
Impact of Frailty on Functional Improvement Following Traumatic Spinal Cord Injury: A Japanese Single-Center Experience

 ,
,
Abstract
1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Makizako, H.; Nishita, Y.; Jeong, S.; Otsuka, R.; Shimada, H.; Iijima, K.; Obuchi, S.; Kim, H.; Kitamura, A.; Ohara, Y.; et al. Trends in the Prevalence of Frailty in Japan: A Meta-Analysis from the Ilsa-J. J. Frailty Aging 2021, 10, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Vale, H. Impact of Japan’s Aging Population on Healthcare Costs and the Long-Term Care Insurance System. Stud. Soc. Sci. Humanit. 2024, 3, 39–44. [Google Scholar]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Prince, M.; Thiyagarajan, J.A.; De Carvalho, I.A.; Bernabei, R.; Chan, P.; Gutierrez-Robledo, L.M.; Michel, J.P.; Morley, J.E.; Ong, P.; et al. Frailty: An Emerging Public Health Priority. J. Am. Med. Dir. Assoc. 2016, 17, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, J.; Denvir, M.; Gunn, J. Frailty assessment in elderly people. Lancet 2013, 381, 1985–1986. [Google Scholar] [CrossRef] [PubMed]
- Kulminski, A.M.; Ukraintseva, S.V.; Kulminskaya, I.V.; Arbeev, K.G.; Land, K.; Yashin, A.I. Cumulative deficits better characterize susceptibility to death in elderly people than phenotypic frailty: Lessons from the Cardiovascular Health Study. J. Am. Geriatr. Soc. 2008, 56, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, M.; Konomi, T.; Maeda, S.; Tabuki, H.; Uemura, O.; Yato, Y. Problems in adjusting discharge during the recovery period of patients with spinal cord injury: Using spinal cord independence measure (SCIM). J. Jpn. Med. Soc. Spinal Cord. Lesion 2020, 33, 140–142. [Google Scholar]
- Katoh, S.; Enishi, T.; Sato, N.; Sairyo, K. High incidence of acute traumatic spinal cord injury in a rural population in Japan in 2011 and 2012: An epidemiological study. Spinal Cord 2014, 52, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Miyakoshi, N.; Suda, K.; Kudo, D.; Sakai, H.; Nakagawa, Y.; Mikami, Y.; Suzuki, S.; Tokioka, T.; Tokuhiro, A.; Takei, H.; et al. A nationwide survey on the incidence and characteristics of traumatic spinal cord injury in Japan in 2018. Spinal Cord 2021, 59, 626–634. [Google Scholar] [CrossRef]
- Fawcett, J.W.; Curt, A.; Steeves, J.D.; Coleman, W.P.; Tuszynski, M.H.; Lammertse, D.; Bartlett, P.F.; Blight, A.R.; Dietz, V.; Ditunno, J.; et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: Spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord. 2007, 45, 190–205. [Google Scholar] [CrossRef]
- Burns, A.S.; Marino, R.J.; Flanders, A.E.; Flett, H. Clinical diagnosis and prognosis following spinal cord injury. Handb. Clin. Neurol. 2012, 109, 47–62. [Google Scholar] [CrossRef]
- Kawano, O.; Maeda, T.; Mori, E.; Takao, T.; Sakai, H.; Masuda, M.; Morishita, Y.; Hayashi, T.; Kubota, K.; Kobayakawa, K.; et al. How much time is necessary to confirm the diagnosis of permanent complete cervical spinal cord injury? Spinal Cord. 2020, 58, 284–289. [Google Scholar] [CrossRef]
- Cowley, A.; Goldberg, S.E.; Gordon, A.L.; Logan, P.A. Rehabilitation potential in older people living with frailty: A systematic mapping review. BMC Geriatr. 2021, 21, 533. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Lee, M.; Kiratli, J. Cardiovascular disease in spinal cord injury: An overview of prevalence, risk, evaluation, and management. Am. J. Phys. Med. Rehabil. 2007, 86, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Berlowitz, D.J.; Wadsworth, B.; Ross, J. Respiratory problems and management in people with spinal cord injury. Breathe 2016, 12, 328–340. [Google Scholar] [CrossRef]
- Van Leeuwen, C.M.; Kraaijeveld, S.; Lindeman, E.; Post, M.W. Associations between psychological factors and quality of life ratings in persons with spinal cord injury: A systematic review. Spinal Cord. 2012, 50, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Catz, A.; Itzkovich, M.; Tamir, A.; Philo, O.; Steinberg, F.; Ring, H.; Ronen, J.; Spasser, R.; Gepstein, R. SCIM--spinal cord independence measure (version II): Sensitivity to functional changes. Harefuah 2002, 141, 1025–1031, 1091. [Google Scholar]
- Itzkovich, M.; Gelernter, I.; Biering-Sorensen, F.; Weeks, C.; Laramee, M.T.; Craven, B.C.; Tonack, M.; Hitzig, S.L.; Glaser, E.; Zeilig, G.; et al. The Spinal Cord Independence Measure (SCIM) version III: Reliability and validity in a multi-center international study. Disabil. Rehabil. 2007, 29, 1926–1933. [Google Scholar] [CrossRef]
- Tsiouris, A.; Hammoud, Z.T.; Velanovich, V.; Hodari, A.; Borgi, J.; Rubinfeld, I. A modified frailty index to assess morbidity and mortality after lobectomy. J. Surg. Res. 2013, 183, 40–46. [Google Scholar] [CrossRef]
- Leven, D.M.; Lee, N.J.; Kothari, P.; Steinberger, J.; Guzman, J.; Skovrlj, B.; Shin, J.I.; Caridi, J.M.; Cho, S.K. Frailty Index Is a Significant Predictor of Complications and Mortality After Surgery for Adult Spinal Deformity. Spine 2016, 41, E1394–E1401. [Google Scholar] [CrossRef]
- Ali, R.; Schwalb, J.M.; Nerenz, D.R.; Antoine, H.J.; Rubinfeld, I. Use of the modified frailty index to predict 30-day morbidity and mortality from spine surgery. J. Neurosurg. Spine 2016, 25, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Dicpinigaitis, A.J.; Al-Mufti, F.; Bempong, P.O.; Kazim, S.F.; Cooper, J.B.; Dominguez, J.F.; Stein, A.; Kalakoti, P.; Hanft, S.; Pisapia, J.; et al. Prognostic Significance of Baseline Frailty Status in Traumatic Spinal Cord Injury. Neurosurgery 2022, 91, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Lucas, J.T.; Ducker, T.B. Motor classification of spinal cord injuries with mobility, morbidity and recovery indices. Am. Surg. 1979, 45, 151–158. [Google Scholar] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Lang, P.O.; Michel, J.P.; Zekry, D. Frailty syndrome: A transitional state in a dynamic process. Gerontology 2009, 55, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Gambassi, G.; van Kan, G.A.; Vellas, B. The frailty phenotype and the frailty index: Different instruments for different purposes. Age Ageing 2014, 43, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Mouchtouris, N.; Luck, T.; Locke, K.; Hines, K.; Franco, D.; Yudkoff, C.; Sivaganesan, A.; Heller, J.; Prasad, S.; Harrop, J.; et al. Comparison of 5-Item and 11-Item Modified Frailty Index as Predictors of Functional Independence in Patients With Spinal Cord Injury. Glob. Spine J. 2023. [Google Scholar] [CrossRef] [PubMed]
- Banaszek, D.; Inglis, T.; Marion, T.E.; Charest-Morin, R.; Moskven, E.; Rivers, C.S.; Kurban, D.; Flexman, A.M.; Ailon, T.; Dea, N.; et al. Effect of Frailty on Outcome after Traumatic Spinal Cord Injury. J. Neurotrauma 2020, 37, 839–845. [Google Scholar] [CrossRef]
- Chu, H.; Chen, L.; Li, J.; Li, J.; Yang, D.; Yang, M.; Du, L.; Wang, M.; Gao, F. Impact of Frailty on Inpatient Outcomes of Acute Traumatic Spinal Cord Injury: Evidence From US National Inpatient Sample. Neurologist 2024, 29, 82–90. [Google Scholar] [CrossRef]
- Rockwood, K.; Song, X.; Mitnitski, A. Changes in relative fitness and frailty across the adult lifespan: Evidence from the Canadian National Population Health Survey. CMAJ 2011, 183, E487–E494. [Google Scholar] [CrossRef] [PubMed]
- Unai, K.; Uemura, O.; Takemura, R.; Kawakami, M.; Liu, M. Association Between SCIM III Total Scores and Individual Item Scores to Predict Independence With ADLs in Persons With Spinal Cord Injury. Arch. Rehabil. Res. Clin. Transl. 2019, 1, 100029. [Google Scholar] [CrossRef] [PubMed]
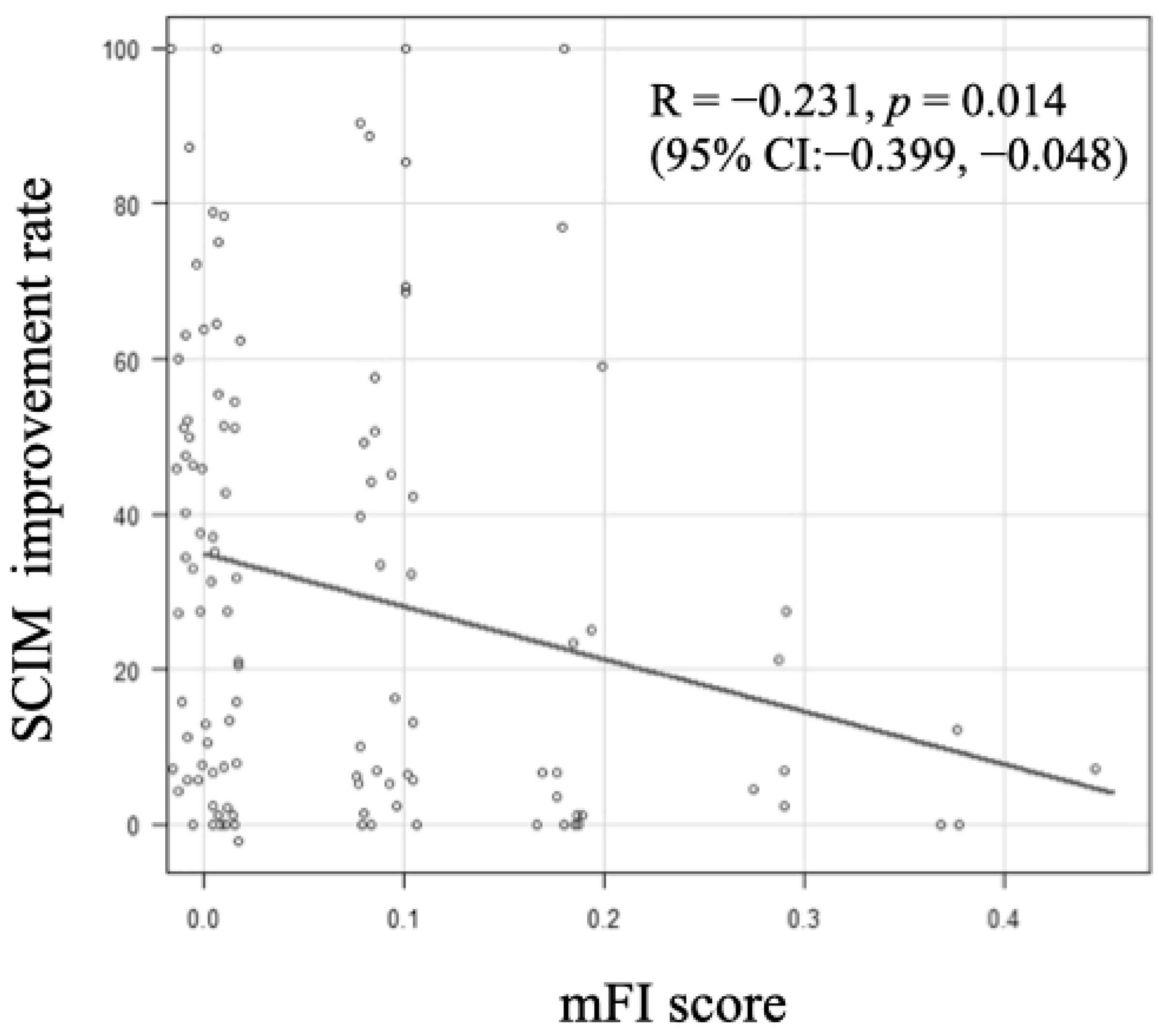

{kind=link}
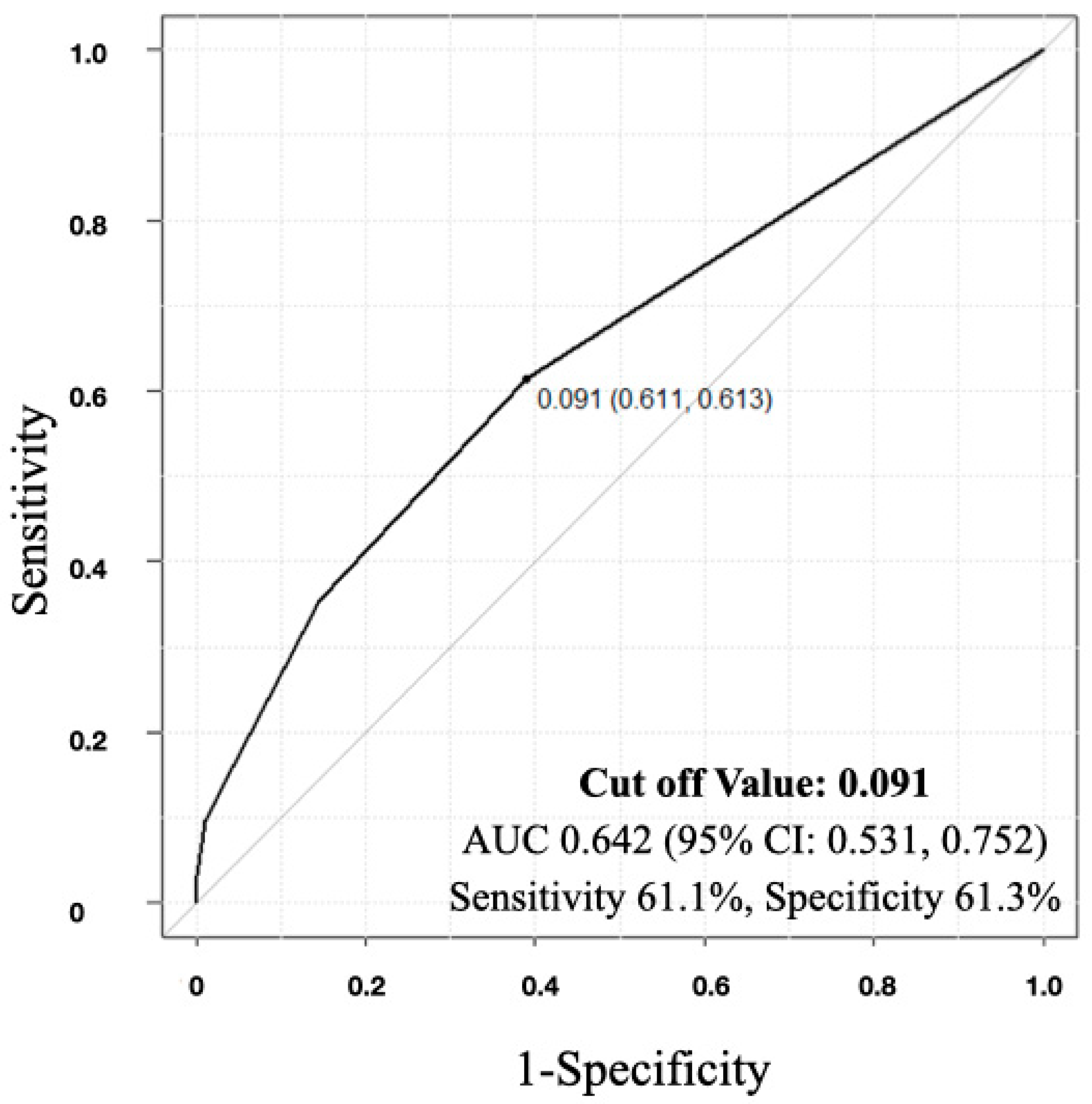
{kind=link}
| Robust (n = 97) | Frail (n = 24) | p | |
|---|---|---|---|
| Age at Injury (Year; Mean [SD]) | 56.6 ± 19.8 | 71.8 ± 9.7 | <0.01 |
| Age Demographic (n [%]) | |||
| <60 | 44 (45.4) | 4 (16.7) | <0.05 |
| 60–74 | 34 (35.1) | 11 (45.8) | - |
| ≥75 | 19 (19.6) | 9 (37.5) | - |
| Sex (Male/Female) | 81:16 | 21:3 | 0.76 |
| Injury Pattern (n [%]) | |||
| Paraplegia | 13 (13.4) | 2 (8.3) | 0.73 |
| Tetraplegia | 84 (86.6) | 22 (91.7) | - |
| Initial Neurological AIS Status (n [%]) | |||
| A | 25 (28.7) | 4 (19.0) | 0.40 |
| B | 18 (20.7) | 8 (38.1) | - |
| C | 21 (24.1) | 5 (23.8) | - |
| D | 23 (26.4) | 4 (19.0) | - |
| Robust (n = 97) | Frail (n = 24) | p | |
|---|---|---|---|
| SCIM Score (Out of 100) | |||
| Initial Score (Mean [SD]) | 27.6 ± 23.5 | 18.5 ± 16.7 | 0.09 |
| Discharge Score (Mean [SD]) | 47.4 ± 29.9 | 30.7 ± 26.5 | <0.05 |
| Percent Recovery (%; Mean [SD]) | 33.5 ± 29.0 | 16.7 ± 26.7 | <0.05 |
| Hospital Stay (Day; Mean [SD]) | 254.1 ± 136.7 | 224.7 ± 129.8 | 0.34 |
| Home Discharge (n [%]) | 66 (68.0) | 11 (45.8) | <0.05 |
| Requiring Total Assistance at Admission (n [%]) | 43 (45.3) | 9 (37.5) | 0.65 |
| Requiring Total Assistance at Discharge (n [%]) | 20 (20.8) | 7 (29.2) | 0.42 |
| Complication | |||
| Tracheostomy (n [%]) | 16 (16.5) | 4 (16.7) | 1 |
| Pressure Ulcer (n [%]) | 18 (18.6) | 8 (33.3) | 0.16 |
| In-Hospital Death (n [%]) | 3 (3.1) | 0 (0.0) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konomi, T.; Yoshikawa, M.; Kajikawa, K.; Kitagawa, T.; Kobayashi, Y.; Furukawa, M.; Fujiyoshi, K.; Yato, Y. Impact of Frailty on Functional Improvement Following Traumatic Spinal Cord Injury: A Japanese Single-Center Experience. J. Clin. Med. 2024, 13, 4154. https://doi.org/10.3390/jcm13144154
Konomi T, Yoshikawa M, Kajikawa K, Kitagawa T, Kobayashi Y, Furukawa M, Fujiyoshi K, Yato Y. Impact of Frailty on Functional Improvement Following Traumatic Spinal Cord Injury: A Japanese Single-Center Experience. Journal of Clinical Medicine. 2024; 13(14):4154. https://doi.org/10.3390/jcm13144154
Chicago/Turabian StyleKonomi, Tsunehiko, Minako Yoshikawa, Keita Kajikawa, Takahiro Kitagawa, Yoshiomi Kobayashi, Mitsuru Furukawa, Kanehiro Fujiyoshi, and Yoshiyuki Yato. 2024. "Impact of Frailty on Functional Improvement Following Traumatic Spinal Cord Injury: A Japanese Single-Center Experience" Journal of Clinical Medicine 13, no. 14: 4154. https://doi.org/10.3390/jcm13144154
APA StyleKonomi, T., Yoshikawa, M., Kajikawa, K., Kitagawa, T., Kobayashi, Y., Furukawa, M., Fujiyoshi, K., & Yato, Y. (2024). Impact of Frailty on Functional Improvement Following Traumatic Spinal Cord Injury: A Japanese Single-Center Experience. Journal of Clinical Medicine, 13(14), 4154. https://doi.org/10.3390/jcm13144154