
The Presence of Myosteatosis Is Associated with Age, Severity of Liver Disease and Poor Outcome and May Represent a Prodromal Phase of Sarcopenia in Patients with Liver Cirrhosis



 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Data
2.3. Muscle Strength Assessment
2.4. Muscle Mass Quantity and Quality Assessment
2.5. Physical Performance Assessment
2.6. Sarcopenia Diagnosis
2.7. Follow-Up
2.8. Statistical Analysis
3. Results
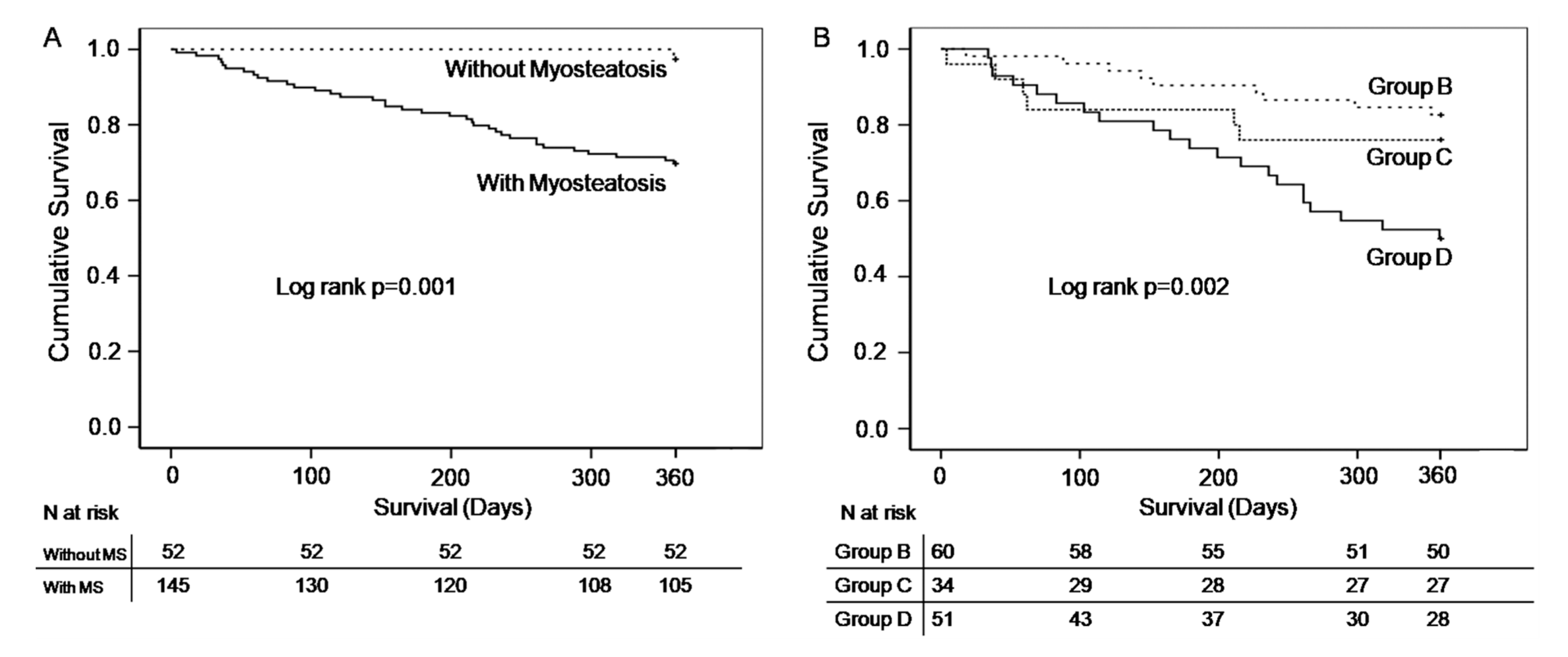
3.1. Survival
3.2. Study of Groups Composed According to the Extent of Muscle Abnormalities
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Correa-De-Araujo, R.; Addison, O.; Miljkovic, I.; Goodpaster, B.H.; Bergman, B.C.; Clark, R.V.; Elena, J.W.; Esser, K.A.; Ferrucci, L.; Harris-Love, M.O.; et al. Myosteatosis in the Context of Skeletal Muscle Function Deficit: An interdisciplinary workshop at the national institute on aging. Front. Physiol. 2020, 11, 963. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Aging 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Lang, T.; Cauley, J.A.; Tylavsky, F.; Bauer, D.; Cummings, S.; Harris, T.B. Computed tomographic measurements of thigh muscle cross-sectional area and attenuation coefficient predict hip fracture: The health, aging, and body composition study. J. Bone Miner Res. 2010, 25, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Frank-Wilson, A.W.; Chalhoub, D.; Figueiredo, P.; Jónsson, P.V.; Siggeirsdóttir, K.; Sigurdsson, S.; Eiriksdottir, G.; Guðnason, V.; Launer, L.; Harris, T.B.; et al. Associations of quadriceps torque properties with muscle size, attenuation, and intramuscular adipose tissue in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Schulze-Hagen, M.; Püngel, T.; Bündgens, L.; Wirtz, T.; Kather, J.N.; Vucur, M.; Paffenholz, P.; Demir, M.; Bruners, P.; et al. Skeletal muscle composition predicts outcome in critically ill patients. Crit. Care Explor. 2020, 2, e0171. [Google Scholar] [CrossRef]
- Fang, T.; Gong, Y.; Wang, Y. Prognostic values of myosteatosis for overall survival in patients with gastric cancers: A meta-analysis with trial sequential analysis. Nutrition 2023, 105, 111866. [Google Scholar] [CrossRef]
- Avesani, C.M.; de Abreu, A.M.; Ribeiro, H.S.; Brismar, T.B.; Stenvinkel, P.; Sabatino, A.; Lindholm, B. Muscle fat infiltration in chronic kidney disease: A marker related to muscle quality, muscle strength and sarcopenia. J. Nephrol. 2023, 36, 895–910. [Google Scholar] [CrossRef] [PubMed]
- Miljkovic, I.; Kuipers, A.; Cauley, J.A.; Prasad, T.; Lee, C.G.; Ensrud, K.; Cawthon, P.M.; Hoffman, A.R.; Dam, T.-T.; Gordon, C.L.; et al. Osteoporotic Fractures in Men Study Group. Greater skeletal muscle fat infiltration is associated with higher all-cause and cardiovascular mortality in older men. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1133–1140. [Google Scholar] [CrossRef]
- Bhanji, R.A.; Moctezuma-Velazquez, C.; Duarte-Rojo, A.; Ebadi, M.; Ghosh, S.; Rose, C.; Montano-Loza, A.J. Myosteatosis and sarcopenia are associated with hepatic encephalopathy in patients with cirrhosis. Hepatol. Int. 2018, 12, 377–386. [Google Scholar] [CrossRef]
- Nardelli, S.; Lattanzi, B.; Merli, M.; Farcomeni, A.; Gioia, S.; Ridola, L.; Riggio, O. Muscle alterations are associated with minimal and overt hepatic encephalopathy in patients with liver cirrhosis. Hepatology 2019, 70, 1704–1713. [Google Scholar] [CrossRef]
- Nardelli, S.; Gioia, S.; Ridola, L.; Carlin, M.; Cioffi, A.D.; Merli, M.; Spagnoli, A.; Riggio, O. Risk of falls in patients with cirrhosis evaluated by timed up and go test: Does muscle or brain matter more? Dig. Liver Dis. 2022, 54, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Lattanzi, B.; Nardelli, S.; Pigliacelli, A.; Di Cola, S.; Farcomeni, A.; D’ambrosio, D.; Gioia, S.; Corradini, S.G.; Lucidi, C.; Mennini, G.; et al. The additive value of sarcopenia, myosteatosis and hepatic encephalopathy in the predictivity of model for end-stage liver disease. Dig. Liver Dis. 2019, 51, 1508–1512. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Tsien, C.; Bhanji, R.A.; Dunichand-Hoedl, A.R.; Rider, E.; Motamedrad, M.; Mazurak, V.C.; Baracos, V.; Montano-Loza, A.J. Skeletal muscle pathological fat infiltration (myosteatosis) is associated with higher mortality in patients with cirrhosis. Cells 2022, 11, 1345. [Google Scholar] [CrossRef] [PubMed]
- Meister, F.A.; Bednarsch, J.; Amygdalos, I.; Boecker, J.; Strnad, P.; Bruners, P.; Lang, S.A.; Ulmer, T.F.; Heij, L.; Santana, D.A.M.; et al. Various myosteatosis selection criteria and their value in the assessment of short- and long-term outcomes following liver transplantation. Sci. Rep. 2021, 11, 13368. [Google Scholar] [CrossRef]
- Czigany, Z.; Kramp, W.; Lurje, I.; Miller, H.; Bednarsch, J.; Lang, S.A.; Ulmer, T.F.; Bruners, P.; Strnad, P.; Trautwein, C.; et al. The role of recipient myosteatosis in graft and patient survival after deceased donor liver transplantation. J. Cachexia Sarcopenia Muscle 2021, 12, 358–367. [Google Scholar] [CrossRef]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef]
- Larson-Meyer, D.E.; Smith, S.R.; Heilbronn, L.K.; Kelley, D.E.; Ravussin, E.; Newcomer, B.R. Look AHEAD Adipose Research Group. Muscle-associated triglyceride measured by computed tomography and magnetic resonance spectroscopy. Obesity 2006, 14, 73–87. [Google Scholar] [CrossRef]
- Ebadi, M.; Bhanji, R.A.; Tandon, P.; Mazurak, V.; Baracos, V.E.; Montano-Loza, A.J. Review article: Prognostic significance of body composition abnormalities in patients with cirrhosis. Aliment. Pharmacol. Ther. 2020, 52, 600–618. [Google Scholar] [CrossRef] [PubMed]
- Tachi, Y.; Kozuka, A.; Hirai, T.; Ishizu, Y.; Honda, T.; Kuzuya, T.; Hayashi, K.; Ishigami, M.; Goto, H. Impact of myosteatosis on skeletal muscle volume loss in patients with chronic liver disease. J. Gastroenterol. Hepatol. 2018, 33, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Berzigotti, A.; Zelber-Sagi, S.; Dasarathy, S.; Montagnese, S.; Genton, L.; Plauth, M.; Parés, A. EASL clinical practice guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardized approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef]
- Georgiou, A.; Papatheodoridis, G.V.; Alexopoulou, A.; Deutsch, M.; Vlachogiannakos, I.; Ioannidou, P.; Papageorgiou, M.V.; Papadopoulos, N.; Yannakoulia, M.; Kontogianni, M.D. Validation of cutoffs for skeletal muscle mass index based on computed tomography analysis against dual energy X-ray absorptiometry in patients with cirrhosis: The KIRRHOS study. Ann. Gastrenterol. 2020, 33, 80–86. [Google Scholar] [CrossRef]
- Freire, A.N.; Guerra, R.O.; Alvarado, B.; Guralnik, J.M.; Zunzunegui, M.V. Validity and reliability of the short physical performance battery in two diverse older adult populations in Quebec and Brazil. J. Aging Health 2012, 24, 863–878. [Google Scholar] [CrossRef]
- Carey, E.; Lai, J.; Wang, C.; Dasarathy, S.; Lobach, I.; Montano-Loza, A.J.; Dunn, M.A. A multicenter study to define sarcopenia in patients with end-stage liver disease. Liver Transpl. 2017, 23, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Davuluri, G.; Allawy, A.; Thapaliya, S.; Rennison, J.H.; Singh, D.; Kumar, A.; Sandlers, Y.; Van Wagoner, D.R.; Flask, C.A.; Hoppel, C.; et al. Hyperammonaemia-induced skeletal muscle mitochondrial dysfunction results in cataplerosis and oxidative stress. J. Physiol. 2016, 594, 7341–7360. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Lario, M.; Álvarez-Mon, M. Cirrhosis-associated immune dysfunction: Distinctive features and clinical relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Tsien, C.; Bhanji, R.A.; Dunichand-Hoedl, A.R.; Rider, E.; Motamedrad, M.; Mazurak, V.C.; Baracos, V.; Montano-Loza, A.J. Myosteatosis in cirrhosis: A review of diagnosis, pathophysiological mechanisms and potential interventions. Cells 2022, 11, 1216. [Google Scholar] [CrossRef]
- Purnak, T.; Yilmaz, Y. Liver disease and malnutrition. Best Pract. Res. Clin. Gastroenterol. 2013, 27, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Okada, H.; Hashimoto, Y.; Kumagai, M.; Nishimura, H.; Oda, Y.; Fukui, M. Relationship between nonalcoholic fatty liver disease and muscle quality as well as quantity evaluated by computed tomography. Liver Int. 2020, 40, 120–130. [Google Scholar] [CrossRef] [PubMed]
- De Munck, T.J.; Verhaegh, P.; Lodewick, T.; Bakers, F.; Jonkers, D.; Masclee, A.A.; Verbeek, J.; Koek, G.H. Myosteatosis in nonalcoholic fatty liver disease: An exploratory study. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101500. [Google Scholar] [CrossRef]
- Nachit, M.; Kwanten, W.J.; Thissen, J.-P.; De Beeck, B.O.; Van Gaal, L.; Vonghia, L.; Verrijken, A.; Driessen, A.; Horsmans, Y.; Francque, S.; et al. Muscle fat content is strongly associated with NASH: A longitudinal study in patients with morbid obesity. J. Hepatol. 2021, 75, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Montano-Loza, A.J.; Angulo, P.; Meza-Junco, J.; Prado, C.M.M.; Sawyer, M.B.; Beaumont, C.; Esfandiari, N.; Ma, M.; Baracos, V.E. Sarcopenic obesity and myosteatosis are associated with higher mortality in patients with cirrhosis. J. Cachexia Sarcopenia Muscle 2016, 7, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.; Kim, D.W.; Ko, Y.; Ha, J.; Bin Shin, Y.; Lee, J.; Sung, Y.S.; Kim, K.W. Updated systematic review and meta-analysis on diagnostic issues and the prognostic impact of myosteatosis: A new paradigm beyond sarcopenia. Ageing Res. Rev. 2021, 70, 101398. [Google Scholar] [CrossRef]
- Henin, G.; Lanthier, N.; Dahlqvist, G. Pathophysiological changes of the liver-muscle axis in end-stage liver disease: What is the right target? Acta Gastroenterol. Belg. 2022, 85, 611–624. [Google Scholar] [CrossRef] [PubMed]
- Bot, D.; Droop, A.; Lucassen, C.J.; van Veen, M.E.; van Vugt, J.L.A.; Feshtali, S.S.; Leistra, E.; Tushuizen, M.E.; van Hoek, B. Both muscle quantity and quality are predictors of waiting list mortality in patients with end-stage liver disease. Clin. Nutr. ESPEN 2021, 42, 272–279. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Total Patients Ν = 197 | Without Myosteatosis Ν = 52 | With Myosteatosis Ν = 145 | p Value |
|---|---|---|---|---|
| Age (years) | 61.0 (52.0–68.0) | 56.0 (50.0–64.0) | 63.0 (55.0–70.0) | 0.004 |
| Gender (% male) | 132 (67) | 40 (76.9) | 92 (63.4) | 0.076 |
| Etiology (%) | 0.028 | |||
| Alcohol | 85 (43.1) | 20 (38.5) | 65 (44.8) | |
| Viral | 46 (23.4) | 19 (36.5) | 27 (18.6) | |
| Other | 66 (33.5) | 13 (25.0) | 53 (38.6) | |
| Dry BMI (kg/m2) | 25.90 (22.28–28.71) | 26.60 (25.60–29.81) | 24.70 (21.79–28.60) | 0.001 |
| Decompensated cirrhosis (%) | 120 (60.9) | 19 (36.5) | 101 (69.7) | <0.001 |
| MELD score | 11.00 (7.50–16.00) | 9.00 (7.00–12.00) | 12.00 (8.00–16,25) | 0.009 |
| Child–Pugh score | 7.0 (5.0–9.0) | 5.0 (5.0–7.0) | 8.0 (6.0–9.0) | <0.001 |
| History of hepatic encephalopathy (%) | 41 (20.8) | 4 (7.7) | 37 (25.5) | 0.013 |
| Handgrip strength (kg) | 27.0 (19.0–34.0) | 30.5 (25.0–39.5) | 26.0 (18.0–32.0) | 0.001 |
| Skeletal mass index (cm2/m2) | 47.35 (41.70–54.13) | 54.11 (48.95–57.42) | 45.12 (40.25–51.27) | <0.001 |
| Low skeletal mass index (N%) | 86 (43.7) | 9 (17.3) | 77 (53.1) | <0.001 |
| Short Physical Performance Battery | 10.0 (8.0–12.0) | 11.5 (10.0–12.0) | 10.0 (6.0–11.0) | <0.001 |
| Visceral Adipose Tissue Index (cm2/m2) | 51.04 (28.48–66.46) | 47.63 (27.76–62.69) | 51.68 (27.30–67.36) | 0.242 |
| Subcutaneous Adipose Tissue Index (cm2/m2) | 58.12 (35.96–87.37) | 64.70 (48.31–89.51) | 56.22 (34.15–86.43) | 0.114 |
| Parameter | Univariate Analysis | p Value | Model 1 | P1 Value | Model 2 | P2 Value | Model 3 | P3 Value |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 1.047 (1.016–1.080) | 0.003 | 1.047 (1.006–1.090) | 0.024 | ||||
| Gender (% male) | 1.920 (0.927–3.978) | 0.079 | ||||||
| Handgrip strength | 0.952 (0.922–0.983) | 0.003 | ||||||
| Decompensated vs. compensated cirrhosis | 3.987 (2.048–7.762) | <0.001 | 3.129 (1.336–7.328) | 0.009 | ||||
| MELD score | 1.105 (1.031–1.184) | 0.005 | ||||||
| Child–Pugh score | 1.400 (1.167–1.680) | <0.001 | 1.320 (1.052–1.657) | 0.017 | ||||
| Skeletal mass index (cm2/m2) | 0.920 (0.883–0.957) | <0.001 | 0.937 (0.885–0.992) | 0.026 | 0.932 (0.882–0.985) | 0.013 | 0.943 (0.893–0.996) | 0.036 |
| Short Physical Performance Battery | 0.695 (0.577–0.839) | <0.001 | 0.777 (0.619–0.976) | 0.030 |
| Parameter | Univariate Analysis | p Value | Multivariate Analysis | p Value |
|---|---|---|---|---|
| HR (95% CI) | HR (95% CI) | |||
| Age * (years) | 1.052 (1.018–1.085) | 0.002 | ||
| Gender * (% male) | 1.243 (0.633–2.442) | 0.527 | ||
| Dry Body Mass Index * | 0.902 (0.839–0.970) | 0.005 | ||
| MELD score * | 1.138 (1.096–1.182) | <0.001 | 4.911 (2.390–10.094) | <0.001 |
| Skeletal mass index * (cm2/m2) | 0.915 (0.880–0.951) | <0.001 | ||
| Short Physical Performance Battery (SPPB) | 0.763 (0.704–0.826) | <0.001 | ||
| Visceral Adipose Tissue Index (VATI) cm2/m2 | 0.997 (0.985–1.009) | 0.601 | ||
| Subcutaneous Adipose Tissue Index * (SATI) cm2/m2 | 0.989 (0.979–0.999) | 0.030 | ||
| Myosteatosis * | 14.042 (1.925–102.400) | 0.008 | 7.778 (1.022–59.206) | 0.048 |
| Group A Neither Myosteatosis Nor Sarcopenia (N = 49) | Group B Myosteatosis Alone (N = 60) | Group C Myosteatosis Combined by Low Handgrip * (N = 34) | Group D Myosteatosis Combined by Low Handgrip and Low SMI * (N = 51) | p | |
|---|---|---|---|---|---|
| Age | 56.0 (50.0–63.5) | 57.5 (51.25–66.00) | 62.5 (57.0–69.5) | 67.00 (59.00–72.50) | <0.001 |
| Gender (Male, N, %) | 37 (75.5) | 40 (66.7) | 17 (50.00) | 35 (68.62) | 0.109 |
| Dry BMI | 26.67 (25.61–29.98) | 24.4 (22.04–28.83) | 28.15 (24.08–34.05) | 23.28 (20.80–26.41) | <0.001 |
| Etiology (N, %): | 0.038 | ||||
| Alcoholic | 20 (40.81) | 24 (40) | 17 (50.00) | 24 (47.05) | |
| Viral | 17 (34.69) | 17 (28.33) | 6 (17.64) | 4 (7.80) | |
| Other | 12 (24.48) | 19 (31.66) | 11 (32.45) | 23 (45.09) | |
| Decompensated cirrhosis (N, %) | 16 (32.65) | 35 (58.33) | 25 (73.52) | 41 (80.39) | <0.001 |
| ΜELD score | 9.0 (7.0–10.75) | 11.0 (7.00–14.0) | 10.0 (7.00–15.75) | 15.0 (11.50–21.50) | <0.001 |
| Child–Pugh score | 5.0 (5.0–7.0) | 7.0 (5.0–9.0) | 7.0 (6.0–8.0) | 9.0 (7.0–10.0) | <0.001 |
| Handgrip strength | 32.0 (24.50–40.0) | 34.00 (30.0–38.00) | 18.50 (15.50–27.25) | 20.0 (14.0–25.0) | <0.001 |
| SMI | 54.20 (49.72–57.48) | 46.84 (42.25–53.03) | 51.03 (44.38–57.82) | 40.50 (31.57–45.54) | <0.001 |
| SPPB | 12.0 (10.0–12.0) | 11.0 (10.0–12.0) | 9.0 (6.75–11.0) | 8.00 (3.75–10.00) | <0.001 |
| VATI | 45.38 (27.97–62.28) | 50.60 (28.85–80.08) | 54.78 (35.72–96.31) | 47.43 (26.16–63.81) | 0.194 |
| SATI | 66.25 (48.62–92.32) | 58.10 (36.35–87.65) | 87.27 (48.62–124.09) | 44.36 (25.90–66.70) | <0.001 |
| Mean attenuation in HU | 37.34 (33.94–40.35) | 30.66 (26.75–35.65) | 27.98 (23.30–31.15) | 27.83 (22.50–32.35) | <0.001 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Age (per 1 year) | 1.040 (1.006–1.075) | 0.022 | 1.020 (0.984–1.057) | 0.275 |
| Gender (men vs. women) | 0.917 (0.465–1.811) | 0.804 | 0.800 (0.394–1.622) | 0.536 |
| Myosteatosis alone (group B) | Reference group | Reference group | ||
| Myosteatosis combined by low handgrip (group C *) | 1.537 (0.547–4.318) | 0.415 | 1.397 (0.492–3.693) | 0.530 |
| Myosteatosis combined by low handgrip and low skeletal muscle index (group D *) | 3.505 (1.603–7.663) | 0.002 | 3.097 (1.338–7.169) | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geladari, E.; Alexopoulos, T.; Kontogianni, M.D.; Vasilieva, L.; Mani, I.; Tenta, R.; Sevastianos, V.; Vlachogiannakos, I.; Alexopoulou, A. The Presence of Myosteatosis Is Associated with Age, Severity of Liver Disease and Poor Outcome and May Represent a Prodromal Phase of Sarcopenia in Patients with Liver Cirrhosis. J. Clin. Med. 2023, 12, 3332. https://doi.org/10.3390/jcm12093332
Geladari E, Alexopoulos T, Kontogianni MD, Vasilieva L, Mani I, Tenta R, Sevastianos V, Vlachogiannakos I, Alexopoulou A. The Presence of Myosteatosis Is Associated with Age, Severity of Liver Disease and Poor Outcome and May Represent a Prodromal Phase of Sarcopenia in Patients with Liver Cirrhosis. Journal of Clinical Medicine. 2023; 12(9):3332. https://doi.org/10.3390/jcm12093332
Chicago/Turabian StyleGeladari, Eleni, Theodoros Alexopoulos, Meropi D. Kontogianni, Larisa Vasilieva, Iliana Mani, Roxane Tenta, Vasilios Sevastianos, Ioannis Vlachogiannakos, and Alexandra Alexopoulou. 2023. "The Presence of Myosteatosis Is Associated with Age, Severity of Liver Disease and Poor Outcome and May Represent a Prodromal Phase of Sarcopenia in Patients with Liver Cirrhosis" Journal of Clinical Medicine 12, no. 9: 3332. https://doi.org/10.3390/jcm12093332
APA StyleGeladari, E., Alexopoulos, T., Kontogianni, M. D., Vasilieva, L., Mani, I., Tenta, R., Sevastianos, V., Vlachogiannakos, I., & Alexopoulou, A. (2023). The Presence of Myosteatosis Is Associated with Age, Severity of Liver Disease and Poor Outcome and May Represent a Prodromal Phase of Sarcopenia in Patients with Liver Cirrhosis. Journal of Clinical Medicine, 12(9), 3332. https://doi.org/10.3390/jcm12093332