
Vascular Complications Following Transcatheter Aortic Valve Implantation, Using MANTA (Collagen Plug-Based) versus PROSTAR (Suture-Based), from a French Single-Center Retrospective Registry
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Analysis of the Femoral Access
- Diameter of the common femoral artery (mm);
- Degree of calcification (Figure 1);
- Location of calcifications (anterior, medial, lateral, posterior);
- Tortuosity (minimal, moderate, severe);
- Bifurcation height;
- Size of the femoral shaft (external diameter, mm).
- Location.
- Size of the shaft.
2.3. Management of Antithrombotic Treatment
2.4. TAVI Procedure
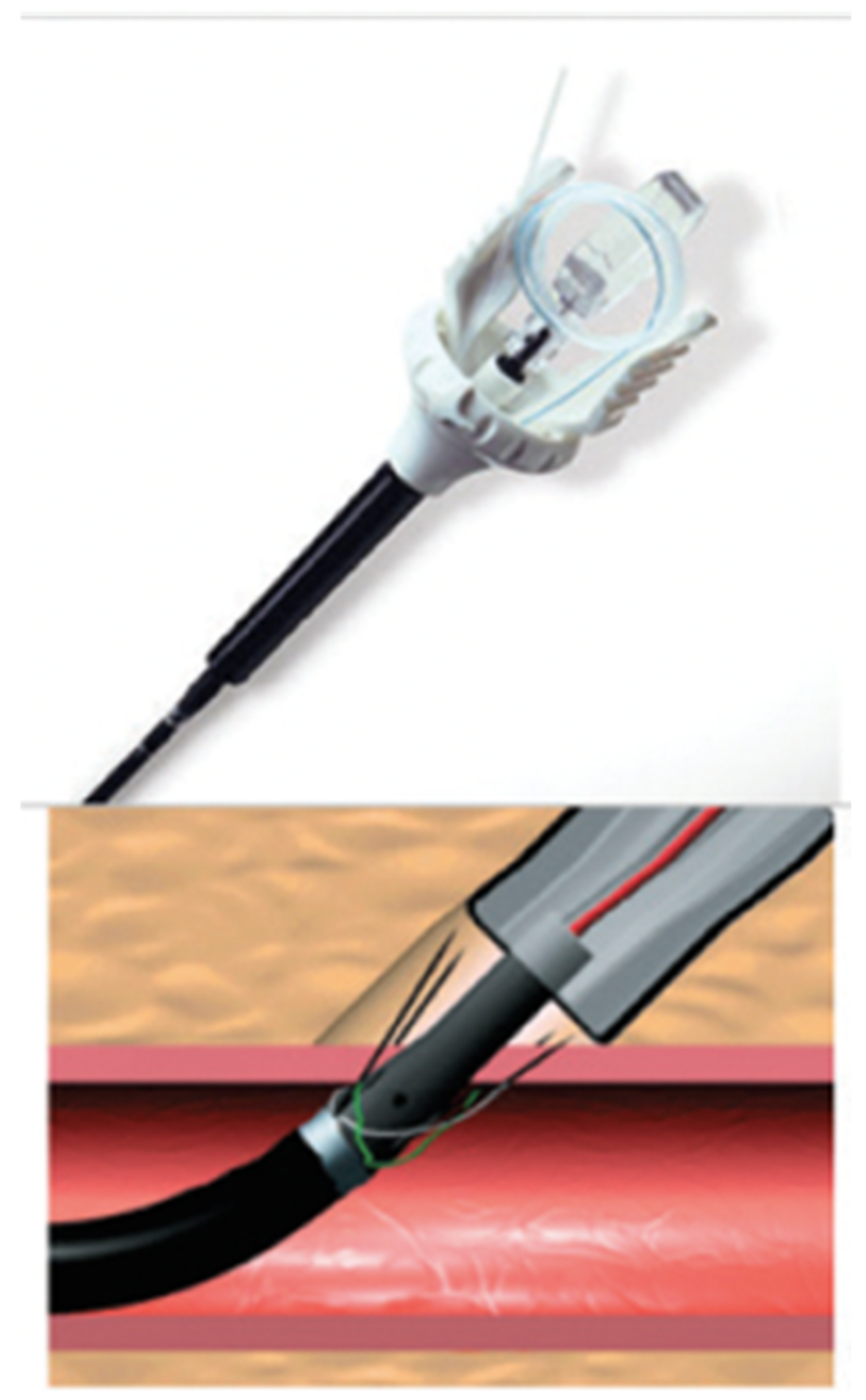
2.5. PROSTAR Closure
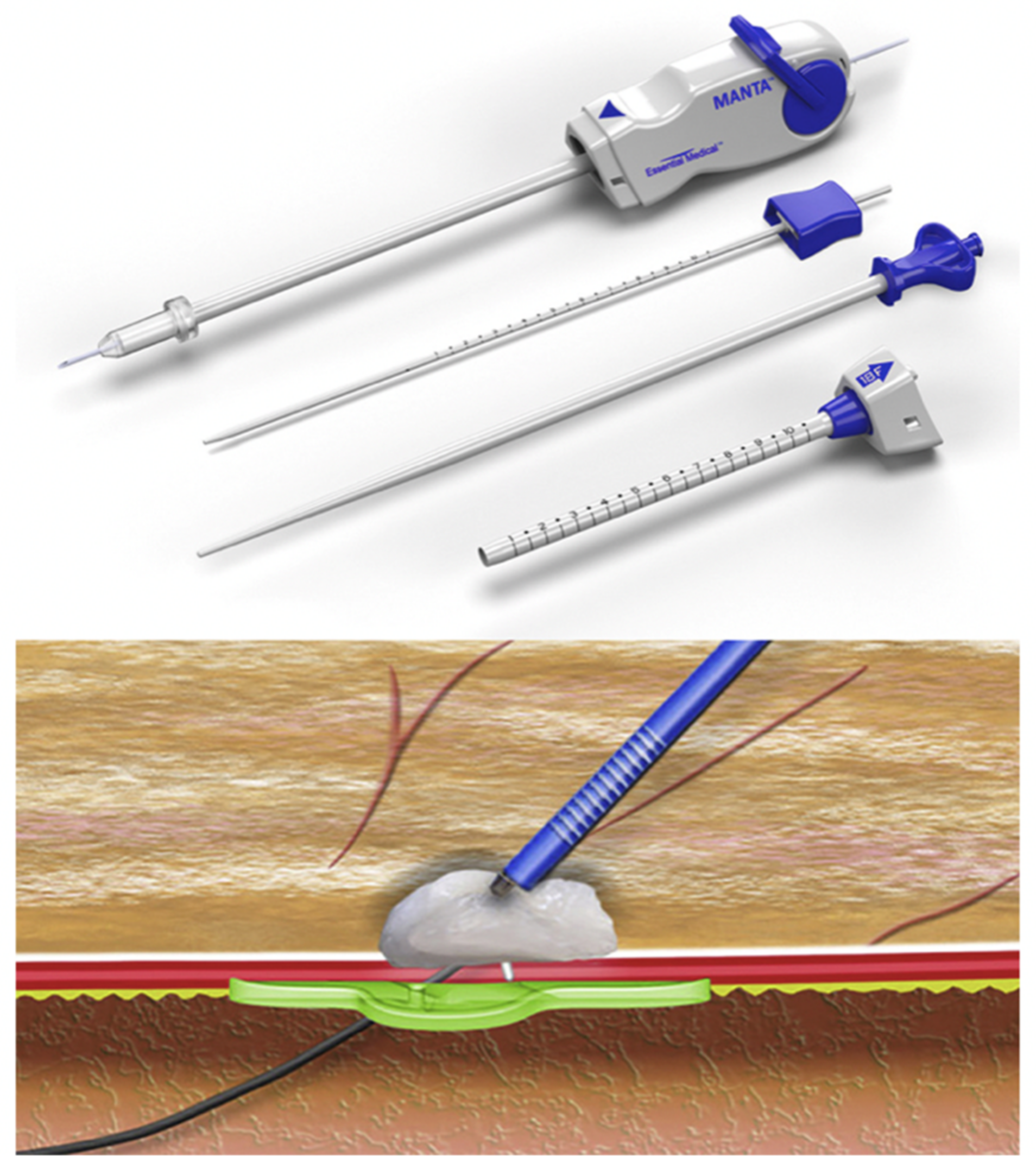
2.6. MANTA Closure
2.7. Monitoring Procedures after Closure of the Approach
2.8. Primary Endpoint
2.9. Secondary Endpoints
- In-hospital mortality.
- Type of vascular complications: false aneurysm, arteriovenous fistula arterial dissection, arterial stenosis (>50% reduction in diameter), homolateral lower limb ischemia, bleeding.
- Bleeding complications: Total, major (defined as loss of more than 3 g/dL of hemoglobin, the need to transfuse more than 2 red blood cells or the need for surgery), and minor (any clinically significant non-life-threatening bleeding that does not meet the criteria for major bleeding).
- Immediate failure of closure of the approach by the device—defined by the need for additional endovascular or surgical closure per procedure.
- Length of stay.
- Study of the risk factors for complications of the approach.
2.10. Ethics
2.11. Statistics
3. Results
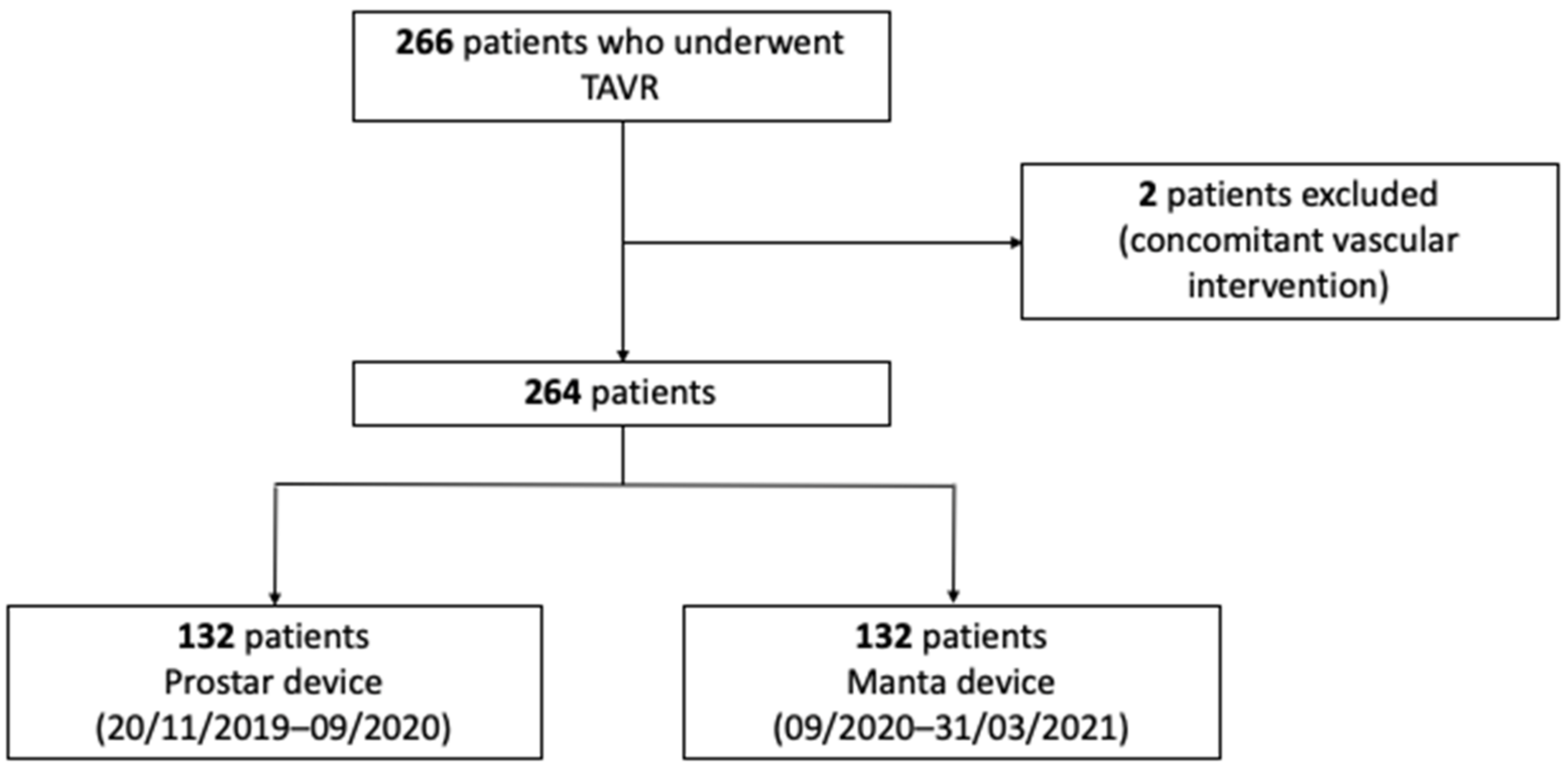
3.1. Flow Chart
3.2. Characteristics of Study Population
3.3. Characteristics of the Femoral Access and Implanted Valve
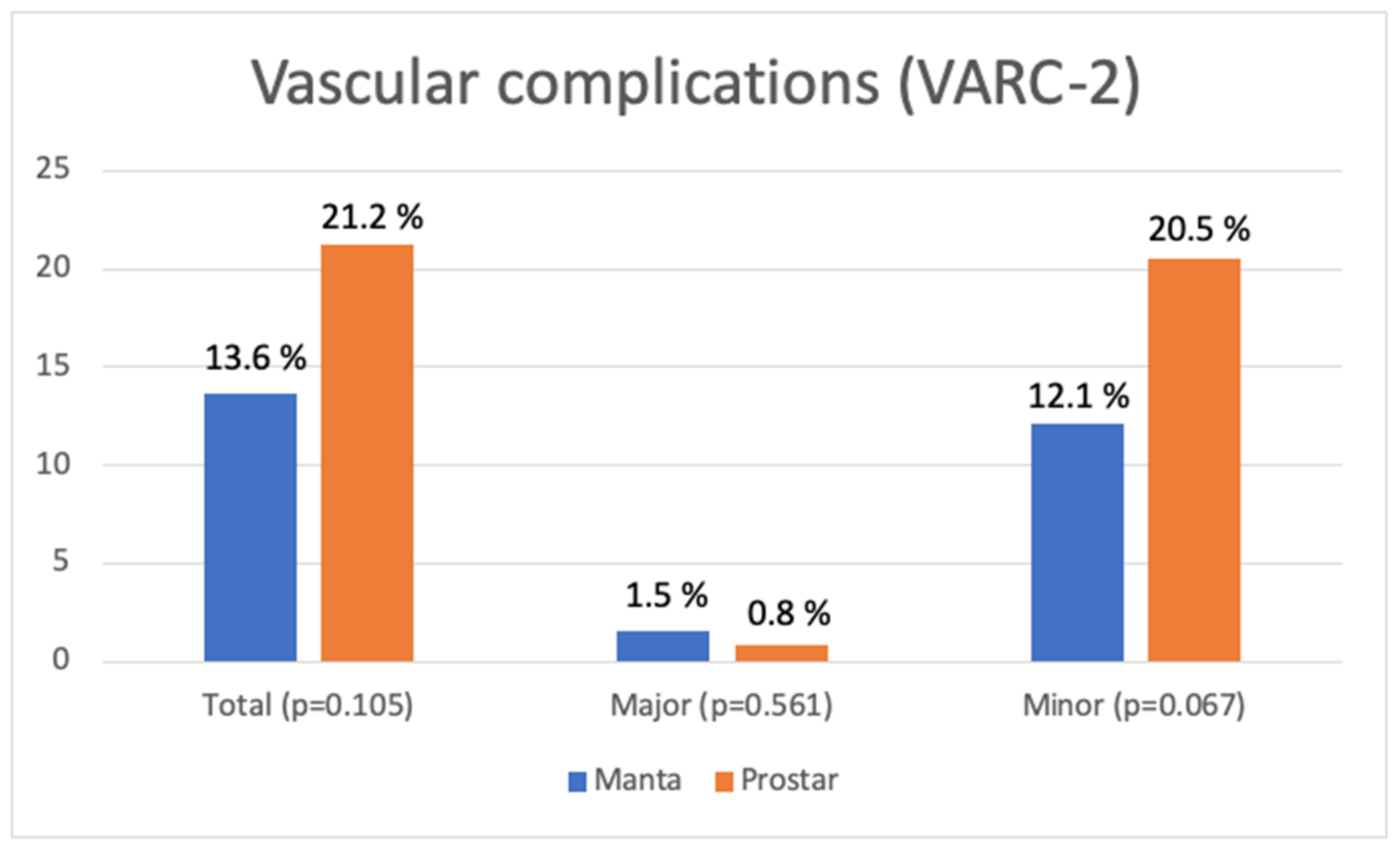
3.4. Vascular Complications of the Main Access
3.5. In-Hospital Mortality and Length of Stay
3.6. Risk Factors for Vascular Complications
4. Discussion
4.1. Vascular Complications
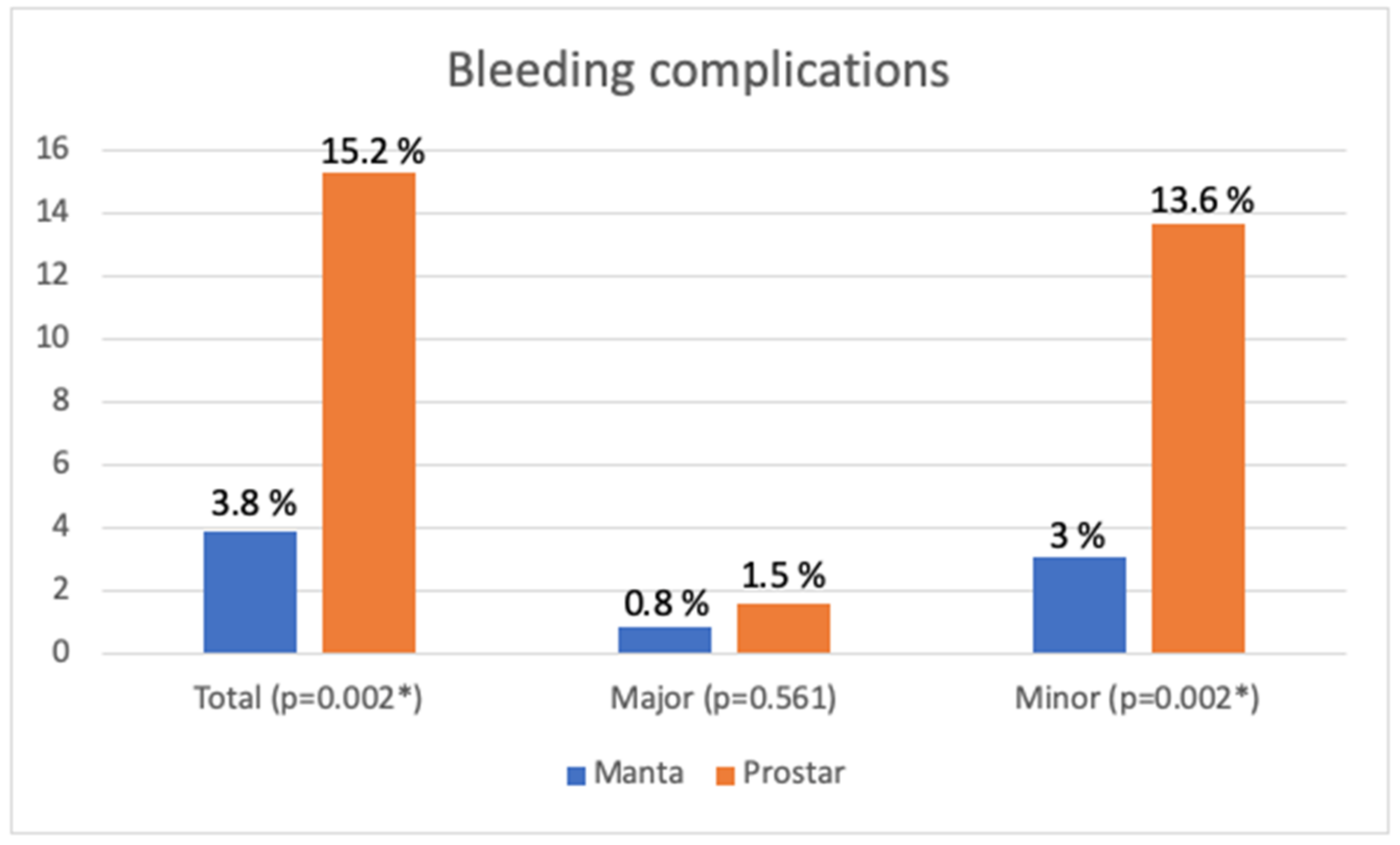
4.2. Bleeding Complications
4.3. Independent Risk Factors of Vascular Complication
- Euroscore logistic is representative of the patient’s severity.
- Finally, diabetes mellitus, which was also a risk factor for false aneurysm in the site of femoral access [35]
4.4. Limits and Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iung, B.; Vahanian, A. Epidemiology of valvular heart disease in the adult. Nat. Rev. Cardiol. 2011, 8, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Horstkotte, D.; Loogen, F. The natural history of aortic valve stenosis. Eur. Heart J. 1988, 9 (Suppl. E), 57–64. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F., Jr.; Otto, C.M. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2017, 30, 372–392. [Google Scholar] [CrossRef] [PubMed]
- Larzon, T.; Geijer, H.; Gruber, G.; Popek, R.; Norgren, L. Fascia suturing of large access sites after endovascular treatment of aortic aneurysms and dissections. J. Endovasc. Ther. 2006, 13, 152–157. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, P.; Al-Ani, A.; von Lueder, T.; Hoffmann, J.; Majak, P.; Hagen, O.; Loose, H.; Kløw, N.E.; Opdahl, A. Access site complications after transfemoral aortic valve implantation—A comparison of Manta and ProGlide. CVIR Endovasc. 2018, 1, 20. [Google Scholar] [CrossRef]
- De Palma, R.; Settergren, M.; Rück, A.; Linder, R.; Saleh, N. Impact of percutaneous femoral arteriotomy closure using the MANTATM device on vascular and bleeding complications after transcatheter aortic valve replacement. Catheter. Cardiovasc. Interv. 2018, 92, 954–961. [Google Scholar] [CrossRef]
- Moriyama, N.; Lindström, L.; Laine, M. Propensity-matched comparison of vascular closure devices after transcatheter aortic valve replacement using MANTA versus ProGlide. EuroIntervention 2019, 14, e1558–e1565. [Google Scholar] [CrossRef]
- Biancari, F.; Romppanen, H.; Savontaus, M.; Siljander, A.; Mäkikallio, T.; Piira, O.P.; Piuhola, J.; Vilkki, V.; Ylitalo, A.; Vasankari, T.; et al. MANTA versus ProGlide vascular closure devices in transfemoral transcatheter aortic valve implantation. Int. J. Cardiol. 2018, 263, 29–31. [Google Scholar] [CrossRef]
- Gheorghe, L.; Brouwer, J.; Mathijssen, H.; Nijenhuis, V.J.; Rensing, B.J.; Swaans, M.J.; Chan Pin Yin, D.R.; Heijmen, R.H.; De Kroon, T.; Sonker, U.; et al. Early Outcomes After Percutaneous Closure of Access Site in Transfemoral Transcatheter Valve Implantation Using the Novel Vascular Closure Device Collagen Plug-Based MANTA. Am. J. Cardiol. 2019, 124, 1265–1271. [Google Scholar] [CrossRef] [PubMed]
- Van Wiechen, M.P.; Tchétché, D.; Ooms, J.F.; Hokken, T.W.; Kroon, H.; Ziviello, F.; Ghattas, A.; Siddiqui, S.; Laperche, C.; Spitzer, E.; et al. Suture- or Plug-Based Large-Bore Arteriotomy Closure: A Pilot Randomized Controlled Trial. JACC Cardiovasc. Interv. 2021, 14, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, M.; Capranzano, P.; Ohno, Y.; Gulino, S.; Sgroi, C.; Immè, S.; Tamburino, C.; Cannata, S.; Patanè, M.; Di Stefano, D.; et al. Comparison of suture-based vascular closure devices in transfemoral transcatheter aortic valve implantation. EuroIntervention 2015, 11, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Barbash, I.M.; Barbanti, M.; Webb, J.; Molina-Martin De Nicolas, J.; Abramowitz, Y.; Latib, A.; Nguyen, C.; Deuschl, F.; Segev, A.; Sideris, K.; et al. Comparison of vascular closure devices for access site closure after transfemoral aortic valve implantation. Eur. Heart J. 2015, 36, 3370–3379. [Google Scholar] [CrossRef] [PubMed]
- Chieffo, A.; Van Mieghem, N.M.; Tchetche, D.; Dumonteil, N.; Giustino, G.; Van der Boon, R.M.A.; Pierri, A.; Marcheix, B.; Misuraca, L.; Serruys, P.W.; et al. Impact of Mixed Aortic Valve Stenosis on VARC-2 Outcomes and Postprocedural Aortic Regurgitation in Patients Undergoing Transcatheter Aortic Valve Implantation: Results From the International Multicentric Study PRAGMATIC (Pooled Rotterdam-Milan-Toulouse in Collaboration). Catheter. Cardiovasc. Interv. 2015, 86, 875–885. [Google Scholar]
- Van Mieghem, N.M.; Tchetche, D.; Chieffo, A.; Dumonteil, N.; Messika-Zeitoun, D.; van der Boon, R.M.A.; Vahdat, O.; Buchanan, G.L.; Marcheix, B.; Himbert, D.; et al. Incidence, predictors, and implications of access site complications with transfemoral transcatheter aortic valve implantation. Am. J. Cardiol. 2012, 110, 1361–1367. [Google Scholar] [CrossRef] [PubMed]
- Généreux, P.; Webb, J.G.; Svensson, L.G.; Kodali, S.K.; Satler, L.F.; Fearon, W.F.; Davidson, C.J.; Eisenhauer, A.C.; Makkar, R.R.; Bergman, G.W.; et al. Vascular complications after transcatheter aortic valve replacement: Insights from the PARTNER (Placement of AoRTic TraNscathetER Valve) trial. J. Am. Coll. Cardiol. 2012, 60, 1043–1052. [Google Scholar] [CrossRef]
- Lauck, S.B.; Wood, D.A.; Baumbusch, J.; Kwon, J.Y.; Stub, D.; Achtem, L.; Blanke, P.; Boone, R.H.; Cheung, A.; Dvir, D.; et al. Vancouver Transcatheter Aortic Valve Replacement Clinical Pathway: Minimalist Approach, Standardized Care, and Discharge Criteria to Reduce Length of Stay. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 312–321. [Google Scholar] [CrossRef]
- Van Mieghem, N.M.; Latib, A.; van der Heyden, J.; van Gils, L.; Daemen, J.; Sorzano, T.; Ligthart, J.; Witberg, K.; de Kroon, T.; Maor, N.; et al. Percutaneous Plug-Based Arteriotomy Closure Device for Large-Bore Access: A Multicenter Prospective Study. JACC Cardiovasc. Interv. 2017, 10, 613–619. [Google Scholar] [CrossRef]
- Wood, D.A.; Krajcer, Z.; Sathananthan, J.; Strickman, N.; Metzger, C.; Fearon, W.; Aziz, M.; Satler, L.F.; Waksman, R.; Eng, M.; et al. Pivotal Clinical Study to Evaluate the Safety and Effectiveness of the MANTA Percutaneous Vascular Closure Device. Circ. Cardiovasc. Interv. 2019, 12, e007258. [Google Scholar] [CrossRef]
- Moccetti, F.; Brinkert, M.; Seelos, R.; Ockert, S.; Bossard, M.; Cuculi, F.; Kobza, R.; Toggweiler, S. Insights From a Multidisciplinary Introduction of the MANTA Vascular Closure Device. JACC Cardiovasc. Interv. 2019, 12, 1730–1736. [Google Scholar] [CrossRef] [PubMed]
- Halim, J.; Missault, L.; Lycke, M.; Van der Heyden, J. Assessment of the MANTA closure device in transfemoral transcatheter aortic valve replacement: A single-centre observational study. Neth. Heart J. 2020, 28, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Kroon, H.G.; Tonino, P.A.L.; Savontaus, M.; Amoroso, G.; Laine, M.; Christiansen, E.H.; Toggweiler, S.; Ten Berg, J.; Sathananthan, J.; Daemen, J.; et al. Dedicated plug based closure for large bore access—The MARVEL prospective registry. Catheter. Cardiovasc. Interv. 2021, 97, 1270–1278. [Google Scholar] [CrossRef] [PubMed]
- Van Wiechen, M.P.; Kroon, H.; Hokken, T.W.; Ooms, J.F.; de Ronde-Tillmans, M.J.; Daemen, J.; de Jaegere, P.P.; Van Mieghem, N.M. Vascular complications with a plug-based vascular closure device after transcatheter aortic valve replacement: Predictors and bail-outs. Catheter. Cardiovasc. Interv. 2021, 98, E737–E745. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.; Dospinescu, C.; Cunnington, M.S.; Malkin, C.J.; Blackman, D.J. A Comparison of Efficacy, Safety and Cost Between MANTATM and Proglide Vascular Closure Devices Following Transfemoral Transcatheter Aortic Valve Implantation. Heart Res. Open J. 2021, 8, 1–7. [Google Scholar] [CrossRef]
- Dumpies, O.; Kitamura, M.; Majunke, N.; Hartung, P.; Haag, A.; Wilde, J.; Desch, S.; Sandri, M.; Crusius, L.; Noack, T.; et al. Manta versus Perclose ProGlide vascular closure device after transcatheter aortic valve implantation: Initial experience from a large European center. Cardiovasc. Revasc. Med. 2022, 37, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Sarathy, K.; Patel, K.P.; Jones, D.M.; Akhtar, M.; Khanna, V.; Broyd, C.; Ozkor, M.; Kennon, S.; Mathur, A.; Baumbach, A.; et al. Large Bore Vascular Access Closure Device Strategies. Struct. Heart 2021, 5, 186–191. [Google Scholar] [CrossRef]
- Abdel-Wahab, M.; Hartung, P.; Dumpies, O.; Obradovic, D.; Wilde, J.; Majunke, N.; Boekstegers, P.; Müller, R.; Seyfarth, M.; Vorpahl, M.; et al. Comparison of a Pure Plug-Based Versus a Primary Suture-Based Vascular Closure Device Strategy for Transfemoral Transcatheter Aortic Valve Replacement: The CHOICE-CLOSURE Randomized Clinical Trial. Circulation 2022, 145, 170–183. [Google Scholar] [CrossRef]
- Al-Abdouh, A.; Abusnina, W.; Mhanna, M.; Barbarawi, M.; Jabri, A.; Bizanti, A.; Abdel-Latif, A.; Goldsweig, A.M.; Alkhouli, M.; Lichaa, H.; et al. MANTA Versus Suture-based Closure Devices Following Transcatheter Aortic Valve Replacement: An Updated Meta-analysis. J. Soc. Cardiovasc. Angiogr. Interv. 2022, 1, 100397. [Google Scholar] [CrossRef]
- Al-Abcha, A.; Saleh, Y.; Halboni, A.; Wang, E.; Salam, M.F.; Abela, G. Meta-Analysis Investigating the Efficacy and Safety of the MANTA Versus ProGlide Vascular Closure Devices After Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2022, 169, 151–154. [Google Scholar] [CrossRef]
- Mahalwar, G.; Shariff, M.; Datla, S.; Agrawal, A.; Rathore, S.S.; Arif, T.B.; Iqbal, K.; Hussain, N.; Majmundar, M.; Kumar, A.; et al. Meta-analysis of ProGlide versus MANTA vascular closure devices for large-bore access site management. Indian Heart J. 2022, 74, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Doshi, R.; Vasudev, R.; Guragai, N.; Patel, K.N.; Kumar, A.; Majmundar, M.; Doshi, P.; Patel, P.; Shah, K.; Santana, M.; et al. Clinical outcomes of MANTA vs suture-based vascular closure devices after transcatheter aortic valve replacement: An updated meta-analysis. Indian Heart J. 2023, 75, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, K.; Lefèvre, T.; Chevalier, B.; Hovasse, T.; Romano, M.; Garot, P.; Mylotte, D.; Uribe, J.; Farge, A.; Donzeau-Gouge, P.; et al. Transfemoral aortic valve implantation new criteria to predict vascular complications. JACC Cardiovasc. Interv. 2011, 4, 851–858. [Google Scholar] [CrossRef]
- Nara, Y.; Watanabe, Y.; Kozuma, K.; Kataoka, A.; Nakashima, M.; Hioki, H.; Kawashima, H.; Nagura, F.; Shirai, S.; Tada, N.; et al. Incidence, Predictors, and Mid-Term Outcomes of Percutaneous Closure Failure After Transfemoral Aortic Valve Implantation Using an Expandable Sheath (from the Optimized Transcatheter Valvular Intervention [OCEAN-TAVI] Registry). Am. J. Cardiol. 2017, 119, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Ates, M.; Sahin, S.; Konuralp, C.; Gullu, U.; Cimen, S.; Kizilay, M.; Gunay, R.; Sensoz, Y.; Akcar, M. Evaluation of risk factors associated with femoral pseudoaneurysms after cardiac catheterization. J. Vasc. Surg. 2006, 43, 520–524. [Google Scholar] [CrossRef] [PubMed]
- Seto, A.H.; Abu-Fadel, M.S.; Sparling, J.M.; Zacharias, S.J.; Daly, T.S.; Harrison, A.T.; Suh, W.M.; Vera, J.A.; Aston, C.E.; Winters, R.J.; et al. Real-time ultrasound guidance facilitates femoral arterial access and reduces vascular complications: FAUST (Femoral Arterial Access With Ultrasound Trial). JACC Cardiovasc. Interv. 2010, 3, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, N.; Dahlbacka, S.; Vähäsilta, T.; Vainikka, T.; Aho, P.; Viikilä, J.; Lammintausta, O.; Laine, M. The Efficacy of the Ultrasound-Navigated MANTA Deployment Following Transfemoral Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2019, 12, 2564–2566. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vascular Complications (Total/Major/Minor) | Other Closing Devices and Vascular Complications | Risk Factors for Vascular Complications | |
|---|---|---|---|
| Van Mieghem et al., 2017 [19] (n = 50) | Manta (n = 50) Total 2% Major 2% Minor 0% | ||
| Biancari et al., 2018 [10] (n = 222) | Manta (n = 107) Total 13% Major 9.3% Minor 3.7% | Proglide (n = 115) Total 14.8% Major 12.2% Minor 2.6% | |
| Hoffman et al., 2018 [7] (n = 151) | Manta (n =75) Major 10.7% | Proglide (n = 76) Major 2.7% | |
| De Palma et al., 2018 [8] (n = 346) | Manta (n = 107) Major and death 1.1% | Prostar XL (n = 239) Major and death 1.9% | |
| Moriyama et al., 2019 [9] (n = 222) | Manta (n = 111) Total 14% Major 7% Minor 6% | Proglide (n = 111) Total 21% Major 8% Minor 13% |
|
| Wood et al. the SAFE MANTA Study, 2019 [20] (n = 263) | Manta (n = 263) Major 4.2% | ||
| Gheorghe et al., 2019 [11] (n = 366) | Manta (n = 168) Total 11.3% Major 0.6% Minor 10.7% | Prostar XL (n = 198) Total 19.7% Major 1.5% Minor 18.2% | |
| Moccetti et al., 2019 [21] (n = 100) | Manta (n = 100) Total 14% Major 9% Minor 5% |
| |
| Halim et al., 2020 [22] (n = 73) | Manta (n = 73) Total 13.7% Major 0% Minor 13.7% | ||
| Kroon et al., the MARVEL Study 2020 [23] (n = 500) | Manta (n = 500) Total 9.6% Major 4% Minor 5.6% |
| |
| Van Wiechen et al., the MASH study, 2021 [12] (n = 206) | Manta (n = 102) Total 10% Major 2% Minor 8% | Proglide (n = 104) Total 4% Major 0% Minor 4% | |
| Van Wiechen et al., 2021 [24] (n = 512) | Manta (n = 512) Total 8% Major 4% Minor 4% |
| |
| Ali et al., 2021 [25] (n = 136) | Manta (n = 50) Total 10% Major 0% Minor 10% | Proglide (n = 86) Total 10.5% Major 3.5% Minor 7% | |
| Dumpies et al., 2021 [26] (n = 578) | Manta (n = 195) Total 10.7% Major 2% Minor 8.7% | Proglide (n = 383) Total 19% Major 6.5% Minor 12.5% | |
| Sarathy et al., 2021 [27] (n = 132) | Manta (n = 86) Total 18% Major 6% Minor 12% | Proglide (n = 86) Total 13% Major 6% Minor 7% | |
| Abdel Wahab et al., 2022 CHOICE-CLOSURE [28] (n = 516) | Manta (n = 258) Total 20.9% Major 5% Minor 15.9% | Proglide (n = 258) Total 14.7% Major 1.9% Minor 12.8% |
| Total (n = 264) | Manta (n = 132) | Prostar (n = 132) | p | |
|---|---|---|---|---|
| Age | 82.6 +/− 0.5 | 82.6 +/− 5.4 | 82.6 +/− 5.5 | 0.973 |
| Gender% Male/Female | 57/43 (151/113) | 54.5/45.5 (72/60) | 59.8/41.2 (79/53) | 0.384 |
| Body Mass Index (BMI) | 26.0 +/− 4.3 | 26.12 +/− 4.16 | 25.90 +/− 4.45 | 0.674 |
| Euroscore logistic | 8.8 +/− 7 | 8.61 +/− 7.13 | 8.99 +/− 6.93 | 0.659 |
| HBP | 77.3% (204/264) | 74.2% (98/132) | 80.3% (106/132) | 0.240 |
| Dyslipidemia | 53.4% (141/264) | 53% (70/132) | 53.8% (71/132) | 0.902 |
| Smoking No Active Cessation | 68.9% (182/264) 1.9% (5/264) 29.2% (77/264) | 65.9% (87/132) 2.3% (3/132) 31.8% (42/132) | 72.0% (95/132) 1.5% (2/132) 26.5% (35/132) | 0.552 |
| Diabetes | 17.4% (46/264) | 15.1% (20/132) | 19.7% (26/132) | 0.330 |
| Stroke | 7.2% (19/264) | 9% (12/132) | 5.3% (7/132) | 0.234 |
| Previous coronary bypass surgery | 6.4% (17/264) | 6% (8/132) | 6.8% (9/132) | 0.802 |
| Aortic valve bioprosthesis | 1.9% (5/264) | 1.5% (2/132) | 2.3% (3/132) | 0.652 |
| Previous coronary stenting | 19.3% (51/264) | 22.7% (30/132) | 15.9% (21/132) | 0.161 |
| PAD | 6.8% (18/264) | 6.8% (9/132) | 6.8% (9/132) | 0.802 |
| Pacemaker | 9.1% (24/264) | 10.6% (14/132) | 7.6% (10/132) | 0.392 |
| Atrial fibrillation | 15.1% (40/264) | 17.4% (23/132) | 14.4% (19/132) | 0.501 |
| Anticoagulation | 31% (82/264) | 25.7% (34/132) | 36.3% (48/132) | 0.063 |
| Hemoglobin (g/dL) | 12.4 +/− 1.4 | 12.36 +/− 1.41 | 12.39 +/− 1.47 | 0.878 |
| Platelets (G/L) | 221 +/− 69 | 230 +/− 77 | 213 +/− 60 | 0.046 * |
| GFR (mL/mn) | 57.3 +/− 22.8 | 55.84 +/− 21.31 | 58.75 +/− 24.20 | 0.302 |
| Total (n = 264) | Manta (n = 132) | Prostar (n = 132) | p | |
|---|---|---|---|---|
| Laterality Right Left | 75% 25% | 67.4% (89/132) 32.5% (43/132) | 81.8% (108/132) 18.2% (24/132) | 0.007 * |
| Diameter (mm) | 7.64 +/− 1.07 | 7.5 +/− 1.0 | 7.8 +/− 1.1 | 0.038 * |
| Sheath/femoral ratio | 0.83 +/−0.11 | 0.84 +/− 0.11 | 0.82 +/− 0.12 | 0.098 |
| Calcifications 0 I II III | 12.5% (33/264) 37.9% (100/264) 37.1% (98/264) 12.5% (33/264) | 10.6% (14/132) 41.7% (55/132) 40.2% (53/132) 7.7% (10/132) | 14.4% (19/132) 34.1% (45/132) 34.1% (45/132) 17.4% (23/132) | 0.057 |
| Calcification location Anterior Medial Lateral Posterior | 12.5% (33/264) 46.6% (123/264) 11.7% (31/264) 71.6% (189/264) | 12.9% (17/132) 46.2% (61/132) 11.4% (15/132) 67.4% (89/132) | 12.1% (16/132) 46.9% (62/132) 12.1% (16/132) 75.8% (100/132) | 0.852 0.902 0.848 0.133 |
| High bifurcation | 9.1% (24/264) | 8.3% (11/132) | 9.8% (13/132) | 0.669 |
| Tortuosity Mild Moderate Severe | 39.4% (104/264) 44.7% (118/264) 15.5% (41/264) | 40.9% (54/132) 47% (62/132) 12.1% (16/132) | 37.9% (50/132) 42.4% (56/132) 18.9% (25/132) | 0.297 |
| Valve implanted Acurate Neo Corevalve Sapiens Portico | 9.1% (24/264) 28.8% (76/264) 60.7% (159/264) 1.1% (3/264) | 11.3% (15/132) 29.5% (39/132) 55.3% (73/132) 2.3% (3/132) | 6.8% (9/132) 28% (37/132) 65.1% (86/132) 0% (0/132) | 0.133 |
| Sheath size (mm) | 6.2 +/− 0.32 | 6.2 +/− 0.32 | 6.2 +/− 0.33 | 0.277 |
| Secondary access Radial Femoral Humeral | 62.9% (176/264) 36.0% (95/264) 1.1% (3/264) | 67.4% (89/132) 31.1% (41/132) 1.5% (2/132) | 58.3% (77/132) 40.9% (54/132) 0.8% (1/132) | 0.225 |
| Total (n =264) | Manta (n = 132) | Prostar (n = 132) | p | |
|---|---|---|---|---|
| Death | 0.4% (1/264) | 0% (0/132) | 0.8% (1/132) | 0.316 |
| Vascular complications Total Major Minor | 17.4% (46/264) 1.1% (3/264) 16.3% (43/264) | 13.6% (18/132) 1.5% (2/132) 12.1% (16/132) | 21.2% (28/132) 0.8% (1/132) 20.5% (27/132) | 0.105 0.561 0.067 |
| Stenosis | 2.3% (6/264) | 4.5% (6/132) | 0% (0/132) | 0.013 * |
| Lower limb ischemia | 0.8% (2/264) | 1.5% (2/132) | 0% (0/132) | 0.156 |
| False aneurysm | 4.5% (12/264) | 3.8% (5/132) | 5.3% (7/132) | 0.555 |
| Arteriovenous fistula | 1.9% (5/264) | 1.5%(2/132) | 2.3% (3/132) | 0.652 |
| Dissection | 3% (8/264) | 2.3% (3/132) | 3.8% (5/132) | 0.473 |
| Closure failure | 9.1% (24/264) | 4.5% (6/132) | 13.6% (18/132) | 0.01 * |
| Bleeding Total Major Minor | 9.5% (25/264) 1.1% (3/264) 8.3% (22/264) | 3.8% (5/132) 0.8% (1/132) 3% (4/132) | 15.2% (20/132) 1.5% (2/132) 13.6% (18/132) | 0.002 * 0.561 0.002 * |
| Covered stent | 8.7% (23/264) | 4.5% (6/132) | 12.9% (17/132) | 0.016 * |
| Vascular surgery | 1.9% (5/264) | 1.5% (2/132) | 2.3% (3/132) | 0.652 |
| Transfusion | 3.8% (10/264) | 1.5% (2/132) | 6% (8/132) | 0.053 |
| Length of stay (days) | 5.95 +/− 5.0 | 4.9 +/− 3.9 | 7.0 +/− 5.7 | 0.001 * |
| Amount contrast medium (mL) | 76.2 +/− 28.5 | 77.3 +/− 27.6 | 75.1 +/− 29.5 | 0.537 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Complications (n = 46) | No Complication (n = 218) | p | OR | IC 95 | p | |
| Diabetes | 30.4% (14/46) | 14.7% (32/218) | 0.01 * | 2.49 | 1.16–5.3 | 0.019 * |
| Sheath/femoral ratio (%) | 87.5 +/− 11.5 | 81.1 +/− 13.7 | 0.003 * | 1.045 | 1.02–1.07 | 0.002 * |
| Euroscore logistic | 9.53 +/− 1.41 | 6.33 +/− 0.43 | 0.043 * | 1.046 | 1.002–1.092 | 0.042 * |
| Creatinine (micromoles/L) | 112.37 +/− 91.94 | 90.33 +/− 42.84 | 0.013 * | 1.005 | 1–1.010 | 0.046 |
| Diameter of the common femoral artery (mm) | 7.26 +/− 1.09 | 7.72 +/− 1.07 | 0.009 * | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benic, C.; Nicol, P.P.; Hannachi, S.; Gilard, M.; Didier, R.; Nasr, B. Vascular Complications Following Transcatheter Aortic Valve Implantation, Using MANTA (Collagen Plug-Based) versus PROSTAR (Suture-Based), from a French Single-Center Retrospective Registry. J. Clin. Med. 2023, 12, 6697. https://doi.org/10.3390/jcm12206697
Benic C, Nicol PP, Hannachi S, Gilard M, Didier R, Nasr B. Vascular Complications Following Transcatheter Aortic Valve Implantation, Using MANTA (Collagen Plug-Based) versus PROSTAR (Suture-Based), from a French Single-Center Retrospective Registry. Journal of Clinical Medicine. 2023; 12(20):6697. https://doi.org/10.3390/jcm12206697
Chicago/Turabian StyleBenic, Clément, Pierre Philippe Nicol, Sinda Hannachi, Martine Gilard, Romain Didier, and Bahaa Nasr. 2023. "Vascular Complications Following Transcatheter Aortic Valve Implantation, Using MANTA (Collagen Plug-Based) versus PROSTAR (Suture-Based), from a French Single-Center Retrospective Registry" Journal of Clinical Medicine 12, no. 20: 6697. https://doi.org/10.3390/jcm12206697
APA StyleBenic, C., Nicol, P. P., Hannachi, S., Gilard, M., Didier, R., & Nasr, B. (2023). Vascular Complications Following Transcatheter Aortic Valve Implantation, Using MANTA (Collagen Plug-Based) versus PROSTAR (Suture-Based), from a French Single-Center Retrospective Registry. Journal of Clinical Medicine, 12(20), 6697. https://doi.org/10.3390/jcm12206697