Myopia Progression in School-Age Children During the COVID-19 Pandemic


Abstract
1. Introduction
2. Materials and Methods
2.1. Demographic Data
2.2. Refractive Power and Progression Calculations
2.3. Statistical Analyses
3. Results
3.1. Demographic Data Results
3.2. Refractive Power and Progression Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bourne, R.R.; Stevens, G.A.; White, R.A.; Smith, J.L.; Flaxman, S.R.; Price, H.; Jonas, J.B.; Keeffe, J.; Leasher, J.; Naidoo, K.; et al. Vision Loss Expert Group. Causes of vision loss worldwide, 1990–2010: A systematic analysis. Lancet Glob. Health 2013, 1, e339–e349. [Google Scholar] [CrossRef]
- Dolgin, E. The myopia boom. Nature 2015, 519, 276–278. [Google Scholar] [CrossRef] [PubMed]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.; Luensmann, D. The prevalence and impact of high myopia. Eye Contact Lens 2012, 38, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Lingham, G.; Mackey, D.A.; Lucas, R.; Yazar, S. How does spending time outdoors protect against myopia? A review. Br. J. Ophthalmol. 2020, 104, 593–599. [Google Scholar] [CrossRef]
- UNESCO. Global Monitoring of School Closures Caused by COVID-19. 2021. Available online: https://en.unesco.org/covid19/educationresponse/ (accessed on 1 March 2024).
- Wang, G.; Zhang, Y.; Zhao, J.; Zhang, J.; Jiang, F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 2020, 395, 945–947. [Google Scholar] [CrossRef]
- Pellegrini, M.; Bernabei, F.; Scorcia, V.; Giannaccare, G. May home confinement during the COVID-19 outbreak worsen the global burden of myopia? Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2069–2070. [Google Scholar] [CrossRef]
- Wang, J.; Li, Y.; Much, D.C.; Wei, N.; Qi, X.; Ding, G.; Li, X.; Li, J.; Song, L.; Zhang, Y.; et al. Progression of Myopia in School-Aged Children After COVID-19 Home Confinement. JAMA Ophthalmol. 2021, 139, 293–300. [Google Scholar] [CrossRef]
- Klaver, C.C.W.; Polling, J.R.; Enthoven, C.A. 2020 as the Year of Quarantine Myopia. JAMA Ophthalmol. 2021, 139, 300–301. [Google Scholar] [CrossRef]
- Republic of Turkey Ministry of National Education. Yuz Yuze Egitimde Ikinci Asama Basladi, Milyonlarca Ogrenci Okullariyla Bulustu. Updated 12 October 2020. Available online: https://www.meb.gov.tr/yuz-yuze-egitimde-ikinci-asama-basladi-milyonlarca-ogrenci-okullariyla-bulustu/haber/21787/tr (accessed on 1 January 2024).
- Rose, K.A.; Morgan, I.G.; Ip, J.; Kifley, A.; Huynh, S.; Smith, W.; Mitchell, P. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology 2008, 115, 1279–1285. [Google Scholar] [CrossRef]
- Tan, D.T.; Lam, D.S.; Chua, W.H.; Shu-Ping, D.F.; Crockett, R.S.; Asian Pirenzepine Study Group. One-year multicenter, double-masked, placebo-controlled, parallel safety and efficacy study of 2% pirenzepine ophthalmic gel in children with myopia. Ophthalmology 2005, 112, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Mao, J.; Luo, R.; Li, F.; Munoz, S.R.; Ellwein, L.B. The progression of refractive error in school-age children: Shunyi district, China. Am. J. Ophthalmol. 2002, 134, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Grosvenor, T.; Perrigin, D.M.; Perrigin, J.; Maslovitz, B. Houston Myopia Control Study: A randomized clinical trial. Part II. Final report by the patient care team. Am. J. Optom. Physiol. Opt. 1987, 64, 482–498. [Google Scholar] [CrossRef] [PubMed]
- Saxena, R.; Vashist, P.; Tandon, R.; Pandey, R.M.; Bhardawaj, A.; Gupta, V.; Menon, V. Incidence and progression of myopia and associated factors in urban school children in Delhi: The North India Myopia Study (NIM Study). PLoS ONE 2017, 12, e0189774. [Google Scholar] [CrossRef]
- Donovan, L.; Sankaridurg, P.; Ho, A.; Naduvilath, T.; Smith, E.L., 3rd; Holden, B.A. Myopia progression rates in urban children wearing single-vision spectacles. Optom. Vis. Sci. 2012, 89, 27–32. [Google Scholar] [CrossRef]
- Öner, V.; Bulut, A.; Oruç, Y.; Özgür, G. Influence of indoor and outdoor activities on progression of myopia during puberty. Int. Ophthalmol. 2016, 36, 121–125. [Google Scholar] [CrossRef]
- Zhang, X.J.; Zhang, Y.; Kam, K.W.; Tang, F.; Li, Y.; Ng, M.P.H.; Young, A.L.; Ip, P.; Tham, C.C.; Chen, L.J.; et al. Prevalence of Myopia in Children Before, During, and After COVID-19 Restrictions in Hong Kong. JAMA Netw. Open 2023, 6, e234080. [Google Scholar] [CrossRef]
- Wang, W.; Zhu, L.; Zheng, S.; Ji, Y.; Xiang, Y.; Lv, B.; Xiong, L.; Li, Z.; Yi, S.; Huang, H.; et al. Survey on the Progression of Myopia in Children and Adolescents in Chongqing During COVID-19 Pandemic. Front. Public Health 2021, 9, 646770. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Wei, S.; Li, S.M.; Yang, X.; Cao, K.; Hu, J.; Fan, S.; Zhang, L.; Wang, N. Progression of myopia in a natural cohort of Chinese children during COVID-19 pandemic. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 2813–2820. [Google Scholar] [CrossRef]
- Ma, M.; Xiong, S.; Zhao, S.; Zheng, Z.; Sun, T.; Li, C. COVID-19 Home Quarantine Accelerated the Progression of Myopia in Children Aged 7 to 12 Years in China. Investig. Ophthalmol. Vis. Sci. 2021, 62, 37. [Google Scholar] [CrossRef]
- Chang, P.; Zhang, B.; Lin, L.; Chen, R.; Chen, S.; Zhao, Y.; Qu, J. Comparison of Myopic Progression before, during, and after COVID-19 Lockdown. Ophthalmology 2021, 128, 1655–1657. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Ma, Y.; Yuan, J.; Zhang, Y.; Wang, H.; Zhang, G.; Tu, C.; Lu, X.; Li, J.; Xiong, Y.; et al. COVID-19 Quarantine Reveals That Behavioral Changes Have an Effect on Myopia Progression. Ophthalmology 2021, 128, 1652–1654. [Google Scholar] [CrossRef] [PubMed]
- Aslan, F.; Sahinoglu-Keskek, N. The effect of home education on myopia progression in children during the COVID-19 pandemic. Eye 2022, 36, 1427–1432. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Li, B.; Sun, Y.; Chen, Q.; Dang, J. Adolescent Vision Health During the Outbreak of COVID-19: Association Between Digital Screen Use and Myopia Progression. Front. Pediatr. 2021, 9, 662984. [Google Scholar] [CrossRef]
- Wong, C.W.; Tsai, A.; Jonas, J.B.; Ohno-Matsui, K.; Chen, J.; Ang, M.; Ting, D.S.W. Digital Screen Time During the COVID-19 Pandemic: Risk for a Further Myopia Boom? Am. J. Ophthalmol. 2021, 223, 333–337. [Google Scholar] [CrossRef]
- Ozturk Eyimaya, A.; Yalçin Irmak, A. Relationship Between Parenting Practices and Children’s Screen Time During the COVID-19 Pandemic in Turkey. J. Pediatr. Nurs. 2021, 56, 24–29. [Google Scholar] [CrossRef]

{kind=link}
| Total (n = 825) | Group A (n = 144) | Group B (n = 314) | Group C (n = 367) | p | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean age (years) (SD) [range] | 13.8 (3.17) [7,8,9,10,11,12,13,14,15,16,17,18] | 8.60 (1.33) [7,8,9,10] | 12.9 (1.11) [11,12,13,14] | 16.6 (1.20) [15,16,17,18] | <0.001 a | ||||
| female (n) [%] | 541 [5.6] | 89 [61.8] | 208 [66.2] | 235 [64.0] | 0.113 b | ||||
| n | mean (D, SD) | N | mean (D, SD) | n | mean (D, SD) | N | mean (D, SD) | ||
| SE_2018 | 499 | −1.77 (1.42) | 84 | −1.49 (1.36) | 178 | −1.84 (1.52) | 237 | −1.81 (1.36) | 0.135 c |
| SE_2019 | 681 | −1.93 (1.50) | 114 | −1.50 (1.29) | 268 | −1.99 (1.56) | 299 | −2.05 (1.49 | <0.001 c |
| SE_2020 | 445 | −2,49 (1.83) | 106 | −1.95 (1.42) | 148 | −2.70 (2.00) | 191 | −2.64 (1.83) | <0.001 c |
| SE_2021 | 741 | −2.77 (1.76) | 132 | −2.47 (1.65) | 292 | −2.81 (1.80) | 317 | −2.86 (1.76) | 0.074 c |
| p | <0.001 d | <0.001 d | <0.001 d | <0.001 d | |||||
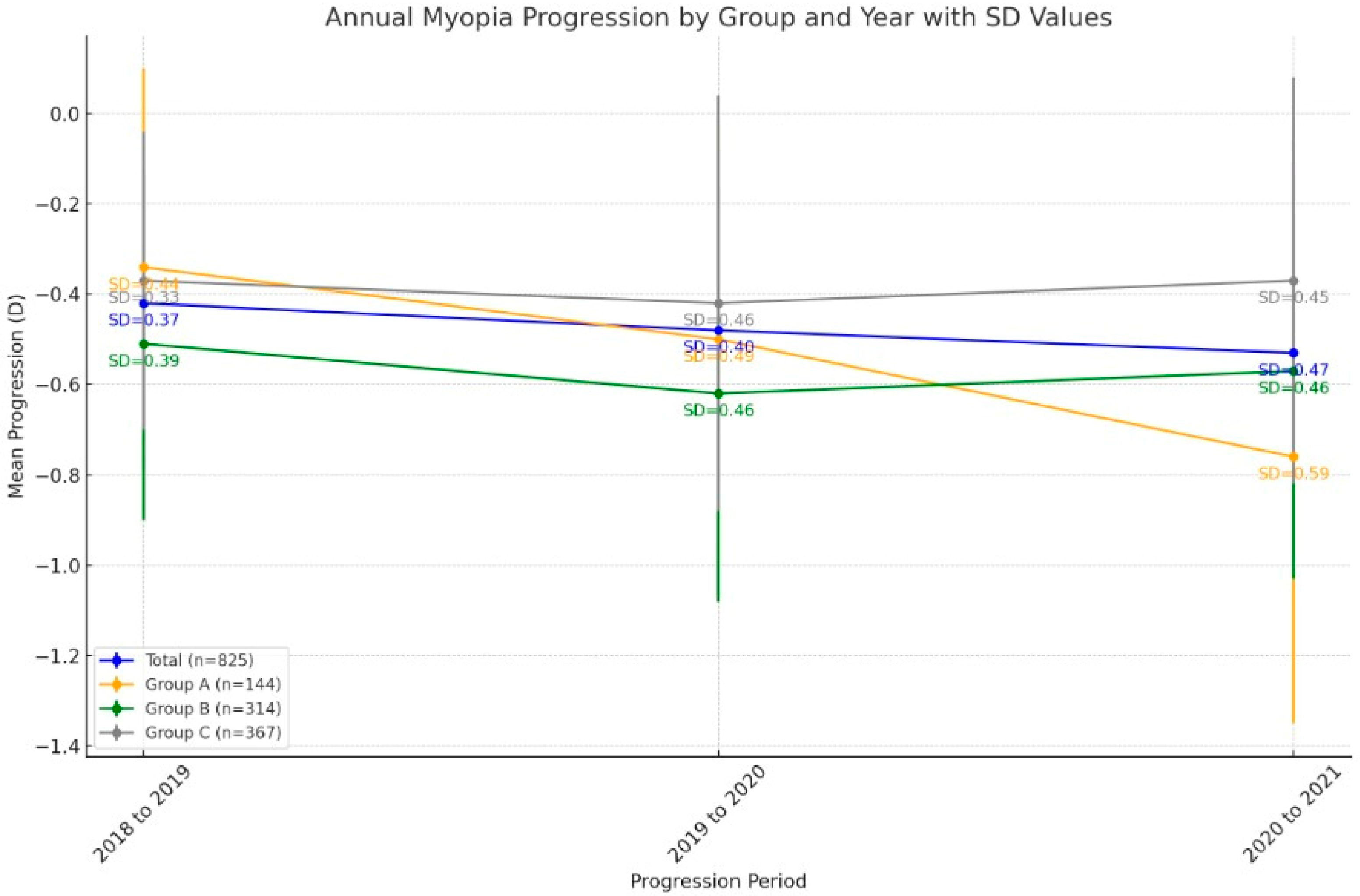
| Mean (D, SD) | na | nb | nc | Pa | Pb | Pc | ||
|---|---|---|---|---|---|---|---|---|
| Total (n = 825) | progression from 2018 to 2019 | −0.42 (0.37) | 237 | 289 | 205 | 0.065 | 0.861 | <0.001 |
| progression from 2019 to 2020 | −0.48 (0.40) | |||||||
| progression from 2020 to 2021 | −0.53 (0.47) | |||||||
| Group A (n = 144) | progression from 2018 to 2019 | −0.34 (0.44) | 60 | 74 | 60 | 0.001 | 0.018 | <0.001 |
| progression from 2019 to 2020 | −0.50 (0.49) | |||||||
| progression from 2020 to 2021 | −0.76 (0.59) | |||||||
| Group B (n = 314) | progression from 2018 to 2019 | −0.51 (0.39) | 73 | 104 | 66 | 0.249 | 0.850 | 0.502 |
| progression from 2019 to 2020 | −0.62 (0.46) | |||||||
| progression from 2020 to 2021 | −0.57 (0.46) | |||||||
| Group C (n = 367) | progression from 2018 to 2019 | −0.37 (0.33) | 103 | 111 | 79 | 0.400 | 0.059 | 0.499 |
| progression from 2019 to 2020 | −0.42 (0.46) | |||||||
| progression from 2020 to 2021 | −0.37 (0.45) |
| R | B | 95% CI | p | |||
|---|---|---|---|---|---|---|
| Progression from 2018 to 2019 | Age | 0.143 | 0.009 | −0.003 | 0.021 | 0.145 |
| Gender | −0.027 | −0.186 | 0.095 | 0.198 | ||
| Progression from 2019 to 2020 | Age | 0.033 | 0.000 | −0.015 | 0.013 | 0.897 |
| Gender | 0.032 | −0.070 | 0.135 | 0.536 | ||
| Progression from 2020 to 2021 | Age | 0.318 | 0.049 | 0.034 | 0.065 | <0.001 |
| Gender | −0.026 | −0.135 | 0.082 | 0.628 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gökgöz Özışık, G.; Yilmaz, H. Myopia Progression in School-Age Children During the COVID-19 Pandemic. J. Clin. Med. 2024, 13, 6849. https://doi.org/10.3390/jcm13226849
Gökgöz Özışık G, Yilmaz H. Myopia Progression in School-Age Children During the COVID-19 Pandemic. Journal of Clinical Medicine. 2024; 13(22):6849. https://doi.org/10.3390/jcm13226849
Chicago/Turabian StyleGökgöz Özışık, Gülce, and Hayati Yilmaz. 2024. "Myopia Progression in School-Age Children During the COVID-19 Pandemic" Journal of Clinical Medicine 13, no. 22: 6849. https://doi.org/10.3390/jcm13226849
APA StyleGökgöz Özışık, G., & Yilmaz, H. (2024). Myopia Progression in School-Age Children During the COVID-19 Pandemic. Journal of Clinical Medicine, 13(22), 6849. https://doi.org/10.3390/jcm13226849