‘Low-Plane’ Fractures of the Distal Humerus in Elderly Patients with Osteoporosis Show High Postoperative Complication Rates

 , ,
, , 
 ,
,
Abstract
1. Introduction
2. Methods
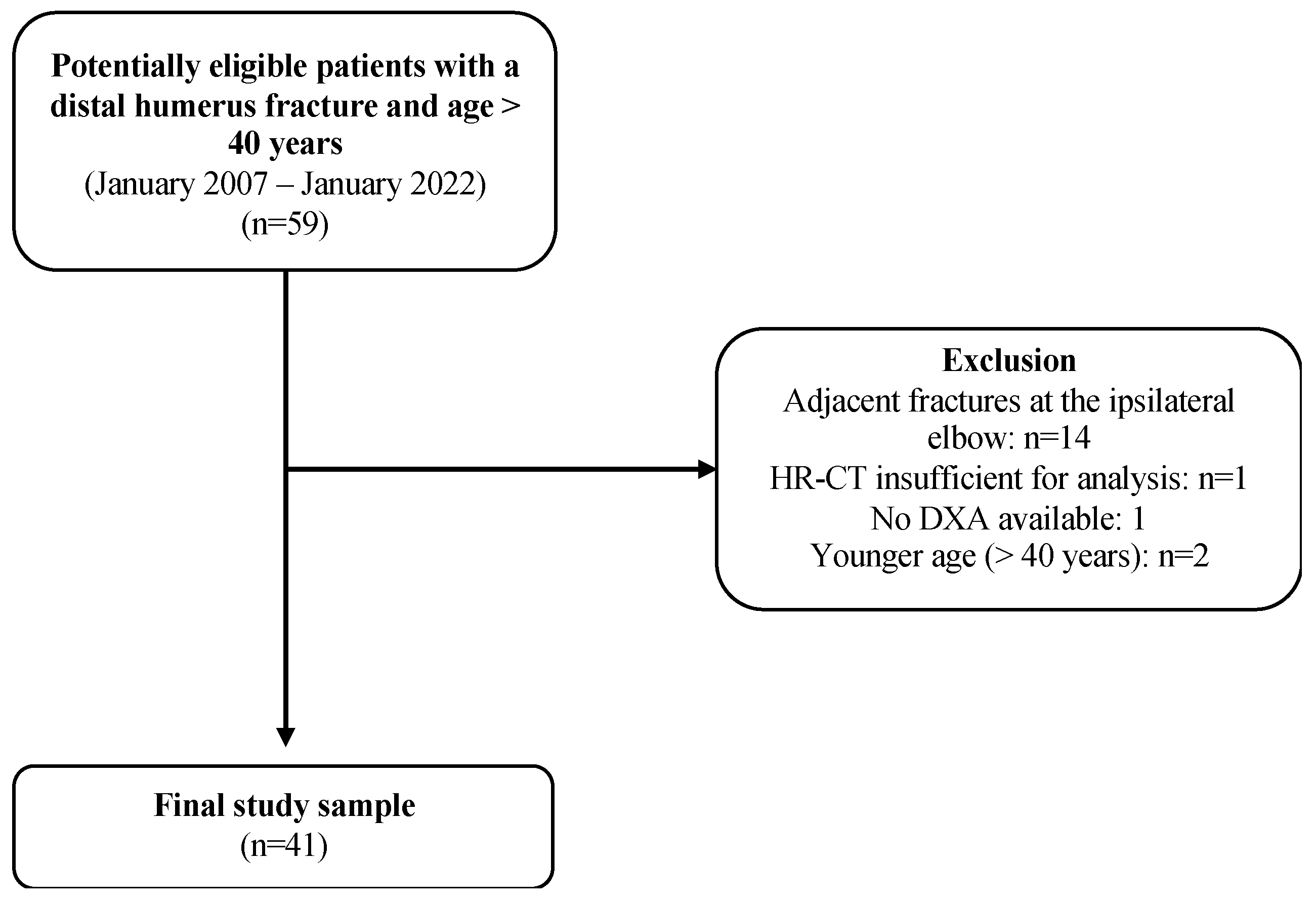
2.1. Patient Selection
2.2. Bone Mineral Density Assessment
2.3. Conventional CT
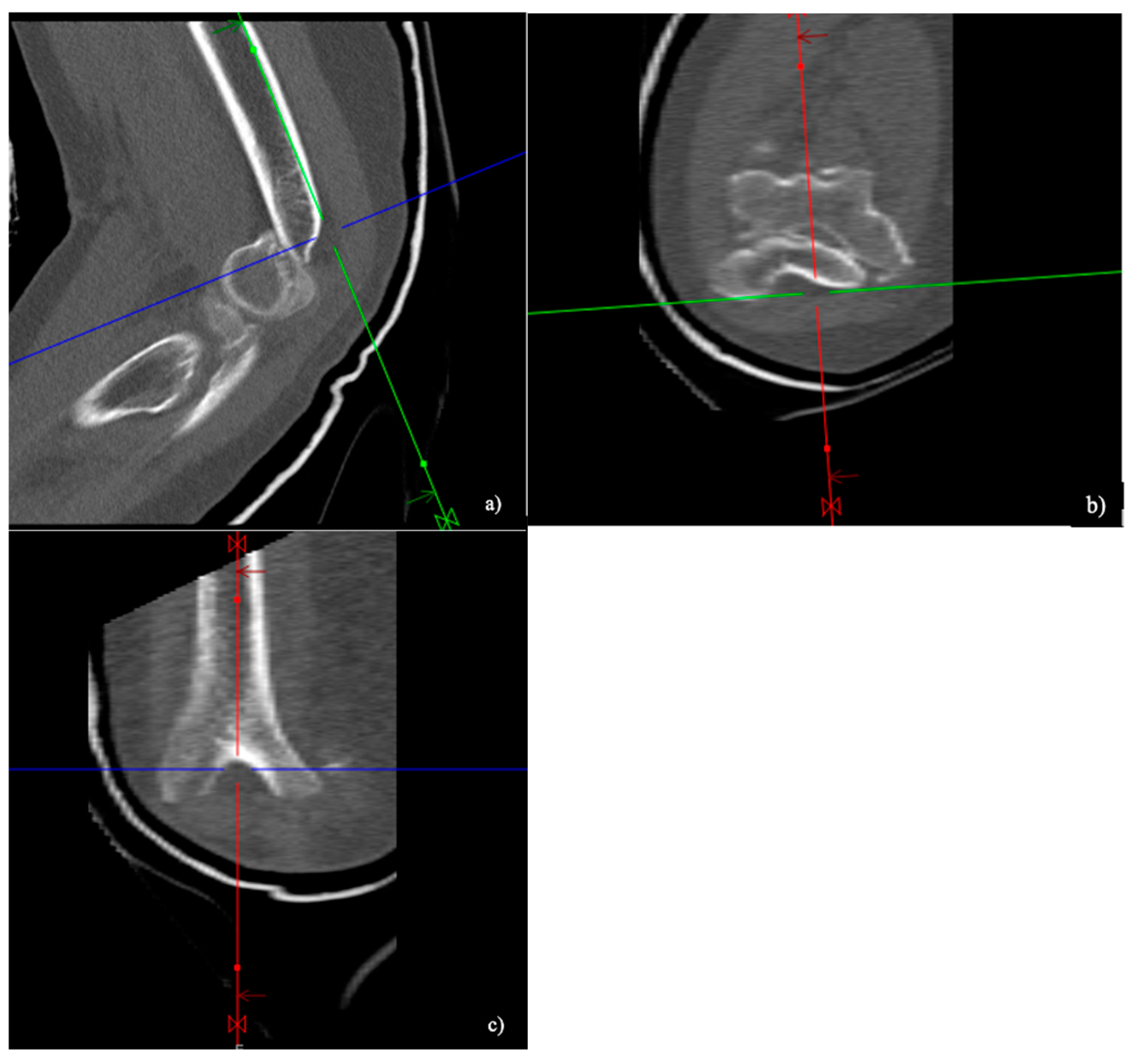
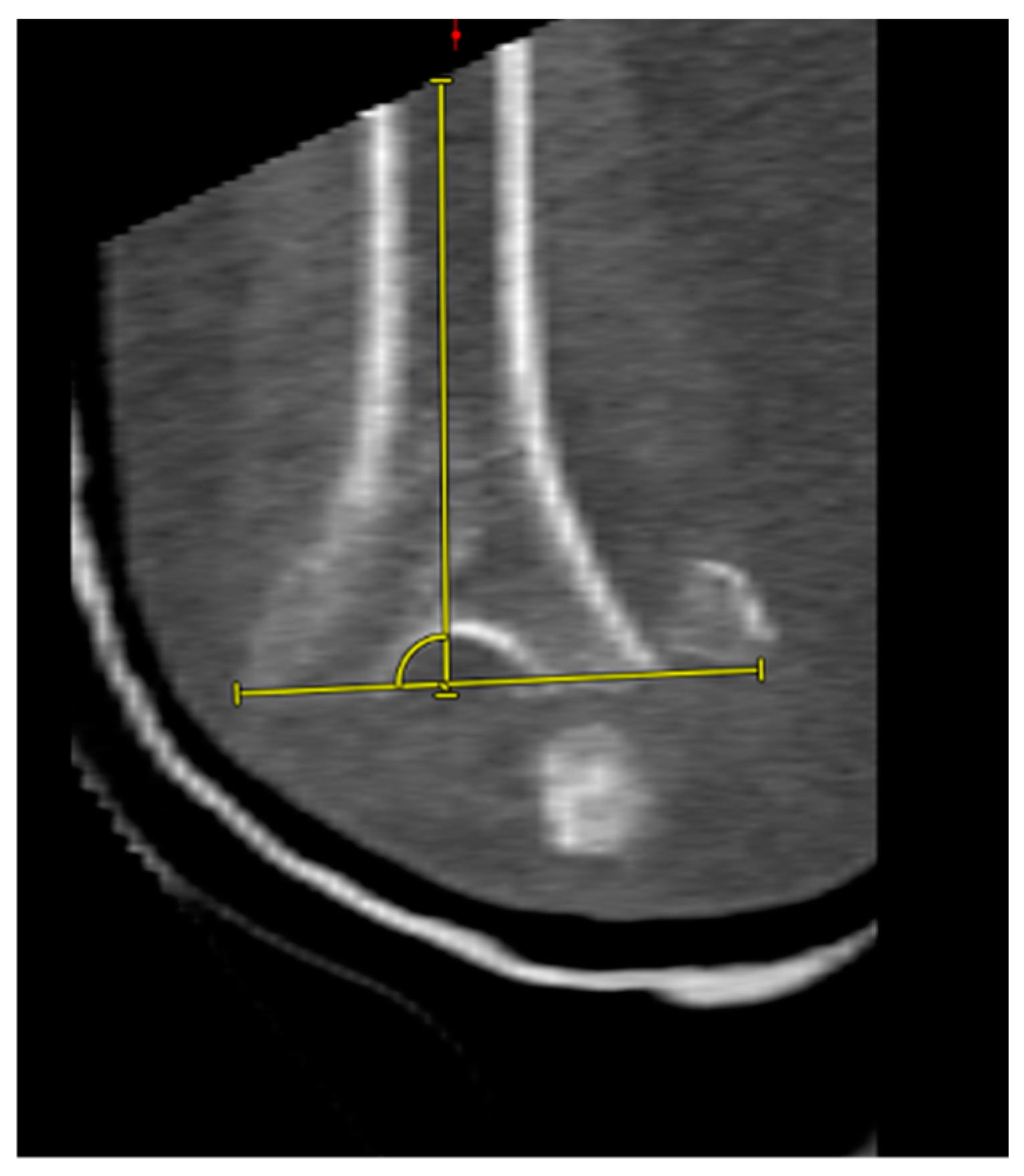
2.4. CT Image Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Surgical Treatment
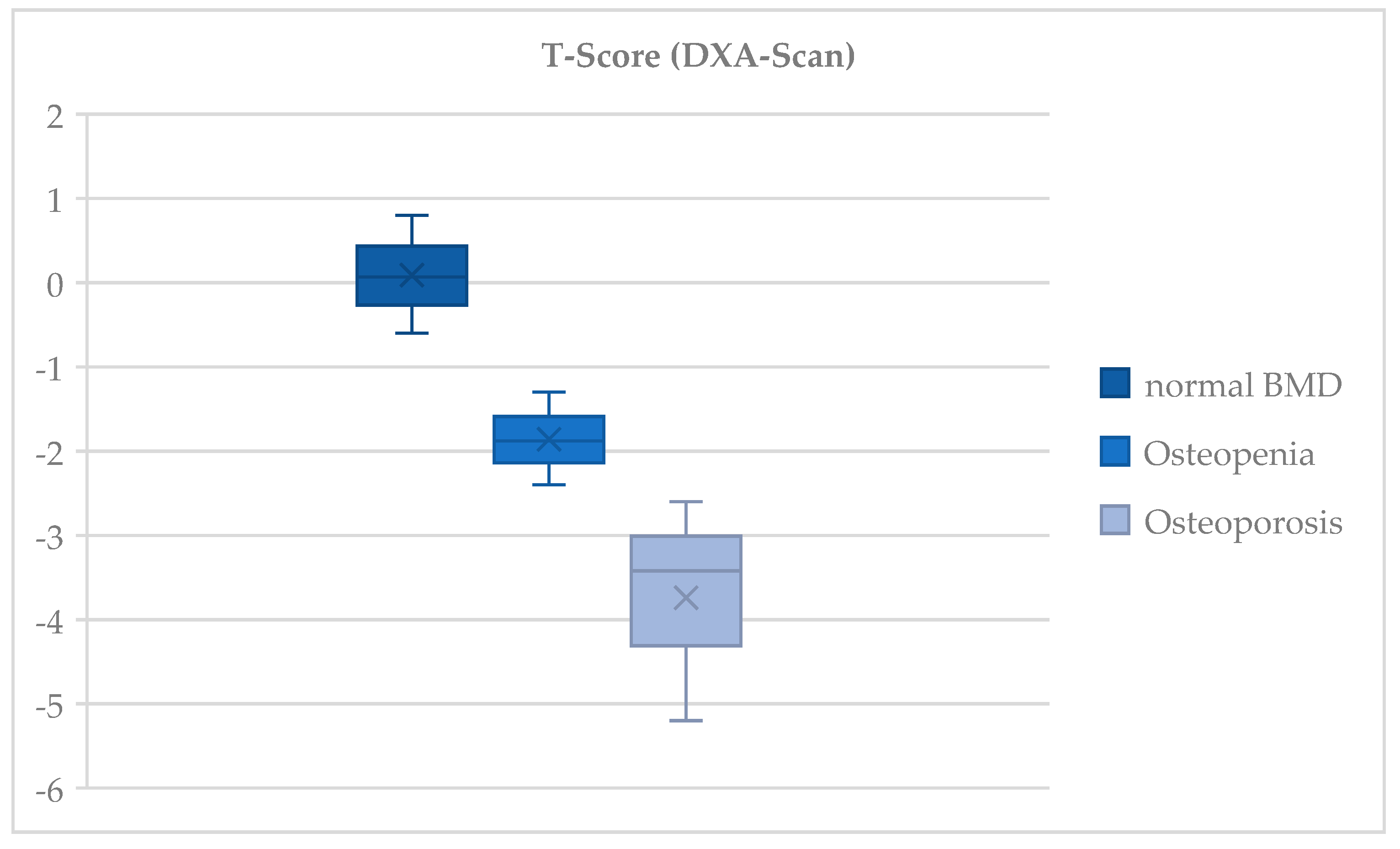
3.3. Bone Mineral Density
3.4. Classification of Fractures
3.5. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rose, S.H.; Melton, L.J., 3rd; Morrey, B.F.; Ilstrup, D.M.; Riggs, B.L. Epidemiologic features of humeral fractures. Clin. Orthop. Relat. Res. 1982, 168, 24–30. [Google Scholar] [CrossRef]
- Jupiter, J. Fracture of the distal humerus in the adult. Elb. Its Disord. 1993, 13, 328–366. [Google Scholar]
- Amir, S.; Jannis, S.; Daniel, R. Distal humerus fractures: A review of current therapy concepts. Curr. Rev. Musculoskelet. Med. 2016, 9, 199–206. [Google Scholar] [CrossRef]
- Robinson, C.M.; Hill, R.M.; Jacobs, N.; Dall, G.; Court-Brown, C.M. Adult distal humeral metaphyseal fractures: Epidemiology and results of treatment. J. Orthop. Trauma 2003, 17, 38–47. [Google Scholar] [CrossRef]
- Koval, K.J.; Zuckerman, J.D. Handbook of Fractures; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Nauth, A.; McKee, M.D.; Ristevski, B.; Hall, J.; Schemitsch, E.H. Distal Humeral Fractures in Adults. J. Bone Jt. Surg. (JBJS) 2011, 93, 686–700. [Google Scholar] [CrossRef]
- Diederichs, G.; Issever, A.S.; Greiner, S.; Linke, B.; Korner, J. Three-dimensional distribution of trabecular bone density and cortical thickness in the distal humerus. J. Shoulder Elb. Surg. 2009, 18, 399–407. [Google Scholar] [CrossRef]
- Frankle, M.A.; Herscovici, D., Jr.; DiPasquale, T.G.; Vasey, M.B.; Sanders, R.W. A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than age 65. J. Orthop. Trauma 2003, 17, 473–480. [Google Scholar] [CrossRef]
- Park, S.H.; Kim, S.J.; Park, B.C.; Suh, K.J.; Lee, J.Y.; Park, C.W.; Shin, I.H.; Jeon, I.H. Three-dimensional osseous micro-architecture of the distal humerus: Implications for internal fixation of osteoporotic fracture. J. Shoulder Elb. Surg. 2010, 19, 244–250. [Google Scholar] [CrossRef]
- Marcoin, A.; Eichler, D.; Kempf, J.F.; Clavert, P. Biomechanical model of distal articular humeral fractures-influence of bone density on the fracture threshold. Int. Orthop. 2020, 44, 1385–1389. [Google Scholar] [CrossRef]
- McKee, M.D.; Veillette, C.J.; Hall, J.A.; Schemitsch, E.H.; Wild, L.M.; McCormack, R.; Perey, B.; Goetz, T.; Zomar, M.; Moon, K.; et al. A multicenter, prospective, randomized, controlled trial of open reduction--internal fixation versus total elbow arthroplasty for displaced intra-articular distal humeral fractures in elderly patients. J. Shoulder Elb. Surg. 2009, 18, 3–12. [Google Scholar] [CrossRef]
- Moursy, M.; Wegmann, K.; Wichlas, F.; Tauber, M. Distal humerus fracture in patients over 70 years of age: Results of open reduction and internal fixation. Arch. Orthop. Trauma Surg. 2022, 142, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Gustilo, R.B.; Anderson, J.T. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: Retrospective and prospective analyses. J. Bone Jt. Surg. Am. 1976, 58, 453–458. [Google Scholar] [CrossRef]
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Reginster, J.Y. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2019, 30, 3–44. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calciu. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011; p. 1132. [Google Scholar] [CrossRef]
- Müller, M.E.; Koch, P.; Nazarian, S.; Joseph Schatzker, F.R.C.S. The Comprehensive Classification of Fractures of Long Bones; Springer: Berlin/Heidelberg, Germany, 1990. [Google Scholar]
- Dubberley, J.H.; Faber, K.J.; Macdermid, J.C.; Patterson, S.D.; King, G.J. Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J. Bone Jt. Surg. Am. 2006, 88, 46–54. [Google Scholar] [CrossRef]
- Södergård, J.; Sandelin, J.; Böstman, O. Mechanical failures of internal fixation in T and Y fractures of the distal humerus. J. Trauma 1992, 33, 687–690. [Google Scholar] [CrossRef]
- Charissoux, J.L.; Vergnenegre, G.; Pelissier, M.; Fabre, T.; Mansat, P. Epidemiology of distal humerus fractures in the elderly. Orthop. Traumatol. Surg. Res. 2013, 99, 765–769. [Google Scholar] [CrossRef]
- Varecka, T.F.; Myeroff, C. Distal Humerus Fractures in the Elderly Population. J. Am. Acad. Orthop. Surg. 2017, 25, 673–683. [Google Scholar] [CrossRef]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef]
- Rashki Kemmak, A.; Rezapour, A.; Jahangiri, R.; Nikjoo, S.; Farabi, H.; Soleimanpour, S. Economic burden of osteoporosis in the world: A systematic review. Med. J. Islam. Repub. Iran. 2020, 34, 154. [Google Scholar] [CrossRef]
- Stoddart, M.T.; Panagopoulos, G.N.; Craig, R.S.; Falworth, M.; Butt, D.; Rudge, W.; Higgs, D.; Majed, A. A systematic review of the treatment of distal humerus fractures in older adults: A comparison of surgical and non-surgical options. Shoulder Elb. 2024, 16, 175–185. [Google Scholar] [CrossRef]
- Githens, M.; Yao, J.; Sox, A.H.; Bishop, J. Open Reduction and Internal Fixation Versus Total Elbow Arthroplasty for the Treatment of Geriatric Distal Humerus Fractures: A Systematic Review and Meta-Analysis. J. Orthop. Trauma 2014, 28, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Lauder, A.; Richard, M.J. Management of distal humerus fractures. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 745–762. [Google Scholar] [CrossRef] [PubMed]
- Aitken, S.A.; Jenkins, P.J.; Rymaszewski, L. Revisiting the ‘bag of bones’: Functional outcome after the conservative management of a fracture of the distal humerus. Bone Jt. J. 2015, 97, 1132–1138. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ‘Low-Plane’ | ‘Non-Low-Plane’ | |
|---|---|---|
| Number of patients | 28 | 13 |
| Age (years) | 75 ± 13 * (41–99) ** | 72 ± 12 * (50–92) ** |
| Male | 7 | 4 |
| Female | 21 | 9 |
| Low-energy trauma | 20 (71%) | 8 (62%) |
| Medium-energy trauma | 8 (29%) | 5 (39%) |
| AO-Classification | ||
| A1 | 0 | 0 |
| A2 | 5 (18%) | 1 (2%) |
| B1 | 1 (2%) | 0 |
| B2 | 2 (5%) | 0 |
| B3 | 1 (2%) | 1 (2%) |
| C1 | 4 (10%) | 0 |
| C2 | 0 | 1 (2%) |
| C3 | 14 (34%) | 10 (24%) |
| Complications | ‘Low-Plane’ | “Non-Low-Plane’ |
|---|---|---|
| Osteosynthesis failure | 3 (10%) | 1 (3%) |
| Ulnar nerve injury | 1 (3%) | - |
| Instability | - | 1 (3%) |
| Soft tissue irritation | 2 (5%) | 1 (3%) |
| Arthrofibrosis | - | 1 (3%) |
| Heterotopic ossification | 1 (3%) | - |
| Failure after olecranon osteotomy | 2 (18%) | 2 (18%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuhn, I.; Goller, S.S.; Böcker, W.; Holzapfel, B.M.; Berthold, D.P.; Gilbert, F.; Boehm, E. ‘Low-Plane’ Fractures of the Distal Humerus in Elderly Patients with Osteoporosis Show High Postoperative Complication Rates. J. Clin. Med. 2024, 13, 6297. https://doi.org/10.3390/jcm13216297
Kuhn I, Goller SS, Böcker W, Holzapfel BM, Berthold DP, Gilbert F, Boehm E. ‘Low-Plane’ Fractures of the Distal Humerus in Elderly Patients with Osteoporosis Show High Postoperative Complication Rates. Journal of Clinical Medicine. 2024; 13(21):6297. https://doi.org/10.3390/jcm13216297
Chicago/Turabian StyleKuhn, Isabella, Sophia S. Goller, Wolfgang Böcker, Boris M. Holzapfel, Daniel P. Berthold, Fabian Gilbert, and Elisabeth Boehm. 2024. "‘Low-Plane’ Fractures of the Distal Humerus in Elderly Patients with Osteoporosis Show High Postoperative Complication Rates" Journal of Clinical Medicine 13, no. 21: 6297. https://doi.org/10.3390/jcm13216297
APA StyleKuhn, I., Goller, S. S., Böcker, W., Holzapfel, B. M., Berthold, D. P., Gilbert, F., & Boehm, E. (2024). ‘Low-Plane’ Fractures of the Distal Humerus in Elderly Patients with Osteoporosis Show High Postoperative Complication Rates. Journal of Clinical Medicine, 13(21), 6297. https://doi.org/10.3390/jcm13216297