

Intranasal Synechiae as Complications of Rhinosurgical Treatment—A Review of Current Knowledge


Abstract
1. Introduction
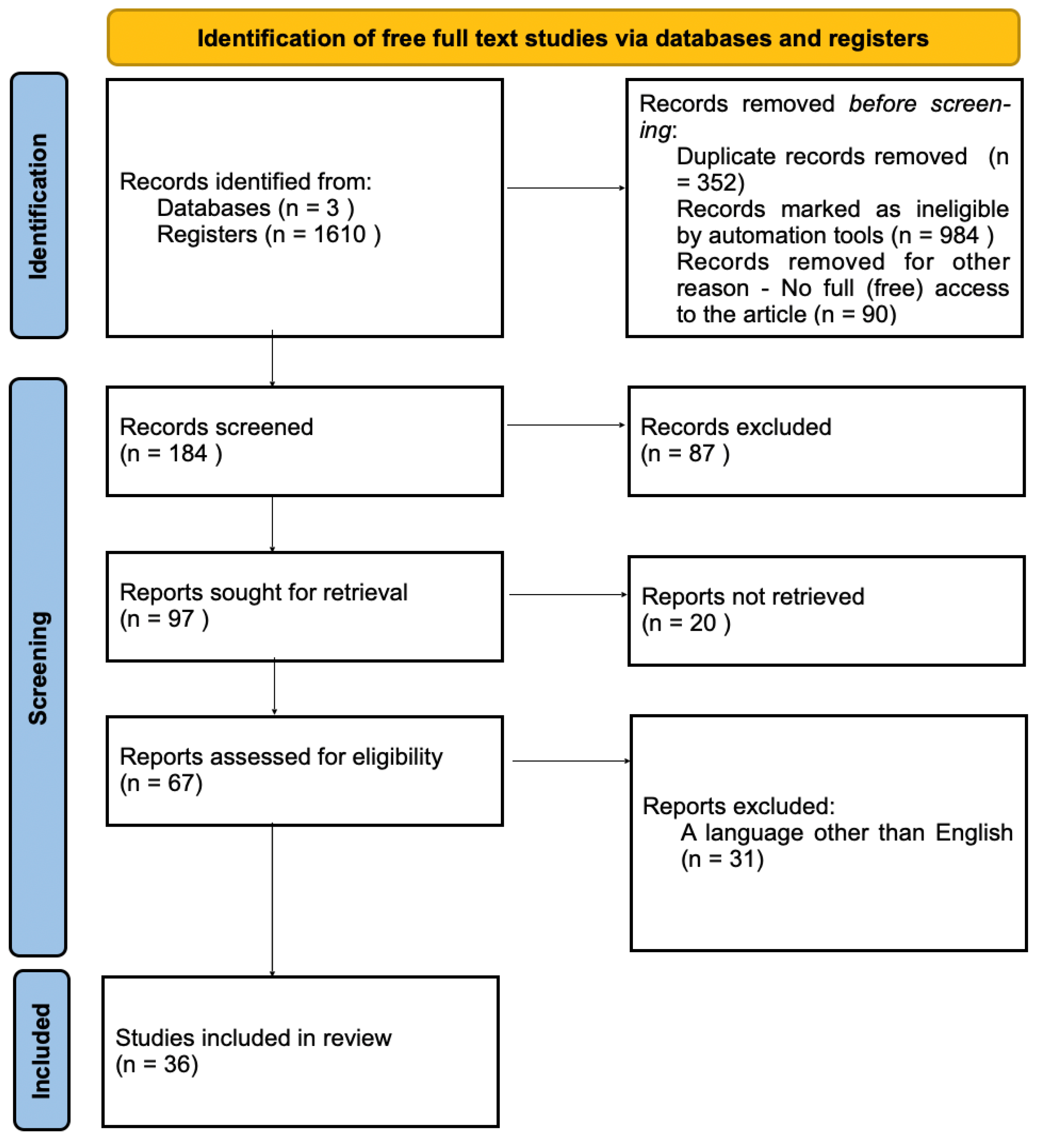
2. Materials and Methods
3. Results
3.1. The Use of Nasal Splints (Separators) as a Prevention of Intranasal Adhesions (Synechiae)
3.1.1. The Use of Nasal Splints in the Surgery of the Inferior Turbinates (Turbinoplasty)
3.1.2. The Use of Nasal Splints in Septoturbinoplasty
3.1.3. Nasal Separators Used in Endoscopic Operations of the Paranasal Sinuses
3.2. The Use of the Suturing of the (Trans)Nasal Septum
3.3. Irrigation of the Nasal Cavity and Paranasal Sinuses after Rhinosurgical Treatment
3.4. The Risk of Intranasal Synechiae and the Intranasal Material Used
3.5. Use of Intranasal Dressings Based on Absorbed Materials
Prevention of Lateralization of the Middle Turbinates after Functional Surgery of the Paranasal Sinuses (FESS)
3.6. Surgical Approaches and the Risk of Intranasal Adhesions
3.7. Application of Mitomycin C
3.8. Intranasal Synechiae in Other Types of Surgery with the Use of Intranasal Approach
4. Discussion
4.1. Surgical Technique, Additional Maneuvers and the Risk of Adhesions
4.2. Care in the Postoperative Period
4.3. Limitations
5. Conclusions
- Irrigation of the nasal cavities in the postoperative period significantly reduces the risk of intranasal adhesions after rhinosurgical treatment. The type and concentration of the solution used during irrigation is also important.
- The use of absorbable materials reduces the risk of intranasal adhesions.
- The use of splints after turbinoplasty clinically significantly reduces the risk of intranasal adhesions.
- The use of splints made of modern materials (e.g., Silastic) after nasal septum surgery and endoscopic surgery of the paranasal sinuses may reduce the risk of intranasal adhesions.
- In carefully selected cases, as a preventive factor or in patients not responding to standard methods, local cytostatic treatment (mitomycin C) should be used.
- The risk of intranasal adhesions is reduced by factors related to the operation itself: simultaneous operation of the inferior turbinates, endoscopic septoplasty, and protection of the middle turbinate against excessive lateralization during FESS.
- An option to reduce the risk of intranasal adhesions after septoplasty is suturing of the nasal septum.
- Further research is required that may result in a universal classification system for intranasal adhesions that could be used as a preventive measure, and on the other hand, facilitate individualization of the therapy (e.g., selection of the appropriate form of treatment depending on the stage of advancement).
- Summarizing—the risk of intranasal adhesions (synechiae) depends on the type of procedure, the surgical technique, materials used and wound care in the postoperative period. Every case requires an individual approach.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shone, G.R.; Clegg, R.T. Nasal adhesions. J. Laryngol. Otol. 1987, 101, 555–557. [Google Scholar] [CrossRef]
- White, A.; Murray, J.A. Intranasal adhesions formation following surgery for chronic nasal obstruction. Clin. Otholaryngol. 1988, 13, 139–143. [Google Scholar] [CrossRef]
- Kim, T.K.; Jeong, J.Y. Deviated nose: Physiological and pathological changes of the nasal cavity. Arch. Plast. Surg. 2020, 47, 505–515. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, D. Synechiae in the Nose treated by Diathermy. Proc. R. Soc. Med. 1915, 8, 74. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.; Elhassan, H.; Singh, N. History of intranasal splints. J. Laryngol. Otol. 2018, 132, 198–201. [Google Scholar] [CrossRef]
- Awad, O.G.; Hamid, K.A. The value of intranasal splints after partial inferior turbinectomy. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 75–80. [Google Scholar] [CrossRef][Green Version]
- Tang, S.; Kacker, A. Should intranasal splints be used after nasal septal surgery? Laryngoscope 2012, 122, 1647–1648. [Google Scholar] [CrossRef]
- Jung, Y.G.; Hong, J.W.; Eun, Y.G.; Kim, M.G. Objective usefulness of thin silastic septal splints after septal surgery. Am. J. Rhinol. Allergy 2011, 25, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.A.; Murrant, N.J.; Evans, K.L.; Lavelle, R.J. Intranasal splints and their effects on intranasal adhesions and septal stability. Clin. Otolaryngol. Allied Sci. 1992, 17, 24–27. [Google Scholar] [CrossRef]
- Veluswamy, A.; Handa, S.; Shivaswamy, S. Nasal septal clips: An alternative to nasal packing after septal surgery? Indian J. Otolaryngol. Head Neck Surg. 2012, 64, 346–350. [Google Scholar] [CrossRef]
- Baguley, C.J.; Stow, N.W.; Weitzel, E.K.; Douglas, R.G. Silastic splints reduce middle meatal adhesions after endoscopic sinus surgery. Am. J. Rhinol. Allergy 2012, 26, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Hartl, T.T.; Ospina, J.; Janjua, A. Silastic “Spring” Spacers for Use Following Endoscopic Sinus Surgery. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 233–237. [Google Scholar] [CrossRef]
- Al-Raggad, D.K.; El-Jundi, A.M.; Al-Momani, O.S.; Al-Serhan, M.M.; Nawasrah, O.O.; Qhawi, M.A.; Husban, A.M. Suturing of the nasal septum after septoplasty, is it an effective alternative to nasal packing? Saudi Med. J. 2007, 28, 1534–1536. [Google Scholar]
- Genç, E.; Ergin, N.T.; Bilezikçi, B. Comparison of suture and nasal packing in rabbit noses. Laryngoscope 2004, 114, 639–645. [Google Scholar] [CrossRef]
- Lemmens, W.; Lemkens, P. Septal suturing following nasal septoplasty, a valid alternative for nasal packing? Acta Otorhinolaryngol. Belg. 2001, 55, 215–221. [Google Scholar] [PubMed]
- Naik, K. A novel way of trans-septal splint suturing without nasal packing for septoplasty. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 48–50. [Google Scholar] [CrossRef]
- Cukurova, I.; Cetinkaya, E.A.; Mercan, G.C.; Demirhan, E.; Gumussoy, M. Retrospective analysis of 697 septoplasty surgery cases: Packing versus trans-septal suturing method. Acta Otorhinolaryngol. Ital. 2012, 32, 111–114. [Google Scholar]
- Meena, R.; Sharma, R.; Malhotra, V.; Rathore, P.K. Comparison of Trans-septal Suturing Technique with Polyvinyl Alcohol Sponge-Based Nasal Packing for Hemostasis in Septoplasty. Cureus 2022, 14, e25161. [Google Scholar] [CrossRef]
- Talbot, A.R.; Herr, T.M.; Parsons, D.S. Mucociliary clearance and buffered hypertonic saline solution. Laryngoscope 1997, 107, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Keojampa, B.K.; Nguyen, M.H.; Ryan, M.W. Effects of buffered saline solution on nasal mucociliary clearance and nasal airway patency. Otolaryngol. Head Neck Surg. 2004, 131, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Kurtaran, H.; Ugur, K.S.; Yilmaz, C.S.; Kaya, M.; Yuksel, A.; Ark, N.; Gunduz, M. The effect of different nasal irrigation solutions following septoplasty and concha radiofrequency: A prospective randomized study. Braz. J. Otorhinolaryngol. 2018, 84, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Macchi, A.; Terranova, P.; Digilio, E.; Castelnuovo, P. Hyaluronan plus saline nasal washes in the treatment of rhino-sinusal symptoms in patients undergoing functional endoscopic sinus surgery for rhino-sinusal remodeling. Int. J. Immunopathol. Pharmacol. 2013, 26, 137–145. [Google Scholar] [CrossRef]
- Lee, E.J.; Hwang, H.J.; Jung, C.M.; Kim, M.K.; Kim, K.S. Anti-adhesive effect of solid mixture of sodium hyaluronate/carboxymethylcellulose in murine nasal cavities. Eur. Arch. Otorhinolaryngol. 2017, 274, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Liu, N.; Wang, Z.; Gao, J.; Zhang, H.; Li, M.; Du, Y.; Gao, X.; Zheng, A. Development and Optimization of Chitosan Nanoparticle-Based Intranasal Vaccine Carrier. Molecules 2022, 27, 204. [Google Scholar] [CrossRef]
- Özbal Koç, A.E.; Türkoğlu Babakurban, S.; Kibar, S.S.; Büyüklü, F. A comparative study on nasal packing after septoplasty: Does it matter in terms of patient comfort, bleeding, and crust or synechia formation? Kulak Burun Bogaz Ihtis. Derg. 2016, 26, 152–158. [Google Scholar] [CrossRef]
- Dutta, S.; Mukherjee, A.; Saha, J.; Biswas, G.; Haldar, D.; Sen, I.; Sinha, R. Modified technique of anterior nasal packing: A comparative study report. Indian J. Otolaryngol. Head Neck Surg. 2012, 64, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cai, C.; Wang, S. Merocel versus Nasopore for nasal packing: A meta-analysis of randomized controlled trials. PLoS ONE 2014, 9, e93959. [Google Scholar] [CrossRef]
- Coey, J.G.; Whittaker, P.J.; Williams, G.; Ikram, U.H.; Page, O.J.R. Fibrin tissue adhesive versus nasal packing in endoscopic nasal surgery: A systematic review and meta-analysis. Rhinology 2019, 57, 21–31. [Google Scholar] [CrossRef]
- Grzeskowiak, B.; Wierzchowska, M.; Walorek, R.; Seredyka-Burduk, M.; Wawrzyniak, K.; Burduk, P.K. Steroid vs. antibiotic impregnated absorbable nasal packing for wound healing after endoscopic sinus surgery: A randomized, double blind, placebo-controlled study. Braz. J. Otorhinolaryngol. 2019, 85, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Athanasiadis, T.; Beule, A.G.; Robinson, B.H.; Robinson, S.R.; Shi, Z.; Wormald, P.J. Effects of a novel chitosan gel on mucosal wound healing following endoscopic sinus surgery in a sheep model of chronic rhinosinusitis. Laryngoscope 2008, 118, 1088–1094. [Google Scholar] [CrossRef]
- Wang, Y.P.; Wang, M.C.; Chen, Y.C.; Leu, Y.S.; Lin, H.C.; Lee, K.S. The effects of Vaseline gauze strip, Merocel, and Nasopore on the formation of synechiae and excessive granulation tissue in the middle meatus and the incidence of major postoperative bleeding after endoscopic sinus surgery. J. Chin. Med. Assoc. 2011, 74, 16–21. [Google Scholar] [CrossRef]
- Wang, T.C.; Tai, C.J.; Tsou, Y.A.; Tsai, L.T.; Li, Y.F.; Tsai, M.H. Absorbable and nonabsorbable packing after functional endoscopic sinus surgery: Systematic review and meta-analysis of outcomes. Eur. Arch. Otorhinolaryngol. 2015, 272, 1825–1831. [Google Scholar] [CrossRef] [PubMed]
- Yan, M.; Zheng, D.; Li, Y.; Zheng, Q.; Chen, J.; Yang, B. Biodegradable nasal packings for endoscopic sinonasal surgery: A systematic review and meta-analysis. PLoS ONE 2014, 9, e115458. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.S.; Park, C.H.; Hong, S.L.; Kim, M.J.; Kim, J.Y.; Kim, Y.W.; Koo, S.K.; Roh, H.J. Comparative analysis of Cutanplast and Spongostan nasal packing after endoscopic sinus surgery: A prospective, randomized, multicenter study. Eur. Arch. Otorhinolaryngol. 2015, 272, 1699–1705. [Google Scholar] [CrossRef] [PubMed]
- Champagne, C.; Ballivet de Régloix, S.; Genestier, L.; Crambert, A.; Maurin, O.; Pons, Y. Endoscopic vs. conventional septoplasty: A review of the literature. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2016, 133, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Alaryani, R.A.; Alhedaithy, R.A. Preventive Measures of Middle Turbinate Lateralization After Endoscopic Sinus Surgery: An Updated Review. Cureus 2021, 13, e15763. [Google Scholar] [CrossRef] [PubMed]
- Sayeed, A.; Alam, M.; Sharma, S.C.; Hasan, S.A. Mitomycin-C in Post-endoscopic Septoplasty Synechiae: Does it Really Helps? Indian. J. Otolaryngol. Head Neck Surg. 2019, 71 (Suppl. 3), 2091–2095. [Google Scholar] [CrossRef] [PubMed]
- Yamaoka, W.Y.; Gregório, L.C. The use of Mitomycin-C to reduce synechia in middle meatus in sinus surgery: Preliminary results. Braz. J. Otorhinolaryngol. 2012, 78, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Aslam, M.A.; Mirza, A.B.; Butt, I.A. Results of endoscopic endonasal dacrocystorhinostomy. J. Pak. Med. Assoc. 2014, 64, 619–623. [Google Scholar] [PubMed]
- Dolci, R.L.L.; Miyake, M.M.; Tateno, D.A.; Cançado, N.A.; Campos, C.A.C.; Dos Santos, A.R.L.; Lazarini, P.R. Postoperative otorhinolaryngologic complications in transnasal endoscopic surgery to access the skull base. Braz. J. Otorhinolaryngol. 2017, 83, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Stannard, W.; O’Callaghan, C. Ciliary function and the role of cilia in clearance. J. Aerosol Med. 2006, 19, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Bassiouni, A.; Naidoo, Y.; Wormald, P.J. Does mucosal remodeling in chronic rhinosinusitis result in irreversible mucosal disease? Laryngoscope 2012, 122, 225–229. [Google Scholar] [CrossRef]
- Postalci, L.; Erdim, I.; Demirgil, B.; Gunaldi, O.; Asilturk, M.; Demirci, H.; Kina, H.; Erdogan, U.; Yazici, M.; Emel, E. Late Postoperative Rhinological Complications After Microscopic Transnasal Hypophysectomy. Turk. Neurosurg. 2017, 27, 182–186. [Google Scholar] [CrossRef] [PubMed]
- McCaffrey, T.V. Nasal manifestations of systemic diseases. Otolaryngol. Pol. 2009, 63, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.C.; Gill, A.S.; Squires, L.D.; Steele, T.O. Sjögren’s Syndrome Sequelae: Nasal Synechiae and Nasopharyngeal Stenosis. Ear Nose Throat J. 2021, 100 (Suppl. 10), 1095S–1097S. [Google Scholar] [CrossRef]
- Alvoa, A.; Sedanob, C.; Olavarríaa, C.h. Bilateral massive nasal synechiae: A rare presentation of a common condition. Otolaryngol. Online J. 2015, 5, 1–7. [Google Scholar]
- Kong, V.; Ko, J.; Cheung, C.; Lee, B.; Leow, P.; Thirayan, V.; Bruce, J.; Laing, G.; Khashram, M.; Clarke, D. Foley Catheter Balloon Tamponade for Actively Bleeding Wounds Following Penetrating Neck Injury is an Effective Technique for Controlling Non-Compressible Junctional External Haemorrhage. World J. Surg. 2022, 46, 1067–1075. [Google Scholar] [CrossRef]
- Daneshrad, P.; Chin Gregory, Y.; Rice, D.H. Fibrin glue presents complications of septal surgery: Findings in a series of 100 patients. Ear Nose Throat J. 2003, 82, 196–198. [Google Scholar] [CrossRef] [PubMed]
- Huang, I.T.; Podkomorska, D.; Murphy, M.N.; Hoffer, I. Toxic shock syndrome following septoplasty and partial turbinectomy. J. Otolaryngol. 1986, 15, 310–312. [Google Scholar]
- Shaw, C.L.; Dymock, R.B.; Cowin, A.; Wormald, P.J. Effect of packing on nasal mucosa of sheep. J. Laryngol. Otol. 2000, 114, 506–509. [Google Scholar] [CrossRef][Green Version]
- Yilmazer, C.; Sener, M.; Yilmaz, I.; Erkan, A.N.; Cagici, C.A.; Donmez, A.; Arslan, G.; Ozluoglu, L.N. Pre-emptive analgesia for removal of nasal packing: A double-blind placebo controlled study. Auris Nasus Larynx 2007, 34, 471–475. [Google Scholar] [CrossRef]
- Naghibzadeh, B.; Peyvandi, A.A.; Naghibzadeh, G. Does post septoplasty nasal packing reduce complications? Acta Med. Iran. 2011, 49, 9–12. [Google Scholar]
- Medtronic Engineer the Extraordinary, ENT Product Catalog 2023. Available online: https://www.medtronic.com/content/dam/medtronic-wide/public/united-states/products/ear-nose-throat/ent-product-catalog.pdf (accessed on 5 September 2023).
- Weber, R.; Keerl, R.; Hochapfel, F.; Draf, W.; Toffel, P.H. Packing in endonasal surgery. Am. J. Otolaryngol. 2000, 22, 306–320. [Google Scholar] [CrossRef] [PubMed]
- Nasopore. The Nasal Dressing for Improved Wound Healing. Available online: https://www.kebomed.dk/files/27/leaflet_nasopore_250612.pdf (accessed on 5 September 2023).
- Hajosch, R.; Suckfuell, M.; Oesser, S.; Ahlers, M.; Flechsenhar, K.; Schlosshauer, B. A novel gelatin sponge for accelerated hemostasis. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 94, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Cenni, E.; Ciapetti, G.; Stea, S.; Corradini, A.; Carozzi, F. Biocompatibility and performance in vitro of a hemostatic gelatin sponge. J. Biomater. Sci. Polym. Ed. 2000, 11, 685–699. [Google Scholar]
- Hu, D.; Sires, B.S.; Tong, D.C.; Royack, G.A.; Oda, D. Effect of brief exposure to mitomycin C on cultured human nasal mucosa fibroblasts. Ophthal Plast. Reconstr. Surg. 2000, 16, 119–125. [Google Scholar] [CrossRef]
- Helal, M.; Messiha, N.; Amayem, A.; el-Maghraby, A.; Elsherif, Z.; Dabees, M. Intraoperative mitomycin-C versus postoperative topical mitomycin-C drops for the treatment of pterygium. Ophthalmic Surg. Lasers. 1996, 27, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Bofares, K.M. Effect of middle turbinate intervention on outcomes of middle meatal endoscopic surgery. Int. J. Otorhinolaryngol. 2015, 1, 13–19. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cause | Examples of Diseases and Circumstances |
|---|---|
| Infectious | Rhinoscleroma, Rhinosporidiosis, Leishmaniasis. Other: Mycobacteria (M. tuberculosis, M. leprae), Syphilis. |
| Autoimmune and non-infectious | Granulomatosis with polyangiitis, Cicatricial pemphigoid, Epidermolysis bullosa acquisita, Sarcoidosis, Sjögren’s syndrome. |
| Traumatic | Accidental (including contact sports, foreign body); Iatrogenic (surgery, packing, etc.). |
| Others | Intranasal drugs (cocaine), physical (radiotherapy) and chemical burns Radiotherapy, Natural Killer/T cell lymphoma-nasal type, Intranasal eosinophilic angiocentric fibrosis. |
| Method | Characteristics | Comments |
|---|---|---|
| Bolgerization | Controlled formation of turbinate–septal adhesion. | Named after the propagator of the method, Bolger. |
| Conchopexy | Connection (through the nasal septum with absorbable surgical suture, size 4–0) of the heads of the middle turbinates. | The most effective method of preventing adhesions (according to many surgeons). |
| Clipping | Fixation of the middle turbinate heads to the septum using metal clips. | This method is not recommended in the case of polypus degeneration of the nasal turbinates or previous (submucosal) resection of the nasal turbinate and the absence of septal cartilage (prevention of iatrogenic septal perforation). |
| Partial turbinate resection | Partial/complete resection of the middle turbinate. | The consequence may be iatrogenic obliteration of the frontal sinus. |
| Implantation of a steroid-eluting stent | Implantation of an absorbable steroid-eluting stent, e.g., mometasone furoate. | In addition (to the mechanical effect, that fixes the turbinate in the correct position) it also has an anti-inflammatory and anti-edematous effect, positively affecting the healing process of the mucous membrane. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stępiński, M.J.; Banaszewski, J. Intranasal Synechiae as Complications of Rhinosurgical Treatment—A Review of Current Knowledge. J. Clin. Med. 2023, 12, 6831. https://doi.org/10.3390/jcm12216831
Stępiński MJ, Banaszewski J. Intranasal Synechiae as Complications of Rhinosurgical Treatment—A Review of Current Knowledge. Journal of Clinical Medicine. 2023; 12(21):6831. https://doi.org/10.3390/jcm12216831
Chicago/Turabian StyleStępiński, Mateusz J., and Jacek Banaszewski. 2023. "Intranasal Synechiae as Complications of Rhinosurgical Treatment—A Review of Current Knowledge" Journal of Clinical Medicine 12, no. 21: 6831. https://doi.org/10.3390/jcm12216831
APA StyleStępiński, M. J., & Banaszewski, J. (2023). Intranasal Synechiae as Complications of Rhinosurgical Treatment—A Review of Current Knowledge. Journal of Clinical Medicine, 12(21), 6831. https://doi.org/10.3390/jcm12216831