
Ultrasound-Guided Intranodal Lipiodol Lymphangiography for the Assessment and Treatment of Chylous Leaks: A Retrospective Case Series from a Single Center in Switzerland and a Systematic Review of the Literature

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Systematic Review of the Literature
2.1.1. Selection Criteria
2.1.2. Data Extraction
2.1.3. Bias/Quality Assessment
2.1.4. Statistical Analysis
2.2. Retrospective Case Series
3. Results
3.1. Systematic Review of the Literature
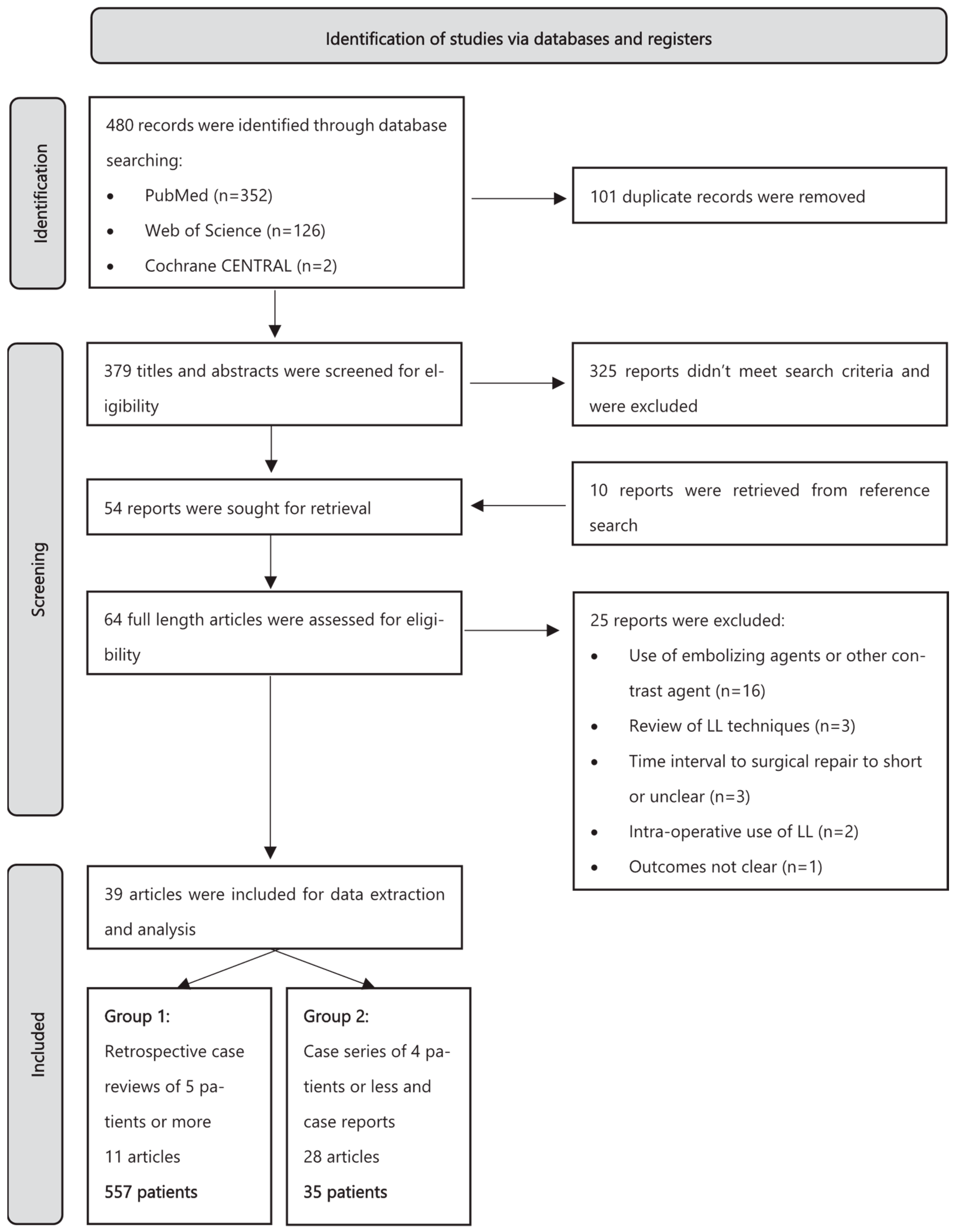
3.1.1. Study Selection
3.1.2. Bias/Quality Assessment
3.1.3. Extracted Data
Diagnosis, Surgical Approach, and Initial Leak Management
Technical Aspects of LL
Technical and Clinical Success Rates of LL
Qualitative Analysis
3.2. Case Series
3.2.1. Pre-Procedure Assessment
3.2.2. LL Interventional Technique
Ultrasound-Guided Intranodal Lymphangiography
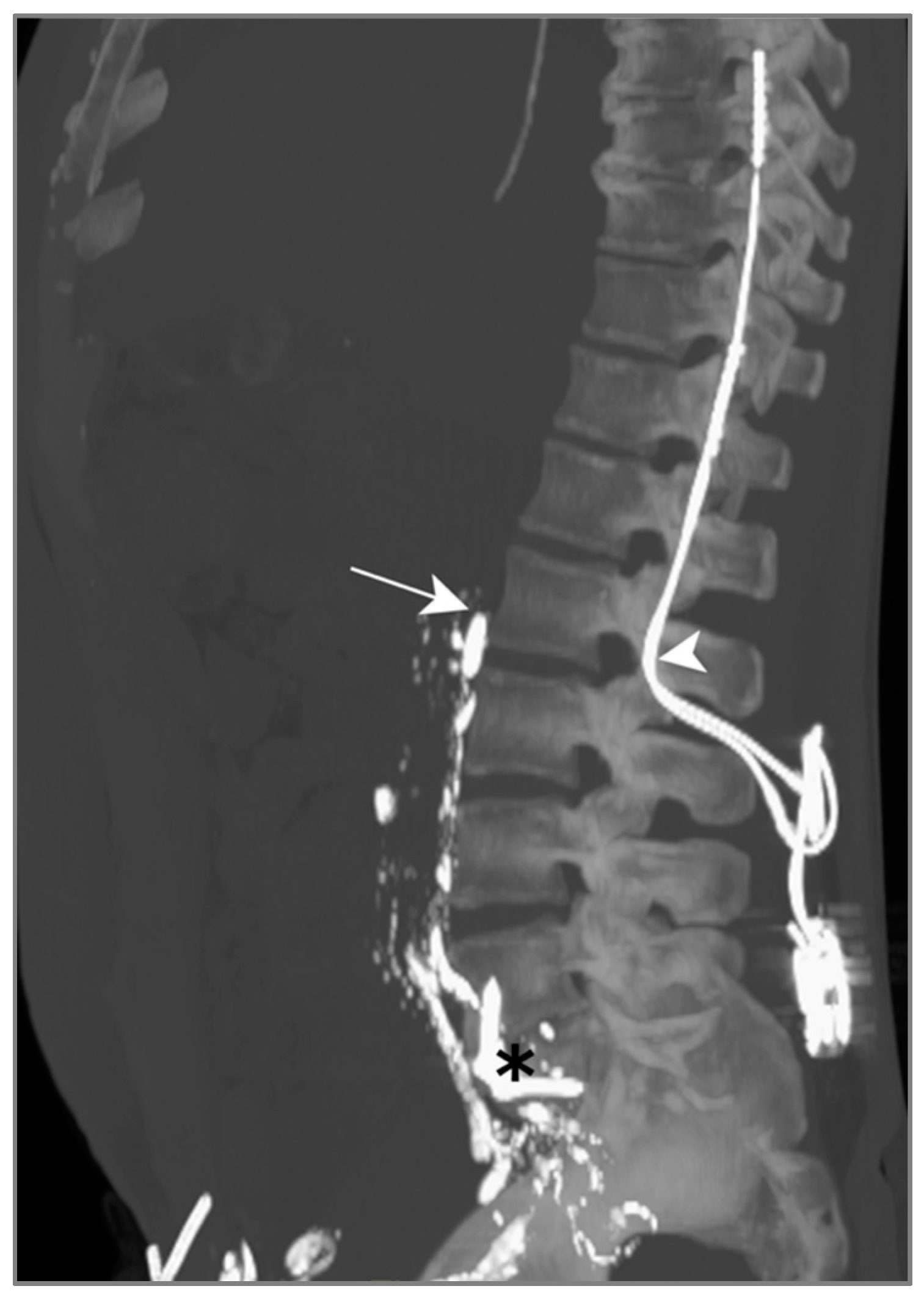
Post-Lymphangiography Unenhanced CT
Clinical and Technical Success of LL
3.2.3. Post-LL Follow-Up
3.2.4. Case Presentation
Patient A—Bilateral Chylothorax Post-Transhiatal Esophagectomy
Patient B—Right Chylothorax Post Distal Esophagectomy
Patient C—Right Chylothorax After Open Right Lower Lobectomy
Patient D—Right Chylothorax Post Thoracoscopic Lobectomy
Patient E—Chylous Ascites After Pancreaticoduodenectomy
3.2.5. Technical and Clinical Success—Case Series
Technical Success:
Clinical Success:
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lv, S.; Wang, Q.; Zhao, W.; Han, L.; Wang, Q.; Batchu, N.; Ulain, Q.; Zou, J.; Sun, C.; Du, J.; et al. A Review of the Postoperative Lymphatic Leakage. 2017. Available online: https://www.impactjournals.com/oncotarget (accessed on 1 September 2024).
- McGrath, E.E.; Blades, Z.; Anderson, P.B. Chylothorax: Aetiology, diagnosis and therapeutic options. Respir. Med. 2010, 104, 1–8. [Google Scholar] [CrossRef]
- Nair, S.K.; Petko, M.; Hayward, M.P. Aetiology and management of chylothorax in adults. Eur. J. Cardio-Thoracic Surg. 2007, 32, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Al-Busafi, S.A.; Ghali, P.; Deschênes, M.; Wong, P. Chylous Ascites: Evaluation and Management. ISRN Hepatol. 2014, 2014, 240473. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.A.; Park, H.; Jeong, S.G.; Lee, C.; Lee, J.M.; Park, C.T. Octreotide therapy for the management of refractory chylous ascites after a staging operation for endometrial adenocarcinoma. J. Obstet. Gynaecol. Res. 2014, 40, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Pieper, C.C.; Hur, S.; Sommer, C.-M.; Nadolski, G.; Maleux, G.; Kim, J.; Itkin, M. Back to the Future: Lipiodol in Lymphography—From Diagnostics to Theranostics; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2019. [Google Scholar] [CrossRef]
- Lee, E.W.; Shin, J.H.; Ko, H.K.; Park, J.; Kim, S.H.; Sung, K.B. Lymphangiography to treat postoperative lymphatic leakage: A technical review. Korean J. Radiol. 2014, 15, 724–732. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097-269. [Google Scholar] [CrossRef]
- Goossen, K.; Tenckhoff, S.; Probst, P.; Grummich, K.; Mihaljevic, A.L.; Büchler, M.W.; Diener, M.K. Optimal literature search for systematic reviews in surgery. Langenbecks Arch. Surg. 2018, 403, 119–129. [Google Scholar] [CrossRef]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; Cochrane: Oxford, UK, 2022; Available online: https://www.training.cochrane.org/handbook (accessed on 1 September 2024).
- Pan, F.; Richter, G.M.; Do, T.D.; Kauczor, H.-U.; Klotz, R.; Hackert, T.; Loos, M.; Sommer, C.M. Treatment of Postoperative Lymphatic Leakage Applying Transpedal Lymphangiography—Experience in 355 Consecutive Patients. RoFo Fortschritte Auf Dem Geb. Der Rontgenstrahlen Und Der Bildgeb. Verfahr. 2022, 194, 634–643. [Google Scholar] [CrossRef]
- Gruber-Rouh, T.; Naguib, N.N.; Lehnert, T.; Harth, M.; Thalhammer, A.; Beeres, M.; Tsaur, I.; Hammersting, R.; Wichmann, J.L.; Vogl, T.J.; et al. Direct lymphangiography as treatment option of lymphatic leakage: Indications, outcomes and role in patient’s management. Eur. J. Radiol. 2014, 83, 2167–2171. [Google Scholar] [CrossRef]
- Alejandre-Lafont, E.; Krompiec, C.; Rau, W.S.; Krombach, G.A. Effectiveness of therapeutic lymphography on lymphatic leakage. Acta Radiol. 2011, 52, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Kos, S.; Haueisen, H.; Lachmund, U.; Roeren, T. Lymphangiography: Forgotten tool or rising star in the diagnosis and therapy of postoperative lymphatic vessel leakage. Cardiovasc. Interv. Radiol. 2007, 30, 968–973. [Google Scholar] [CrossRef]
- Jardinet, T.; Van Veer, H.; Nafteux, P.; Depypere, L.; Coosemans, W.; Maleux, G. Intranodal lymphangiography with high-dose ethiodized oil shows efficient results in patients with refractory, high-output postsurgical chylothorax: A retrospective study. Am. J. Roentgenol. 2021, 217, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, R.; Sugimoto, K.; Fujii, M.; Miyamoto, N.; Okada, T.; Yamaguchi, M.; Sugimura, K. Therapeutic effectiveness of diagnostic lymphangiography for refractory postoperative chylothorax and chylous ascites: Correlation with radiologic findings and preceding medical treatment. Am. J. Roentgenol. 2013, 201, 659–666. [Google Scholar] [CrossRef]
- Yoshimatsu, R.; Yamagami, T.; Miura, H.; Matsumoto, T. Prediction of therapeutic effectiveness according to CT findings after therapeutic lymphangiography for lymphatic leakage. Jpn. J. Radiol. 2013, 31, 797–802. [Google Scholar] [CrossRef]
- Matsumoto, T.; Yamagami, T.; Kato, T.; Hirota, T.; Yoshimatsu, R.; Masunami, T.; Nishimura, T. The effectiveness of lymphangiography as a treatment method for various chyle leakages. Br. J. Radiol. 2009, 82, 286–290. [Google Scholar] [CrossRef]
- Abe, T.; Kawakami, J.; Uemura, N.; Kawai, R.; Sato, Y.; Inaba, Y.; Ito, S.; Komori, K.; Fukaya, M.; Shinoda, M.; et al. Therapeutic strategy for chylous leakage after esophagectomy: Focusing on lymphangiography using Lipiodol. Esophagus 2016, 13, 237–244. [Google Scholar] [CrossRef]
- Li, L.; Wu, X.; Liu, D.; Zhang, W.; Yang, L.; Pan, F. Preliminary Exploration of Transpedal Lymphangiography with High-Dose Ethiodized Oil Application in the Treatment of Postoperative Chylothorax. Front. Med. 2021, 8, 754781. [Google Scholar] [CrossRef]
- Tabchouri, N.; Frampas, E.; Marques, F.; Blanchard, C.; Jirka, A.; Regenet, N. Chylous Ascites Management After Pancreatic Surgery. World J. Surg. 2017, 41, 1054–1060. [Google Scholar] [CrossRef]
- Iwai, T.; Uchida, J.; Matsuoka, Y.; Kosoku, A.; Shimada, H.; Nishide, S.; Kabei, K.; Kuwabara, N.; Yamamoto, A.; Naganuma, T.; et al. Experience of Lymphangiography as a Therapeutic Tool for Lymphatic Leakage After Kidney Transplantation. Transpl. Proc. 2018, 50, 2526–2530. [Google Scholar] [CrossRef]
- Liu, J.; Sato, Y.; Motoyama, S.; Ishiyama, K.; Yamada, K.; Yamamoto, M.; Wakita, A.; Kawakita, Y.; Imai, K.; Saito, H.; et al. Ultrasound-guided intranodal Lipiodol lymphangiography from the groin is useful for assessment and treatment of post-esophagectomy chylothorax in three cases. Int. J. Surg. Case Rep. 2016, 29, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Kariya, S.; Nakatani, M.; Yoshida, R.; Ueno, Y.; Komemushi, A.; Tanigawa, N. Repeated Intranodal Lymphangiography for the Treatment of Lymphatic Leakage. Lymphology 2015, 48, 59–63. [Google Scholar] [PubMed]
- Chen, C.Y.; Chen, Y.H.; Shiau, E.L.; Liang, H.L.; Chang, H.S.; Chen, H.C. Therapeutic role of ultrasound-guided intranodal lymphangiography in refractory cervical chylous leakage after neck dissection: Report of a case and review of the literature. Head Neck 2016, 38, E54–E60. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.F.; Wu, C.T.; Hsieh, W.C.; Huang, J.J. Management of intractable post-adrenalectomy chylous ascites with microsurgical intra-abdominal lymphaticovenous anastomosis: A case report and literature review. Microsurgery 2021, 41, 480–487. [Google Scholar] [CrossRef]
- Sheybani, A.; Gaba, R.C.; Minocha, J. Cerebral embolization of ethiodized oil following intranodal lymphangiography. Semin. Interv. Radiol. 2015, 32, 10–13. [Google Scholar] [CrossRef]
- Taki, Y.; Sato, S.; Suzuki, K.; Nagai, E.; Watanabe, M.; Shishido, Y.; Nakajima, N.; Takagi, M. A case of acute respiratory distress syndrome due to lymphography with Lipiodol for chylothorax after esophagectomy. Surg. Case Rep. 2019, 5, 1. [Google Scholar] [CrossRef]
- Lamine, N.; Agrafiotis, A.C.; Lardinois, I. Lipiodol lymphangiography as a treatment for refractory postoperative chylothorax: A case report. Monaldi Arch. Chest Dis. 2021, 91, 4. [Google Scholar] [CrossRef]
- Nawabi, A.; Kahle, A.C.; Baral, P.; King, C.D.; Nawabi, P. Lymphangiography with Lipiodol as a diagnostic and therapeutic approach for Chyle Leak ascites following Simultaneous Pancreas-Kidney Transplant. J. Surg. Case Rep. 2021, 2021, rjab029. [Google Scholar] [CrossRef]
- Ushijima, H.; Hida, J.I.; Haeno, M.; Koda, M.; Ueda, K.; Kawamura, J. Successful treatment of intractable chylous ascites after laparoscopic low anterior resection using lymphangiography and embolization with Lipiodol: A case report. Int. J. Surg. Case Rep. 2021, 84, 106064. [Google Scholar] [CrossRef]
- Nakamura, K.; Nakayama, K.; Minamoto, T.; Ishibashi, T.; Ohnishi, K.; Yamashita, H.; Ono, R.; Sasamori, H.; Razia, S.; Kamrunnahar, S.; et al. Ultrasound-guided intranodal lymphangiography with Lipiodol for treatment of chylous ascites following surgery for ovarian cancer: A case report. Mol. Clin. Oncol. 2018, 9, 178–180. [Google Scholar] [CrossRef]
- Verhaeghe, L.; Van Holsbeeck, A.; Kager, J.; Ampe, J.; Mermuys, K.; Maleux, G. Postoperative lymphocele causing obturator nerve entrapment, treated with percutaneous drainage and intranodal poppyseed oil (Lipiodol)-based lymphangiography. J. Vasc. Surg. Cases Innov. Tech. 2021, 7, 698–700. [Google Scholar] [CrossRef] [PubMed]
- Hirata, M.; Shimizu, A.; Abe, S.; Ichinose, A.; Sugiyama, A.; Tanino, Y.; Watanabe, S.; Nakano, R.; Kato, Y.; Miyahara, T.; et al. CT-Guided Intranodal Lymphangiography for Postoperative Chylous Ascites. Cardiovasc. Interv. Radiol. 2017, 40, 1281–1284. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Kubo, N.; Yamamoto, A.; Sakurai, K.; Toyokawa, T.; Tanaka, H.; Muguruma, K.; Yashiro, M.; Maeda, K.; Hirakawa, K.; et al. Cervical chylous leakage following esophagectomy that was successfully treated by intranodal Lipiodol lymphangiography: A case report. BMC Surg. 2017, 17, 20. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, R.; Mokuno, Y.; Matsubara, H.; Kaneko, H.; Sato, Y.; Iyomasa, S. Chylothorax after hepatectomy: A case report. J. Med. Case Rep. 2018, 12, 347. [Google Scholar] [CrossRef]
- Han, J.; Aron, M. Refractory Lymphatic Ascites After Radical Prostatectomy. Urology 2020, 145, 9–10. [Google Scholar] [CrossRef]
- Rubio, J.S.; Wojtowicz, D.; Amore, M.A.; Iriarte, G.; Di Pietrantonio, S. Giant idiopathic lymphocele 18 years after kidney transplantation, treated using lymphatic embolization with Lipiodol: Report of a rare case. Exp. Clin. Transplant. 2021, 19, 1099–1102. [Google Scholar] [CrossRef]
- Onikubo, Y.; Yagi, S.; Yamada, K.; Kato, D.; Wake, H.; Enomoto, N.; Nohara, K.; Tajima, T.; Kokudo, N. Computed tomography-guided lymphangiography from the para-aortic lymph node: A useful approach for chylothorax after esophagectomy. Gen. Thorac. Cardiovasc. Surg. 2022, 70, 308–311. [Google Scholar] [CrossRef]
- Rouiller, B.; Lutz, J.A.; Kocher, G.J.; Magnusson, L. Bilateral thoracic duct ligation for persisting postoperative chylothorax. Interact. Cardiovasc. Thorac. Surg. 2020, 31, 583–584. [Google Scholar] [CrossRef]
- Kitahara, H.; Yoshitake, A.; Hachiya, T.; Inaba, Y.; Tamura, K.; Yashiro, H.; Nakatsuka, S.; Shimizu, H. Management of Aortic Replacement-Induced Chylothorax by Lipiodol Lymphography. Ann. Vasc. Dis. 2015, 8, 110–112. [Google Scholar] [CrossRef]
- Minegishi, K.; Tsubochi, H.; Hamamoto, K.; Endo, S. Massive lymphatic leakage after lung cancer surgery via median sternotomy. J. Surg. Case Rep. 2019, 2019, rjz178. [Google Scholar] [CrossRef]
- Lee, K.H.; Jung, J.S.; Cho, S.B.; Lee, S.H.; Kim, H.J.; Son, H.S. Thoracic duct embolization with Lipiodol for chylothorax due to thoracic endovascular aortic repair with debranching procedure. Korean J. Thorac. Cardiovasc. Surg. 2015, 48, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Tsuneki, T.; Yuasa, Y.; Nishino, T.; Tomibayashi, A.; Motoki, T.; Fukumura, Y. A case of aortoduodenal fistula presenting with postoperative lymphatic leakage. Int. J. Surg. Case Rep. 2022, 94, 107147. [Google Scholar] [CrossRef] [PubMed]
- Takeno, A.; Tamura, S.; Miki, H.; Tanigawa, N.; Taniguchi, H.; Nakahira, S.; Suzuki, R.; Nakata, K.; Takeda, Y.; Kato, T. Chyluria after ligation of the thoracic duct: A rare complication after thoracoscopic-assisted esophagectomy for esophageal cancer. Surg. Today 2014, 44, 757–760. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.T.; Chen, T.M. Chylous ascites after pedicled transverse rectus abdominis myocutaneous flap harvest. Acta Chir. Belg. 2016, 116, 256–259. [Google Scholar] [CrossRef]
- Mine, S.; Udagawa, H.; Kinoshita, Y.; Makuuchi, R. Post-esophagectomy chylous leakage from a duplicated left-sided thoracic duct ligated successfully with left-sided video-assisted thoracoscopic surgery. Interact. Cardiovasc. Thorac. Surg. 2008, 7, 1186–1188. [Google Scholar] [CrossRef]
- Vázquez-Vicente, D.; Navarro, B.; García, J.E.; Fernández, B.; Urbano, J.; Plaza, J. Management of a postsurgical chylous ascites following a laparoscopic retroperitoneal para-Aortic lymphadenectomy. Eur. J. Gynaecol. Oncol. 2018, 39, 151–153. [Google Scholar] [CrossRef]
- Masaaki, Y. Yamamoto 2015. Anticancer Res. 2015, 35, 891–895. [Google Scholar]
- Guerbet LLC. LIPIODOL® (Ethiodized Oil) Injection. Available online: https://www.swissmedic.ch (accessed on 1 September 2024).
- Hill, H.; Srinivasa, R.N.; Gemmete, J.J.; Hage, A.; Bundy, J.; Chick, J.F.B. Endolymphatic Ethiodized Oil Intranodal Lymphangiography and Cyanoacrylate Glue Embolization for the Treatment of Postoperative Lymphatic Leak After Robot-Assisted Laparoscopic Pelvic Resection. J. Endourol. Case Rep. 2018, 4, 66–71. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The clavien-dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Sommer, C.M.; Pieper, C.C.; Itkin, M.; Nadolski, G.J.; Hur, S.; Kim, J.; Maleux, G.; Kauczor, H.-U.; Richter, G.M. Conventional Lymphangiography (CL) in the Management of Postoperative Lymphatic Leakage (PLL): A Systematic Review. RoFo Fortschritte Auf Dem Geb. Der Rontgenstrahlen Und Der Bildgeb. Verfahr. 2020, 192, 1025–1035. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS | Inclusion | Exclusion |
|---|---|---|
| Population | Adult patients > 18 years of age Presenting post-operative lymphatic leakage | Non-post-operative lymphatic leaks LL performed in pediatric cases |
| Intervention | LL for diagnostic or therapeutic purposes | LL using alternative contrast agent and the use of glue/coils/other percutaneous procedures for embolization |
| Comparison | Conservative treatment measures of lymphatic leaks | N/A |
| Outcome | Therapeutic and clinical success of LL | No report of therapeutic and clinical success of LL |
| Study design | Clinical studies and case series | Animal and cadaveric studies Reviews, congress abstracts, letters |
| Author/Year | Title | N | Surgical Indication | Surgical Intervention |
|---|---|---|---|---|
| Pan/ 2022 [12] | Treatment of postoperative lymphatic leakage applying transpedal lymphangiography—experience in 355 consecutive patients | 258 (355) | Terminal renal insufficiency (20.8%) Abdominal carcinoma/sarcoma (16.6%) PAOD (10.1%) Malignant melanoma (6.5%) Aortic aneurysm/dissection (5.9%) Pelvic carcinoma/sarcoma (5.4%) Vulvar squamous cell carcinoma (4.8%) Esophagus carcinoma (4.5%) Coronary heart disease (3.4%) Valvular heart disease (2.0%) Other benign diseases (11.3%) Other malignant tumors (8.7%) | Exlap with tumor resection (26.8%) Kidney transplantation (18.9%) Transfemoral catheterization (14.9%) Cutaneous/s.c. tumor resection (14.9%) Peripheral artery bypass (6.8%) Thoracic-abdominal esophagus resection (5.4%) Vulvectomy (3.9%) S.c. hematomectomy with vascular repair (2.5%) Explorative thoracotomy (0.8%) Radical thyroid tumor resection (0.8%) Artificial femoral head replacement (0.8%) Others (3.4%) |
| Gruber-Rouh /2014 [13] | Direct lymphangiography as treatment option of lymphatic leakage: Indications, outcomes, and role in patient’s management | 71 | Cutaneous Melanoma (52.1%) Merkel Cell Carcinoma (4.2%) Ovarian cancer (2.8%) Other (40.9%) | Inguinal LND (52.1%) Pelvic LND (2.8%) Renal transplantation (14%) Radical prostatectomy (9.8%) Cystectomy (2.8%) Splenectomy (1.4%) Esophagectomy (9.8%) Gastrectomy (7%) |
| Alejandre-Lafont/ 2010 [14] | Effectiveness of therapeutic lymphography on lymphatic leakage | 33 | Bronchial carcinoma (10%) Aneurysmal disease (6%)) Osteochondrosis (2%) Coronary heart disease (4%) Liver cirrhosis (8%) Lymphangiomyomatosis (2%) Morbus Hodgkin (2%) Non-Hodgkin lymphoma (8%) Esophageal carcinoma (14%) Sarcoidosis (2%) Pancreatitis (2%) Appendicitis (2%) Nephrotic syndrome (8%) Endometrium carcinoma (2%) Testicular carcinoma (4%) Bladder carcinoma (4%) Melanoma (2%) Penile carcinoma (2%) Prostate carcinoma (2%) | Pneumectomy + LND (10%) Cystectomy (6%) Spondylodesis (2%) Cardiac bypass (4%) Esophagectomy + LND (14%) Duodeno-pancreatectomy (2%) Appendectomy (2%) Kidney transplantation (8%) Hysterectomy + LND (2%) Cystectomy (4%) LND (6%) |
| Kos/ 2007 [15] | Lymphangiography: forgotten tool or rising star in the diagnosis and therapy of postoperative lymphatic vessel leakage | 22 | Bronchial carcinoma (9%) Renal cell carcinoma (4.5%) Polycystic kidney disease (4.5%) Esophageal carcinoma (9%) Melanoma (18%) M. Hodgkin (4.5%) Vulval carcinoma (4.5%) Penile carcinoma (4.5%) Myasthenia gravis (4.5%) Aneurysmal disease (9%) Embryonic carcinoma (4.5%) Prostate carcinoma (4.5%) Coronary heart disease (4.5%) PAOD (4.5%) Gastric carcinoma (4.5%) Thigh seroma (4.5%) | Pneumectomy (9%) Nephrectomy (9%) Esophagectomy (9% LND (18%) Thymectomy (18%) Endoaneurysmoraphy (4.5%) Semicastration + retroperitoneal LND (9%) Prostatectomy (4.5%) Vascular bypass (9%) Partial gastrectomy (4.5%) Soft-tissue resection (4.5%) |
| Jardinet/ 2020 [16] | Intranodal lymphangiography with high-dose ethiodized oil shows efficient results in patients with refractory, high-output postsurgical chylothorax: a retrospective study | 18 | N.S. | Esophagectomy (72%) Lobectomy (10%) Explorative thoracotomy (4.5%) Pericardiectomy (4.5%) Nissen fundoplication (4.5% Pericardiectomy (4.5%) |
| Kawasaki/ 2013 [17] | Therapeutic effectiveness of diagnostic lymphangiography for refractory postoperative chylothorax and chylous ascites: correlation with radiologic findings and preceding medical treatment | 14 | Gastric cancer (14.2%) Esophageal carcinoma (42.8%) Esophageal melanoma (7.1%) Aortic valve stenosis (7.1%) Dissected aneurysm (7.1%) Thoracoabdominal aortic aneurysm (14.2%) Ruptured thoracic aortic aneurysm (7.1%) | Partial esophagectomy (28.5%) Total esophagectomy (14.2%) Thoracic/thoracoabdominal aortic replacement (28.5%) Aortic valve replacement with mitral valvuloplasty (7.1%) Distal gastrectomy (14.2%) Subtotal esophagectomy (7.1%) |
| Yoshimatsu/ 2013 [18] | Prediction of therapeutic effectiveness according to CT findings after therapeutic lymphangiography for lymphatic leakage | 14 | Esophageal cancer (42.8%) Gastric cancer (7.1%) Rectal cancer (7.1%) Annulo-aortic ectasia (14.2%) Scoliosis (7.1%) Colon cancer (7.1%) Testicular cancer (14.2%) | Esophagectomy (42.8%) Gastrectomy (7.1%) Proctectomy (7.1%) Aortic root replacement (7.1%) Surgery for scoliosis (7.1%) Colectomy (7.1%) Retroperitoneal (7.1%) LND (14.2%) |
| Matsumoto/ 2009 [19] | The effectiveness of lymphangiography as a treatment method for various chyle leakages | 9 | Esophageal cancer (44.5%) Breast cancer (11.1%) Ovarian cancer (11.1%) Testicular cancer (11.1%) Annuloaortic ectasia (11.1%) | Esophagectomy (44.5%) Axillary LND (11.1%) Pelvic LND (11.1%) Retroperitoneal LND (11.1%) Aortic root replacement (11.1%) |
| Abe/ 2016 [20] | Therapeutic strategy for chylous leakage after esophagectomy: focusing on lymphangiography using Lipiodol | 9 | Esophageal cancer (100%) | Subtotal esophagectomy and LND via right thoracotomy and laparotomy (100%) |
| Li/ 2021 [21] | Preliminary exploration of transpedal lymphangiography with high-dose ethiodized oil application in the treatment of postoperative chylothorax | 7 | Oesophageal carcinoma (28.5%) Non-small-cell lung carcinoma (71.5%) | Pulmonary resection + mediastinal LND (57.1%) Sublobar resection + mediastinal LND (14.3%) Esophagectomy + mediastinal LND (28.6%) |
| Tabchouri/ 2016 [22] | Chylous ascites management after pancreatic surgery | 5 | Cancer as primary diagnosis | Pancreatic surgery (100%) |
| Author/Year | Lymphatic Leak Presentation | Leak management Before LL | Timeframe of Conservative Measures |
|---|---|---|---|
| Pan/ 2022 [12] | Cervical chylous fistula (1.6%) Chylothorax (10.1%) Chylous ascites (21.3%) Chylo-retroperitoneum (2.7%) Pelvic lymphocele (20.5%) Lymphocutaneous fistula (43.8%) | Nutrition management Somatostatin analogs Drainage Wound vacuum therapy | More than 2 weeks |
| Gruber-Rouh /2014 [13] | Lymphatic fistula (52.1%) Lymphocele (15.49%) Chylothorax (18.3%) Chylous ascites (14%) | Nutrition management: TPN Drainage Pressure dressing | More than 3 weeks |
| Alejandre-Lafont/ 2010 [14] | Chylothorax (60%) Lymphocele (18%) Chylous ascites (6%) Chylothorax + chylous ascites (8%) Chylous ascites + lymphocele (8%) | Nutrition management: TPN or MCT Diet Iterative drainage/paracentesis Compression bandages Diuretics Sclerotherapy | No timeframe |
| Kos/ 2007 [15] | Chylothorax (36.4%) Chylous ascites (4.5%) Lymphatic fistula (41%) Lymphocele (13.6%) Chylothorax + chylous ascites (4.5%) | Nutrition management: TPN or MCT Diet Compression Drainage | No timeframe/in addition to LL |
| Jardinet/ 2020 [16] | Bilateral chylothorax (39%) Unilateral chylothorax (61%) | Nutrition management: TPN or MCT Diet Attempt at TDL | No timeframe/in addition to LL |
| Kawasaki/ 2013 [17] | Chylothorax (78.5%) Chylous ascites (14.2%) Chylothorax + chylous ascites (7.14%) | Nutrition management: NBM, TPN Drainage Octreotide (300 μg/day) Attempt at TDL/pleurodesis | No timeframe |
| Yoshimatsu/ 2013 [18] | Chylothorax (50%) Chylous ascites (35.7%) Lymphocele (7.1%) lymphatic fistula (7.1%) | Nutrition management: TPN or MCT Diet Drainage | No timeframe |
| Matsumoto/ 2009 [19] | Chylothorax (55.5%) Chylous ascites (22.2%) Lymphatic fistula (22.2%) | Nutrition management: TPN or MCT Diet Drainage | No timeframe |
| Abe/ 2016 [20] | Chylothorax (100%) | Nutrition management: TPN or MCT Diet Drainage Octreotide acetate | No timeframe |
| Li/ 2021 [21] | Chylothorax (100%) | Nutrition management: TPN Somatostatin | More than 2 weeks |
| Tabchouri/ 2016 [22] | Chylous ascites (100%) | Nutrition management: NBM, TPN, MCT Diet Drainage Somatostatin for 3 days | For 10–14 days |
| Author/Year | Access Site for LL | Lipiodol Quantity and Injection Speed | Imaging Post LL |
|---|---|---|---|
| Pan/ 2022 [12] | Monopedal (88.7%) Bipedal (11.3%) | 10 mL (7–14) At 0.1–0.5 mL/min for an hour | X-ray: 0–1 h, 1–3 h, and 4–6 h If indeterminate Lipiodol extravasation: CT If Lipiodol extravasation is still not marked, CT at 24 h |
| Gruber-Rouh /2014 [13] | Monopedal (66.1%) lymphatic fistula or lymphocele Bipedal (33.8%) chylothorax or chylous ascites | 11.7 mL (4–20) At 6–8 mL/h | X-ray overview of the feet and legs If the lymphatic leakage was not visible, about 24 h after the procedure unenhanced CT was performed |
| Alejandre-Lafont/ 2010 [14] | Monopedal (92%) Bipedal (8%) | 1 mL/10 kg, max 20 mL At 5–10 mL/h | X-ray shortly after starting the injection and again after finishing the injection (about 2 h after start of injection) |
| Kos/ 2007 [15] | Monopedal (91%) Bipedal (9%) | 1 mL/10 kg per foot, max 14 mL At 4–7 mL/h | X-ray during filling phase plus late-phase after about 24 h |
| Jardinet/ 2020 [16] | Inguinal intranodal (100%) | 75 mL (40–140) Speed not specified | Radiographic guidance Cone-beam CT |
| Kawasaki/ 2013 [17] | Bipedal (100%) | 16 mL total (8/foot) Injection pressure 1.5–2.0 kg/cm2 | CT and X-ray from the pelvis to chest just after LL |
| Yoshimatsu/ 2013 [18] | Bipedal (100%) | 8 mL/foot not t exceeding a volume of 12 mL At 0.1 mL/min | CT and X-ray |
| Matsumoto/ 2009 [19] | Monopedal (55.5%) Bipedal (45.5%) | 9.8 mL (6–12) At 0.1 mL/min | Abdominal + chest X-ray 2 h after LL Native CT 5–28 h after LL |
| Abe/ 2016 [20] | Monopedal (66.6%) Intranodal (33.3%) | 10 mL At 0.1 mL/min | Abdominal X-ray 1–2 h after LL Chest and abdominal X-ray + CT 2–6 h after LL |
| Li/ 2021 [21] | Monopedal (100%) | 27.6 mL (21.2–30) At 0.4 mL/min | Fluoroscopy every 2–5 min until opacification of the left jugular vein angle CT immediate and at 24 h |
| Tabchouri/ 2016 [22] | Bipedal (100%) | 12 mL maximum over 30–45 min | An abdominal and pelvic CT scan 120 min after LL |
| Author/Year | Indication for LL | Time to LL | Technical Success | Clinical Success | Mean Daily Leakage Before LL | Mean Daily Leakage After LL | Mean Leakage Timeframe After LL | Bailout Procedures |
|---|---|---|---|---|---|---|---|---|
| Pan/ 2022 [12] | Failed CM for >2 weeks | 26 days (16–49 days) | 169/258 (65.5%) | 159/258 (61.6%) 159/169 (94%) | 500 mL (300–1100 mL) | N.S. | 5 days (2–7 days) | Surgical revision, percutaneous sclerotherapy, low-dose RT, and continuous CM |
| Gruber-Rouh /2014 [13] | Unlikely to be cured by CM for >3 weeks | N.S. (>21 days) | 64/71 (90.1%) | 45/71 (63.3%) 45/64 (70.3%) | 300.4 mL (10–1000 mL) | N.S. <200 mL (n = 33) >200 mL (n = 31) | N.S. (10 days–4 weeks) | Surgical revision |
| Alejandre-Lafont/ 2010 [14] | Failed CM/surgical intervention too risky No timeframe | 24 days (3–117 days) | 43/49 (87.7%) | 27/49 (55.1%) 27/43 (63%) | N.S. (500–2500 mL) | N.S. | N.S. (1–14 days) | TDL or resection of the lymphocele |
| Kos/ 2007 [15] | N.S. | N.S. (5–154 days) | 20/22 (90%) | 11/22 (50%) 11/20) (55%) | N.S. (200–3000 mL) | N.S. | N.S. (Maximum 3 weeks) | Lymphocele fenestration, surgical clipping |
| Jardinet/ 2020 [16] | Failed CM/Post TDL No timeframe | 28 days (4–104 days) | 17/18 (94%) | 15/18 (83%) 11/14 (78%) * | 1852 mL (525–3760 mL) | N.S. | 12 days (1–25 days) | TDL |
| Kawasaki/ 2013 [17] | Failed CM No timeframe | 13.5 days (3–62 days) | 14/14 (100%) | 9/14 (64.3%) | 950 mL (300–3000 mL) | N.S. 2–100 mL (n = 5) 100–200 mL (n = 4) >700 mL (n = 5) | 8 days (3–29 days) | TDL or pleurodesis |
| Yoshimatsu/ 2013 [18] | Unlikely to be cured by CM No timeframe | N.S | 14/14 (100%) | 8/14(57%) | 1005 mL (150–3000 mL) | 806 mL (50–3000 mL) | N.S. | Pleurosclerosis Implantation of a peritoneovenous shunt |
| Matsumoto/ 2009 [19] | Unlikely to be cured by CM No timeframe | N.S. (10–42 days) | 9/9 (100%) | 8/9(89%) | 533 mL (150–1500 mL) | 256 mL (50–1500) | 17 days (4–31 days) | TDL |
| Abe/ 2016 [20] | Failed CM No timeframe | 15 days (6–23 days) | 9/9 (100%) | 2/9(22.2%) | N.S. <500 mL (n = 1) 500–1000 mL (n = 2) >1000 mL (n = 6) | N.S. <500 mL (n = 5) 500–1000 mL (n = 1) >1000 mL (n = 3) | 13 days (4–21 days) | Chemical pleurodesis or TDL/clipping |
| Li/ 2021 [21] | Failed CM for >2 weeks | 20 days (15–31 days) | 7/7 (100%) | 6/7(86%) | 1500 mL (1100–2000 mL) | N.S. | 7 days (4–13 days) | Percutaneous afferent lymphatic vessel sclerotherapy |
| Tabchouri/ 2016 [22] | N.S. | 30 days (15–55 days) | N.S. | 5/5(100%) | 1700 mL (600–3700 mL) | N.S. | 7.6 days (2–21 days) | None |
| Age/Gender (Unique I.D) | Surgical Indication/Intervention | Lymphatic Leak Presentation | Management Before LL | Technical Aspects of LL | Technical Success | Clinical Success | Mean Daily Leakage Before LL | Mean Daily Leakage After LL | Bailout Procedures | Length of Stay |
|---|---|---|---|---|---|---|---|---|---|---|
| 67 F (A) | Esophageal carcinoma/Esophagectomy | Bilateral Chylothorax | TPN | 15 mL POD6 | Yes | Yes | 1080 mL | Day 1: 550 mL Day 4: 50 mL | - | 25 days |
| 46 M (B) | Esophageal carcinoma/Esophagectomy | Unilateral Chylothorax | N.S. | 10 mL POD6 | No * | No | 1000 mL | 1000 mL No change | Back to CM—TPN | 20 days |
| 62 M (C) | Bronchial carcinoma/Lobectomy | Unilateral Chylothorax | TPN TDL | 10 mL POD16 | Yes | No | 900 mL | Day 3: 500 mL ** | TDL | 35 days |
| 68 M (D) | Bronchial carcinoma/Lobectomy | Unilateral Chylothorax | TPN | 20 mL POD14 | Yes | Yes | 1700 mL | Day 1: 60 ml | - | 21 days |
| 67 M (E) | Duodenal carcinoma/Lobectomy | Chylous Ascites | TPN | 15 mL POD8 | Yes | Yes | 750 mL | Day 1: 95 mL Day 3: 60 mL | - | 15 days |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulz, S.N.; Miftaroski, A.; Rouiller, B.; Egger, B.; Lutz, J.A.; Widmer, L. Ultrasound-Guided Intranodal Lipiodol Lymphangiography for the Assessment and Treatment of Chylous Leaks: A Retrospective Case Series from a Single Center in Switzerland and a Systematic Review of the Literature. J. Clin. Med. 2024, 13, 6432. https://doi.org/10.3390/jcm13216432
Schulz SN, Miftaroski A, Rouiller B, Egger B, Lutz JA, Widmer L. Ultrasound-Guided Intranodal Lipiodol Lymphangiography for the Assessment and Treatment of Chylous Leaks: A Retrospective Case Series from a Single Center in Switzerland and a Systematic Review of the Literature. Journal of Clinical Medicine. 2024; 13(21):6432. https://doi.org/10.3390/jcm13216432
Chicago/Turabian StyleSchulz, Stephanie Nicole, Almir Miftaroski, Benoit Rouiller, Bernard Egger, Jon A. Lutz, and Lucien Widmer. 2024. "Ultrasound-Guided Intranodal Lipiodol Lymphangiography for the Assessment and Treatment of Chylous Leaks: A Retrospective Case Series from a Single Center in Switzerland and a Systematic Review of the Literature" Journal of Clinical Medicine 13, no. 21: 6432. https://doi.org/10.3390/jcm13216432
APA StyleSchulz, S. N., Miftaroski, A., Rouiller, B., Egger, B., Lutz, J. A., & Widmer, L. (2024). Ultrasound-Guided Intranodal Lipiodol Lymphangiography for the Assessment and Treatment of Chylous Leaks: A Retrospective Case Series from a Single Center in Switzerland and a Systematic Review of the Literature. Journal of Clinical Medicine, 13(21), 6432. https://doi.org/10.3390/jcm13216432