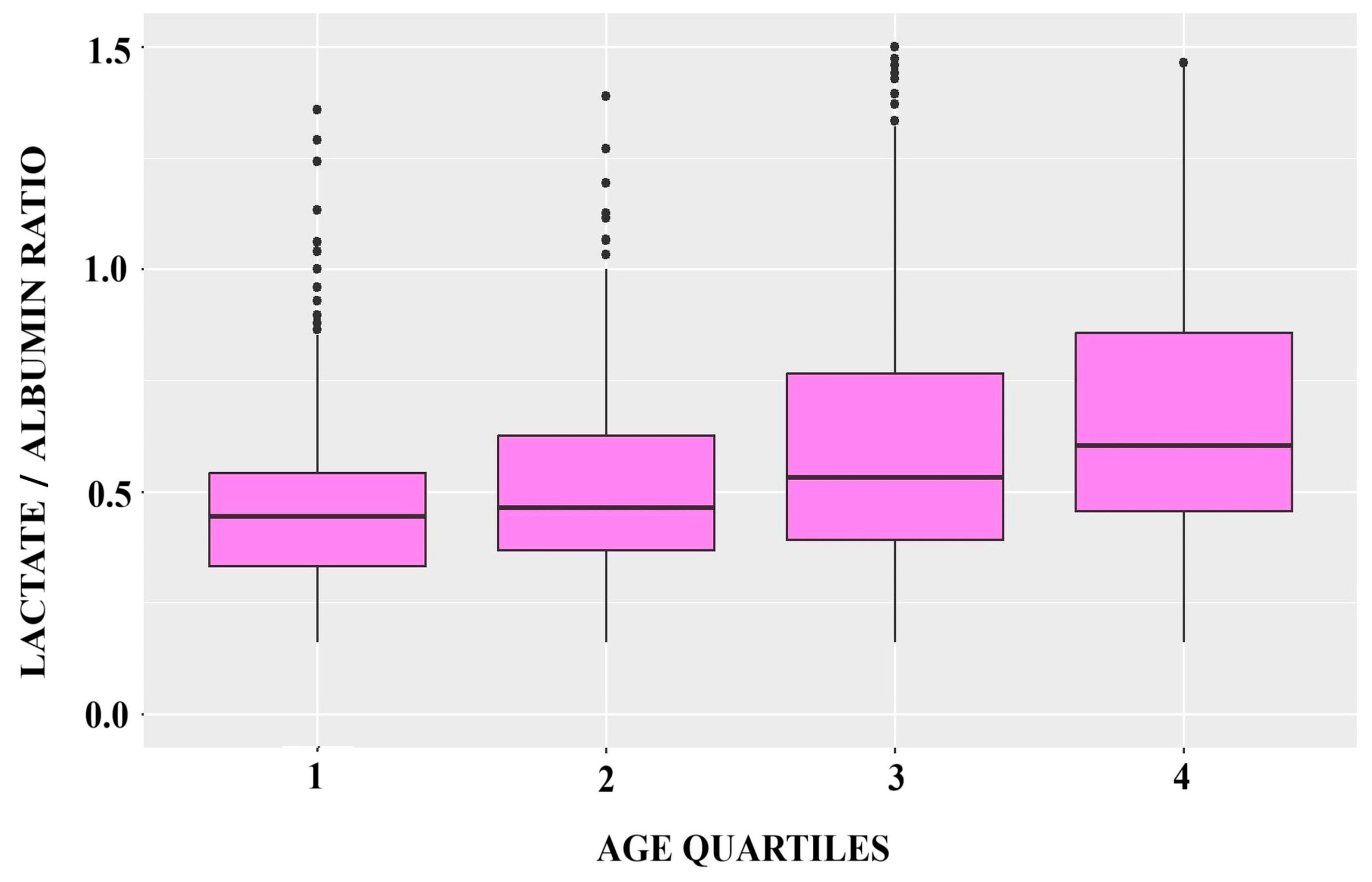
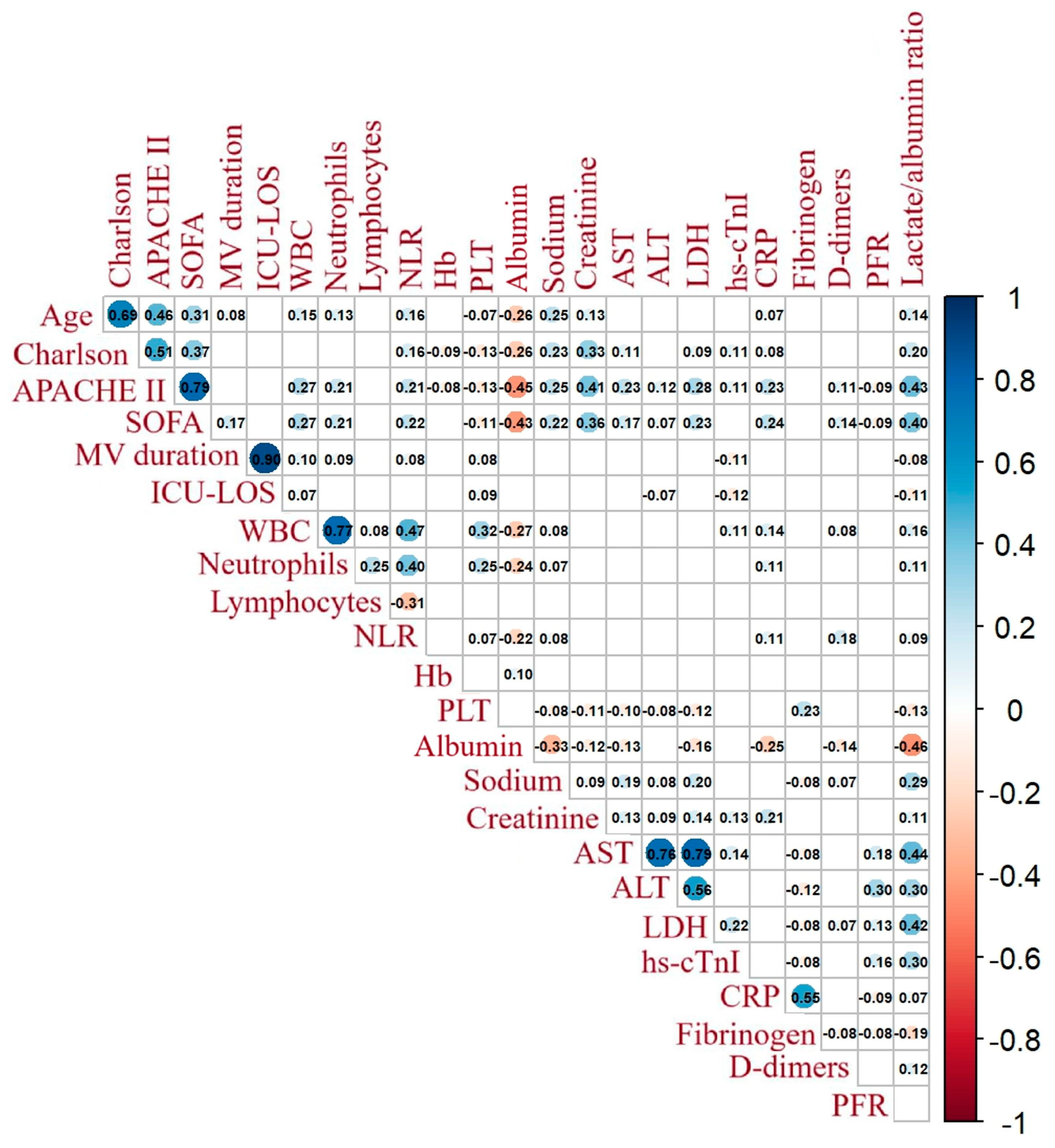
3.2. Correlations of Lactate/Albumin Ratio with Other Variables
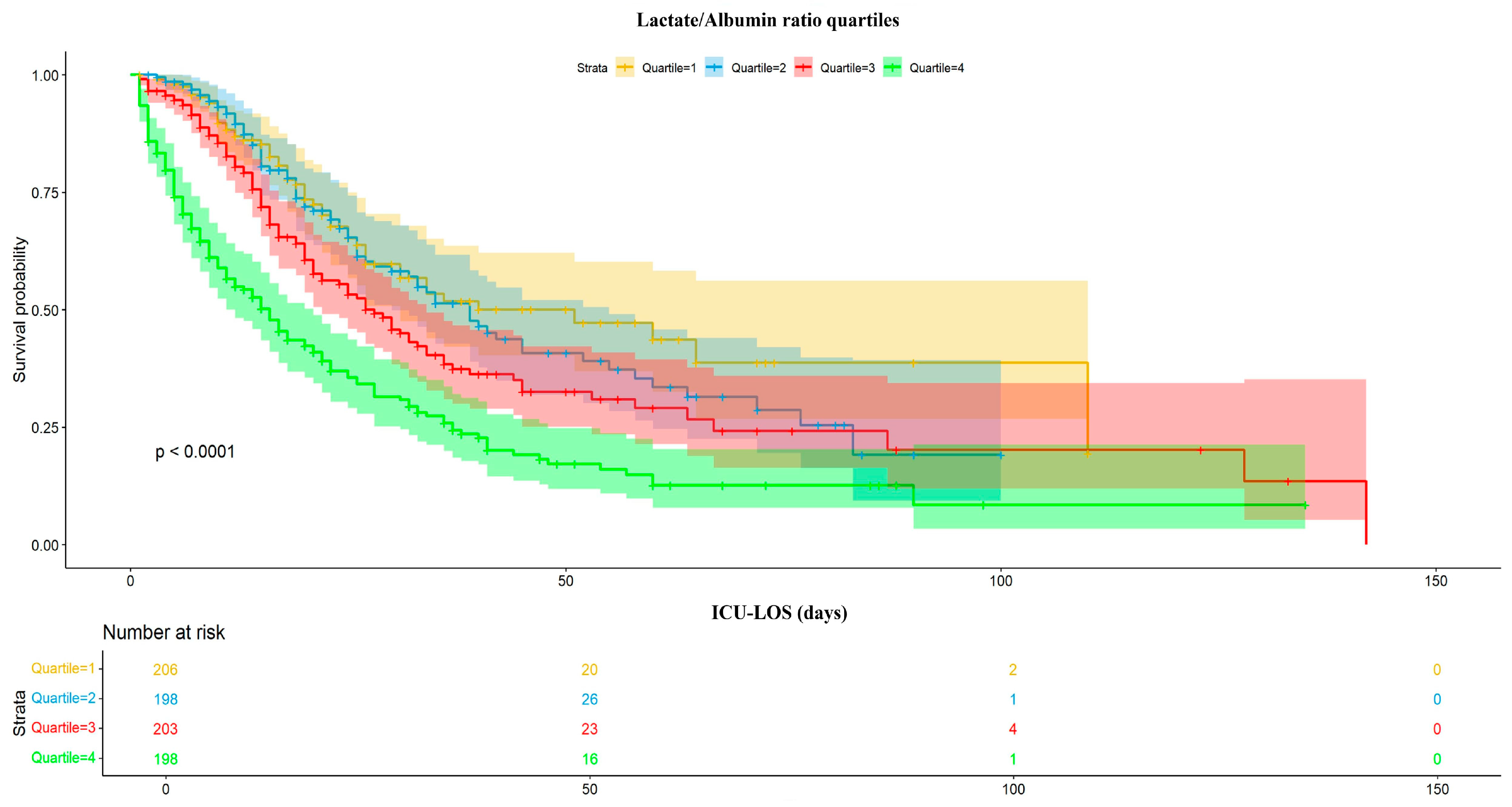
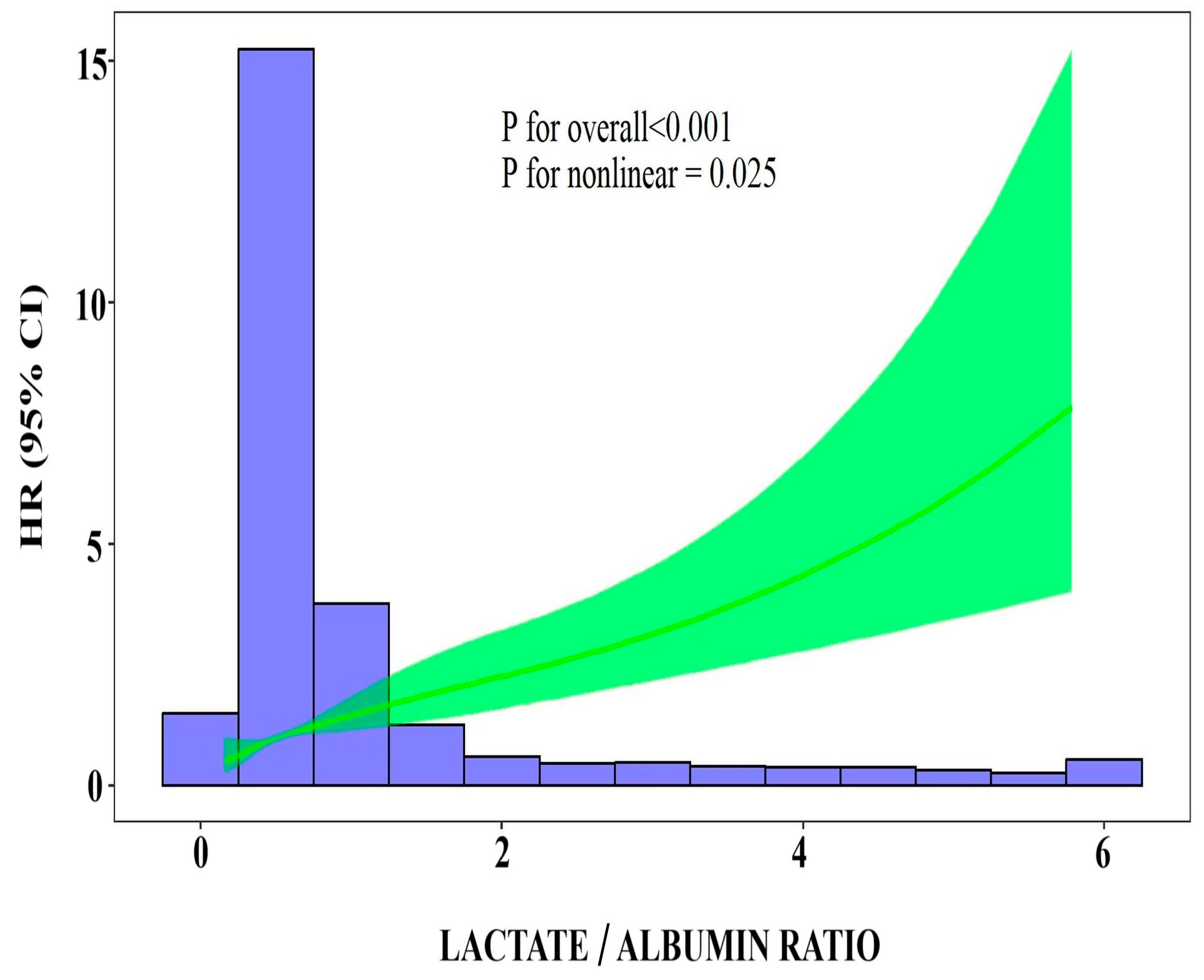
3.3. Survival Analysis
3.4. ROC Curves Analysis
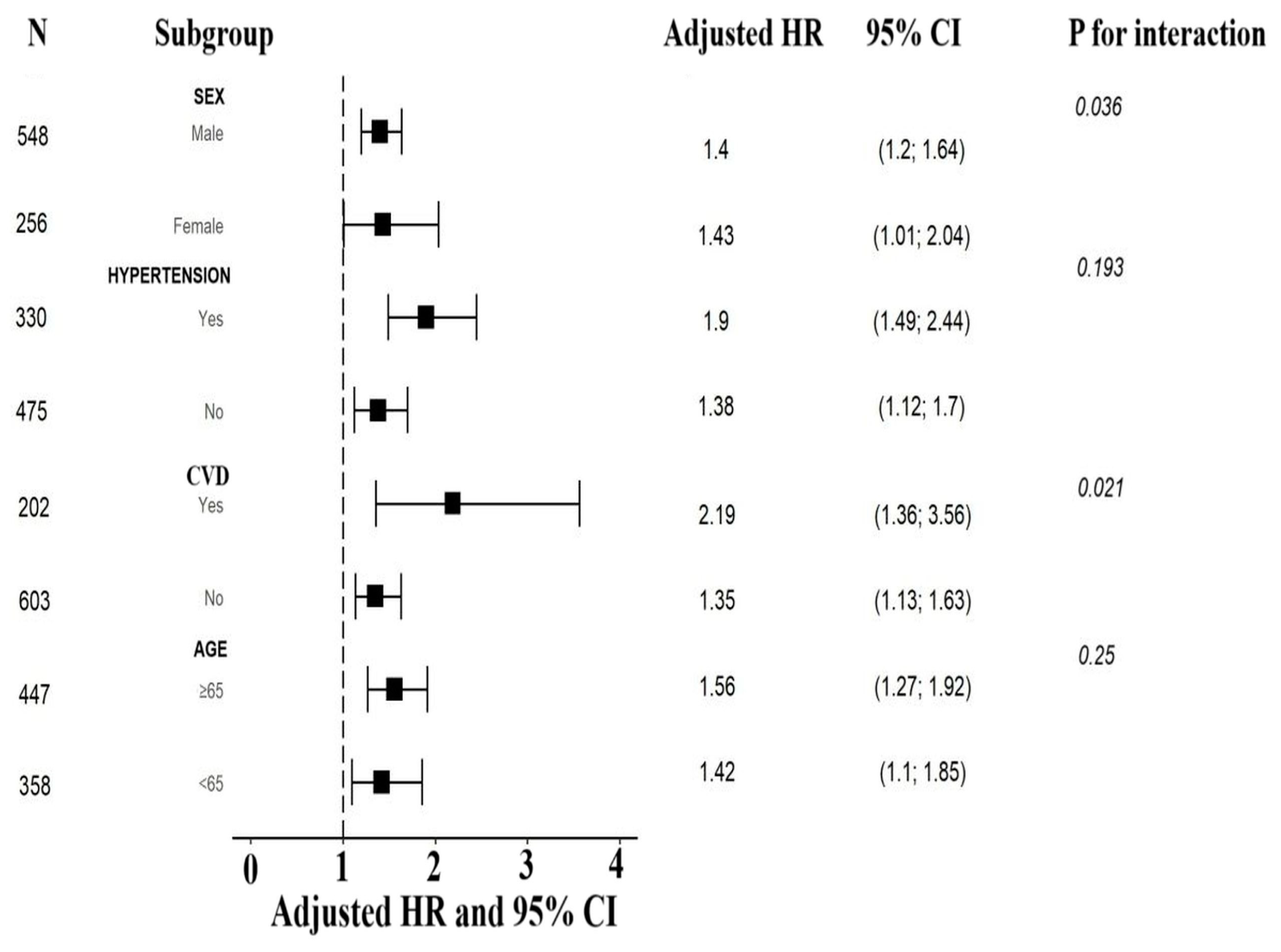
3.5. Subgroup Analyses
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rashkin, M.; Boxkin, C.; Baughman, R. Oxygen delivery in critically ill patients: Relationship to blood lactate and survival. Chest 1985, 87, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Bakker, J.; Vincent, J.-L. The oxygen-supply dependency phenomenon is associated with increased blood lactate levels. J. Crit. Care 1991, 6, 152–159. [Google Scholar] [CrossRef]
- Kraut, J.A.; Madias, N.E. Lactic Acidosis. N. Engl. J. Med. 2014, 371, 2309–2319. [Google Scholar] [CrossRef] [PubMed]
- Gibot, S. On the origins of lactate during sepsis. Crit. Care 2012, 16, 151. [Google Scholar] [CrossRef]
- Routsi, C.; Bardouniotou, E.; Delivoria-loannidou, V.; Kazi, D.; Roussos, C.; Zakynthinos, S. Pulmonary lactate release in patients with acute lung injury is not attributable to lung tissue hypoxia. Crit. Care Med. 1999, 27, 2469–2473. [Google Scholar] [CrossRef]
- Michaeli, B.; Martinez, A.; Revelly, J.P.; Cayeux, M.C.; Chioléro, R.L.; Tappy, L.; Berger, M.M. Effects of endotoxin on lactate metabolism in humans. Crit. Care 2012, 16, R139. [Google Scholar] [CrossRef]
- Bakker, J.; Coffernil, M.; Leon, M.; Gris, P.; Vincent, J.L. Blood Lactate Levels Are Superior to Oxygen-Derived Variables in Predicting Outcome in Human Septic Shock. Chest 1991, 99, 956–962. [Google Scholar] [CrossRef]
- Bakker, J.; Nijsten, M.W.; Jansen, T.C. Clinical use of lactate monitoring in critically ill patients. Ann. Intensive Care 2013, 3, 12. [Google Scholar] [CrossRef]
- Fleck, A.; Raines, G.; Hawker, F.; Trotter, J.; Wallace, P.I.; Lendingham, I.M.; Calman, K.C. Increased vascular permeability: A major cause of hypoalbuminaemia in disease and injury. Lancet 1985, 1, 781–784. [Google Scholar] [CrossRef]
- Soeters, P.B.; Wolfe, R.R.; Shenkin, A. Hypoalbuminemia: Pathogenesis and clinical significance. J. Parenter. Enteral Nutr. 2019, 43, 181–193. [Google Scholar] [CrossRef]
- Arnau-Barres, I.; Guerri-Fernandez, R.; Luque, S.; Sorli, L.; Vázquez, O.; Miralles, R. Serum albumin is a strong predictor of sepsis outcome in elderly patients. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 743–746. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Chen, G.; Cao, Y.; Xue, J.; Li, J.; Wu, Y. Correlation of lactate/albumin ratio level to organ failure and mortality in severe sepsis and septic shock. J. Crit. Care 2015, 30, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Hwang, S.Y.; Jo, I.J.; Kim, W.Y.; Ryoo, S.M.; Kang, G.H.; Kim, K.; Jo, Y.H.; Chung, S.P.; Joo, Y.S.; et al. Prognostic value of the lactate/albumin ratio for predicting 28-day mortality in critically ill sepsis patients. Shock 2018, 50, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Cakir, E.; Turan, O. Lactate/albumin ratio is more effective than lactate or albumin alone in predicting clinical outcomes in intensive care patients with sepsis. Scand. J. Clin. Lab. Investig. 2021, 81, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Lichtenauer, M.; Wernly, B.; Ohnewein, B.; Franz, M.; Kabisch, B.; Muessig, J.; IMasyuk, M.; Lauten, A.; Schulze, P.C.; Hoppe, U.C.; et al. The Lactate/Albumin Ratio: A Valuable Tool for Risk Stratification in Septic Patients Admitted to ICU. Int. J. Mol. Sci. 2017, 18, 1893. [Google Scholar] [CrossRef]
- Chen, Q.; Zhan, H.; Chen, J.; Mo, J.; Huang, S. Predictive value of lactate/albumin ratio for death and multiple organ dysfunction syndrome in patients with sepsis. J. Med. Biochem. 2024, 43, 617–625. [Google Scholar] [CrossRef]
- Shadvar, K.; Nader-Djalal, N.; Vahed, N.; Sanaie, S.; Iranpour, A.; Mahmoodpoor, A.; Vahedian-Azimi, A.; Samim, A.; Rahimi-Bashar, F. Comparison of lactate/albumin ratio to lactate and lactate clearance for predicting outcomes in patients with septic shock admitted to intensive care unit: An observational study. Sci. Rep. 2022, 12, 1304. [Google Scholar] [CrossRef]
- Bou Chebl, R.; Jamali, S.; Sabra, M.; Safa, R.; Berbari, I.; Shami, A.; Makki, M.; Tamim, H.; Abou Dagher, G. Lactate/Albumin Ratio as a Predictor of In-Hospital Mortality in Septic Patients Presenting to the Emergency Department. Front. Med. 2020, 7, 550182. [Google Scholar] [CrossRef]
- Gharipour, A.; Razavi, R.; Gharipour, M.; Mukasa, D. Lactate/albumin ratio: An early prognostic marker in critically ill patients. Am. J. Emerg. Med. 2020, 38, 2088–2095. [Google Scholar] [CrossRef]
- Karakike, E.; Giamarellos-Bourboulis, E.J.; Kyprianou, M.; Fleischmann-Struzek, C.; Pletz, M.W.; Netea, M.G.; Reinhart, K.; Kyriazopoulou, E. Coronavirus disease 2019 as cause of viral sepsis: A systematic review and meta-analysis. Crit. Care Med 2021, 49, 2042–2057. [Google Scholar] [CrossRef]
- Bergersen, K.V.; Pham, K.; Li, J.; Ulrich, M.T.; Merrill, P.; He, Y.; Alaama, S.; Qiu, X.; Harahap-Carrillo, I.S.; Ichii, K.; et al. Health disparities in COVID-19: Immune and vascular changes are linked to disease severity and persist in a high-risk population in Riverside County, California. BMC Public Health 2023, 23, 584. [Google Scholar] [CrossRef]
- Kokkoris, S.; Kanavou, A.; Katsaros, D.; Karageorgiou, S.; Kremmydas, P.; Gkoufa, A.; Ntaidou, T.; Giannopoulos, C.; Kardamitsi, M.A.; Dimopoulou, G.; et al. Temporal trends in laboratory parameters in survivors and non-survivors of critical COVID-19 illness and the effect of dexamethasone treatment. Biomed. Rep. 2023, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Su, C.; Hoffman, K.L.; Xu, Z.; Sanchez, E.; Siempos, I.I.; Harrington, J.S.; Racanelli, A.C.; Plataki, M.; Wang, F.; Schenck, E.J. Evaluation of Albumin Kinetics in Critically Ill Patients with Coronavirus Disease 2019 Compared to Those with Sepsis-Induced Acute Respiratory Distress Syndrome. Crit. Care Explor. 2021, 3, e0589. [Google Scholar] [CrossRef] [PubMed]
- Carpenè, G.; Onorato, D.; Nocini, R.; Fortunato, G.; Rizk, J.G.; Henry, B.M.; Lippi, G. Blood lactate concentration in COVID-19: A systematic literature review. Clin. Chem. Lab. Med. 2021, 60, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Vassiliou, A.G.; Tsipilis, S.; Keskinidou, C.; Vrettou, C.S.; Jahaj, E.; Gallos, P.; Routsi, C.; Orfanos, S.E.; Kotanidou, A.; Dimopoulou, I. Lactate and Lactate-to-Pyruvate Ratio in Critically Ill COVID-19 Patients: A Pilot Study. J. Pers. Med. 2022, 12, 171. [Google Scholar] [CrossRef]
- Iepsen, U.W.; Plovsing, R.R.; Tjelle, K.; Foss, N.B.; Meyhoff, C.S.; Ryrsø, C.K.; Berg, R.M.G.; Secher, N.H. The role of lactate in sepsis and COVID-19: Perspective from contracting skeletal muscle metabolism. Exp. Physiol. 2022, 107, 665–673. [Google Scholar] [CrossRef]
- Routsi, C.; Magira, E.; Kokkoris, S.; Siempos, I.; Vrettou, C.; Zervakis, D.; Ischaki, E.; Malahias, S.; Sigala, I.; Asimakos, A.; et al. Hospital resources may be an important aspect of mortality rate among critically ill patients with COVID-19: The paradigm of Greece. J. Clin. Med. 2020, 9, 3730. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.; Jaeschke, R.; Mebazaa, A.; Pinsky, M.R.; Teboul, J.L.; et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.H.; Heo, M.; Lee, S.J.; Jeong, Y.Y.; Lee, J.D.; Yoo, J.W. Clinical Usefulness of Red Cell Distribution Width/Albumin Ratio to Discriminate 28-Day Mortality in Critically Ill Patients with Pneumonia Receiving Invasive Mechanical Ventilation, Compared with Lacate/Albumin Ratio: A Retrospective Cohort Study. Diagnostics 2021, 11, 2344. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Kang, Q.; Wang, F.; Yu, W. Association of lactate/albumin ratio with in-hospital mortality in ICU patients with acute respiratory failure: A retrospective analysis based on MIMIC-IV database. Medicine 2023, 102, e35410. [Google Scholar] [CrossRef]
- Wang, H.X.; Huang, X.H.; Ma, L.Q.; Yang, Z.J.; Wang, H.L.; Xu, B.; Luo, M.Q. Association between lactate-to-albumin ratio and short-time mortality in patients with acute respiratory distress syndrome. J. Clin. Anesth. 2024, 99, 111632. [Google Scholar] [CrossRef]
- Jin, P.; Bian, Y.; Cui, Q.; Liang, X.; Sun, Y.; Zheng, Q. Association between lactate/albumin ratio and 28-day all-cause mortality in critically ill patients with acute myocardial infarction. Sci. Rep. 2024, 14, 23677. [Google Scholar] [CrossRef]
- Guo, W.; Zhao, L.; Zhao, H.; Zeng, F.; Peng, C.; Guo, W.; Yan, H. The value of lactate/albumin ratio for predicting the clinical outcomes of critically ill patients with heart failure. Ann. Transl. Med. 2021, 9, 118. [Google Scholar] [CrossRef]
- Liu, J.; Min, J.; Lu, J.; Zhong, L.; Luo, H. Association between lactate/albumin ratio and prognosis in critically ill patients with acute kidney injury undergoing continuous renal replacement therapy. Ren. Fail. 2024, 46, 2374451. [Google Scholar] [CrossRef]
- Dudoignon, E.; Quennesson, T.; De Tymowski, C.; Moreno, N.; Coutrot, M.; Chaussard, M.; Guillemet, L.; Abid, S.; Fratani, A.; Ressaire, Q.; et al. Usefulness of lactate albumin ratio at admission to predict 28-day mortality in critically ill severely burned patients: A retrospective cohort study. Burns 2022, 48, 1836–1844. [Google Scholar] [CrossRef]
- Choi, S.J.; Ha, E.J.; Jhang, W.K.; Park, S.J. Association between the lactate/albumin ratio and mortality in pediatric septic shock patients with underlying chronic disease: Retrospective pilot study. Minerva Pediatr. 2021, 73, 67–72. [Google Scholar] [CrossRef]
- Lu, Y.; Guo, H.; Chen, X.; Zhang, Q. Lactate/albumin ratio and all-cause mortality in patients with acute respiratory failure. PLoS ONE 2021, 16, e0255744. [Google Scholar] [CrossRef]
- Kokkoris, S.; Gkoufa, A.; Maneta, E.; Doumas, G.; Mizi, E.; Georgakopoulou, V.E.; Sigala, I.; Dima, E.; Papachatzakis, I.; Ntaidou, T.K.; et al. Older adults with severe coronavirus disease 2019 admitted to intensive care unit: Prevalence, characteristics and risk factors for mortality. Minerva Anestesiol. 2022, 88, 803–814. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall N = 805 | Survival N = 421 | Non-Survival N = 384 | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Sex, male, n (%) | 548 (68%) | 285 (68%) | 263 (68%) | 0.8 |
| Age, years | 67 (57, 76) | 61 (52, 70) | 73 (65, 79) | <0.001 |
| Age quartiles | <0.001 | |||
| 1 | 201 (25%) | 158 (38%) | 43 (11%) | |
| 2 | 192 (24%) | 127 (30%) | 65 (17%) | |
| 3 | 210 (26%) | 86 (20%) | 124 (32%) | |
| 4 | 202 (25%) | 50 (12%) | 152 (40%) | |
| Severity scores | ||||
| Charlson comorbidity index | 3 (2, 5) | 2 (1, 4) | 4 (3, 6) | <0.001 |
| APACHE II score | 14 (11, 19) | 11 (9, 14) | 18.0 (14, 23) | <0.001 |
| SOFA score | 7 (4, 9) | 6 (2, 7) | 8 (7, 10) | <0.001 |
| Outcomes | ||||
| CRRT, n (%) | 238 (30%) | 51 (12%) | 187 (49%) | <0.001 |
| MV duration, days | 11 (4, 24) | 8 (0, 23) | 14 (7, 25) | <0.001 |
| ICU-LOS, days | 15 (8, 29) | 15 (8, 33) | 15 (8, 26) | 0.056 |
| Laboratory tests | ||||
| WBC count, ×109/L | 10 (7, 15) | 9 (7, 13) | 11 (8, 16) | <0.001 |
| Neutrophil count, ×109/L | 8.7 (5.7, 12.9) | 8.0 (5.4, 11.9) | 9.7 (6.6, 14.4) | <0.001 |
| Lymphocyte count, ×109/L | 0.76 (0.51, 1.10) | 0.80 (0.55, 1.11) | 0.73 (0.47, 1.10) | 0.015 |
| NLR | 12 (7, 20) | 10 (6, 17) | 14 (8, 23) | <0.001 |
| Hb, g/dL | 12.4 (10.8, 13.7) | 12.7 (11.4, 13.8) | 11.9 (10.1, 13.5) | <0.001 |
| PLT count, ×109/L | 241 (182, 309) | 254 (199, 321) | 226 (164, 296) | <0.001 |
| Albumin, g/dL | 3.2 (2.8, 3.6) | 3.4 (3.1, 3.6) | 3.0 (2.6, 3.4) | <0.001 |
| Sodium, mEq/L | 140 (137, 143) | 139 (136, 142) | 141 (138, 145) | <0.001 |
| Creatinine, mg/dL | 0.9 (0.7, 1.3) | 0.8 (0.7, 1.0) | 1.1 (0.8, 1.6) | <0.001 |
| AST, IU/L | 38 (25, 66) | 37 (25, 60) | 39 (25, 72) | 0.2 |
| ALT, IU/L | 32 (19, 54) | 34 (21, 54) | 28 (17, 58) | 0.020 |
| LDH, IU/L | 456 (347, 624) | 437 (312, 573) | 488 (370, 669) | <0.001 |
| hs-cTnI, ng/L | 24 (10, 77) | 15 (7, 41) | 42 (17, 123) | <0.001 |
| CRP, mg/dL | 11 (5, 18) | 10 (4, 17) | 12 (7, 20) | <0.001 |
| Fibrinogen, mg/dL | 579 (474, 701) | 575 (485, 686) | 583 (459, 708) | >0.9 |
| D-dimers, mg/L | 1.6 (0.9, 3.9) | 1.2 (0.7, 2.7) | 2.2 (1.1, 5.0) | <0.001 |
| PaO2/FiO2 ratio | 126 (88, 187) | 136 (93, 206) | 118 (83, 173) | <0.001 |
| Lactate, mmol/L | 1.70 (1.30, 2.30) | 1.50 (1.20, 1.90) | 2.00 (1.45, 2.90) | <0.001 |
| Lactate/albumin ratio | 0.53 (0.39, 0.79) | 0.46 (0.35, 0.58) | 0.64 (0.46, 1.02) | <0.001 |
| Lactate/albumin ratio quartiles | <0.001 | |||
| 1 | 206 (26%) | 150 (36%) | 56 (15%) | |
| 2 | 198 (25%) | 123 (29%) | 75 (20%) | |
| 3 | 203 (25%) | 96 (23%) | 107 (28%) | |
| 4 | 198 (25%) | 52 (12%) | 146 (38%) | |
| Treatment | ||||
| Full vaccination, n (%) | 61 (7.6%) | 26 (6.2%) | 35 (9.1%) | 0.12 |
| Remdesivir, n (%) | 391 (49%) | 221 (52%) | 170 (44%) | 0.020 |
| Dexamethasone, n (%) | 637 (79%) | 328 (78%) | 309 (80%) | 0.4 |
| Tocilizumab, n (%) | 36 (4.5%) | 28 (6.7%) | 8 (2.1%) | 0.002 |
| MV on admission, n (%) | 588 (73%) | 252 (60%) | 336 (88%) | <0.001 |
| HFNC on admission, n (%) | 158 (20%) | 116 (28%) | 42 (11%) | <0.001 |
| Shock on admission, n (%) | 304 (38%) | 172 (41%) | 132 (34%) | 0.058 |
| Comorbidities | ||||
| Hypertension, n (%) | 330 (41%) | 159 (38%) | 171 (45%) | 0.051 |
| Diabetes mellitus, n (%) | 204 (25%) | 99 (24%) | 105 (27%) | 0.2 |
| Obesity, n (%) | 104 (13%) | 63 (15%) | 41 (11%) | 0.070 |
| Cardiovascular disease, n (%) | 202 (25%) | 81 (19%) | 121 (32%) | <0.001 |
| Chronic pulmonary disease, n (%) | 106 (13%) | 40 (9.5%) | 66 (17%) | 0.001 |
| Malignancy, n (%) | 85 (11%) | 24 (5.7%) | 61 (16%) | <0.001 |
| Chronic kidney disease, n (%) | 65 (8.1%) | 15 (3.6%) | 50 (13%) | <0.001 |
| Characteristic | Quartile 1 N = 206 | Quartile 2 N = 198 | Quartile 3 N = 203 | Quartile 4 N = 198 | p-Value |
|---|---|---|---|---|---|
| Demographics | |||||
| Sex, male, n (%) | 134 (65%) | 141 (71%) | 139 (68%) | 134 (68%) | 0.6 |
| Age, years | 61 (52, 70) | 64 (54, 73) | 70 (61, 77) | 72 (63, 80) | <0.001 |
| Severity scores | |||||
| Charlson comorbidity index | 3 (1, 4) | 3 (1, 4) | 4 (2, 5) | 4 (3, 6) | <0.001 |
| APACHE II score | 11 (8, 16) | 13 (9, 16) | 14 (12, 18) | 19 (15, 24) | <0.001 |
| SOFA score | 6 (2, 7) | 6 (3, 8) | 7 (6, 8) | 8 (7, 11) | <0.001 |
| Outcomes | |||||
| ICU outcome, death, n (%) | 56 (27%) | 75 (38%) | 107 (53%) | 146 (74%) | <0.001 |
| CRRT, n (%) | 49 (24%) | 44 (22%) | 65 (32%) | 80 (40%) | <0.001 |
| MV duration, days | 9 (0, 20) | 13 (5, 26) | 14 (6, 26) | 10 (4, 23) | <0.001 |
| ICU-LOS, days | 14 (8, 25) | 17 (9, 33) | 17 (10, 31) | 12 (5, 28) | <0.001 |
| Laboratory tests | |||||
| WBC count, ×109/L | 8 (6, 11) | 9 (7, 13) | 11 (8, 15) | 14 (10, 20) | <0.001 |
| Neutrophil count, ×109/L | 6.5 (4.6, 9.5) | 8.2 (5.4, 11.9) | 9.3 (7.1, 13.7) | 12.4 (8.0, 17.4) | <0.001 |
| Lymphocyte count, ×109/L | 0.70 (0.49, 1.07) | 0.80 (0.54, 1.11) | 0.66 (0.48, 0.99) | 0.84 (0.54, 1.24) | 0.022 |
| NLR | 9 (5, 16) | 10 (6, 16) | 14 (8, 22) | 16 (8, 24) | <0.001 |
| Hb, g/dL | 12 (11, 14) | 13 (11, 14) | 12 (11, 14) | 12 (9, 13) | <0.001 |
| PLT count, ×109/L | 231 (180, 295) | 263 (203, 325) | 251 (194, 326) | 222 (159, 303) | <0.001 |
| Albumin, g/dL | 3.6 (3.3, 3.8) | 3.3 (3.1, 3.6) | 3.0 (2.8, 3.4) | 2.8 (2.4, 3.1) | <0.001 |
| Sodium, mEq/L | 139 (137, 141) | 140 (136, 142) | 140 (137, 143) | 143 (138, 147) | <0.001 |
| Creatinine, mg/dL | 0.8 (0.7, 1.1) | 0.8 (0.7, 1.0) | 0.9 (0.7, 1.3) | 1.2 (0.8, 1.9) | <0.001 |
| AST, IU/L | 41 (26, 64) | 38 (26, 65) | 36 (22, 59) | 38 (24, 95) | 0.12 |
| ALT, IU/L | 34 (21, 54) | 33 (21, 55) | 30 (19, 51) | 29 (15, 67) | 0.2 |
| LDH, IU/L | 430 (298, 550) | 455 (352, 591) | 469 (350, 634) | 478 (358, 842) | 0.001 |
| hs-cTnI, ng/L | 13 (7, 38) | 16 (8, 47) | 23 (12, 62) | 74 (27, 223) | <0.001 |
| CRP, mg/dL | 11 (4, 18) | 11 (5, 17) | 11 (5, 18) | 13 (6, 21) | 0.085 |
| Fibrinogen, mg/dL | 595 (513, 726) | 588 (506, 679) | 593 (485, 721) | 510 (375, 669) | <0.001 |
| D-dimers, mg/L | 1.1 (0.7, 2.2) | 1.3 (0.7, 2.7) | 2.2 (1.1, 4.3) | 2.5 (1.3, 10.0) | <0.001 |
| PaO2/FiO2 | 121 (90, 183) | 121 (87, 180) | 132 (86, 192) | 140 (94, 200) | 0.3 |
| Lactate, mmol/L | 1.1 (0.9, 1.3) | 1.5 (1.4, 1.6) | 1.9 (1.7, 2.2) | 3.3 (2.7, 5.4) | <0.001 |
| Shock on admission, n (%) | 74 (36%) | 92 (46%) | 94 (46%) | 44 (22%) | <0.001 |
| Treatment | |||||
| Full vaccination, n (%) | 15 (7.3%) | 12 (6.1%) | 14 (6.9%) | 20 (10%) | 0.5 |
| Remdesivir, n (%) | 100 (49%) | 109 (55%) | 102 (50%) | 80 (40%) | 0.031 |
| Dexamethasone, n (%) | 150 (73%) | 166 (84%) | 182 (90%) | 139 (70%) | <0.001 |
| Tocilizumab, n (%) | 5 (2.4%) | 11 (5.6%) | 13 (6.4%) | 7 (3.5%) | 0.2 |
| MV on admission, n (%) | 104 (50%) | 139 (70%) | 169 (83%) | 176 (89%) | <0.001 |
| HFNC on admission, n (%) | 71 (34%) | 46 (23%) | 28 (14%) | 13 (6.6%) | <0.001 |
| Comorbidities | |||||
| Hypertension, n (%) | 84 (41%) | 77 (39%) | 85 (42%) | 84 (42%) | 0.9 |
| Diabetes, n (%) | 59 (29%) | 51 (26%) | 47 (23%) | 47 (24%) | 0.6 |
| Obesity, n (%) | 37 (18%) | 27 (14%) | 29 (14%) | 11 (5.6%) | 0.002 |
| Cardiovascular disease, n (%) | 40 (19%) | 42 (21%) | 54 (27%) | 66 (33%) | 0.006 |
| Chronic pulmonary disease, n (%) | 25 (12%) | 22 (11%) | 30 (15%) | 29 (15%) | 0.6 |
| Malignancy, n (%) | 23 (11%) | 19 (9.6%) | 18 (8.9%) | 25 (13%) | 0.6 |
| Chronic kidney disease, n (%) | 16 (7.8%) | 10 (5.1%) | 15 (7.4%) | 24 (12%) | 0.073 |
| Univariate Model | * Multivariate Model | |||
|---|---|---|---|---|
| Variable | HR (95%CI) | p-Value | HR (95%CI) | p-Value |
| Lactate/albumin ratio | 1.60 (1.40–1.70) | <0.001 | 1.39 (1.27–1.52) | <0.001 |
| Lactate/Albumin Ratio Threshold | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|
| 0.43 | 80 | 44 | 56 | 71 |
| 0.57 (optimal cut-off value) * | 63 | 73 | 68 | 68 |
| 0.64 | 50 | 80 | 70 | 64 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kokkoris, S.; Gkoufa, A.; Katsaros, D.E.; Karageorgiou, S.; Kavallieratos, F.; Tsilivarakis, D.; Dimopoulou, G.; Theodorou, E.; Mizi, E.; Kotanidou, A.; et al. Lactate to Albumin Ratio and Mortality in Patients with Severe Coronavirus Disease-2019 Admitted to an Intensive Care Unit. J. Clin. Med. 2024, 13, 7106. https://doi.org/10.3390/jcm13237106
Kokkoris S, Gkoufa A, Katsaros DE, Karageorgiou S, Kavallieratos F, Tsilivarakis D, Dimopoulou G, Theodorou E, Mizi E, Kotanidou A, et al. Lactate to Albumin Ratio and Mortality in Patients with Severe Coronavirus Disease-2019 Admitted to an Intensive Care Unit. Journal of Clinical Medicine. 2024; 13(23):7106. https://doi.org/10.3390/jcm13237106
Chicago/Turabian StyleKokkoris, Stelios, Aikaterini Gkoufa, Dimitrios E. Katsaros, Stavros Karageorgiou, Fotios Kavallieratos, Dimitrios Tsilivarakis, Georgia Dimopoulou, Evangelia Theodorou, Eleftheria Mizi, Anastasia Kotanidou, and et al. 2024. "Lactate to Albumin Ratio and Mortality in Patients with Severe Coronavirus Disease-2019 Admitted to an Intensive Care Unit" Journal of Clinical Medicine 13, no. 23: 7106. https://doi.org/10.3390/jcm13237106
APA StyleKokkoris, S., Gkoufa, A., Katsaros, D. E., Karageorgiou, S., Kavallieratos, F., Tsilivarakis, D., Dimopoulou, G., Theodorou, E., Mizi, E., Kotanidou, A., Dimopoulou, I., & Routsi, C. (2024). Lactate to Albumin Ratio and Mortality in Patients with Severe Coronavirus Disease-2019 Admitted to an Intensive Care Unit. Journal of Clinical Medicine, 13(23), 7106. https://doi.org/10.3390/jcm13237106