
Spontaneous Ventilation Thoracoscopic Lung Biopsy in Undetermined Interstitial Lung Disease: Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Outcome Definition
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis and Statistical Analysis
3. Results
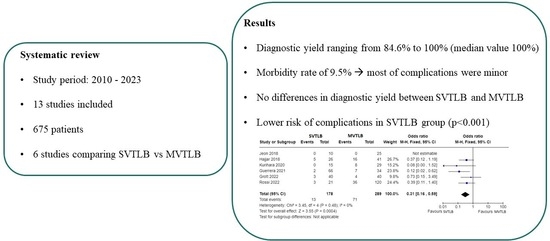
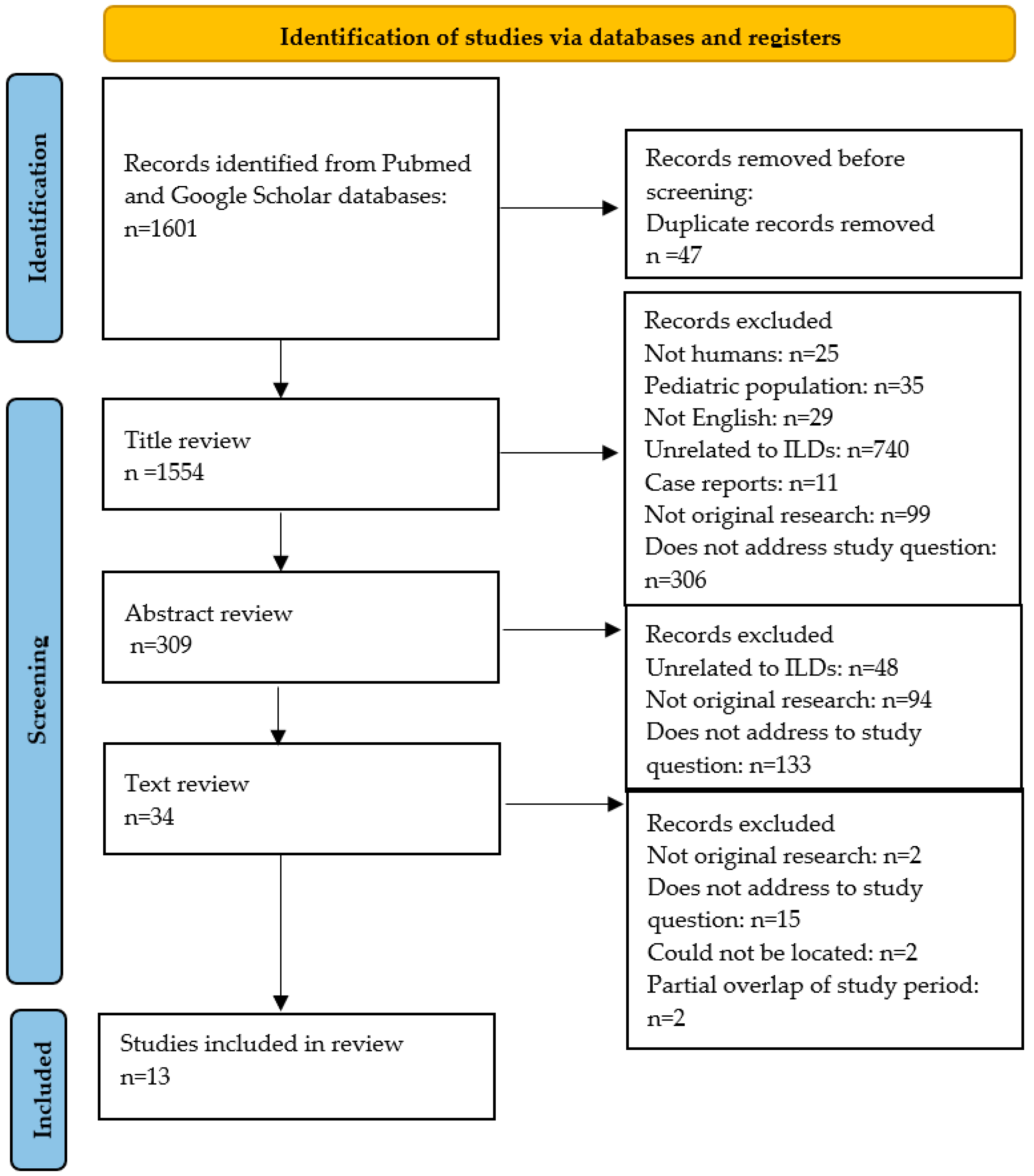
3.1. Study Search and Selection
3.2. Study Characteristics
3.3. Patients’ Characteristics
3.4. Anesthesia and Surgery
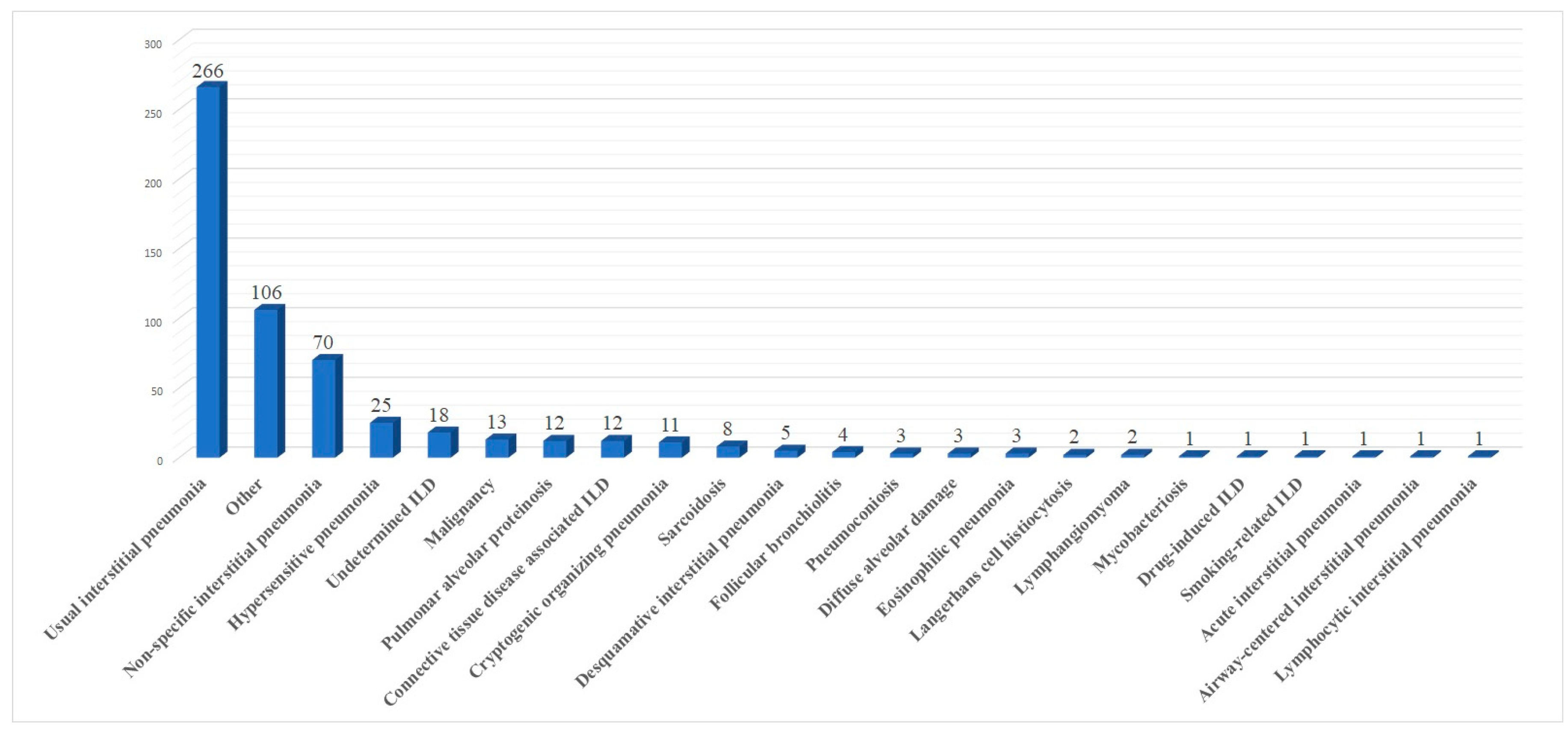
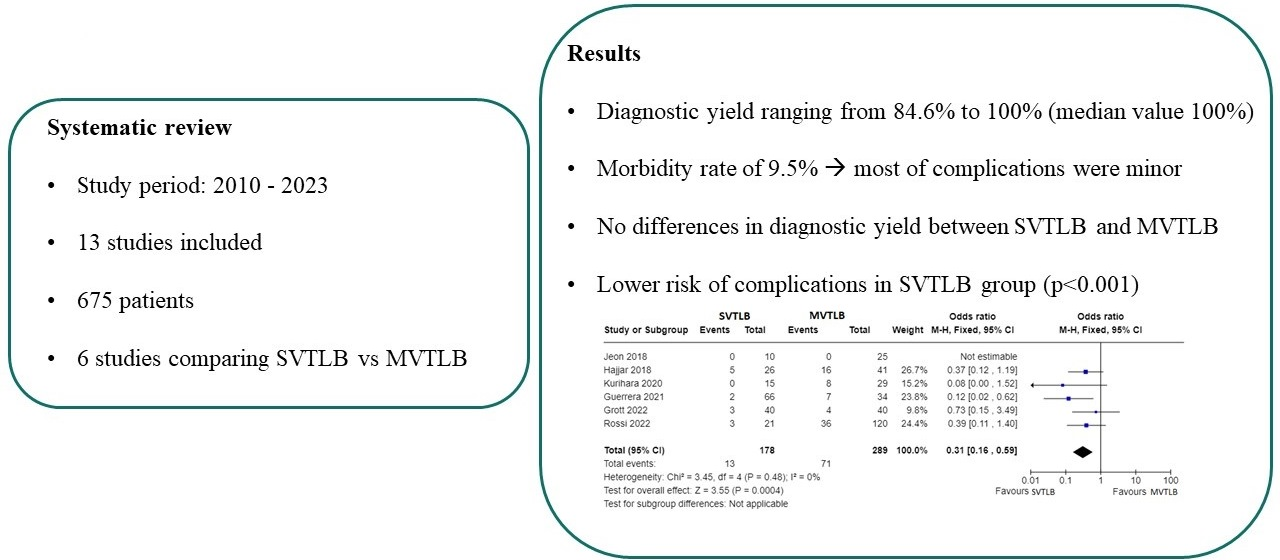
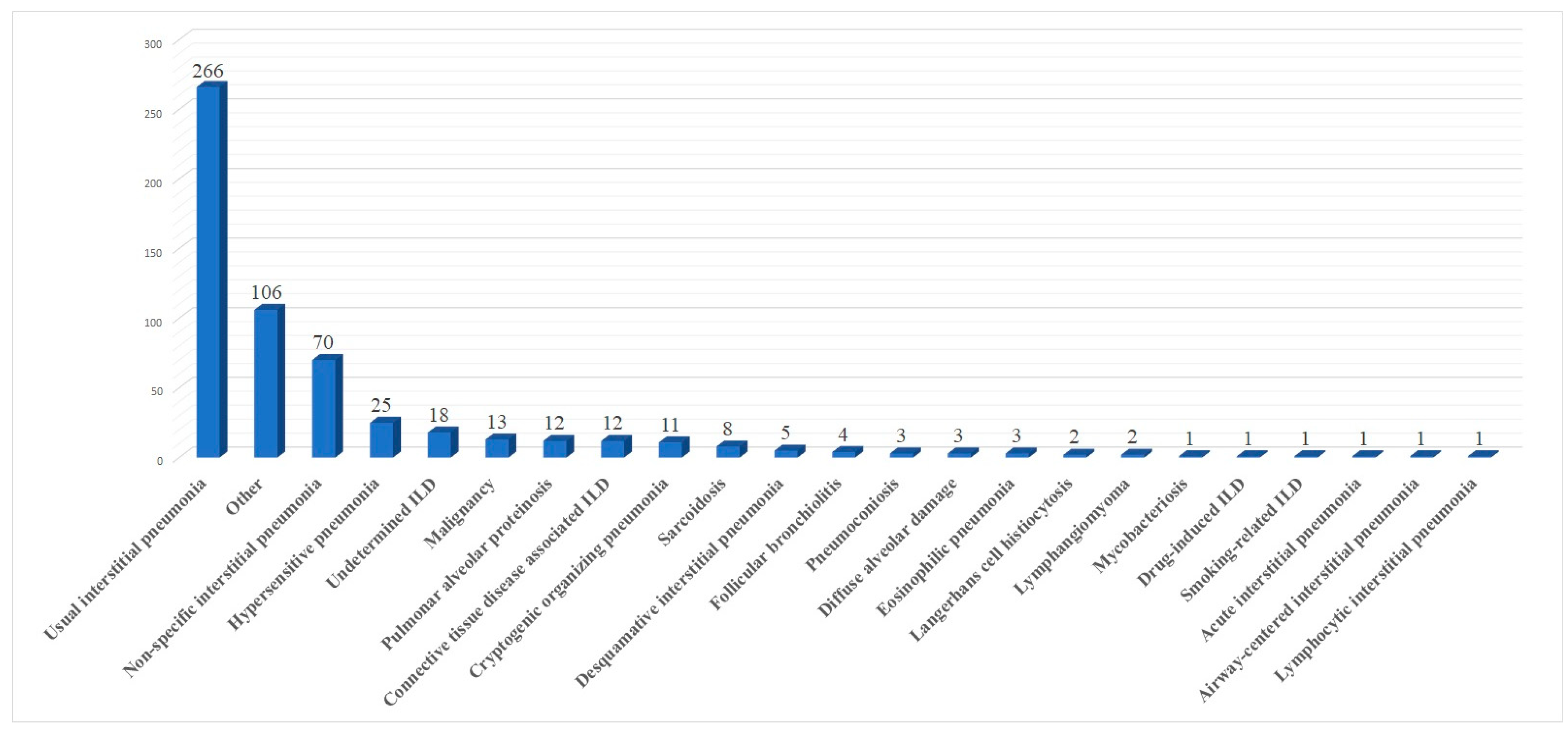
3.5. Histological Results and Diagnostic Yield
3.6. Post-Operative Outcome
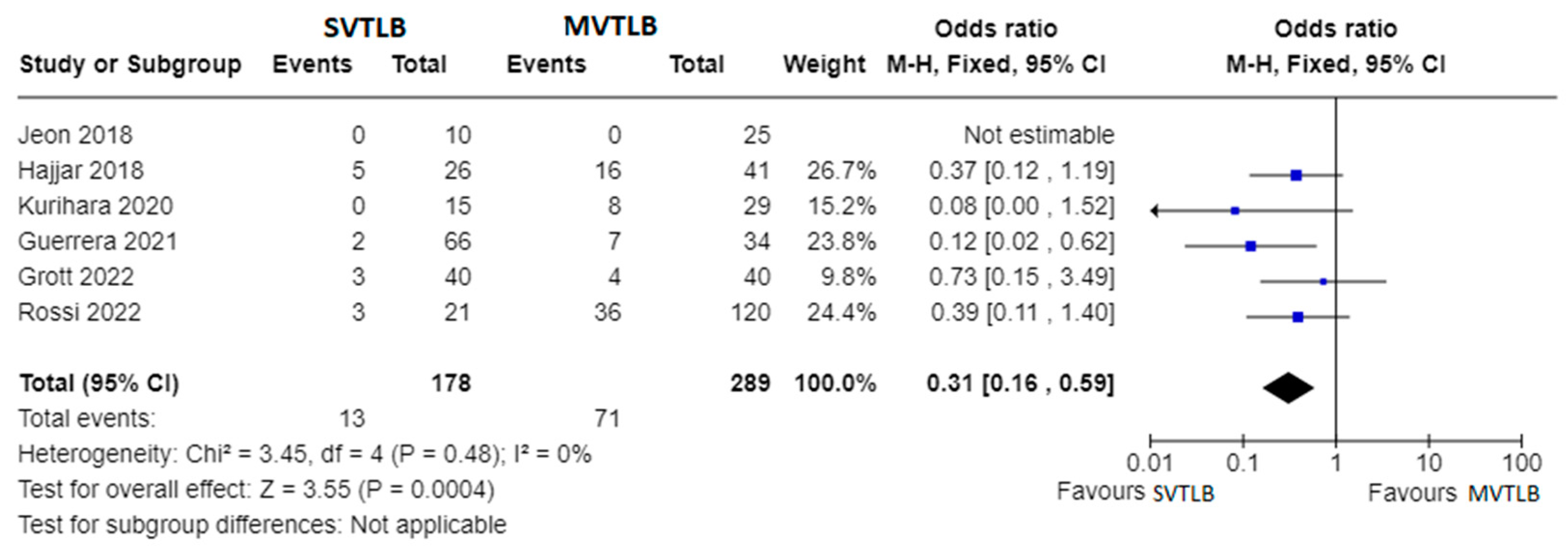
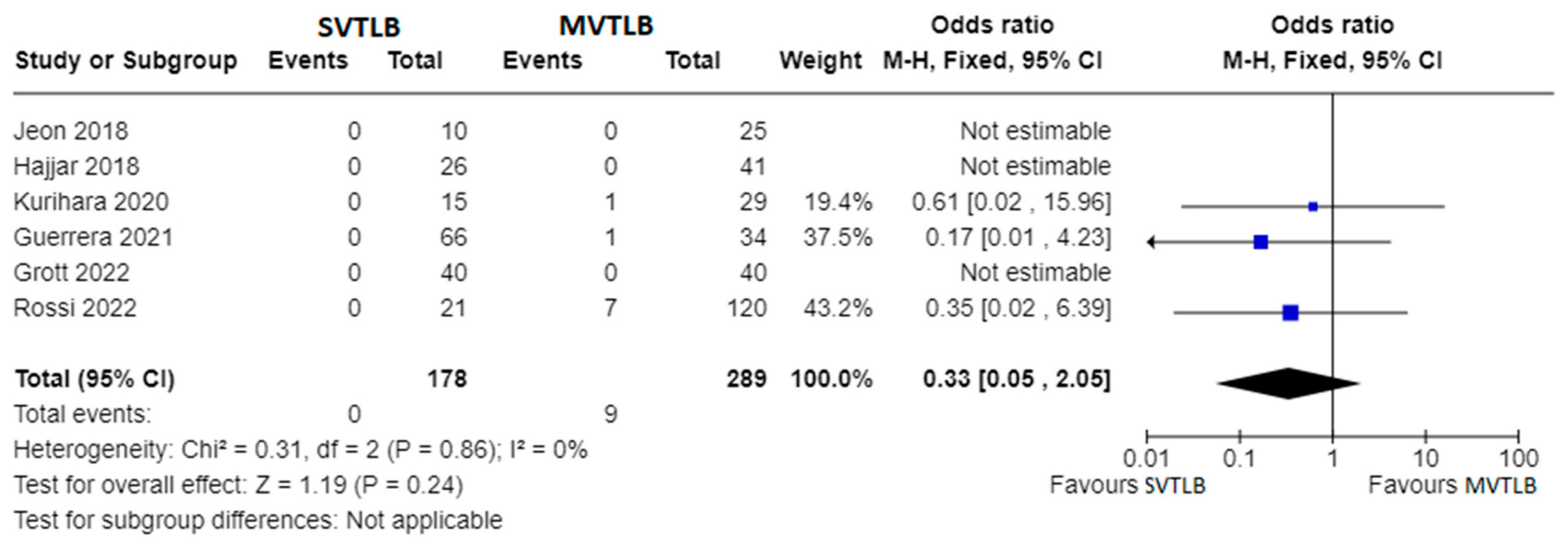
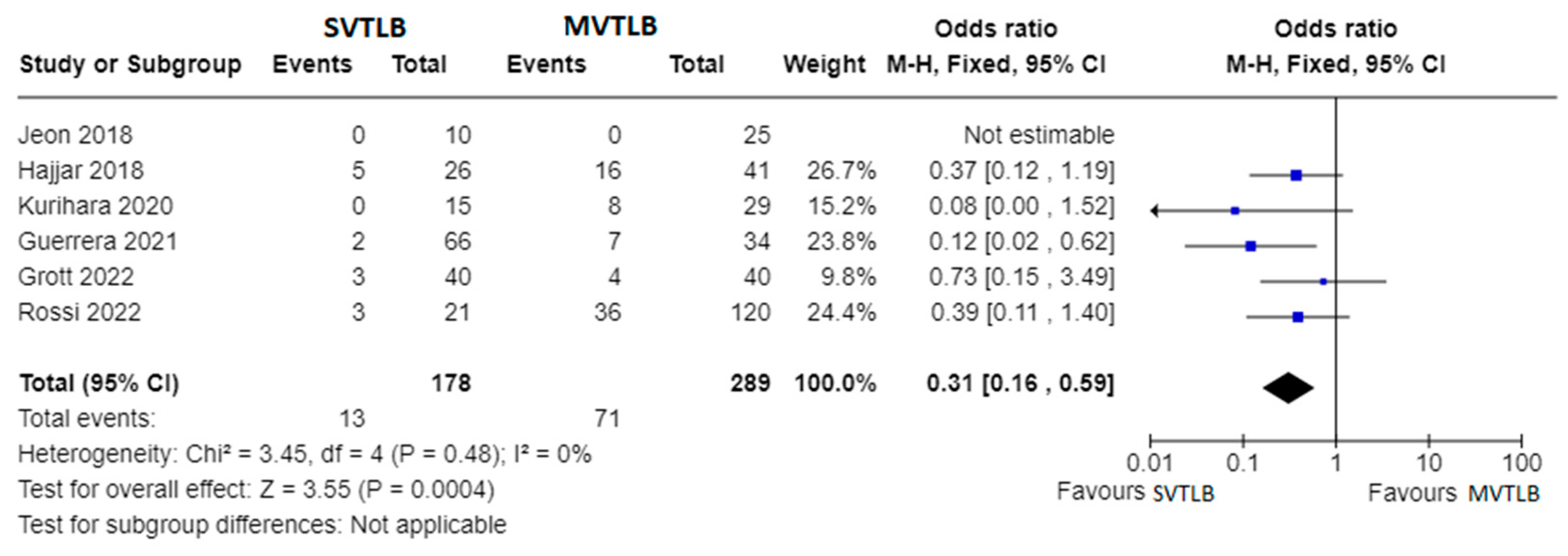
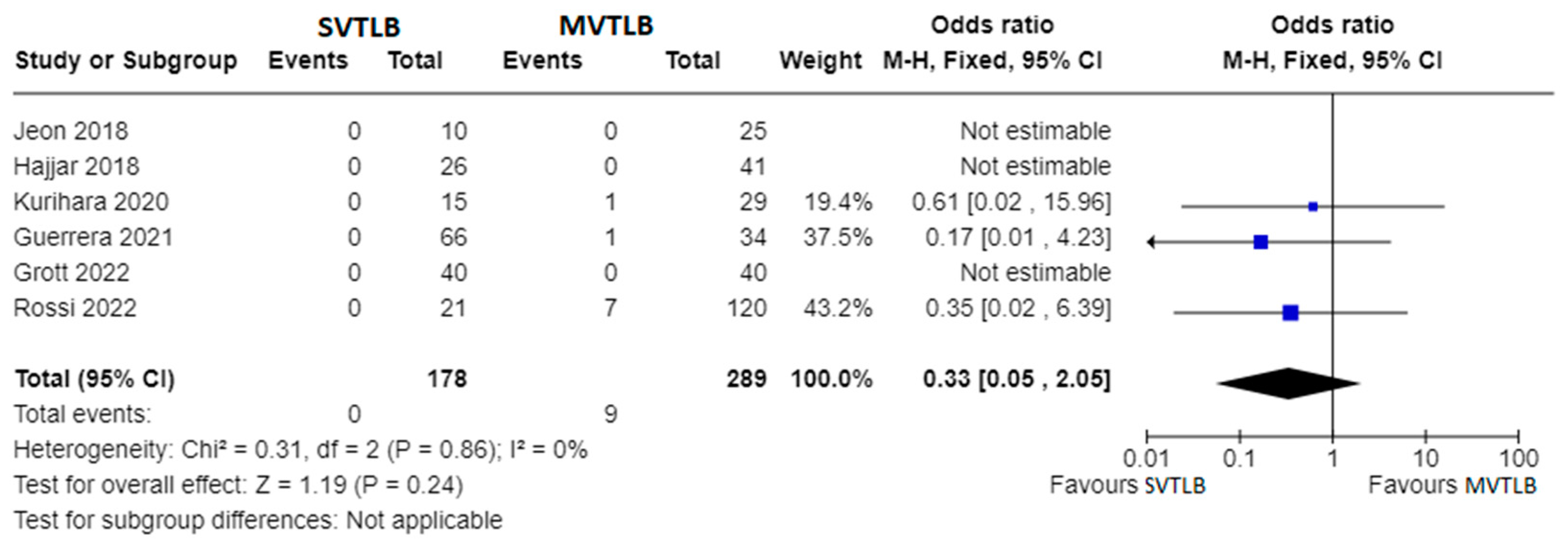
3.7. Comparison between SVTLB and MVTLB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- George, P.M.; Spagnolo, P.; Kreuter, M.; Altinisik, G.; Bonifazi, M.; Martinez, F.J.; Molyneaux, P.L.; Renzoni, E.A.; Richeldi, L.; Tomassetti, S.; et al. Progressive fibrosing interstitial lung disease: Clinical uncertainties, consensus recommendations, and research priorities. Lancet Respir. Med. 2020, 8, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Sharp, M.; Mustafa, A.M.; Farah, N.; Bonham, C.A. Interstitial Lung Disease and Sarcoidosis. Clin. Chest Med. 2023, 44, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Remy-Jardin, M.; Richeldi, L.; Thomson, C.C.; Inoue, Y.; Johkoh, T.; Kreuter, M.; Lynch, D.A.; Maher, T.M.; Martinez, F.J.; et al. Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2022, 205, e18–e47. [Google Scholar] [CrossRef] [PubMed]
- Lentz, R.J.; Argento, A.C.; Colby, T.V.; Rickman, O.B.; Maldonado, F. Transbronchial cryobiopsy for diffuse parenchymal lung disease: A state-of-the-art review of procedural techniques, current evidence, and future challenges. J. Thorac. Dis. 2017, 9, 2186–2203. [Google Scholar] [CrossRef] [PubMed]
- Iftikhar, I.H.; Alghothani, L.; Sardi, A.; Berkowitz, D.; Musani, A.I. Transbronchial Lung Cryobiopsy and Video-assisted Thoracoscopic Lung Biopsy in the Diagnosis of Diffuse Parenchymal Lung Disease. A Meta-analysis of Diagnostic Test Accuracy. Ann. Am. Thorac. Soc. 2017, 14, 1197–1211. [Google Scholar] [CrossRef]
- Han, Q.; Luo, Q.; Xie, J.X.; Wu, L.L.; Liao, L.Y.; Zhang, X.X.; Chen, R.C. Diagnostic yield and postoperative mortality associated with surgical lung biopsy for evaluation of interstitial lung diseases: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2015, 149, 1394–1401.e1. [Google Scholar] [CrossRef] [PubMed]
- Durheim, M.T.; Kim, S.; Gulack, B.C.; Burfeind, W.R.; Gaissert, H.A.; Kosinski, A.S.; Hartwig, M.G. Mortality and Respiratory Failure After Thoracoscopic Lung Biopsy for Interstitial Lung Disease. Ann. Thorac. Surg. 2017, 104, 465–470. [Google Scholar] [CrossRef]
- Sigurdsson, M.I.; Isaksson, H.J.; Gudmundsson, G.; Gudbjartsson, T. Diagnostic surgical lung biopsies for suspected interstitial lung diseases: A retrospective study. Ann. Thorac. Surg. 2009, 88, 227–232. [Google Scholar] [CrossRef]
- Hutchinson, J.P.; McKeever, T.M.; Fogarty, A.W.; Navaratnam, V.; Hubbard, R.B. Surgical lung biopsy for the diagnosis of interstitial lung disease in England: 1997–2008. Eur. Respir. J. 2016, 48, 1453–1461. [Google Scholar] [CrossRef]
- Pompeo, E.; Rogliani, P.; Cristino, B.; Schillaci, O.; Novelli, G.; Saltini, C. Awake thoracoscopic biopsy of interstitial lung disease. Ann. Thorac. Surg. 2013, 95, 445–452. [Google Scholar] [CrossRef]
- Kmet, L.M.; Lee, R.C.; Cook, L.S.; Alberta Heritage Foundation for Medical Research. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Alberta Heritage Foundation for Medical Research: Edmonton, AB, Canada, 2004; Available online: https://www.deslibris.ca/ID/200548 (accessed on 31 December 2023).
- Peng, G.; Liu, M.; Luo, Q.; Chen, H.; Yin, W.; Wang, W.; Huang, J.; Qiu, Y.; Guo, Z.; Liang, L.; et al. Spontaneous ventilation anesthesia combined with uniportal and tubeless thoracoscopic lung biopsy in selected patients with interstitial lung diseases. J. Thorac. Dis. 2017, 9, 4494–4501. [Google Scholar] [CrossRef] [PubMed]
- Jeon, C.S.; Yoon, D.W.; Moon, S.M.; Shin, S.; Cho, J.H.; Lee, S.M.; Ahn, H.J.; Kim, J.A.; Yang, M. Non-intubated video-assisted thoracoscopic lung biopsy for interstitial lung disease: A single-center experience. J. Thorac. Dis. 2018, 10, 3262–3268. [Google Scholar] [CrossRef] [PubMed]
- Pompeo, E.; Rogliani, P.; Atinkaya, C.; Guerrera, F.; Ruffini, E.; Iñiguez-Garcia, M.A.; Peer, M.; Voltolini, L.; Caviezel, C.; Weder, W.; et al. Nonintubated surgical biopsy of undetermined interstitial lung disease: A multicentre outcome analysis. Interact. Cardiovasc. Thorac. Surg. 2019, 28, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Hajjar, W.M.; Al-Nassar, S.A.; Al-Sugair, G.S.; Al-Oqail, A.; Al-Mansour, S.; Al-Haweel, R.; Hajjar, A.W. Evaluation of safety and efficacy of regional anesthesia compared with general anesthesia in thoracoscopic lung biopsy procedure on patient with idiopathic pulmonary fibrosis. Saudi J. Anaesth. 2018, 12, 46–51. [Google Scholar] [CrossRef]
- Kurihara, C.; Tolly, B.; DeWolf, A.; Nader, A.; Kim, S.; Odell, D.D.; Argento, A.C.; Budinger, G.R.S.; Bharat, A. Thoracoscopic lung biopsy under regional anesthesia for interstitial lung disease. Reg. Anesth. Pain. Med. 2020, 45, 255–259. [Google Scholar] [CrossRef]
- Souza, J.M.; Pereira, I.R.P.D.; Borgmann, A.V.; Chiaradia, R.E.; Boscardim, P.C.B. Uniportal surgical biopsy, without orotraqueal intubation, without thoracic drainage in intersticial pulmonary disease: Initial results. Rev. Col. Bras. Cir. 2021, 48, e20202914. [Google Scholar] [CrossRef]
- Guerrera, F.; Costardi, L.; Rosboch, G.L.; Lyberis, P.; Ceraolo, E.; Solidoro, P.; Filippini, C.; Verri, G.; Brazzi, L.; Albera, C.; et al. Awake or intubated surgery in diagnosis of interstitial lung diseases? A prospective study. ERJ Open Res. 2021, 7, 00630–02020. [Google Scholar] [CrossRef]
- Rossi, G.; Spagnolo, P.; Wuyts, W.A.; Ryerson, C.J.; Valli, M.; Valentini, I.; Grani, G.; Gennari, A.; Bizzarro, T.; Lazzari-Agli, L. Pathologic comparison of conventional video-assisted thoracic surgical (VATS) biopsy versus non-intubated/“awake” biopsy in fibrosing interstitial lung diseases. Respir. Med. 2022, 195, 106777. [Google Scholar] [CrossRef]
- Zhang, L.; Xie, T.; Li, Y.; Zhang, B.; Fu, Y.; Ding, Y.; Wu, H. Diagnostic value and safety of medical thoracoscopy under local anesthesia for unexplained diffuse interstitial lung disease: A retrospective study. Chron. Respir. Dis. 2022, 19, 14799731221133389. [Google Scholar] [CrossRef]
- Cherchi, R.; Ferrari, P.A.; Guerrera, F.; Grimaldi, G.; Pinna-Susnik, M.; Murenu, A.; Rosboch, G.L.; Lybéris, P.; Ibba, F.; Balsamo, L.; et al. Lung Biopsy With a Non-intubated VATS Approach in an Obese Population: Indications and Results. Front. Surg. 2022, 9, 829976. [Google Scholar] [CrossRef]
- Katgi, N.; Çimen, P.; Çirak, A.K.; Şimşek, T.; Ceylan, K.C.; Samancilar, Ö.; Duman, E.; Erer, O.F.; Tuksavul, F.F. Complication and cost analysis of transbronchial lung cryobiopsy and awake video-assisted thoracic surgery in diagnosis of interstitial lung disease. Sarcoidosis Vasc. Diffuse Lung Dis. 2022, 39, e2022005. [Google Scholar] [CrossRef] [PubMed]
- Grott, M.; Wimmer, C.D.; Kreuter, M.; Prasse, A.; Eichhorn, M.E.; Eichhorn, F.; Herth, F.J.F.; Seeliger, B.; Kriegsmann, K.; Schmidt, W.; et al. Surgical Lung Biopsy for Interstitial Lung Disease: A Two Center Propensity Score Matching Analysis. Respiration 2022, 101, 910–917. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Lettieri, C.J.; Veerappan, G.R.; Helman, D.L.; Mulligan, C.R.; Shorr, A.F. Outcomes and safety of surgical lung biopsy for interstitial lung disease. Chest 2005, 127, 1600–1605. [Google Scholar] [CrossRef] [PubMed]
- Cilli, A.; Kocaturk, C.; Tertemiz, K.C.; Kalafat, C.E.; Hanta, I.; Odemis, A.; Sevinc, C.; Dertsiz, L.; Akanil Fener, N. Morbidity and mortality of surgical lung biopsy in the diagnosis of usual interstitial pneumonia. ANZ J. Surg. 2021, 91, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Pastre, J.; Khandhar, S.; Barnett, S.; Ksovreli, I.; Mani, H.; Brown, A.W.; Shlobin, O.A.; Ahmad, K.; Khangoora, V.; Aryal, S.; et al. Surgical Lung Biopsy for Interstitial Lung Disease. Safety and Feasibility at a Tertiary Referral Center. Ann. Am. Thorac. Soc. 2021, 18, 460–467. [Google Scholar] [CrossRef]
- Rodrigues, I.; Estêvão Gomes, R.; Coutinho, L.M.; Rego, M.T.; Machado, F.; Morais, A.; Novais Bastos, H. Diagnostic yield and safety of transbronchial lung cryobiopsy and surgical lung biopsy in interstitial lung diseases: A systematic review and meta-analysis. Eur. Respir. Rev. 2022, 31, 210280. [Google Scholar] [CrossRef]
- Wen, Y.; Liang, H.; Qiu, G.; Liu, Z.; Liu, J.; Ying, W.; Liang, W.; He, J. Non-intubated spontaneous ventilation in video-assisted thoracoscopic surgery: A meta-analysis. Eur. J. Cardiothorac. Surg. 2020, 57, 428–437. [Google Scholar] [CrossRef]
- Marini, J.J.; Rocco, P.R.M.; Gattinoni, L. Static and Dynamic Contributors to Ventilator-induced Lung Injury in Clinical Practice. Pressure, Energy, and Power. Am. J. Respir. Crit. Care Med. 2020, 201, 767–774. [Google Scholar] [CrossRef]
- Kubota, T.; Miyata, A. Postoperative respiratory failure caused by acute exacerbation of idiopathic interstitial pneumonia. J. Anesth. 2011, 25, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Collard, H.R.; Ryerson, C.J.; Corte, T.J.; Jenkins, G.; Kondoh, Y.; Lederer, D.J.; Lee, J.S.; Maher, T.M.; Wells, A.U.; Antoniou, K.M.; et al. Acute Exacerbation of Idiopathic Pulmonary Fibrosis. An International Working Group Report. Am. J. Respir. Crit. Care Med. 2016, 194, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Tacconi, F.; Pompeo, E. Non-intubated video-assisted thoracic surgery: Where does evidence stand? J. Thorac. Dis. 2016, 8 (Suppl. S4), S364–S375. [Google Scholar] [CrossRef] [PubMed]
- Pompeo, E.; Rogliani, P.; Tacconi, F.; Dauri, M.; Saltini, C.; Novelli, G.; Mineo, T.C.; Awake Thoracic Surgery Research Group. Randomized comparison of awake nonresectional versus nonawake resectional lung volume reduction surgery. J. Thorac. Cardiovasc. Surg. 2012, 143, 47–54.e1. [Google Scholar] [CrossRef]
- Troy, L.K.; Grainge, C.; Corte, T.J.; Williamson, J.P.; Vallely, M.P.; Cooper, W.A.; Mahar, A.; Myers, J.L.; Lai, S.; Mulyadi, E.; et al. Diagnostic accuracy of transbronchial lung cryobiopsy for interstitial lung disease diagnosis (COLDICE): A prospective, comparative study. Lancet Respir. Med. 2020, 8, 171–181. [Google Scholar] [CrossRef]
- Ravaglia, C.; Bonifazi, M.; Wells, A.U.; Tomassetti, S.; Gurioli, C.; Piciucchi, S.; Dubini, A.; Tantalocco, P.; Sanna, S.; Negri, E.; et al. Safety and Diagnostic Yield of Transbronchial Lung Cryobiopsy in Diffuse Parenchymal Lung Diseases: A Comparative Study versus Video-Assisted Thoracoscopic Lung Biopsy and a Systematic Review of the Literature. Respiration 2016, 91, 215–227. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Study Type | Study Period | N. of Patients | Age | Male/Female | Diagnostic Yield | Conversion to Mechanical Ventilation Rate | Post-Operative Complication | Comparison with MVTLB | N. Patient Control Group |
|---|---|---|---|---|---|---|---|---|---|---|
| Pompeo, 2013 [10] | Prospective | Dec 2009–Jan 2012 | 30 | 62.0 ± 10.0 | 15/15 | 97.0% | 0.0% | 1/30 (3.3%) | No | - |
| Peng, 2017 [12] | Retrospective | Jan 2014–May 2015 | 43 | 49.6 ± 10.7 | 23/20 | 88.4% | 0.0% | 3/43 (7.0%) | No | - |
| Jeon, 2018 [13] | Retrospective | Jan 2016–June 2016 | 10 | 61.2 ± 6.6 | 6/4 | 100.0% | 0.0% | 0/10 (0.0%) | Yes | 25 |
| Pompeo, 2018 [14] | Retrospective | Jun 2017–Nov 217 | 112 | 60.0 ± 12.0 | 65/47 | 96.0% | 4.5% | 8/112 (7.1%) | No | - |
| Hajjari, 2018 [15] | Retrospective | Jan 2008–Dec 2015 | 26 | NR | NR | NR | 0.0% | 5/26 (19.2%) | Yes | 41 |
| Kurihara, 2020 [16] | Prospective | Mar 2016–Mar 2018 | 15 | 62.8 ± 14.7 | 7/8 | 100.0% | 0.0% | 0/15 (0.0%) | Yes | 29 |
| Souza, 2021 [17] | Retrospective | Jan 2019–Jan 2020 | 14 | 65.8 # | 7/7 | 100.0% | 0.0% | 2/14 (14.2%) | No | - |
| Guerrera, 2021 [18] | Prospective | Jun 2016–Feb 2020 | 66 | 60.4 ± 2.0 | 42/24 | 100.0% | 0.0% | 2/66 (3.0%) | Yes | 34 |
| Rossi, 2022 [19] | Retrospective | Jan 2018–Dec 2020 | 21 | 69.5 # | 6/15 | 100.0% | 0.0% | 3/21 (14.0%) | Yes | 120 |
| Zhang, 2022 [20] | Retrospective | Jan 2015–Jul 2021 | 52 | 53.6 ± 15.2 | 25/27 | 84.6% | 0.0% | 3/52/5.8%) | No | - |
| Cherchi, 2022 [21] | Retrospective | Apr 2015–Nov 2021 | 202 | 67.4 (60.0–73.5) * | 142/60 | 99.0% | 0.0% | 22/202 (10.9%) | No | - |
| Katgi, 2022 [22] | Retrospective | 2015–2020 | 44 | 56.3 ± 12.6 | 20/24 | 100.0% | 0.0% | 12/44 (27.3%) | No | - |
| Grott, 2022 [23] | Retrospective | Feb 2013–Apr 2021 | 40 | 62.3 ± 10.7 | 30/10 | 100.0% | 0.0% | 3/40 (7.5%) | Yes | 40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patirelis, A.; Elia, S.; Cristino, B.; Puxeddu, E.; Cavalli, F.; Rogliani, P.; Pompeo, E. Spontaneous Ventilation Thoracoscopic Lung Biopsy in Undetermined Interstitial Lung Disease: Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 374. https://doi.org/10.3390/jcm13020374
Patirelis A, Elia S, Cristino B, Puxeddu E, Cavalli F, Rogliani P, Pompeo E. Spontaneous Ventilation Thoracoscopic Lung Biopsy in Undetermined Interstitial Lung Disease: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(2):374. https://doi.org/10.3390/jcm13020374
Chicago/Turabian StylePatirelis, Alexandro, Stefano Elia, Benedetto Cristino, Ermanno Puxeddu, Francesco Cavalli, Paola Rogliani, and Eugenio Pompeo. 2024. "Spontaneous Ventilation Thoracoscopic Lung Biopsy in Undetermined Interstitial Lung Disease: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 2: 374. https://doi.org/10.3390/jcm13020374
APA StylePatirelis, A., Elia, S., Cristino, B., Puxeddu, E., Cavalli, F., Rogliani, P., & Pompeo, E. (2024). Spontaneous Ventilation Thoracoscopic Lung Biopsy in Undetermined Interstitial Lung Disease: Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(2), 374. https://doi.org/10.3390/jcm13020374