
Risk Factors of Reoperation in Patients with Intestinal Behçet’s Disease Treated by Initial Bowel Resection

 , , , , , , , ,
, , , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
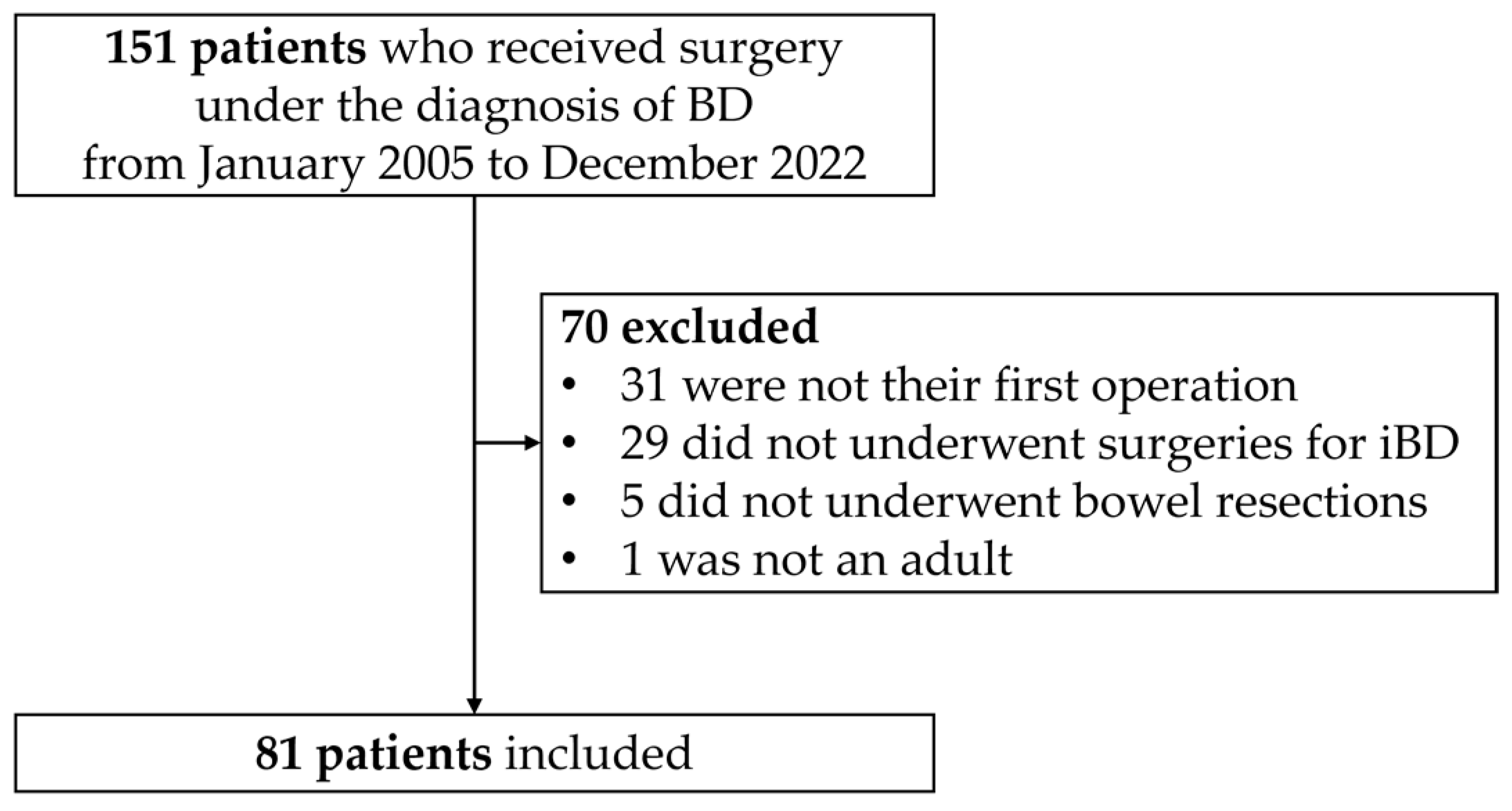
2.1. Study Population
2.2. Definition of Variables
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Perioperative Outcomes
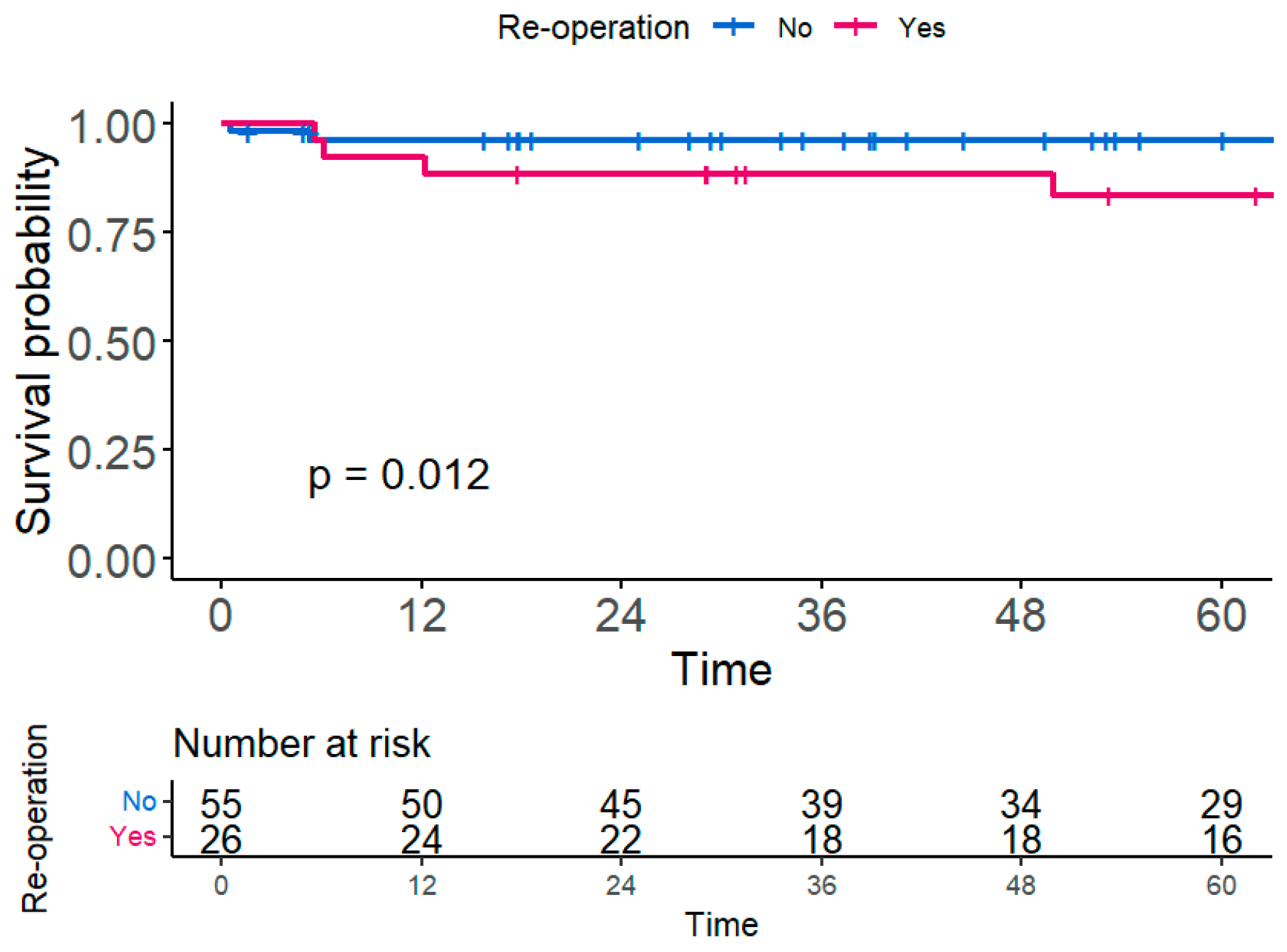
3.3. Reoperation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nguyen, A.; Upadhyay, S.; Javaid, M.A.; Qureshi, A.M.; Haseeb, S.; Javed, N.; Cormier, C.; Farooq, A.; Sheikh, A.B. Behcet’s Disease: An In-Depth Review about Pathogenesis, Gastrointestinal Manifestations, and Management. Inflamm. Intestig. Dis. 2021, 6, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Vaiopoulos, A.G.; Sfikakis, P.P.; Kanakis, M.A.; Vaiopoulos, G.; Kaklamanis, P.G. Gastrointestinal manifestations of Behçet’s disease: Advances in evaluation and management. Clin. Exp. Rheumatol. 2014, 32, S140–S148. [Google Scholar] [PubMed]
- Tong, B.; Liu, X.; Xiao, J.; Su, G. Immunopathogenesis of Behcet’s Disease. Front. Immunol. 2019, 10, 665. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Yao, X. A Contemporary Review of Behcet’s Syndrome. Clin. Rev. Allergy Immunol. 2021, 61, 363–376. [Google Scholar] [CrossRef]
- Skef, W.; Hamilton, M.J.; Arayssi, T. Gastrointestinal Behcet’s disease: A review. World J. Gastroenterol. 2015, 21, 3801–3812. [Google Scholar] [CrossRef]
- Joo, Y.Y.; Lee, B.I.; Kim, S.J.; Lee, H.H.; Kim, J.S.; Park, J.M.; Cho, Y.S.; Lee, K.M.; Kim, S.W.; Choi, H.; et al. Clinical Course of Patients with Intestinal Behçet’s Disease According to Consensus-Based Diagnostic Categories. Gut Liver 2022, 16, 746–753. [Google Scholar] [CrossRef]
- Jung, Y.S.; Yoon, J.Y.; Lee, J.H.; Jeon, S.M.; Hong, S.P.; Kim, T.I.; Kim, W.H.; Cheon, J.H. Prognostic factors and long-term clinical outcomes for surgical patients with intestinal Behcet’s disease. Inflamm. Bowel Dis. 2011, 17, 1594–1602. [Google Scholar] [CrossRef]
- Manuelyan, Z.; Butt, E.; Parupudi, S. Gastrointestinal Behcet’s disease: Manifestations, diagnosis, and management. Dis. Mon. 2024, 70, 101674. [Google Scholar] [CrossRef]
- Liu, Y.; Gao, F.; Yang, D.Q.; Jiao, Y. Intestinal Behcet’s disease: A review of clinical diagnosis and treatment. World J. Gastrointest. Surg. 2024, 16, 1493–1500. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Mathew, G.; Agha, R.; Albrecht, J.; Goel, P.; Mukherjee, I.; Pai, P.; D’Cruz, A.K.; Nixon, I.J.; Roberto, K.; Enam, S.A.; et al. STROCSS 2021: Strengthening the reporting of cohort, cross-sectional and case-control studies in surgery. Int. J. Surg. 2021, 96, 106165. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.J.; Kim, C.W.; Cho, M.S.; Jang, H.A.; Baik, S.H.; Hur, H.; Min, B.S.; Kim, N.K. Surgical Treatment and Outcomes in Patients with Intestinal Behcet Disease: Long-Term Experience of a Single Large-Volume Center. Dis. Colon Rectum 2015, 58, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.E.; Cheon, J.H.; Park, J.; Lee, J.H.; Lee, H.J.; Park, S.J.; Kim, T.I.; Kim, W.H. The outcomes and risk factors of early reoperation after initial intestinal resective surgery in patients with intestinal Behcet’s disease. Int. J. Color. Dis. 2017, 32, 591–594. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.A.; Park, J.W.; Park, Y.; Park, S.J.; Kim, T.I.; Kim, W.H.; Cho, M.S.; Cheon, J.H. C-reactive protein is associated with postoperative outcomes in patients with intestinal Behcet’s disease. BMC Gastroenterol. 2021, 21, 362. [Google Scholar] [CrossRef] [PubMed]
- Esatoglu, S.N.; Hatemi, G.; Salihoglu, A.; Hatemi, I.; Soysal, T.; Celik, A.F. A reappraisal of the association between Behçet’s disease, myelodysplastic syndrome and the presence of trisomy 8: A systematic literature review. Clin. Exp. Rheumatol. 2015, 33, S145–S151. [Google Scholar]
- Handa, T.; Nakatsue, T.; Baba, M.; Takada, T.; Nakata, K.; Ishii, H. Clinical features of three cases with pulmonary alveolar proteinosis secondary to myelodysplastic syndrome developed during the course of Behçet’s disease. Respir. Investig. 2014, 52, 75–79. [Google Scholar] [CrossRef]
- Kanamitsu, K.; Shimada, A.; Nishiuchi, R.; Shigemura, T.; Nakazawa, Y.; Koike, K.; Kodama, Y.; Shinkoda, Y.; Kawano, Y.; Yasui, K.; et al. Pediatric intestinal Behcet disease complicated by myeloid malignancies. Int. J. Hematol. 2017, 105, 377–382. [Google Scholar] [CrossRef]
- Park, J.B.; Han, S.J.; Lee, S.B.; Kim, D.H.; Cheon, J.H.; Hwang, S.W.; Ye, B.D.; Yang, S.K.; Park, S.J.; Park, S.H.; et al. Optimal Treatment Approaches to Intestinal Behcet’s Disease Complicated by Myelodysplastic Syndrome: The KASID and KSBD Multicenter Study. Yonsei Med. J. 2024, 65, 265–275. [Google Scholar] [CrossRef]
- Kubo, T.; Ono, S.; Ueno, H.; Shinto, E.; Yamamoto, J.; Hase, K. Elevated preoperative C-reactive protein levels are a risk factor for the development of postoperative infectious complications following elective colorectal surgery. Langenbeck’s Arch. Surg. 2013, 398, 965–971. [Google Scholar] [CrossRef]
- Kühn, F.; Nixdorf, M.; Schwandner, F.; Klar, E. Risk Factors for Early Surgery and Surgical Complications in Crohn’s Disease. Zentralbl. Chir. 2018, 143, 596–602. [Google Scholar]
- Kono, T.; Fichera, A.; Maeda, K.; Sakai, Y.; Ohge, H.; Krane, M.; Katsuno, H.; Fujiya, M. Kono-S Anastomosis for Surgical Prophylaxis of Anastomotic Recurrence in Crohn’s Disease: An International Multicenter Study. J. Gastrointest. Surg. 2016, 20, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Horisberger, K.; Birrer, D.L.; Rickenbacher, A.; Turina, M. Experiences with the Kono-S anastomosis in Crohn’s disease of the terminal ileum-a cohort study. Langenbeck’s Arch. Surg. 2021, 406, 1173–1180. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Overall (n = 81) | Reoperation Group (n = 26) | Non-Reoperation Group (n = 55) | p-Value | |
|---|---|---|---|---|
| Sex | 0.621 | |||
| Male | 28 (34.6%) | 8 (30.8%) | 20 (36.4%) | |
| Female | 53 (65.4%) | 18 (69.2%) | 35 (63.6%) | |
| Age at diagnosis of BD (years) | 39.4 ± 13.0 | 38.8 ± 12.5 | 39.7 ± 13.4 | 0.755 |
| Age at diagnosis of iBD (years) | 43.7 ± 12.2 | 43.4 ± 13.4 | 43.8 ± 11.7 | 0.877 |
| Age at initial surgery (years) | 46.9 ± 12.3 | 45.6 ± 13.2 | 47.5 ± 12.0 | 0.537 |
| Time to initial surgery from diagnosis (month) | 16.8 (3.4, 51.7) | 15.1 (3.3, 3.8) | 16.8 (3.3, 64.7) | 0.479 |
| BMI at initial surgery (kg/m2) | 20.9 ± 3.8 | 19.6 ± 4.2 | 21.5 ± 3.6 | 0.039 |
| Hematological disorder | 17 (21.0%) | 12 (46.2%) | 5 (9.1%) | <0.001 |
| Operative history | 14 (17.3%) | 5 (19.2%) | 16 (29.1%) | 0.344 |
| Drugs used before initial surgery | 0.627 | |||
| Multiple | 56 (69.1%) | 17 (65.4%) | 39 (70.9%) | |
| Single | 19 (23.5%) | 6 (23.1%) | 13 (23.6%) | |
| None | 6 (7.4%) | 3 (11.5%) | 3 (5.5%) | |
| Indication for initial surgery | 0.420 | |||
| Medical intractability | 53 (65.4%) | 18 (69.2%) | 35 (63.6%) | |
| Abscess/fistula | 3 (3.7%) | 1 (3.8%) | 2 (3.6%) | |
| Stenosis | 4 (4.9%) | 1 (3.8%) | 3 (5.5%) | |
| Bleeding | 6 (7.4%) | 0 (0%) | 6 (10.9%) | |
| Perforation | 13 (16.0%) | 6 (23.1%) | 7 (12.7%) | |
| Other | 2 (2.5%) | 0 (0%) | 2 (3.6%) | |
| ASA score | 0.499 | |||
| 1–2 | 57 (70.4%) | 17 (65.4%) | 40 (72.7%) | |
| 3–4 | 24 (29.6%) | 9 (34.6%) | 15 (27.3%) | |
| CRP before initial surgery(mg/dL) | 54.4 (20, 109) | 84.7 (39.1, 168.8) | 46.3 (14.6, 80.5) | 0.004 |
| Albumin before initial surgery (g/dL) | 3.4 ± 0.6 | 3.2 ± 0.6 | 3.5 ± 0.7 | 0.066 |
| Hb before initial surgery (g/dL) | 10.1 ± 1.5 | 9.6 ± 1.4 | 10.3 ± 1.6 | 0.052 |
| Overall (n = 81) | Reoperation Group (n = 26) | Non-Reoperation Group (n = 55) | p-Value | |
|---|---|---|---|---|
| Emergency operation | 19 (23.5%) | 8 (30.8%) | 11 (20.0%) | 0.286 |
| Open conversion | 2 (2.5%) | 0 (0%) | 2 (3.6%) | >0.999 |
| Operation name | 0.041 | |||
| Ileocecectomy | 51 (63.0%) | 15 (57.7%) | 36 (65.5%) | |
| Right hemicolectomy | 22 (27.2%) | 6 (23.1%) | 16 (29.1%) | |
| Segmental resection of small bowel | 6 (7.4%) | 5 (19.2%) | 1 (1.8%) | |
| Total colectomy | 2 (2.5%) | 0 (0%) | 2 (3.6%) | |
| Operative method | 0.383 | |||
| Open | 20 (24.7%) | 8 (30.8%) | 12 (21.8%) | |
| Laparoscopic | 61 (75.3%) | 18 (69.2%) | 43 (78.2%) | |
| Operation time (min) | 142 (111, 192) | 152 (122, 193) | 135 (107, 192) | 0.227 |
| Intraoperative blood loss (mL) | 20 (0.100) | 35 (0, 125) | 10 (0, 100) | 0.319 |
| Anastomosis type | 0.767 | |||
| End-to-end | 12 (14.8%) | 5 (19.2%) | 7 (12.7%) | |
| End-to-side | 55 (67.9%) | 17 (65.4%) | 38 (69.1%) | |
| Side-to-side | 14 (17.3%) | 4 (15.4%) | 10 (18.2%) | |
| Anastomosis method | 0.953 | |||
| Hand-sewn | 37 (45.7%) | 12 (46.2%) | 25 (45.5%) | |
| Stapler-assisted | 44 (54.3%) | 14 (53.8%) | 30 (54.5%) | |
| Multiple anastomosis | 2 (2.5%) | 1 (3.8%) | 1 (1.8%) | 0.542 |
| Stoma formation | 3 (3.7%) | 2 (7.7%) | 1 (1.8%) | 0.240 |
| Postoperative antibiotics use (days) | 8 (5, 16) | 12 (7, 26) | 7 (5, 13) | 0.012 |
| Postoperative hospital stay (days) | 10 (7, 22) | 18 (8, 33) | 9 (7, 16) | 0.011 |
| Postoperative complication | ||||
| Overall | 42 (51.9%) | 18 (69.2%) | 24 (43.6%) | 0.031 |
| Intra-abdominal infection | 14 (17.3%) | 7 (26.9%) | 7 (12.7%) | 0.115 |
| Anastomosis leak | 2 (2.5%) | 2 (7.7%) | 0 (0%) | 0.037 |
| Bleeding | 3 (3.7%) | 0 (0%) | 3 (5.5%) | 0.547 |
| Ileus | 7 (8.6%) | 3 (11.5%) | 4 (7.3%) | 0.675 |
| Colitis | 11 (13.6%) | 6 (23.1%) | 5 (9.1%) | 0.086 |
| Wound infection | 13 (16.0%) | 10 (38.5%) | 3 (5.5%) | <0.001 |
| Other | 15 (18.5%) | 7 (26.9%) | 10 (18.2%) | 0.367 |
| Grade | 0.036 | |||
| I | 7 (8.6%) | 3 (11.5%) | 4 (7.3%) | |
| II | 20 (24.7%) | 10 (38.5%) | 10 (18.2%) | |
| IIIa | 4 (4.9%) | 1 (3.8%) | 3 (5.5%) | |
| IIIb | 5 (6.2%) | 3 (11.5%) | 2 (3.6%) | |
| IV | 1 (1.2%) | 1 (3.8%) | 0 (0%) | |
| V | 1 (1.2%) | 0 (0%) | 1 (1.8%) | |
| Pathology of specimen | 0.503 | |||
| Inflammation | 3 (3.7%) | 1 (3.8%) | 0 (3.6%) | |
| Ulcer | 49 (60.5%) | 14 (53.8%) | 35 (63.6%) | |
| Necrosis | 1 (1.2%) | 1 (3.8%) | 0 (0%) | |
| Perforation | 28 (34.6%) | 10 (38.5%) | 18 (32.7%) | |
| Resection length (cm) | 29.5 ± 17.2 | 26.0 ± 13.8 | 31.2 ± 18.4 | 0.208 |
| Maximum luminal diameter (cm) | 7.4 ± 2.4 | 7.5 ± 2.4 | 7.3 ± 2.4 | 0.852 |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Sex (Male) | 1.37 (0.59–3.16) | 0.459 | ||
| Age at initial surgery (years) | 1 (0.97–1.03) | 0.976 | ||
| BMI at initial surgery (kg/m2) | 0.87 (0.78–0.97) | 0.016 | 0.071 | |
| ASA score (3–4) | 1.83 (0.81–4.14) | 0.144 | ||
| Hematological disorder | 6.21 (2.83–13.63) | <0.001 | 9.13 (3.79–22.02) | <0.001 |
| Operative history | 0.64 (0.24–1.71) | 0.376 | ||
| Drugs used before initial surgery (None) | 0.262 | |||
| Single | 0.37 (0.09–1.52) | 0.168 | ||
| Multiple | 0.36 (0.1–1.24) | 0.105 | ||
| Indication for initial surgery (Medical intractability) | 0.987 | |||
| Abscess/fistula | 0.89 (0.12–6.67) | 0.909 | ||
| Stenosis | 0.54 (0.07–4.02) | 0.543 | ||
| Bleeding | 0 (0–0) | 0.978 | ||
| Perforation | 1.22 (0.48–3.07) | 0.680 | ||
| Other | 0 (0–0) | 0.989 | ||
| CRP before initial surgery (mg/L) | 1.01 (1–1.01) | <0.001 | 1.01 (1.01–1.02) | <0.001 |
| Albumin before initial surgery (g/dL) | 0.48 (0.26–0.91) | 0.023 | 0.077 | |
| Hb before initial surgery (g/dL) | 0.73 (0.56–0.94) | 0.016 | 0.557 | |
| Indication for initial surgery (Medical intractability) | 0.289 | 0.441 | ||
| Perforations | 1.16 (0.48–2.78) | 0.136 | 0.29 (0.03–2.9) | 0.293 |
| Others | 0.22 (0.03–1.62) | 0.745 | 0.21 (0.01–5.08) | 0.337 |
| Emergency operation | 1.37 (0.59–3.17) | 0.461 | ||
| Open conversion | 0.05 (0–954.6) | 0.547 | ||
| Operation name (Ileocecectomy) | 0.153 | |||
| Right hemicolectomy | 0.94 (0.36–2.43) | 0.901 | ||
| Segmental resection of small bowel | 3.08 (1.12–8.49) | 0.030 | ||
| Total colectomy | 0 (0–0) | 0.986 | ||
| Operative method (Open) | 1.06 (0.46–2.46) | 0.884 | ||
| Operation time (min) | 1.00 (0.99–1.01) | 0.904 | ||
| Intraoperative blood loss (mL) | 1.00 (1.00–1.00) | 0.523 | ||
| Anastomosis type (End-to-end) | 0.893 | |||
| End-to-side | 0.85 (0.31–2.31) | 0.744 | ||
| Side-to-side | 0.73 (0.19–2.72) | 0.636 | ||
| Anastomosis method (Stapler-assisted) | 1.03 (0.48–2.23) | 0.944 | ||
| Multiple anastomosis | 1.16 (0.16–8.61) | 0.883 | ||
| Stoma formation | 3.26 (0.74–14.28) | 0.117 | ||
| Postoperative antibiotics use (days) | 1.02 (1.01–1.03) | <0.001 | 0.090 | |
| Postoperative hospital stay (days) | 1.02 (1.01–1.03) | <0.001 | 0.106 | |
| Postoperative complication | 2.46 (1.07–5.67) | 0.034 | 0.229 | |
| Pathology of specimen (inflammation) | 0.018 | 0.848 | ||
| Ulcer | 0.46 (0.06–3.61) | 0.460 | 0.665 | |
| Perforation | 0.50 (0.06–4.08) | 0.521 | 0.847 | |
| Necrosis | 39.1 (1.38–1113.10) | 0.032 | 0.391 | |
| Resection length (cm) | 0.99 (0.96–1.01) | 0.310 | 0.96 (0.93–0.99) | 0.011 |
| Maximum luminal diameter (≥5 cm) | 0.99 (0.85–1.16) | 0.904 | ||
| First Author/s, Year | Inclusion Period (Year) | Inclusion Criteria | Patients (N) | Outcomes | Risk Factors |
|---|---|---|---|---|---|
| Jung et al., 2011 [7] | 1986–2010 | All surgical patients | 72 | Reoperation | Volcano-shaped ulcer, higher preoperative CRP, postoperative steroids use |
| Baek et al., 2015 [12] | 1995–2012 | All surgical patients | 91 | Reoperation | Postoperative steroid use, postoperative complications, lower BMI |
| Park et al., 2017 [13] | 2006–2016 | Patients with repeated surgery | 41 | Early reoperation (<6 months) | Initial emergency operation, higher ESR |
| Kang et al., 2021 [14] | 2005–2018 | All surgical patients | 90 | Reoperation | Higher postoperative CRP, perioperative steroids use |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.J.; Park, E.J.; Bae, H.W.; Lee, Y.J.; Park, M.Y.; Yang, S.Y.; Han, Y.D.; Cho, M.S.; Hur, H.; Carmichael, J.C.; et al. Risk Factors of Reoperation in Patients with Intestinal Behçet’s Disease Treated by Initial Bowel Resection. J. Clin. Med. 2024, 13, 6771. https://doi.org/10.3390/jcm13226771
Kim SJ, Park EJ, Bae HW, Lee YJ, Park MY, Yang SY, Han YD, Cho MS, Hur H, Carmichael JC, et al. Risk Factors of Reoperation in Patients with Intestinal Behçet’s Disease Treated by Initial Bowel Resection. Journal of Clinical Medicine. 2024; 13(22):6771. https://doi.org/10.3390/jcm13226771
Chicago/Turabian StyleKim, Sun Jung, Eun Ji Park, Hyeon Woo Bae, Yong Joon Lee, Min Young Park, Seung Yoon Yang, Yoon Dae Han, Min Soo Cho, Hyuk Hur, Joseph C. Carmichael, and et al. 2024. "Risk Factors of Reoperation in Patients with Intestinal Behçet’s Disease Treated by Initial Bowel Resection" Journal of Clinical Medicine 13, no. 22: 6771. https://doi.org/10.3390/jcm13226771
APA StyleKim, S. J., Park, E. J., Bae, H. W., Lee, Y. J., Park, M. Y., Yang, S. Y., Han, Y. D., Cho, M. S., Hur, H., Carmichael, J. C., Min, B. S., & Lee, K. Y. (2024). Risk Factors of Reoperation in Patients with Intestinal Behçet’s Disease Treated by Initial Bowel Resection. Journal of Clinical Medicine, 13(22), 6771. https://doi.org/10.3390/jcm13226771