
Characterization of Hypomagnesemia in Alcoholic Hepatitis Patients and Its Association with Liver Injury and Severity Markers


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Analysis of Liver Injury and Severity Based on Disease Severity
3.1.1. Demographics and Drinking History
3.1.2. Liver Injury Markers and Serum Magnesium Levels
3.1.3. Liver Disease Severity
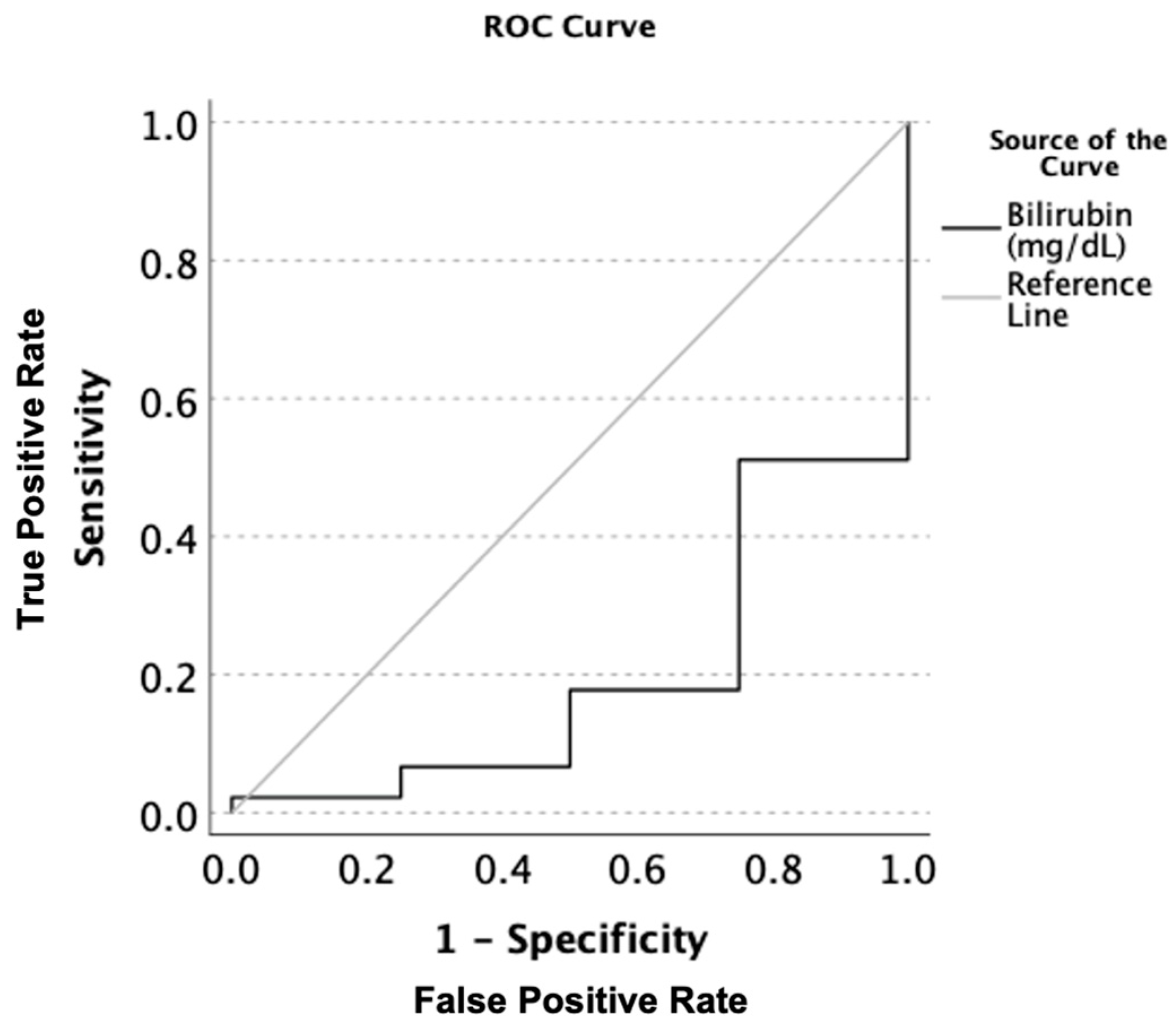
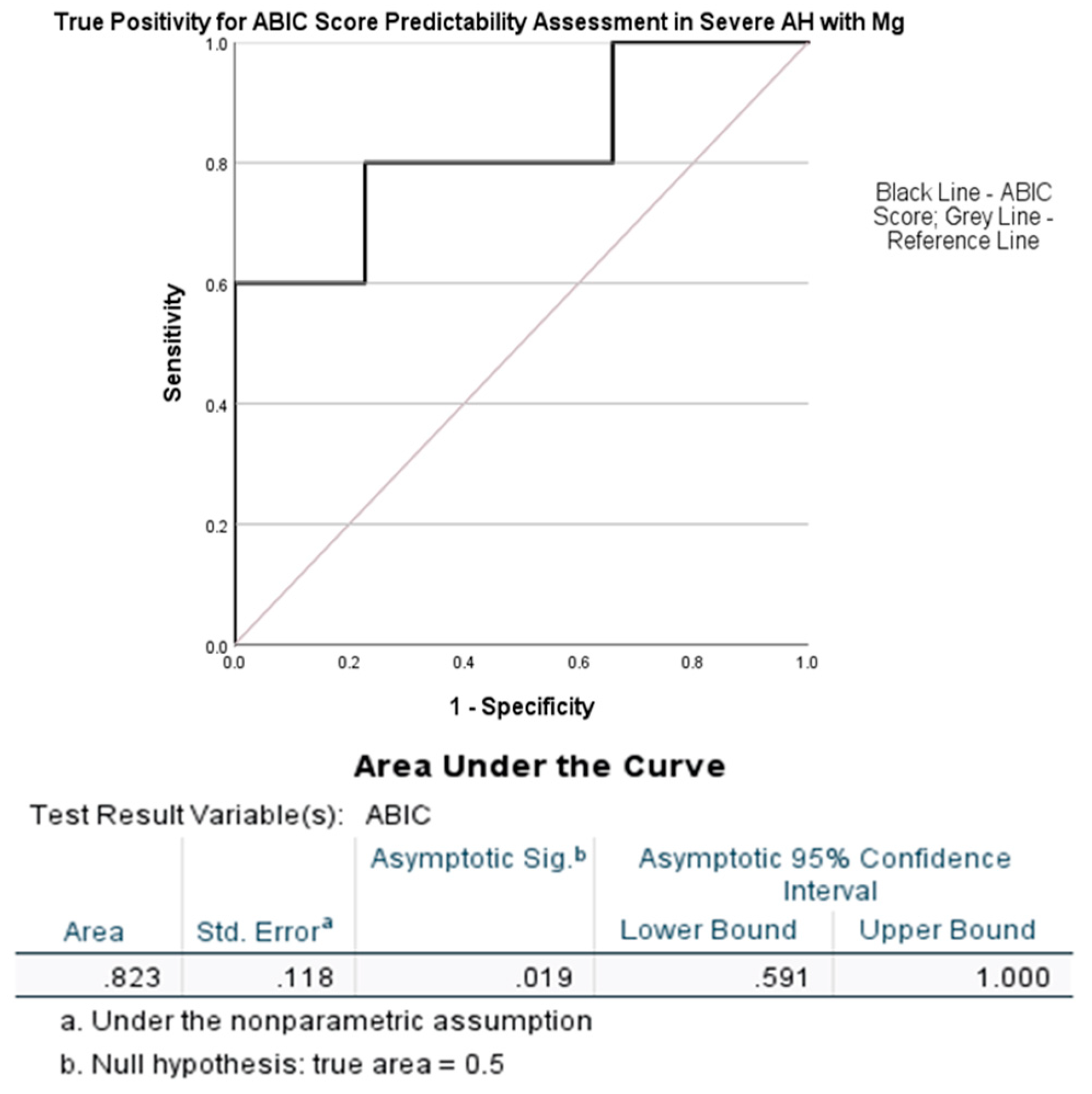
3.2. Analysis of Liver Injury and Severity Based on Specificity and Sensitivity of Serum Magnesium
3.2.1. Demographics and Drinking History
3.2.2. Liver Injury Markers
3.2.3. Liver Disease Severity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AH | Alcohol-associated hepatitis |
| AUD | Alcohol use disorder |
| AUDIT | Alcohol use disorders identification test |
| CS | Clinically significant |
| LTDH | Lifetime drinking history |
| NCS | Clinically non-significant |
| ABIC | Algorithm made from age, serum bilirubin, INR, and serum creatinine |
| serum ALT | Alanine aminotransferase |
| serum AST | Aspartate aminotransferase |
| AUROC | Area under the receiver operating characteristics |
| SM | Serum magnesium |
| SOC | Standard of care |
References
- Gala, K.S.; Vatsalya, V. Emerging noninvasive biomarkers, and medical management strategies for alcoholic hepatitis: Present understanding and scope. Cells 2020, 9, 524. [Google Scholar] [CrossRef]
- Crabb, D.W.; Bataller, R.; Chalasani, N.P.; Kamath, P.S.; Lucey, M.; Mathurin, P.; McClain, C.; McCullough, A.; Mitchell, M.C.; Morgan, T.R.; et al. Standard definitions and common data elements for clinical trials in patients with alcoholic hepatitis: Recommendation from the NIAAA Alcoholic Hepatitis Consortia. Gastroenterology 2016, 150, 785–790. [Google Scholar] [CrossRef]
- Vatsalya, V.; Gala, K.S.; Mishra, M.; Schwandt, M.L.; Umhau, J.; Cave, M.C.; Parajuli, D.; Ramchandani, V.A.; McClain, C.J. Lower serum magnesium concentrations are associated with specific heavy drinking markers, pro-inflammatory response and early-stage alcohol-associated liver injury. Alcohol Alcohol. 2020, 55, 164–170. [Google Scholar] [CrossRef]
- Elisaf, M.; Merkouropoulos, M.; Tsianos, E.; Siamopoulos, K. Pathogenetic mechanisms of hypomagnesemia in alcoholic patients. J. Trace Elem. Med. Biol. 1995, 9, 210–214. [Google Scholar] [CrossRef]
- Grochowski, C.; Blicharska, E.; Baj, J.; Mierzwińska, A.; Brzozowska, K.; Forma, A.; Maciejewski, R. Serum iron, magnesium, copper, and manganese levels in alcoholism: A systematic review. Molecules 2019, 24, 1361. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Yang, H.; Mao, Y. Magnesium and liver disease. Ann. Transl. Med. 2019, 7, 578. [Google Scholar] [CrossRef]
- Winrich, E.J.; Gala, K.S.; Rajhans, A.; Rios-Perez, C.D.; Royer, A.J.; Zamani, Z.; Parthasarathy, R.; Marsano-Obando, L.S.; Barve, A.J.; Schwandt, M.L.; et al. Association of Hypomagnesemia and Liver Injury, Role of Gut-Barrier Dysfunction and Inflammation: Efficacy of Abstinence, and 2-Week Medical Management in Alcohol Use Disorder Patients. Int. J. Mol. Sci. 2022, 23, 11332. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhu, X.; Fan, L.; Kabagambe, E.K.; Song, Y.; Tao, M.; Zhong, X.; Hou, L.; Shrubsole, M.J.; Liu, J.; et al. Magnesium intake and mortality due to liver diseases: Results from the Third National Health and Nutrition Examination Survey Cohort. Sci. Rep. 2017, 7, 17913. [Google Scholar] [CrossRef] [PubMed]
- Tangvoraphonkchai, K.; Davenport, A. Magnesium and cardiovascular disease. Adv. Chronic Kidney Dis. 2018, 25, 251–260. [Google Scholar] [CrossRef]
- He, L.; Vatsalya, V.; Ma, X.; Zhang, J.; Yin, X.; Kim, S.; Feng, W.; McClain, C.J.; Zhang, X. Metabolic profiling of bile acids in urine of patients with acute alcohol associated hepatitis. Hepatology 2020, 72 (Suppl. S1), 176A–177A. [Google Scholar]
- Vatsalya, V.; Cave, M.C.; Kong, M.; Gobejishvili, L.; Falkner, K.C.; Craycroft, J.; Mitchell, M.; Szabo, G.; McCullough, A.; Dasarathy, S.; et al. Keratin 18 is a diagnostic and prognostic factor for acute alcoholic hepatitis. Clin. Gastroenterol. Hepatol. 2020, 18, 2046–2054. [Google Scholar] [CrossRef]
- Vatsalya, V.; Kong, M.; Gobejishvili, L.; Chen, W.Y.; Srivastava, S.; Barve, S.; McClain, C.J.; Joshi-Barve, S. Urinary acrolein metabolite levels in severe acute alcoholic hepatitis patients. Am. J. Physiol.-Gastrointest. Liver Physiol. 2019, 316, G115–G122. [Google Scholar] [CrossRef]
- Zhou, Y.; Vatsalya, V.; Gobejishvili, L.; Lamont, R.J.; McClain, C.J.; Feng, W. Porphyromonas gingivalis as a possible risk factor in the development/severity of acute alcoholic hepatitis. Hepatol. Commun. 2019, 3, 293–304. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; De la Fuente, J.R.; Grant, M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Skinner, H.A.; Sheu, W.J. Reliability of alcohol use indices. The Lifetime Drinking History and the MAST. J. Stud. Alcohol 1982, 43, 1157–1170. [Google Scholar] [CrossRef]
- Maddrey, W.C.; Boitnott, J.K.; Bedine, M.S.; Weber, F.L., Jr.; Mezey, E.; White, R.I., Jr. Corticosteroid therapy of alcoholic hepatitis. Gastroenterology 1978, 75, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Kim, W.R. The model for end-stage liver disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef]
- Dominguez, M.; Rincón, D.; Abraldes, J.G.; Miquel, R.; Colmenero, J.; Bellot, P.; Joan-Carles, G.-P.; Rosamelia, F.; Montserrat, M.; Rafael, B.; et al. A new scoring system for prognostic stratification of patients with alcoholic hepatitis. Am. J. Gastroenterol. 2008, 103, 2747–2756. [Google Scholar] [CrossRef] [PubMed]
- Louvet, A.; Naveau, S.; Abdelnour, M.; Ramond, M.J.; Diaz, E.; Fartoux, L.; Dharancy, S.; Texier, F.; Hollebecque, A.; Serfaty, L.; et al. The Lille model: A new tool for therapeutic strategy in patients with severe alcoholic hepatitis treated with steroids. Hepatology 2007, 45, 1348–1354. [Google Scholar] [CrossRef]
- Musso, C.G. Magnesium metabolism in health and disease. Int. Urol. Nephrol. 2009, 41, 357–362. [Google Scholar] [CrossRef]
- McClain, C.J.; Marsano, L.; Burk, R.F.; Bacon, B. Trace metals in liver disease. In Seminars in Liver Disease; Thieme Medical Publishers, Inc.: New York, NY, USA, 1991; Volume 11, pp. 321–339. [Google Scholar]
- Pasqualetti, P.; Casale, R.; Colantonio, D.; Di Lauro, G.; Festuccia, V.; Natali, L.; Natali, G. Serum levels of magnesium in hepatic cirrhosis. Quad. Sclavo Diagn. Clin. Lab. 1987, 23, 12–17. [Google Scholar]
- Vandemergel, X.; Simon, F. Evolution of metabolic abnormalities in alcoholic patients during withdrawal. J. Addict. 2015, 2015, 541536. [Google Scholar] [CrossRef]
- Shane, S.; Flink, E. Magnesium deficiency in alcohol addiction and withdrawal. Magnes. Trace Elem. 1991, 10, 263–268. [Google Scholar]
- Dyer, S.A.; Sampson, H.W. Magnesium levels in alcohol-treated rodents using different consumption paradigms. Alcohol 1998, 16, 195–199. [Google Scholar] [CrossRef]
- Adachi, M.; Brenner, D.A. Clinical syndromes of alcoholic liver disease. Dig. Dis. 2005, 23, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Stankovic, M.S.; Janjetovic, K.; Velimirovic, M.; Milenkovic, M.; Stojkovic, T.; Puskas, N.; Zaletel, I.; De Luka, S.R.; Jankovic, S.; Stefanovic, S.; et al. Effects of IL-33/ST2 pathway in acute inflammation on tissue damage, antioxidative parameters, magnesium concentration and cytokines profile. Exp. Mol. Pathol. 2016, 101, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Rayssiguier, Y.; Mazur, A. Magnesium and inflammation: Lessons from animal models. Clin. Calcium 2005, 15, 245–248. [Google Scholar] [PubMed]
- Elin, R.J. Magnesium metabolism in health and disease. Disease-a-Month 1988, 34, 166–218. [Google Scholar] [CrossRef]
- Romani, A.; Marfella, C.; Scarpa, A. Cell magnesium transport and homeostasis: Role of intracellular compartments. Miner. Electrolyte Metab. 1993, 19, 282–289. [Google Scholar]
- Bois, P.; Gascon, A.; Beaulnes, A. Histamine-liberating effect of magnesium deficiency in the rat. Nature 1963, 197, 501–502. [Google Scholar] [CrossRef]
- Panov, A.; Scarpa, A. Mg2+ control of respiration in isolated rat liver mitochondria. Biochemistry 1996, 35, 12849–12856. [Google Scholar] [CrossRef] [PubMed]
- Jahnen-Dechent, W.; Ketteler, M. Magnesium basics. Clin. Kidney J. 2012, 5 (Suppl. S1), i3–i14. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; O’Keefe, J.H.; Wilson, W. Subclinical magnesium deficiency: A principal driver of cardiovascular disease and a public health crisis. Open Heart 2018, 5, e000668. [Google Scholar] [CrossRef]
- Dhand, A. Neurologic Complications of Electrolyte Disturbances. In SPEC Aminoff’s Neurology and General Medicine eBook, 6th ed.; Academic Press Inc.: Cambridge, MA, USA, 2021; Volume 273. [Google Scholar]
- Randall, R.E., Jr.; Coheen, M.D.; Spray, C.C., Jr.; Rossmeisl, E.C. Hypermagnesemia in renal failure: Etiology and toxic manifestations. Ann. Intern. Med. 1964, 6, 73–88. [Google Scholar] [CrossRef]
- Markiewicz-Górka, I.; Zawadzki, M.; Januszewska, L.; Hombek-Urban, K.; Pawlas, K. Influence of selenium and/or magnesium on alleviation alcohol induced oxidative stress in rats, normalization function of liver and changes in serum lipid parameters. Hum. Exp. Toxicol. 2011, 30, 1811–1827. [Google Scholar] [CrossRef] [PubMed]
- El-Tantawy, W.H.; Sabry, D.; Abd Al Haleem, E.N. Comparative study of antifibrotic activity of some magnesium-containing supplements on experimental liver toxicity. Molecular study. Drug Chem. Toxicol. 2017, 40, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Poikolainen, K.; Alho, H. Magnesium treatment in alcoholics: A randomized clinical trial. Subst. Abus. Treat. Prev. Policy 2008, 3, 1. [Google Scholar] [CrossRef]
- Eshraghian, A.; Nikeghbalian, S.; Geramizadeh, B.; Malek-Hosseini, S.A. Serum magnesium concentration is independently associated with non-alcoholic fatty liver and non-alcoholic steatohepatitis. United Eur. Gastroenterol. J. 2018, 6, 97–103. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measures | Group 1 (Mild AH; MELD < 12) | Group 2 (Moderate AH; MELD ≥ 12 and ≤19) | Group 3 (Severe AH; MELD > 19) | Between Group p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Males (n = 3; 6.12%) | Females (n = 2; 4.08%) | Total (n = 5; 10.20%) | Males (n = 9; 18.37%) | Females (n = 4; 8.16%) | Total (n = 13; 26.53%) | Males (n = 21; 42.86%) | Females (n = 10; 20.41%) | Total (n = 31; 63.27%) | ||
| Demographic Data | ||||||||||
| Age (years) | 59.0 ± 2.2 | 52.5 ± 13.5 | 56.40 ± 9.27 | 49.4 ± 6.9 | 48.3 ± 7.1 | 49.1 ± 7.0 | 47.5 ± 10.8 | 42.3 ± 8.8 | 45.8 ± 10.5 | 0.083 |
| BMI (kg/m2) | 29.8 ± 6.2 | 27.1 ± 5.1 | 28.7 ± 5.9 | 30.2 ± 7.7 | 27.9 ± 5.7 | 29.5 ± 7.2 | 29.6 ± 6.13 | 25.3 ± 6.8 | 28.2 ± 6.6 | 0.854 |
| Drinking History | ||||||||||
| AUDIT | 22.7 ± 13.0 | 15.5 ± 2.5 | 19.8 ± 10.8 | 22.4 ± 7.1 | 20.3 ± 8.6 | 21.8 ± 7.6 | 21.9 ± 8.0 | 23.9 ± 6.8 | 22.5 ± 7.7 | 0.787 |
| LTDH a | 41.3 ± 3.1 | 32.5 ± 11.5 | 37.8 ± 8.8 | 25.1 ± 7.5 | 16.3 ± 9.0 | 22.9 ± 8.8 | 22.8 ± 12.3 | 25.3 ± 9.0 | 23.6 ± 11.4 | 0.028 |
| Serum Magnesium Level | ||||||||||
| Magnesium (mmol/L) | 0.65 ± 0.033 | 0.68 ± 0.028 | 0.66 ± 0.032 | 0.59 ± 0.080 | 0.63 ± 0.033 | 0.60 ± 0.071 | 0.70 ± 0.129 | 0.65 ± 0.067 | 0.68 ± 0.115 | 0.056 |
| Markers of Liver Injury | ||||||||||
| Bilirubin (mg/dL) | 1.40 ± 0.26 | 2.00 ± 0.57 | 1.64 ± 0.47 | 7.51 ± 5.50 | 4.43 ± 0.85 | 6.56 ± 4.75 | 16.47 ± 8.07 | 12.57 ± 7.06 | 15.21 ± 7.86 | <0.001 |
| ALT (IU/L) | 46.3 ± 14.7 | 38.5 ± 1.5 | 43.2 ± 12.0 | 108.9 ± 45.6 | 28.8 ± 10.2 | 84.2 ± 53.3 | 53.0 ± 53.2 | 40.9 ± 22.5 | 49.1 ± 46.0 | 0.655 |
| AST (IU/L) | 84.0 ± 29.4 | 88.0 ± 22.0 | 85.6 ± 26.8 | 206.6 ± 97.8 | 104.8 ± 24.4 | 175.2 ± 94.4 | 198.8 ± 278.3 | 113.1 ± 57.3 | 171.2 ± 234.7 | 0.072 |
| AST:ALT | 1.81 ± 0.17 | 2.27 ± 0.46 | 1.99 ± 0.40 | 2.08 ± 1.25 | 4.21 ± 1.94 | 2.74 ± 1.79 | 3.59 ± 1.41 | 3.25 ± 1.50 | 3.48 ± 1.44 | 0.083 |
| Liver Severity Scores | ||||||||||
| MELD | 8.7 ± 0.5 | 9.0 ± 1.0 | 8.8 ± 0.75 | 15.3 ± 2.9 | 17.8 ± 1.6 | 16.1 ± 2.8 | 26.9 ± 5.7 | 25.1 ± 5.0 | 26.3 ± 5.51 | N/A |
| Maddrey’s DF | −3.0 ± 1.3 | 4.3 ± 0.4 | −0.1 ± 3.7 | 18.9 ± 24.5 | 28.4 ± 11.3 | 21.8 ± 21.8 | 74.5 ± 50.5 | 63.7 ± 19.8 | 71.0 ± 43.4 | <0.001 |
| Child Pugh Score | 5.6 ± 0.5 | 6.5 ± 1.5 | 6.0 ± 1.1 | 8.9 ± 1.5 | 9.5 ± 0.9 | 9.1 ± 1.4 | 10.9 ± 1.1 | 11.1 ± 1.4 | 11.0 ± 1.2 | <0.001 |
| ABIC Score | 7.13 ± 0.23 | 6.52 ± 2.01 | 6.89 ± 1.07 | 6.77 ± 0.79 | 6.71 ± 0.93 | 6.75 ± 0.79 | 8.27 ± 1.43 | 7.25 ± 1.14 | 7.94 ± 1.41 | 0.012 |
| Lille Score b | 0.93 ± N/A | N/A ± N/A | 0.93 ± N/A | 0.80 ± 0.20 | 0.83 ± 0.08 | 0.81 ± 0.17 | 0.89 ± 0.20 | 0.72 ± 0.29 | 0.83 ± 0.24 | 0.890 |
| Measures | Group 4 (Patients with Mg ≥ 0.78 mmol/L) | Group 5 (Patients with Mg < 0.78 mmol/L) | Between Group p-Value | ||||
|---|---|---|---|---|---|---|---|
| Males (n = 5; 10.20%) | Females (n = 0; 0%) | Total (n = 5; 10.20%) | Males (n = 28; 57.14%) | Females (n = 16; 32.65%) | Total (n = 44; 89.80%) | ||
| Demographic Data | |||||||
| Age (years) | 44 ± 4 | N/A | 44 ± 4 | 50 ± 11 | 45 ± 10 | 48 ± 11 | 0.339 |
| BMI (kg/m2) | 29.84 ± 8.50 | N/A | 29.84 ± 8.50 | 29.77 ± 6.52 | 26.17 ± 6.62 | 28.46 ± 6.71 | 0.672 |
| Drinking History | |||||||
| AUDIT | 23.30 ± 10.47 | N/A | 23.30 ± 10.47 | 21.89 ± 8.31 | 21.94 ± 7.71 | 21.91 ± 8.00 | 0.741 |
| LTDH a | 20.80 ± 8.50 | N/A | 20.80 ± 8.50 | 26.04 ± 12.47 | 24.43 ± 11.00 | 25.59 ± 11.87 | 0.399 |
| Serum Magnesium Level | |||||||
| Magnesium (mmol/L) | 0.89 ± 0.083 | N/A | 0.89 ± 0.083 | 0.63 ± 0.075 | 0.65 ± 0.057 | 0.63 ± 0.069 | N/A |
| Markers of Liver Injury | |||||||
| Bilirubin (mg/dL) | 22.58 ± 10.38 | N/A | 22.58 ± 10.38 | 10.88 ± 7.35 | 9.21 ± 7.11 | 10.28 ± 7.23 | 0.001 |
| ALT (IU/L) | 43.80 ± 12.64 | N/A | 43.80 ± 12.64 | 71.86 ± 59.65 | 37.56 ± 19.81 | 59.39 ± 51.47 | 0.507 |
| AST (IU/L) | 150.80 ± 35.74 | N/A | 150.80 ± 35.74 | 197.57 ± 253.72 | 107.87 ± 49.83 | 164.95 ± 207.83 | 0.881 |
| AST:ALT | 3.55 ± 0.90 | N/A | 3.55 ± 0.90 | 2.92 ± 1.61 | 3.37 ± 1.70 | 3.08 ± 1.64 | 0.532 |
| Liver Severity Scores | |||||||
| MELD | 33.40 ± 8.26 | N/A | 33.40 ± 8.26 | 20.07 ± 6.55 | 21.25 ± 7.09 | 20.50 ± 6.70 | <0.001 |
| Maddrey’s DF | 116.19 ± 89.66 | N/A | 116.19 ± 89.66 | 40.84 ± 34.62 | 47.45 ± 28.57 | 43.24 ± 32.37 | <0.001 |
| Child Pugh Score | 10.80 ± 1.10 | N/A | 10.80 ± 1.10 | 9.71 ± 2.11 | 10.13 ± 2.09 | 9.86 ± 2.09 | 0.331 |
| ABIC Score | 9.27 ± 1.76 | N/A | 9.27 ± 1.76 | 7.49 ± 1.15 | 7.02 ± 1.15 | 7.32 ± 1.15 | 0.001 |
| Lille Score b | 0.93 ± 0.10 | N/A | 0.93 ± 0.10 | 0.85 ± 0.21 | 0.74 ± 0.26 | 0.81 ± 0.23 | 0.398 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winrich, E.J.; Tiwari, H.; Gala, K.S.; Royer, A.J.; Parajuli, D.; Vatsalya, V. Characterization of Hypomagnesemia in Alcoholic Hepatitis Patients and Its Association with Liver Injury and Severity Markers. J. Clin. Med. 2023, 12, 2968. https://doi.org/10.3390/jcm12082968
Winrich EJ, Tiwari H, Gala KS, Royer AJ, Parajuli D, Vatsalya V. Characterization of Hypomagnesemia in Alcoholic Hepatitis Patients and Its Association with Liver Injury and Severity Markers. Journal of Clinical Medicine. 2023; 12(8):2968. https://doi.org/10.3390/jcm12082968
Chicago/Turabian StyleWinrich, Evan J., Harsh Tiwari, Khushboo S. Gala, Amor J. Royer, Dipendra Parajuli, and Vatsalya Vatsalya. 2023. "Characterization of Hypomagnesemia in Alcoholic Hepatitis Patients and Its Association with Liver Injury and Severity Markers" Journal of Clinical Medicine 12, no. 8: 2968. https://doi.org/10.3390/jcm12082968
APA StyleWinrich, E. J., Tiwari, H., Gala, K. S., Royer, A. J., Parajuli, D., & Vatsalya, V. (2023). Characterization of Hypomagnesemia in Alcoholic Hepatitis Patients and Its Association with Liver Injury and Severity Markers. Journal of Clinical Medicine, 12(8), 2968. https://doi.org/10.3390/jcm12082968