
Preliminary Data on SNP of Transplantation-Related Genes after Haploidentical Stem Cell Transplantation

 , ,
, ,
Abstract

1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Assessment of the Outcomes after Haplo-HSCT
2.3. Selection of Candidate SNPs
2.4. Sample Collection and SNP Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Clinical Outcomes of Patients Receiving Haplo-HSCT
3.3. Association of Recipient Genotypes with the Outcomes of Patients Receiving Haplo-HSCT
3.4. Association of Donor Genotypes with the Outcomes of Patients Receiving Haplo-HSCT
3.5. Association of Mismatch between Donor and Recipient Genotypes with the Outcomes of Patients Receiving Haplo-HSCT
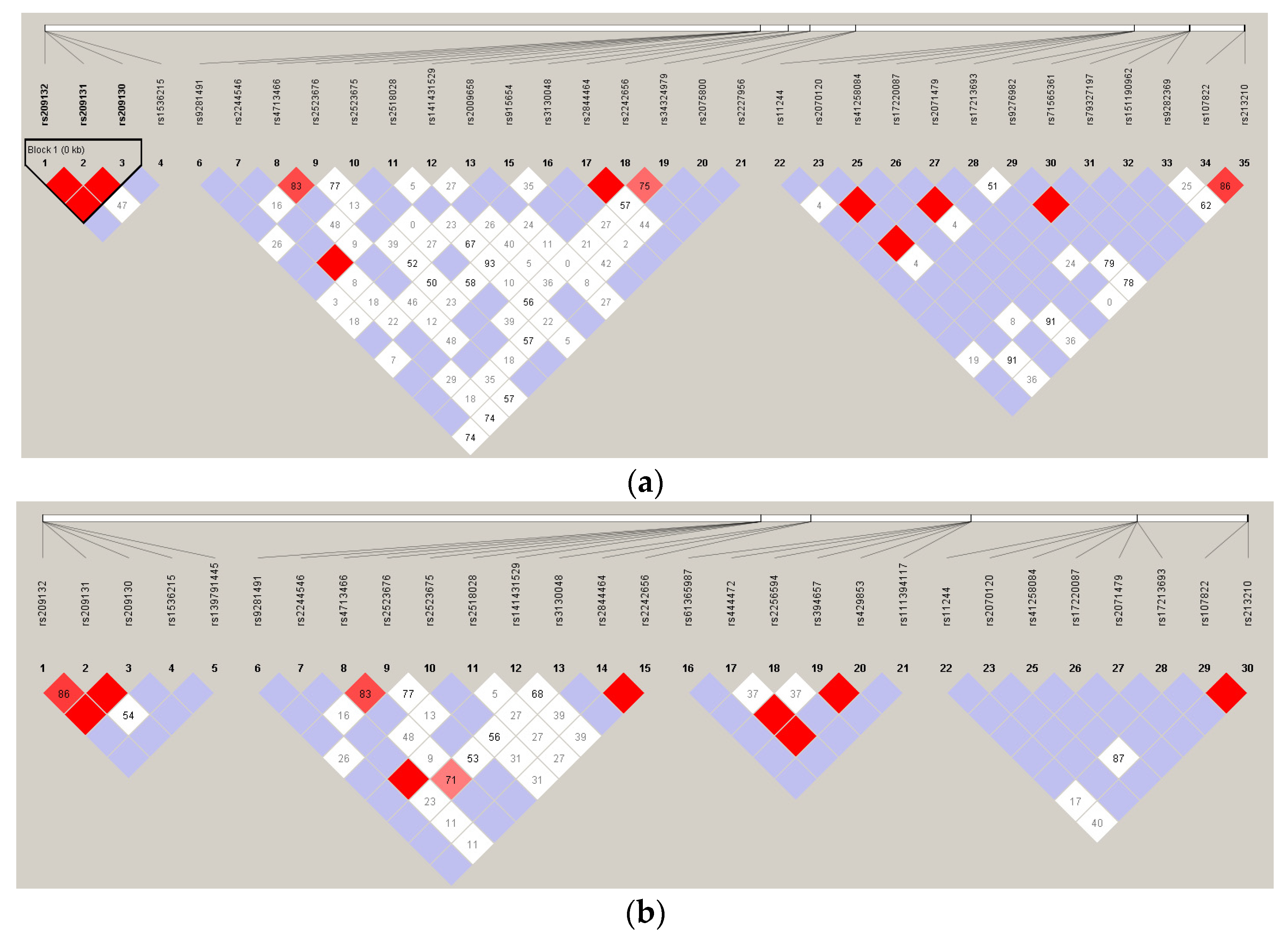
3.6. Linkage Disequilibrium Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Khaddour, K.; Hana, C.K.; Mewawalla, P. Hematopoietic Stem Cell Transplantation. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK536951/ (accessed on 15 September 2023).
- Petersdorf, E.W. Genetics of graft-versus-host disease: The major histocompatibility complex. Blood Rev. 2013, 27, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, E.R. How important is histocompatibility in bone marrow transplantation? Bone Marrow Transplant. 1989, 4, 439–444. [Google Scholar] [PubMed]
- Besse, K.; Maiers, M.; Confer, D.; Albrecht, M. On modeling human leukocyte antigen–identical sibling match probability for allogeneic hematopoietic cell transplantation: Estimating the need for an unrelated donor source. Biol. Blood Marrow Transpl. 2015, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, D.E.; Zachary, A.; Fuchs, E.J.; Luznik, L.; Kasamon, Y.L.; Jones, R.J.; Leffell, M.S. Desensitization for mismatched hematopoietic stem cell transplantation (HSCT). Blood 2011, 118, 1955. [Google Scholar] [CrossRef]
- Reisner, Y.; Bachar-Lustig, E.; Li, H.W.; Aversa, F.; Velardi, A.; Martelli, M.F. The role of megadose CD34+ progenitor cells in the treatment of leukemia patients without a matched donor and in tolerance induction for organ transplantation. Ann. N. Y. Acad. Sci. 1999, 872, 336–348, discussion 348–350. [Google Scholar] [CrossRef] [PubMed]
- Wieduwilt, M.J.; Metheny, I.I.I.L.; Zhang, M.J.; Wang, H.L.; Estrada-Merly, N.; Marks, D.I.; Al-Homsi, A.S.; Muffly, L.; Chao, N.; Rizzieri, D.; et al. Haploidentical vs sibling, unrelated, or cord blood hematopoietic cell transplantation for acute lymphoblastic leukemia. Blood Adv. 2022, 6, 339–357. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Tian, Z. Which is better, HLA-matched sibling or haploidentical transplantation? Cell. Mol. Immunol. 2021, 18, 1347. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.P.; Chang, S.W.; Wang, P.N.; Hus, F.P.; Tseng, C.P. Association between single nucleotide polymorphisms within HLA region and disease relapse for patients with hematopoietic stem cell transplantation. Sci. Rep. 2019, 9, 13731. [Google Scholar] [CrossRef]
- Chen, D.P.; Wen, Y.H.; Wang, P.N.; Hour, A.L.; Lin, W.T.; Hsu, F.P.; Wang, W.T. The adverse events of haematopoietic stem cell transplantation are associated with gene polymorphism within human leukocyte antigen region. Sci. Rep. 2021, 11, 1475. [Google Scholar] [CrossRef]
- Chen, D.P.; Chang, S.W.; Wang, P.N.; Lin, W.T.; Hsu, F.P.; Wang, W.T.; Tseng, C.P. The association between single-nucleotide polymorphisms of co-stimulatory genes within non-HLA region and the prognosis of leukemia patients with hematopoietic stem cell transplantation. Front. Immunol. 2021, 12, 730507. [Google Scholar] [CrossRef]
- Symons, H.J.; Leffell, M.S.; Rossiter, N.D.; Zahurak, M.; Jones, R.J.; Fuchs, E.J. Improved survival with inhibitory killer immunoglobulin receptor (KIR) gene mismatches and KIR haplotype B donors after nonmyeloablative, HLA-haploidentical bone marrow transplantation. Biol. Blood Marrow Transpl. 2010, 16, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Dubreuil, L.; Chevallier, P.; Retière, C.; Gagne, K. Relevance of Polymorphic KIR and HLA Class I Genes in NK-Cell-Based Immunotherapies for Adult Leukemic Patients. Cancers 2021, 13, 3767. [Google Scholar] [CrossRef] [PubMed]
- Dhuyser, A.; Aarnink, A.; Pérès, M.; Jayaraman, J.; Nemat-Gorgani, N.; Rubio, M.T.; Trowsdale, J.; Traherne, J. KIR in allogeneic hematopoietic stem cell transplantation: Need for a unified paradigm for donor selection. Front. Immunol. 2022, 13, 821533. [Google Scholar] [CrossRef] [PubMed]
- Schoemans, H.M.; Lee, S.J.; Ferrara, J.L.; Wolff, D.; Levine, J.E.; Schultz, K.R.; Shaw, B.E.; Flowers, M.E.; Ruutu, T.; Greinix, H.; et al. EBMT-NIH-CIBMTR Task Force position statement on standardized terminology & guidance for graft-versus-host disease assessment. Bone Marrow Transpl. 2018, 53, 1401–1415. [Google Scholar] [CrossRef]
- Justiz Vaillant, A.A.; Modi, P.; Mohammadi, O. Graft-Versus-Host Disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538235/ (accessed on 15 September 2023).
- Mo, X.D.; Zhang, X.H.; Xu, L.P.; Wang, Y.; Yan, C.H.; Chen, H.; Chen, Y.H.; Han, W.; Wang, F.R.; Wang, J.Z.; et al. Haploidentical hematopoietic stem cell transplantation for myelodysplastic syndrome. Biol. Blood Marrow Transpl. 2017, 23, 2143–2150. [Google Scholar] [CrossRef] [PubMed]
- Petersdorf, E.W.; Malkki, M.; Horowitz, M.M.; Spellman, S.R.; Haagenson, M.D.; Wang, T. Mapping MHC haplotype effects in unrelated donor hematopoietic cell transplantation. Blood 2013, 121, 1896–1905. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of LD and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, S.B.; Schaffner, S.F.; Nguyen, H.; Moore, J.M.; Roy, J.; Blumenstiel, B.; Higgins, J.; DeFelice, M.; Lochner, A.; Faggart, M.; et al. The structure of haplotype blocks in the human genome. Science 2002, 296, 2225–2229. [Google Scholar] [CrossRef] [PubMed]
- Van Coillie, S.; Wiernicki, B.; Xu, J. Molecular and cellular functions of CTLA-4. Adv. Exp. Med. Biol. 2020, 1248, 7–32. [Google Scholar] [CrossRef]
- Wu, J.; Tang, J.L.; Wu, S.J.; Lio, H.Y.; Yang, Y.C. Functional polymorphism of CTLA-4 and ICOS genes in allogeneic hematopoietic stem cell transplantation. Clin. Chim. Acta 2009, 403, 229–233. [Google Scholar] [CrossRef]
- Sinnett, D.; Beaulieu, P.; Bélanger, H.; Lefebvre, J.F.; Langlois, S.; Théberge, M.C.; Drouin, S.; Zotti, C.; Hudson, T.J.; Labuda, D. Detection and characterization of DNA variants in the promoter regions of hundreds of human disease candidate genes. Genomics 2006, 87, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Deng, N.; Zhou, H.; Fan, H.; Yuan, Y. Single nucleotide polymorphisms and cancer susceptibility. Oncotarget 2017, 8, 110635–110649. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.T.; Pai, A.A.; Pickrell, J.K.; Gaffney, D.J.; Pique-Regi, R.; Degner, J.F.; Gilad, Y.; Pritchard, J.K. DNA methylation patterns associate with genetic and gene expression variation in HapMap cell lines. Genome Biol. 2011, 12, R10. [Google Scholar] [CrossRef]
- Chen, D.P.; Lin, W.T.; Wen, Y.H.; Wang, W.T. Investigation of the correlation between immune thrombocytopenia and T cell activity-regulated gene polymorphism using functional study. Sci. Rep. 2022, 12, 6601. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.Y.; Wang, Y.; Li, G.X.; Qin, Y.Z.; Wang, F.R.; Xu, L.P.; Chen, H.; Han, W.; Wang, J.Z.; Zhang, X.H.; et al. CTLA-4 polymorphisms and haplotype correlate with survival in ALL after allogeneic stem cell transplantation from related HLA-haplotype-mismatched donor. J. Transl. Med. 2016, 14, 100. [Google Scholar] [CrossRef]
- Santos, N.; Rodríguez-Romanos, R.; De La Cámara, R.; Brunet, S.; Nieto, J.B.; Buño, I.; Martínez, C.; Jiménez-Velasco, A.; Vallejo, C.; González, M.; et al. PD-1 genotype of the donor is associated with acute graft-versus-host disease after HLA-identical sibling donor stem cell transplantation. Ann. Hematol. 2018, 97, 2217–2224. [Google Scholar] [CrossRef] [PubMed]
- Cruz, D.; Rodríguez-Romanos, R.; Gonzalez-Bartulos, M.; García-Cadenas, I.; de la Camara, R.; Heras, I.; Buño, I.; Santos, N.; Lloveras, N.; Velarde, P.; et al. LAG3 genotype of the donor and clinical outcome after allogeneic transplantation from HLA-identical sibling donors. Front. Immunol. 2023, 14, 1066393. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhong, W.; Hinrichs, D.; Wu, X.; Weinberg, A.; Hall, M.; Spencer, D.; Wegmann, K.; Rosenbaum, J.T. Activation of OX40 augments Th17 cytokine expression and antigen-specific uveitis. Am. J. Pathol. 2010, 177, 2912–2920. [Google Scholar] [CrossRef] [PubMed]
- Bossini-Castillo, L.; Broen, J.C.; Simeon, C.P.; Beretta, L.; Vonk, M.C.; Ortego-Centeno, N.; Espinosa, G.; Carreira, P.; Camps, M.T.; Navarrete, N.; et al. A replication study confirms the association of TNFSF4 (OX40L) polymorphisms with systemic sclerosis in a large European cohort. Ann. Rheum. Dis. 2011, 70, 638–641. [Google Scholar] [CrossRef]
- Nordmark, G.; Kristjansdottir, G.; Theander, E.; Appel, S.; Eriksson, P.; Vasaitis, L.; Kvarnström, M.; Delaleu, N.; Lundmark, P.; Lundmark, A.; et al. Association of EBF1, FAM167A(C8orf13)-BLK and TNFSF4 gene variants with primary Sjögren’s. Genes Immun. 2011, 12, 100–109. [Google Scholar] [CrossRef]
- Shen, Y.; Liu, Y.; Wang, X.; Ke, X.; Kang, H.; Hong, S. Association between TNFSF4 and BLK gene polymorphisms and susceptibility to allergic rhinitis. Mol. Med. Rep. 2017, 16, 3224–3232. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.P.; Wen, Y.H.; Wang, W.T.; Lin, W.T. Exploring the bio-functional effect of single nucleotide polymorphisms in the promoter region of the TNFSF4, CD28, and PDCD1 genes. J. Clin. Med. 2023, 12, 2157. [Google Scholar] [CrossRef] [PubMed]
- Kulski, J.K. Long noncoding RNA HCP5, a hybrid HLA class I endogenous retroviral gene: Structure, expression, and disease associations. Cells 2019, 8, 480. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, Z.; Leng, K.; Xu, Y.; Ji, D.; Huang, L.; Cui, Y.; Jiang, X. ZEB 1-AS 1: A crucial cancer-related long non-coding RNA. Cell Prolif. 2018, 51, e12423. [Google Scholar] [CrossRef] [PubMed]
- Cotton, T.R.; Lechtenberg, B.C. Chain reactions: Molecular mechanisms of RBR ubiquitin ligases. Biochem. Soc. Trans. 2020, 48, 1737–1750. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Tang, Y.D.; Zhai, J.; Zheng, C. The RING finger protein family in health and disease. Signal Transduct. Target. Ther. 2022, 7, 300. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.P.; Chang, S.W.; Jaing, T.H.; Wang, W.T.; Hsu, F.P.; Tseng, C.P. Single nucleotide polymorphisms within HLA region are associated with the outcomes of unrelated cord blood transplantation. Sci. Rep. 2021, 11, 21925. [Google Scholar] [CrossRef] [PubMed]
- GeneCards. The Human Gene Database: HLA-DOA Gene—Major Histocompatibility Complex, Class II, DO Alpha. 2023. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=HLA-DOA (accessed on 17 May 2023).
- Courtney, A.H.; Lo, W.L.; Weiss, A. TCR signaling: Mechanisms of initiation and propagation. Trends Biochem. Sci. 2018, 43, 108–123. [Google Scholar] [CrossRef] [PubMed]
- Vaeth, M.; Feske, S. NFAT control of immune function: New Frontiers for an Abiding Trooper. F1000Res 2018, 7, 260. [Google Scholar] [CrossRef]
- Huang, T.; Shu, Y.; Cai, Y.D. Genetic differences among ethnic groups. BMC Genom. 2015, 16, 1093. [Google Scholar] [CrossRef]
- Mirgayazova, R.; Khadiullina, R.; Chasov, V.; Mingaleeva, R.; Miftakhova, R.; Rizvanov, A.; Bulatov, E. Therapeutic editing of the TP53 gene: Is CRISPR/Cas9 an option? Genes 2020, 11, 704. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Gene | Source | Candidate SNPs under Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| HCP5 | Donor | rs9281491 | rs2244546 | rs4713466 | rs2523676 | rs2523675 | rs2518028 | rs1414315 |
| NOTCH4 | Donor | rs111394117 | rs429853 | rs394657 | rs2256594 | rs444472 | rs61365987 | |
| HLA-DOA | Recipient | rs9276982 | rs71565361 | rs79327197 | rs151190962 | rs9282369 | ||
| LTA | Recipient | rs2009658 | rs736160 | rs915654 | ||||
| HSPA1L | Recipient | rs34324979 | rs2075800 | rs2227956 | ||||
| BAG6 | Mismatch | rs3130048 | rs2844464 | rs2242656 | ||||
| RING1 | Mismatch | rs107822 | rs213210 | |||||
| TRIM27 | Mismatch | rs209132 | rs209131 | rs209130 | rs1536215 | rs139791445 | ||
| HLA-DOB | Mismatch | rs11244 | rs2070120 | rs56150445 | rs41258084 | rs17220087 | rs2071479 | rs17213693 |
| Gene | Genomic Region | Candidate SNP under Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| CTLA4 | Promoter | rs11571315 | rs733618 | rs4553808 | rs11571316 | rs62182595 | rs573554201 | rs16840252 |
| rs945677329 | rs5742909 | |||||||
| Exon 1 | rs231775 | |||||||
| Exon 4 | rs56102377 | rs56217811 | rs55696217 | |||||
| 3′-UTR | rs231721 | rs778932058 | rs3087243 | rs11571319 | ||||
| TNFSF4 | Promoter | rs1234314 | rs45454293 | rs181758110 | ||||
| CD28 | Promoter | rs1879877 | rs3181096 | rs3181097 | rs3181098 | rs28718975 | rs28688913 | rs28541784 |
| rs201801072 | rs200353921 | |||||||
| PDCD1 | Promoter | rs5839828 | rs36084323 | |||||
| Intron 4 | rs41386349 | rs6705653 | ||||||
| Exon 5 | rs2227982 | |||||||
| Gene | Primer Sequences a | PCR Program |
|---|---|---|
| CD28 | F: 5′-GGGTGGTAAGAATGTGGATGAATC-3′ R: 5′-CAAGGCATCCTGACTGCAGCA-3′ | 1 cycle of 95 °C for 4 min, 30 cycles of 94 °C for 30 s, 58 °C for 30 s, and 72 °C for 45 s, and 1 cycle of 72 °C for 10 min |
| HCP5 | F: 5′-GGGCAACTAAGTCAGGTCTAG-3′ R: 5′-TCTGCAGGTCTCATGGAGAG-3′ | |
| HLA-DOA | F: 5′-CAACAACGTAAAGCTAACGTCTGTG-3′ R: 5′-GCACCACTCTTAGTTATGTATAGG-3′ | |
| HLA-DOB | F: 5′-TCTTCTGAAGACTGTGGAGACTGC-3′ R: 5′-TCCCATAGGAGCTCAGTCTGAAT-3′ | |
| HSPA1L | F: 5′-TCCCCTTCAAGGTACATTCACAGCC-3′ R: 5′-TGATCCAGGTGTATGAGGGCGAGAG-3′ | |
| LTA | F: 5′-AGCATAAAAGGCAAAGGGGCAG-3′ R: 5′-TTAGGTATGAGGTGGACACCTC-3′ | |
| NOTCH4 | F: 5′-GATTGTCTGTTGGGTGACCTGAG-3′ R: 5′-TGAGGCTGATCACAATGAGTGCCTCTC-3′ | |
| RING1 | F: 5′-TAATCGACTCTGGCGCCCACAT-3′ R: 5′-AACAACCTTAGCCTCGGTTCCCTT-3′ | |
| TRIM27 | F: 5′-AGTCGGGATTACAGAAATGCACC-3′ R: 5′-GCAGGACATTTGAAGGTAACC-3′ | |
| BAG6 | F: 5′-ATTCATTCAGGGGCACAAGGGG-3′ R: 5′-GCGGAGGTTGAAGAGAATAGAAGC-3′ | 1 cycle of 95 °C for 3 min, 30 cycles of 95 °C for 30 s, 60 °C for 30 s, and 72 °C for 60 s, and 1 cycle of 72 °C for 10 min |
| TNFSF4 | F: 5′-GGCTTGGAGTCTATGATATTGTGCC-3′ R: 5′-GAAGGGCGTTTAACCACACTTTACG-3′ | |
| CTLA4-1 | F: 5′-GGCAACAGAGACCCCACCGTT-3′ R: 5′-GAGGACCTTCCTTAAATCTGGAGAG-3′ | 1 cycle of 95 °C for 10 min, 35 cycles of 94 °C for 30 s, 65.5 °C for 30 s, and 72 °C for 60 s, and 1 cycle of 72 °C for 3 min |
| CTLA4-2 | F: 5′-CTCTCCAGATTTAAGGAAGGTCCT C-3′ R: 5′-GGAATACAGAGC CAGCCAAGC C-3′ | |
| CTLA4-3 | F: 5′-CTAGGGACCCAATATGTGTTG-3′ R: 5′-AGAAACATCCCAGCT CTGTC-3′ | 1 cycle of 95 °C for 10 min, 35 cycles of 94 °C for 30 s, 59 °C for 30 s, and 72 °C for 60 s, and 1 cycle of 72 °C for 3 min |
| CTLA4-4 | F: 5′-GCTTGGAAACTGGATGAGGTCATAGC-3′ R: 5′-AGAGGAAGAGACACAGACAGAGTTGC-3′ | |
| PDCD1-1 | F: 5′-ACCCACACAGCCTCACATCTCT-3′ R: 5′-AAACTGAGGGTGGAAGGTCCCT-3′ | 1 cycle at 94 °C for 4 min, 30 cycles at 94 °C for 30 s, 55 °C for 30 s, and 72 °C for 60 s, and 1 cycle at 72 °C for 7 min |
| PDCD1-2 | F: 5′-TGGTGACCCCAAGTGTGTTTCTC-3′ R: 5′-GAGGAATTT TTCACCGGAGGGC-3′ | 1 cycle at 94 °C for 4 min, 30 cycles at 95 °C for 30 s, 61 °C for 30 s, and 72 °C for 120 s, and 1 cycle at 72 °C for 10 min |
| Patient Characteristics | N (%) |
|---|---|
| Number of patients | 24 |
| Gender (female/male) | |
| Recipient | 12 (50.0):12 (50.0) |
| Donor | 9 (37.5):15 (62.5) |
| Age, median years (range) | 43.9 (8 m–67 y) |
| Diseases | |
| AML | 17 (70.8) |
| ALL | 7 (29.2) |
| Type of donor | |
| Parents | 4 (16.7) |
| Siblings | 12 (50.0) |
| Offspring | 6 (25.0) |
| Unrelated | 2 (8.3) |
| Sex pairing (donor → recipient) | |
| M → F | 8 (33.3) |
| M → M | 7 (29.2) |
| F → F | 4 (16.7) |
| F → M | 5 (20.8) |
| Graft source | |
| Peripheral blood | 24 (100.0) |
| Conditioning regimen | |
| Myeloablative | 10 (42) |
| Reduced intensity | 14 (58) |
| GVHD prophylaxis | |
| Post-transplant cyclophosphamide | 24 (100.0) |
| CMV serostatus | |
| R-/D- | 1 (4.1) |
| R-/D+ | 0 (0) |
| R+/D- | 4 (16.7) |
| R+/D+ | 15 (62.5) |
| Unknown | 4 (16.7) |
| Median follow-up among survivors, months (range) | 29 (6–99) |
| Clinical Outcomes | N (%) |
|---|---|
| Survival status | |
| Alive | 13 (54.2) |
| Death | 11 (45.8) |
| Relapse status | |
| Relapse | 16 (66.7) |
| No relapse | 8 (33.3) |
| aGVHD | 14 (58.3) |
| GVHD I–II | 8 (33.3) |
| GVHD III–IV | 6 (25.0) |
| cGVHD | 4 (16.7) |
| No GVHD | 6 (25.0) |
| Other complications | |
| Hemorrhagic cystitis (BK virus related) | 6 (25.0) |
| Myelitis | 1 (4.1) |
| Secondary graft failure | 2 (8.2) |
| Septic shock and congestive heart failure | 1 (4.1) |
| None | 14 (58.3) |
| SNP | Genes | Outcome | No. of Patients (%) | Model | p-Value | ||
|---|---|---|---|---|---|---|---|
| rs79327197 | HLA-DOA | Survival | AA | AG | GG | Heterozygous | 0.031 |
| Alive | 13 (65.0) | 0 (0.0) | 0 (0.0) | ||||
| Death | 7 (35.0) | 4 (100.0) | 0 (0.0) | ||||
| rs107822 | RING1 | Survival | TT | CT | CC | Dominant | 0.036 |
| Alive | 10 (71.4) | 2 (25.0) | 0 (0.0) | ||||
| Death | 4 (28.6) | 6 (75.0) | 1 (100.0) | ||||
| SNP | Genes | Outcome | No of Patients (%) | Model | p-Value | ||
|---|---|---|---|---|---|---|---|
| rs5742909 | CTLA4 | Survival | CC | CT | TT | Heterozygous | 0.041 |
| Alive | 8 (42.1) | 5 (100.0) | 0 (0.0) | ||||
| Death | 11 (57.9) | 0 (0.0) | 0 (0.0) | ||||
| rs1234314 | TNFSF4 | Survival | CC | CG | GG | Dominant | 0.033 |
| Alive | 7 (87.5) | 4 (36.4) | 2 (40.0) | ||||
| Death | 1 (12.5) | 7 (63.6) | 3 (60.0) | ||||
| rs107822 | RING1 | Relapse | TT | CT | CC | Additive | 0.047 |
| Yes | 9 (75.0) | 2 (22.2) | 1 (33.3) | Dominant | 0.014 | ||
| No | 3 (25.0) | 7 (77.8) | 2 (66.7) | Heterozygous | 0.030 | ||
| rs36084323 | PDCD1 | Relapse | CC | CT | TT | Additive | 0.042 |
| Yes | 1 (14.3) | 6 (54.5) | 5 (83.3) | ||||
| No | 6 (85.7) | 5 (45.5) | 1 (16.7) | ||||
| rs5839828 | PDCD1 | Relapse | del/del | del/G | GG | Additive | 0.014 |
| Yes | 6 (85.7) | 6 (50.0) | 0 (0.0) | Recessive | 0.037 | ||
| No | 1 (14.3) | 6 (50.0) | 5 (100.0) | Homozygous | 0.015 | ||
| rs2523676 | HCP5 | GVHD | CC | CT | TT | Additive | 0.026 |
| Yes | 4 (40.0) | 10 (83.3) | 0 (0.0) | ||||
| No | 6 (60.0) | 2 (16.7) | 2 (100.0) | ||||
| rs213210 | RING1 | GVHD I-II | GG | AG | AA | Additive | 0.045 |
| Yes | 2 (22.2) | 6 (60.0) | 0 (0.0) | ||||
| No | 7 (77.8) | 4 (40.0) | 5 (100.0) | ||||
| rs213210 | RING1 | GVHD III-IV | GG | AG | AA | Additive | 0.031 |
| Yes | 3 (33.3) | 0 (0.0) | 3 (60.0) | ||||
| No | 6 (66.7) | 10 (100.0) | 2 (40.0) | ||||
| rs107822 | RING1 | cGVHD | TT | CT | CC | Additive | 0.018 |
| Yes | 0 (0.0) | 4 (44.4) | 0 (0.0) | Heterozygous | 0.021 | ||
| No | 12 (100.0) | 5 (55.6) | 3 (100.0) | ||||
| SNP | Gene | Outcome | Mismatched Frequency (%) | p-Value | |
|---|---|---|---|---|---|
| rs107822 | RING1 | Relapse | Matched | Mismatched | 0.006 |
| Yes | 9 (81.8) | 3 (25) | |||
| No | 2 (18.2) | 9 (75) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, C.-P.; Lin, T.-L.; Tsai, S.-H.; Lin, W.-T.; Hsu, F.-P.; Wang, W.-T.; Chen, D.-P. Preliminary Data on SNP of Transplantation-Related Genes after Haploidentical Stem Cell Transplantation. J. Clin. Med. 2024, 13, 4681. https://doi.org/10.3390/jcm13164681
Tseng C-P, Lin T-L, Tsai S-H, Lin W-T, Hsu F-P, Wang W-T, Chen D-P. Preliminary Data on SNP of Transplantation-Related Genes after Haploidentical Stem Cell Transplantation. Journal of Clinical Medicine. 2024; 13(16):4681. https://doi.org/10.3390/jcm13164681
Chicago/Turabian StyleTseng, Ching-Ping, Tung-Liang Lin, Shu-Hui Tsai, Wei-Tzu Lin, Fang-Ping Hsu, Wei-Ting Wang, and Ding-Ping Chen. 2024. "Preliminary Data on SNP of Transplantation-Related Genes after Haploidentical Stem Cell Transplantation" Journal of Clinical Medicine 13, no. 16: 4681. https://doi.org/10.3390/jcm13164681
APA StyleTseng, C.-P., Lin, T.-L., Tsai, S.-H., Lin, W.-T., Hsu, F.-P., Wang, W.-T., & Chen, D.-P. (2024). Preliminary Data on SNP of Transplantation-Related Genes after Haploidentical Stem Cell Transplantation. Journal of Clinical Medicine, 13(16), 4681. https://doi.org/10.3390/jcm13164681