
Electrophysiological and Imaging Biomarkers to Evaluate Exercise Training in Patients with Neuromuscular Disease: A Systematic Review


Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
- (1)
- The patients studied had a confirmed diagnosis of neuromuscular disease (we excluded patients with diagnoses of diabetic neuropathies, compression, or entrapment neuropathies,, radiculopathy, thoracic outlet syndrome, or complex regional pain syndrome).
- (2)
- The study involved a longitudinal exercise intervention of more than 6 weeks, the minimal period for neural adaptations.
- (3)
- The key outcomes were measured by MRI, MRS, sEMG, ultrasound, or NIRS.
- (4)
- The study included a comparison with non-exercise intervention controls within NMD patients, and/or a comparison before and after the intervention within NMD patients, and/or a comparison with healthy controls.
2.2. Search Strategy
2.3. Study Selection and Data Extraction
- Method: date of the study and study type.
- Participants: number, age, gender, disease, and baseline characteristics.
- Interventions: intervention (frequency, intensity, type, time), comparison, concomitant treatments, and excluded treatments.
- Outcomes: primary and secondary outcomes specified and collected, and time points. p-values were provided when given.
2.4. Risk of Bias
2.5. Best Evidence Synthesis
3. Results
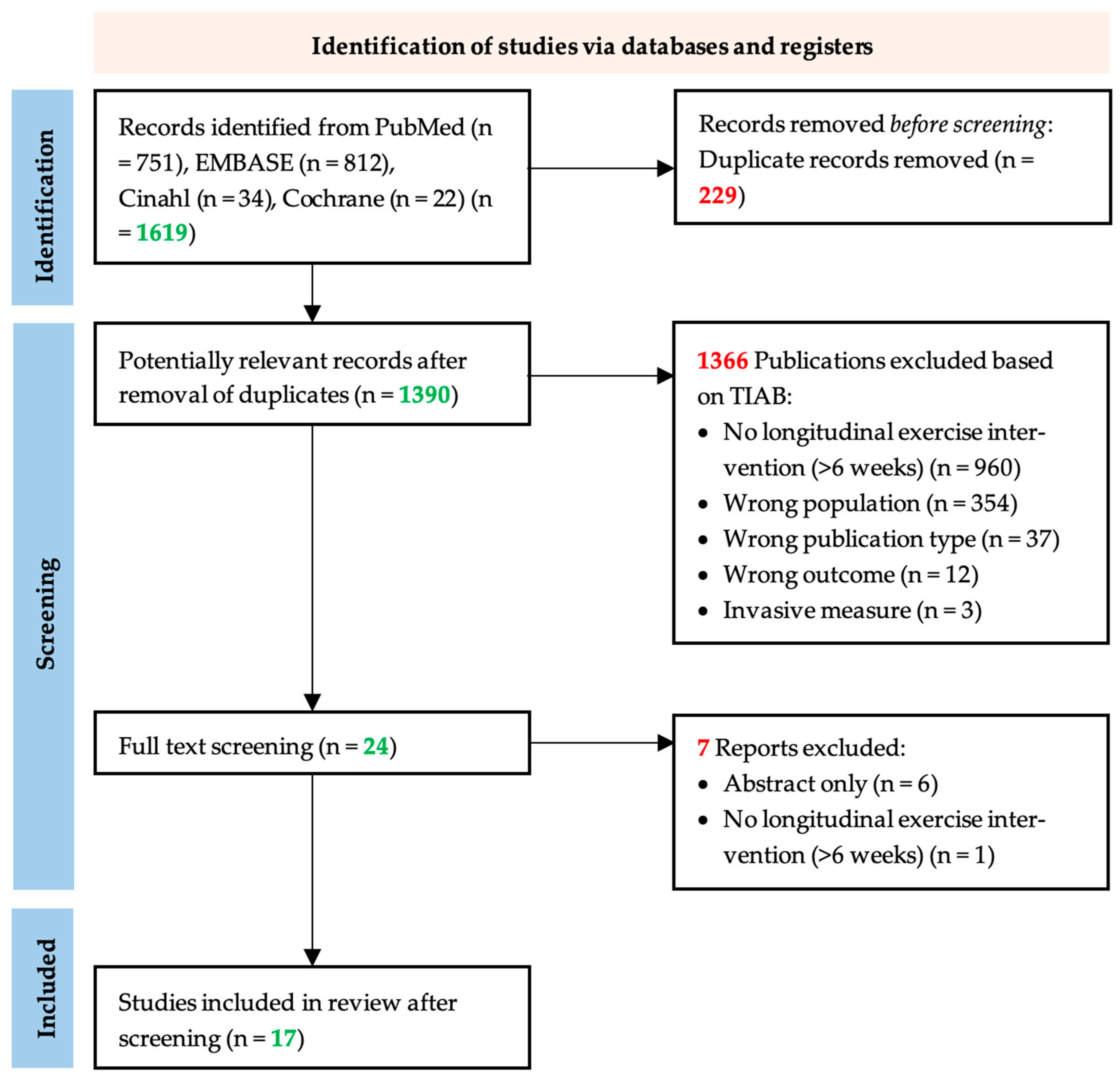
3.1. Study Selection
3.2. Study Characteristics and Quality Assessment
3.3. Exercise Intervention Characteristics
3.4. Best Evidence Synthesis
3.4.1. Biomarkers Measured by MRI
3.4.2. Biomarkers Measured by MRS
3.4.3. Biomarkers Measured by EMG
3.4.4. Biomarkers Measured by Ultrasound
3.4.5. Biomarkers Measured by NIRS
3.5. Quality of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Holloszy, J.O.; Coyle, E.F. Adaptations of skeletal muscle to endurance exercise and their metabolic consequences. J. Appl. Physiol. 1984, 56, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Saltin, B. Physiological adaptation to physical conditioning: Old problems revisited. Acta Medica Scand. 1986, 220, 11–24. [Google Scholar] [CrossRef]
- Cox, M.H. Exercise training programs and cardiorespiratory adaptation. Clin. Sports Med. 1991, 10, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, J. Effects of physical training on the metabolism of skeletal muscle. Diabetes Care 1992, 15, 1701–1711. [Google Scholar] [CrossRef]
- Neufer, P.D. The effect of detraining and reduced training on the physiological adaptations to aerobic exercise training. Sports Med. 1989, 8, 302–320. [Google Scholar] [CrossRef] [PubMed]
- Boutcher, S.H. High-intensity intermittent exercise and fat loss. J. Obes. 2011, 2011, 868305. [Google Scholar] [CrossRef]
- Rhea, M.R.; Oliverson, J.R.; Marshall, G.; Peterson, M.D.; Kenn, J.G.; Ayllón, F.N. Noncompatibility of Power and Endurance Training Among College Baseball Players. J. Strength Cond. Res. 2008, 22, 230–234. [Google Scholar] [CrossRef]
- Folland, J.P.; Williams, A.G. The adaptations to strength training: Morphological and neurological contributions to increased strength. Sports Med. 2007, 37, 145–168. [Google Scholar] [CrossRef]
- Gabriel, D.A.; Kamen, G.; Frost, G. Neural adaptations to resistive exercise: Mechanisms and recommendations for training practices. Sports Med. 2006, 36, 133–149. [Google Scholar] [CrossRef] [PubMed]
- Legerlotz, K.; Marzilger, R.; Bohm, S.; Arampatzis, A. Physiological Adaptations following Resistance Training in Youth Athletes—A Narrative Review. Pediatr. Exerc. Sci. 2016, 28, 501–520. [Google Scholar] [CrossRef]
- Stefanetti, R.J.; Blain, A.; Jimenez-Moreno, C.; Errington, L.; Ng, Y.S.; McFarland, R.; Turnbull, D.M.; Newman, J.; Gorman, G.S. Measuring the effects of exercise in neuromuscular disorders: A systematic review and meta-analyses. Wellcome Open Res. 2020, 5, 84. [Google Scholar] [CrossRef] [PubMed]
- Habets, L.E.; Bartels, B.; Asselman, F.-L.; Hooijmans, M.T.; Berg, S.v.D.; Nederveen, A.J.; van der Pol, W.L.; Jeneson, J.A.L. Magnetic resonance reveals mitochondrial dysfunction and muscle remodelling in spinal muscular atrophy. Brain 2022, 145, 1422–1435. [Google Scholar] [CrossRef] [PubMed]
- Habets, L.E.; Bartels, B.; Asselman, F.-L.; Hulzebos, E.H.; Stegeman, D.F.; Jeneson, J.A.; van der Pol, W.L. Motor Unit and Capillary Recruitment During Fatiguing Arm-Cycling Exercise in Spinal Muscular Atrophy Types 3 and 4. J. Neuromuscul. Dis. 2022, 9, 397–409. [Google Scholar] [CrossRef] [PubMed]
- Beretta-Piccoli, M.; Boccia, G.; Ponti, T.; Clijsen, R.; Barbero, M.; Cescon, C. Relationship between Isometric Muscle Force and Fractal Dimension of Surface Electromyogram. BioMed Res. Int. 2018, 2018, 846. [Google Scholar] [CrossRef]
- Beretta-Piccoli, M.; Calanni, L.; Negro, M.; Ricci, G.; Bettio, C.; Barbero, M.; Berardinelli, A.; Siciliano, G.; Tupler, R.; Soldini, E.; et al. Increased resistance towards fatigability in patients with facioscapulohumeral muscular dystrophy. Eur. J. Appl. Physiol. 2021, 121, 1617–1629. [Google Scholar] [CrossRef]
- Moreira, A.L.; Mendonça, R.H.; Polido, G.J.; Oliveira, M.C.B.; Silva, A.M.S.; Zanoteli, E. Muscle Ultrasound Changes Correlate With Functional Impairment in Spinal Muscular Atrophy. Ultrasound Med. Biol. 2023, 49, 1569–1574. [Google Scholar] [CrossRef]
- Katti, G.; Ara, S.A.; Shireen, A. Magnetic resonance imaging (MRI)–A review. Int. J. Dent. Clin. 2011, 3, 65–70. [Google Scholar]
- Cox, I. Development and applications of in vivo clinical magnetic resonance spectroscopy. Prog. Biophys. Mol. Biol. 1996, 65, 45–81. [Google Scholar] [CrossRef]
- Argov, Z.; Bank, W.J. Phosphorus magnetic resonance spectroscopy (31P MRS) in neuromuscular disorders. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 1991, 30, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Pilkar, R.; Momeni, K.; Ramanujam, A.; Ravi, M.; Garbarini, E.; Forrest, G.F. Use of Surface EMG in Clinical Rehabilitation of Individuals With SCI: Barriers and Future Considerations. Front. Neurol. 2020, 11, 578559. [Google Scholar] [CrossRef]
- Garcia, M.C.; Vieira, T. Surface electromyography: Why, when and how to use it. Rev. Andal. Med. Deporte 2011, 4, 17–28. [Google Scholar]
- Boushel, R.; Langberg, H.; Olesen, J.; Gonzales-Alonzo, J.; Bülow, J.; Kjaer, M. Monitoring tissue oxygen availability with near infrared spectroscopy (NIRS) in health and disease. Scand. J. Med. Sci. Sports 2001, 11, 213–222. [Google Scholar] [CrossRef]
- Morrison, B.M. Neuromuscular diseases. Semin. Neurol. 2016, 36, 409–418. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.M. Physical Activity, Health Impairments, and Disability in Neuromuscular Disease. Am. J. Phys. Med. Rehabil. 2002, 81, S108–S120. [Google Scholar] [CrossRef] [PubMed]
- Voet, N.B. Exercise in neuromuscular disorders: A promising intervention. Acta Myol. 2019, 38, 207. [Google Scholar] [PubMed]
- Janssen, B.; Voet, N.; Geurts, A.; van Engelen, B.; Heerschap, A. Quantitative MRI reveals decelerated fatty infiltration in muscles of active FSHD patients. Neurology 2016, 86, 1700–1707. [Google Scholar] [CrossRef]
- Pino, M.G.; Rich, K.A.; Kolb, S.J. Update on Biomarkers in Spinal Muscular Atrophy. Biomark. Insights 2021, 16, 643. [Google Scholar] [CrossRef]
- Fischmann, A.; Fischer, D. Neuromuscular imaging in muscular dystrophies and other muscle diseases. Imaging Med. 2013, 5, 237. [Google Scholar] [CrossRef]
- Higgins, J.P.; Sterne, J.; Savovic, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10, 29–31. [Google Scholar]
- SSterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Page, M.J.; Bountron, I.; Hoffman, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.; Akl, E.A.; Brennan, S.E.; Moher, D.; Chou, R.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 372. [Google Scholar] [CrossRef] [PubMed]
- Rahbek, M.A.; Mikkelsen, E.E.; Overgaard, K.; Vinge, L.; Andersen, H.; Dalgas, U. Exercise in myasthenia gravis: A feasibility study of aerobic and resistance training. Muscle Nerve 2017, 56, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Bulut, N.; Karaduman, A.; Alemdaroğlu-Gürbüz, İ.; Yılmaz, Ö.; Topaloğlu, H.; Özçakar, L. The effect of aerobic training on motor function and muscle architecture in children with Duchenne muscular dystrophy: A randomized controlled study. Clin. Rehabil. 2022, 36, 1062–1071. [Google Scholar] [CrossRef]
- Chung, Y.-L.; Alexanderson, H.; Pipitone, N.; Morrison, C.; Dastmalchi, M.; Ståhl-Hallengren, C.; Richards, S.; Thomas, E.L.; Hamilton, G.; Bell, J.D.; et al. Creatine supplements in patients with idiopathic inflammatory myopathies who are clinically weak after conventional pharmacologic treatment: Six-month, double-blind, randomized, placebo-controlled trial. Arthritis Rheum. 2007, 57, 694–702. [Google Scholar] [CrossRef]
- Burns, J.; Sman, A.D.; Cornett, K.M.D.; Wojciechowski, E.; Walker, T.; Menezes, M.P.; Mandarakas, M.R.; Rose, K.J.; Bray, P.; Sampaio, H.; et al. Safety and efficacy of progressive resistance exercise for Charcot-Marie-Tooth disease in children: A randomised, double-blind, sham-controlled trial. Lancet Child Adolesc. Heal. 2017, 1, 106–113. [Google Scholar] [CrossRef]
- Taivassalo, T.; De Stefano, N.; Chen, J.; Karpati, G.; Arnold, D.; Argov, Z. Short-term aerobic training response in chronic myopathies. Muscle Nerve 1999, 22, 1239–1243. [Google Scholar] [CrossRef]
- Alexanderson, H.; Stenström, C.H.; Jenner, G.; Lundberg, I. The safety of a resistive home exercise program in patients with recent onset active polymyositis or dermatomyositis. Scand. J. Rheumatol. 2000, 29, 295–301. [Google Scholar]
- Alexanderson, H.; Stenström, C.H.; Lundberg, I. Safety of a home exercise programme in patients with polymyositis and dermatomyositis: A pilot study. Rheumatology 1999, 38, 608–611. [Google Scholar] [CrossRef]
- Spector, S.A.; Gordon, P.L.; Feuerstein, I.M.; Sivakumar, K.; Hurley, B.F.; Dalakas, M.C. Strength gains without muscle injury after strength training in patients with postpolio muscular atrophy. Muscle Nerve 1996, 19, 1282–1290. [Google Scholar] [CrossRef]
- Taivassalo, T.; De Stefano, N.; Argov, Z.; Matthews, P.M.; Chen, J.; Genge, A.; Karpati, G.; Arnold, D.L. Effects of aerobic training in patients with mitochondrial myopathies. Neurology 1998, 50, 1055–1060. [Google Scholar] [CrossRef]
- Tollbäck, A.; Eriksson, S.; Wredenberg, A.; Jenner, G.; Vargas, R.; Borg, K.; Ansved, T. Effects of high resistance training in patients with myotonic dystrophy. Scand. J. Rehabil. Med. 1999, 31, 9–16. [Google Scholar]
- Taivassalo, T.; Shoubridge, E.A.; Chen, J.; Kennaway, N.G.; DiMauro, S.; Arnold, D.L.; Haller, R.G. Aerobic conditioning in patients with mitochondrial myopathies: Physiological, biochemical, and genetic effects. Ann. Neurol. 2001, 50, 133–141. [Google Scholar] [CrossRef]
- Trenell, M.I.; Sue, C.M.; Kemp, G.J.; Sachinwalla, T.; Thompson, C.H. Aerobic exercise and muscle metabolism in patients with mitochondrial myopathy. Muscle Nerve 2006, 33, 524–531. [Google Scholar] [CrossRef]
- El Mhandi, L.; Millet, G.Y.; Calmels, P.; Richard, A.; Oullion, R.; Gautheron, V.; Féasson, L. Benefits of interval-training on fatigue and functional capacities in Charcot–Marie–Tooth disease. Muscle Nerve 2008, 37, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Porcelli, S.; Marzorati, M.; Morandi, L.; Grassi, B. Home-based aerobic exercise training improves skeletal muscle oxidative metabolism in patients with metabolic myopathies. J. Appl. Physiol. 2016, 121, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Westerberg, E.; Molin, C.J.; Ness, S.S.; Widenfalk, J.; Punga, A.R. The impact of physical exercise on neuromuscular function in Myasthenia gravis patients: A single-subject design study. Medicine 2018, 97, e11510. [Google Scholar] [CrossRef] [PubMed]
- Lott, D.J.; Taivassalo, T.; Cooke, K.D.; Park, H.; Moslemi, Z.; Batra, A.; Forbes, S.C.; Byrne, B.J.; Walter, G.A.; Vandenborne, K. Safety, feasibility, and efficacy of strengthening exercise in Duchenne muscular dystrophy. Muscle Nerve 2021, 63, 320–326. [Google Scholar] [CrossRef]
- Voet, N.B.; van der Kooi, E.L.; van Engelen, B.G.; Geurts, A.C. Strength training and aerobic exercise training for muscle disease. Cochrane Database Syst. Rev. 2019, 12, CD003907. [Google Scholar] [CrossRef]
- Hoppeler, H.; Baum, O.; Lurman, G.; Mueller, M. Molecular mechanisms of muscle plasticity with exercise. Compr. Physiol. 2011, 1, 1383–1412. [Google Scholar] [PubMed]
- Schoenfeld, B.J. The mechanisms of muscle hypertrophy and their application to resistance training. J. Strength Cond. Res. 2010, 24, 2857–2872. [Google Scholar] [CrossRef]
- Seynnes, O.R.; de Boer, M.; Narici, M.V.; Franchi, M.V.; Maffiuletti, N.A.; McGlory, C.; Devries, M.C.; Phillips, S.M.; Łochyński, D.; Kaczmarek, D.; et al. Early skeletal muscle hypertrophy and architectural changes in response to high-intensity resistance training. J. Appl. Physiol. 2007, 102, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Molin, C.J.; Punga, A.R. Compound Motor Action Potential: Electrophysiological Marker for Muscle Training. J. Clin. Neurophysiol. 2016, 33, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, E.; Bertini, E.; Iannaccone, S.T. Childhood spinal muscular atrophy: Controversies and challenges. Lancet Neurol. 2012, 11, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Tizzano, E.F.; Finkel, R.S. Spinal muscular atrophy: A changing phenotype beyond the clinical trials. Neuromuscul. Disord. 2017, 27, 883–889. [Google Scholar] [CrossRef]
- Zhou, H.; Meng, J.; Malerba, A.; Catapano, F.; Sintusek, P.; Jarmin, S.; Feng, L.; Lu-Nguyen, N.; Sun, L.; Mariot, V.; et al. Myostatin inhibition in combination with antisense oligonucleotide therapy improves outcomes in spinal muscular atrophy. J. Cachexia Sarcopenia Muscle 2020, 11, 768–782. [Google Scholar] [CrossRef]
- Bartels, B.; Montes, J.; van der Pol, W.L.; de Groot, J.F. Physical exercise training for type 3 spinal muscular atrophy. Cochrane Database Syst. Rev. 2019, 2019, CD012120. [Google Scholar] [CrossRef]

{kind=link}
| First Author | Year | Study Type | Risk of Bias | NMD | Number of Participants | Gender (M/F) | Age (y) 4 |
|---|---|---|---|---|---|---|---|
| Chung [34] 2 | 2007 | RCT | Some concerns | PM and DM | n = 18; 12 PM, 6 DM | 3/15 | Mean 50 |
| Janssen [26] 3 | 2016 | RCT | High | FSHD1 | n = 9 | 7/4 | 56 ± 15 |
| Burns [35] 3 | 2017 | RCT | Low | CMT | n = 30 | 16/14 | 11.5 ± 3.3 |
| Rahbek [32] | 2017 | RCT | High | MG | n = 15 | 7/8 | 55.6 ± 17.2 |
| Bulut [33] 3 | 2022 | RCT | High | DMD | n = 10 | 10 M | 7.9 (7.2–8.7) |
| Taivassalo [36] 3 | 1999 | N-RCT | Serious | MM and NMM | n = 24; 14 MM, 10 NMM | 9/15 | 14–63 |
| Spector [39] | 1996 | Pre–post | Some concerns | PPS | n = 6 | 5/1 | 53 ± 7 |
| Taivassalo [40] | 1998 | Pre–post | Some concerns | MM | n = 10 | 4/6 | 36 ± 9 |
| Alexanderson [38] | 1999 | Pre–post | High | PM and DM | n = 10; 5 PM, 5 DM | 2/8 | 27–60 |
| Tollbäck [41] | 1999 | Pre–post | Some concerns | MD 1 | n = 9 | 2/7 | 37 ± 8.6 |
| Alexanderson [37] | 2000 | Pre–post | High | PM and DM | n = 11; 7 PM, 4 DM | 3/8 | 23–80 |
| Taivassalo [42] | 2001 | Pre–post | Some concerns | MM | n = 10 | 4/6 | 39.3 ± 9.5 |
| Trenell [43] | 2005 | Pre–post | Some concerns | MM | n = 10 | 3/7 | 42 ± 14 |
| Mhandi [44] | 2007 | Pre–post | Some concerns | CMT | n = 8 | 8 M | 23–45 |
| Porcelli [45] | 2016 | Pre–post | Some concerns | MM and McA | n = 13; 6 MM, 7 McA | 4/2, 3/4 | 51 ± 16, 41 ± 13 |
| Westerberg [46] | 2018 | Pre–post | Some concerns | MG | n = 11 | 5/6 | 60 ± 18 |
| Lott [47] | 2021 | Pre–post | Some concerns | DMD | n = 8 | 8 M | 9.3 ± 0.8 |
| Study | Frequency | Intensity | Type | Time (Min) |
|---|---|---|---|---|
| Chung [34] | 5 d/w program and 7 d/w walk for 6 m | Moderate | Strength and endurance | 15 + 15 walk |
| Janssen [26] | 3 d/w for 16 w | 50 to 65% of HR reserve | Endurance (cycling) | 30 + 5–10 walk, increased by 1 min daily |
| Burns [35] | 3 d/w for 6 m | Resistance at 50 to 70% of the repetition max; Sham at <10% of the repetition max | Strength or sham | 25 |
| Rahbek [32] | 5 d/2 w for 8 w (20 sessions) | Moderate to high | (1) Endurance (cycling); (2) Progressive resistance (full-body program) | (1) 3 × 10–12 with 3 min rest; (2) Various |
| Bulut [33] | 3 d/w for 12 w | 60% of max HR | Endurance (cycling) | 40 |
| Taivassalo [36] | 3–4 d for 8 w | 70–85% of HRR | Endurance (treadmill) | 20–30 |
| Spector [39] | 3 d/w for 10 w | 75% of the three-repetition maximum | Strength | NR |
| Taivassalo [40] | 3–4 d for 8 w | 60–80% of HRR | Endurance (treadmill) | 20–30 |
| Alexanderson [38] | 5 d/w for 12 w | Moderate | Strength and endurance | 15 + 15 walk |
| Tollbäck [41] | 3 d/w for 12 w | 80% of one-repetition maximum | Strength | ~10 min (program) |
| Alexanderson 1 [37] | <3 d/w program and 5 d/w walk for 12 w | Moderate | Strength and endurance | 15 + 15 walk |
| Taivassalo [42] | 3–4 d for 14 w (50 sessions) | 70–80% of max HR | Endurance (cycling) | 30–40 |
| Trenell [43] | 3 d/w for 12 w | 70–80% of their age-predicted max HR | Endurance (cycling) | 30 |
| Mhandi [44] | 3 d/w for 24 w | HR at 80% max aerobic power | Interval-endurance (cycling) | 45 (program) |
| Porcelli [45] | 4 d/w for 12 w | 65–70% of max HR | Stretching and endurance (cycling) | 15 stretching + 30–45 endurance |
| Westerberg [46] | 2 d/w for 12 w | Minimum to 80% max HR | Endurance, strength and balance | 90 (program) |
| Lott [47] | 3 d/w for 12 w | Mild-moderate (50% MVC and after 6 w 60% MVC) | Strength | 90 |
| First Author | Measurement Day | Baseline | End Intervention | |
|---|---|---|---|---|
| MRI biomarkers | ||||
| Muscle volume | Burns [35] | 0, 182 | 1.2 ± 0.3 (scaled score)/control: 1.2 ± 0.4 | 1.1 ± 0.3 (scaled score)/control: 1.1 ± 0.3 (p = 0.24) |
| Trenell [43] | 0, 84 | 11.8 ± 1.5 dm3 | 12.8 ± 1.6 dm3 (p < 0.05) | |
| Muscle maximum area | Trenell [43] | 0, 84 | 464 ± 65 cm2 | 497 ± 70 cm2 (p < 0.05) |
| Tollbäck [41] | 0, 84 | 4090 ± 591 mm2 | 4154 ± 585 mm2 | |
| Spector [39] | 0, 70 | n.a. | Not significantly changed | |
| Fat infiltration | Burns [35] | 0, 182 | 0.1 ± 0.1 (scaled score)/control: 0.1 ± 0.1 | 0.1 ± 0.1 (scaled score)/control: 0.1 ± 0.1 (p = 0.25) |
| Alexanderson [38] | 0, 84 | n.a. | Increased amount of fat in n = 1 | |
| Alexanderson [37] | 0, 84 | No fat infiltration | No change | |
| Tollbäck [41] | 0, 84 | Fatty replacement in n = 4 | n.a. | |
| Fat fraction | Janssen [26] | 0, 112 | 32 ± 36% | Increase in fat fraction normalized per year: 2.9% (p = 0.03) (Significantly decelerated compared with UC (6.7%)) |
| Inflammation | Alexanderson [38] | 0, 84 | n.a. | No increased muscle inflammation |
| Alexanderson [37] | 0, 84 | Inflammation in n = 3 | Inflammation in n = 2, no signs of inflammation in n = 5 | |
| Tollbäck [41] | 0, 84 | n.a. | No increased muscle inflammation | |
| Muscle damage | Lott [47] | 0, 84 | KE = 47 ± 5 ms and KF = 44.5 ± 3 ms | KE = +2.3% (SD 3.6) and KF = +0.4% (SD 4.6) |
| 31P MRS biomarkers | ||||
| Resting PCr | Trenell [43] | 0, 84 | 29 ± 1 mmol.L−1 | 27 ± 1 mmol.L−1 |
| Resting ADP | Trenell [43] | 0, 84 | 28 ± 5 μmol.L−1 | 34 ± 5 μmol.L−1 |
| Resting pH | Trenell [43] | 0, 84 | 7.04 ± 0.01 | 7.06 ± 0.01 |
| PCr hydrolysis during exercise | Trenell [43] | 0, 84 | 13 ± 1 mmol.L−1 | 12 ±1 mmol.L−1 |
| pH fall during exercise | Trenell [43] | 0, 84 | −0.3 ± −0.1 | −0.3 ± −0.1 |
| End exercise ADP | Trenell [43] | 0, 84 | 57 ± 5 μmol.L−1 | 59 ± 10 μmol.L−1 |
| V | Trenell [43] | 0, 84 | 0.4 ± 0.1 mmol.L−1.min−1 | 0.7 ± 0.1 mmol.L−1.min−1 (p < 0.05) |
| Taivassalo [42] | 0, 98 | 10.0 ± 4.7 mmol.L−1.min−1 | 14.1 ± 5.5 mM/min (p < 0.05) | |
| Qmax | Trenell [43] | 0, 84 | 20 ± 3 mmol.L−1.min−1 | 26 ± 2 mmol.L−1.min−1 (p < 0.05) |
| Taivassalo [42] | 0, 98 | 12.6 ± 6.0 mmol.L−1.min−1 | 17.2 ± 6.5 mM/min (p < 0.05) | |
| Initial pH recovery rate | Trenell [43] | 0, 84 | 5 ± 2 mmol.L−1.min−1 | 5 ± 2 mmol.L−1.min−1 |
| dE/d(pH fall) rate | Trenell [43] | 0, 84 | 20 ± 3 mmol.L−1.min−1(pH unit)−1 | 19 ± 1 mmol.L−1.min−1(pH unit)−1 |
| ADP t1/2 | Taivassalo [40] | 0, 56 | * 3.50 ± 0.56 min/** 0.68 ± 0.48 min | * 0.59 ± 0.18 min/** 0.40 ± 0.22 min (p < 0.04) |
| Taivassalo [36] | 0, 56 | MM: 1.27 ± 1.30 min/NMM: 0.35 ± 0.23 min | MM: 0.48 ± 0.33 min (p < 0.01)/NMM: 0.28 ± 0.15 min | |
| PCr/β-NTP ratio | Chung [34] | 0, 91, 182 | 4.03 ± 0.29 | 4.05 ± 0.31 |
| sEMG biomarkers | ||||
| Fatigue indices | Mhandi [44] | 0, 84, 168 | −8.9 ± 7.2% | −6.9 ± 5.5% |
| Root mean square | Mhandi [44] | 0, 84, 168 | 58% | 58% |
| Coactivation | Mhandi [44] | 0, 84, 168 | 11% | 6.5% |
| Mean frequency | Mhandi [44] | 0, 84, 168 | 68 Hz | 63 Hz |
| Integrated EMG | Rahbek [32] | 0, 56 | PRT: 10.9 ± 4.2 μV/ET: 8.5 ± 2.4 μV | PRT: 13.0 ± 7.0 μV (p = 0.31)/ET: 7.0 ± 3.4 μV (p = 0.52) |
| CMAP amplitude | Westerberg [46] | 0, 84 | Quadriceps: 4.5 ± 2.6 mV/BB: 5.5 ± 2.1 mV | Quadriceps: 5.3 ± 2.8 mV (p = 0.016)/BB: 4.6 ± 1.3 mV (p = 0.63) |
| Ultrasound biomarkers | ||||
| Thickness | Westerberg [46] | 0, 84 | Rectus femoris: 19.6 ± 5.6 mm/vastus intermedius: 18.0 ± 5.8 mm/BB: 33.3 ± 6.5 mm | Rectus femoris: 23.0 ± 3.9 mm (p = 0.0098)/vastus intermedius: 22.0 ± 6.2 mm (p = 0.034)/BB: 32.1 ± 6.2 mm (p = 0.11) |
| Bulut [33] | 0, 84 | Vastus lateralis: D—2.1 ± 0.5 cm/ND—2.2 ± 0.4 cm (control: D—2.1 ± 0.2 cm/ND—2.2 ± 0.2 cm) | Vastus lateralis: D—2.3 ± 0.6 cm/ND—2.3 ± 0.4 cm (control: D—2.4 ± 0.5 cm (p *** = 0.6)/ND—2.5 ± 0.5 cm (p *** = 0.5)) | |
| Pennation angle | Bulut [33] | 0, 84 | Vastus lateralis: D—18.9 ± 3.7°/ND—19.6 ± 3.4° (control: D—17.7 ± 3.3°/ND—18.4 ± 2.8°) | Vastus lateralis: D—19.7 ± 5.3°/ND—18.5 ± 6.3° (control: D—18.8 ± 2.3° (p *** = 0.9)/ND—20.4 ± 2.6° (p *** = 0.3)) |
| Fascicle Length | Bulut [33] | 0, 84 | Vastus lateralis: D—7.0 ± 1.5 cm/ND—6.7 ± 1.5 cm (control: D—7.5 ± 1.6 cm/ND—6.8 ± 1.7 cm) | Vastus lateralis: D—7.0 ± 1.3 cm/ND—7.5 ± 1.7 cm (control: D—7.6 ± 0.9 cm (p *** = 0.8)/ND—7.3 ± 0.6 cm (p *** = 0.6)) |
| NIRS biomarkers | ||||
| Δ[deoxy(Hb + Mb)] | Porcelli [45] | 0, 84 | MM: 22.0 ± 6.7% of ischemia/McA: 23.4 ± 6.2% of ischemia | MM: 34.2 ± 5.9% of ischemia (p < 0.05)/McA: 40.6 ± 7.2% of ischemia (p < 0.05) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomp, L.; Jeneson, J.A.L.; van der Pol, W.L.; Bartels, B. Electrophysiological and Imaging Biomarkers to Evaluate Exercise Training in Patients with Neuromuscular Disease: A Systematic Review. J. Clin. Med. 2023, 12, 6834. https://doi.org/10.3390/jcm12216834
Pomp L, Jeneson JAL, van der Pol WL, Bartels B. Electrophysiological and Imaging Biomarkers to Evaluate Exercise Training in Patients with Neuromuscular Disease: A Systematic Review. Journal of Clinical Medicine. 2023; 12(21):6834. https://doi.org/10.3390/jcm12216834
Chicago/Turabian StylePomp, Lisa, Jeroen Antonius Lodewijk Jeneson, W. Ludo van der Pol, and Bart Bartels. 2023. "Electrophysiological and Imaging Biomarkers to Evaluate Exercise Training in Patients with Neuromuscular Disease: A Systematic Review" Journal of Clinical Medicine 12, no. 21: 6834. https://doi.org/10.3390/jcm12216834
APA StylePomp, L., Jeneson, J. A. L., van der Pol, W. L., & Bartels, B. (2023). Electrophysiological and Imaging Biomarkers to Evaluate Exercise Training in Patients with Neuromuscular Disease: A Systematic Review. Journal of Clinical Medicine, 12(21), 6834. https://doi.org/10.3390/jcm12216834