
Cardiovascular Magnetic Resonance in Patients with Cardiac Electronic Devices: Evidence from a Multicenter Study

 ,
,  , , , , , , , ,
, , , , , , , ,  , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. CMR Imaging
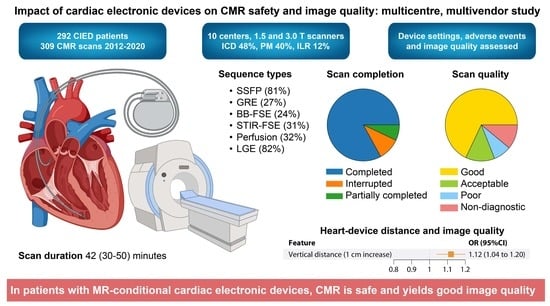
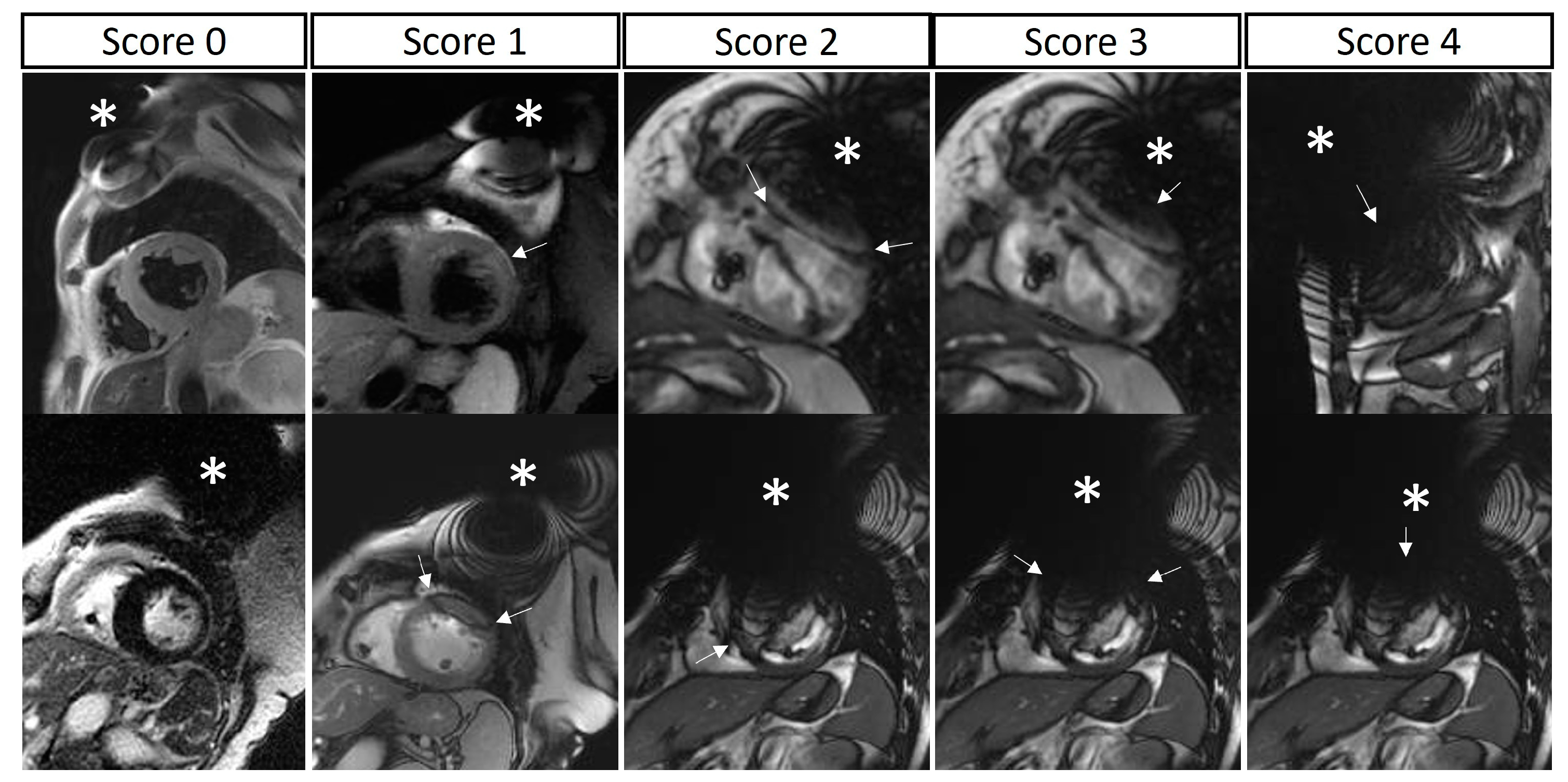
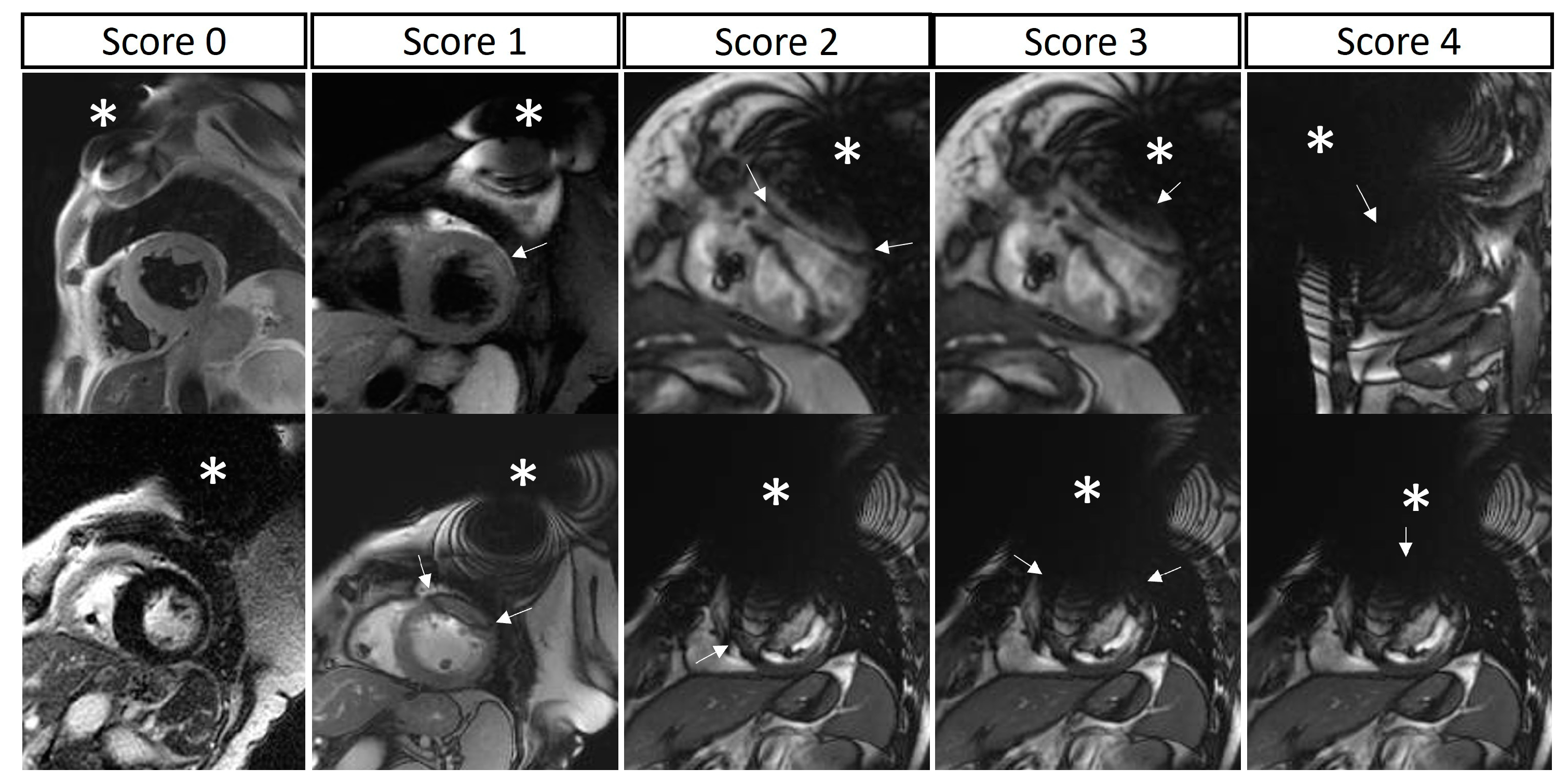
2.3. Image Quality Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 17. [Google Scholar] [CrossRef]
- Levine, G.N.; Gomes, A.S.; Arai, A.E.; Bluemke, D.A.; Flamm, S.D.; Kanal, E.; Manning, W.J.; Martin, E.T.; Smith, J.M.; Wilke, N.; et al. Safety of magnetic resonance imaging in patients with cardiovascular devices: An American heart association scientific statement from the committee on diagnostic and interventional cardiac catheterization, council on clinical cardiology, and the council on cardiovascular radiology and intervention. Circulation 2007, 116, 2878–2891. [Google Scholar] [CrossRef]
- Dill, T. Contraindications to magnetic resonance imaging. Heart 2008, 94, 943–948. [Google Scholar] [CrossRef]
- Shellock, F.G.; Crues, J.V. MR safety and the American College of Radiology White Paper. Am. J. Roentgenol. 2002, 178, 1349–1352. [Google Scholar] [CrossRef] [PubMed]
- Kanal, E.; Barkovich, A.J.; Bell, C.; Borgstede, J.P.; Bradley, W.G.; Froelich, J.W.; Gimbel, J.R.; Gosbee, J.W.; Kuhni-Kaminski, E.; Larson, P.A.; et al. ACR guidance document on MR safe practices: 2013. J. Magn. Reson. Imaging 2013, 37, 501–530. [Google Scholar] [CrossRef] [PubMed]
- Barison, A.; Baritussio, A.; Cipriani, A.; De Lazzari, M.; Aquaro, G.D.; Guaricci, A.I.; Pica, S.; Pontone, G.; Todiere, G.; Indolfi, C.; et al. Cardiovascular magnetic resonance: What clinicians should know about safety and contraindications. Int. J. Cardiol. 2021, 331, 322–328. [Google Scholar] [CrossRef]
- Miller, J.D.; Nazarian, S.; Halperin, H.R. Implantable Electronic Cardiac Devices and Compatibility with Magnetic Resonance Imaging. J. Am. Coll. Cardiol. 2016, 68, 1590–1598. [Google Scholar] [CrossRef] [PubMed]
- Symons, R.; Zimmerman, S.L.; Bluemke, D.A. CMR and CT of the Patient with Cardiac Devices: Safety, Efficacy, and Optimization Strategies. JACC Cardiovasc. Imaging 2019, 12, 890–903. [Google Scholar] [CrossRef] [PubMed]
- Stühlinger, M.; Burri, H.; Vernooy, K.; Garcia, R.; Lenarczyk, R.; Sultan, A.; Brunner, M.; Sabbag, A.; Özcan, E.E.; Ramos, J.T.; et al. EHRA consensus on prevention and management of interference due to medical procedures in patients with cardiac implantable electronic devices for the European Heart Rhythm Association (EHRA), Heart Rhythm Society (HRS), Latin America Heart Rhythm Society (LAHRS), Asian Pacific Heart Rhythm Society (APHRS). EP Eur. 2022, 24, 1512–1537. [Google Scholar] [CrossRef]
- Blaschke, F.; Lacour, P.; Walter, T.; Wutzler, A.; Huemer, M.; Parwani, A.; Attanasio, P.; Boldt, L.H.; Markowski, M.; Denecke, T.; et al. Cardiovascular Magnetic Resonance Imaging in Patients with an Implantable Loop Recorder. Ann. Noninvasive Electrocardiol. 2016, 21, 319–324. [Google Scholar] [CrossRef]
- Sasaki, T.; Hansford, R.; Zviman, M.M.; Kolandaivelu, A.; Bluemke, D.A.; Berger, R.D.; Calkins, H.; Halperin, H.R.; Nazarian, S. Quantitative assessment of artifacts on cardiac magnetic resonance imaging of patients with pacemakers and implantable cardioverter-defibrillators. Circ. Cardiovasc. Imaging 2011, 4, 662–670. [Google Scholar] [CrossRef] [PubMed]
- Schwitter, J.; Kanal, E.; Schmitt, M.; Anselme, F.; Albert, T.; Hayes, D.L.; Bello, D.; Tóth, A.; Chang, Y.; Van Osch, D.; et al. Impact of the Advisa MRI pacing system on the diagnostic quality of cardiac MR images and contraction patterns of cardiac muscle during scans: Advisa MRI randomized clinical multicenter study results. Heart Rhythm 2013, 10, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Raphael, C.E.; Vassiliou, V.; Alpendurada, F.; Prasad, S.K.; Pennell, D.J.; Mohiaddin, R.H. Clinical value of cardiovascular magnetic resonance in patients with MR-conditional pacemakers. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Hilbert, S.; Jahnke, C.; Loebe, S.; Oebel, S.; Weber, A.; Spampinato, R.; Richter, S.; Doering, M.; Bollmann, A.; Sommer, P.; et al. Cardiovascular magnetic resonance imaging in patients with cardiac implantable electronic devices: A device-dependent imaging strategy for improved image quality. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1051–1061. [Google Scholar] [CrossRef]
- Löbe, S.; Paetsch, I.; Hilbert, S.; Spampinato, R.; Oebel, S.; Richter, S.; Döring, M.; Sommer, P.; Bollmann, A.; Hindricks, G.; et al. Evaluation of the right heart using cardiovascular magnetic resonance imaging in patients with cardiac devices. Int. J. Cardiol. 2020, 316, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Schwitter, J.; Gold, M.R.; Al Fagih, A.; Lee, S.; Peterson, M.; Ciuffo, A.; Zhang, Y.; Kristiansen, N.; Kanal, E.; Sommer, T. Image Quality of Cardiac Magnetic Resonance Imaging in Patients with an Implantable Cardioverter Defibrillator System Designed for the Magnetic Resonance Imaging Environment. Circ. Cardiovasc. Imaging 2016, 9, e004025. [Google Scholar] [CrossRef]
- Ibrahim, E.-S.H.; Runge, M.; Stojanovska, J.; Agarwal, P.; Ghadimi-Mahani, M.; Attili, A.; Chenevert, T.; den Harder, C.; Bogun, F. Optimized cardiac magnetic resonance imaging inversion recovery sequence for metal artifact reduction and accurate myocardial scar assessment in patients with cardiac implantable electronic devices. World J. Radiol. 2018, 10, 100–107. [Google Scholar] [CrossRef]
- Do, D.H.; Eyvazian, V.; Bayoneta, A.J.; Hu, P.; Finn, J.P.; Bradfield, J.S.; Shivkumar, K.; Boyle, N.G. Cardiac magnetic resonance imaging using wideband sequences in patients with nonconditional cardiac implanted electronic devices. Heart Rhythm 2018, 15, 218–225. [Google Scholar] [CrossRef]
- Bhuva, A.N.; Kellman, P.; Graham, A.; Ramlall, M.; Boubertakh, R.; Feuchter, P.; Hawkins, A.; Lowe, M.; Lambiase, P.D.; Sekhri, N.; et al. Clinical impact of cardiovascular magnetic resonance with optimized myocardial scar detection in patients with cardiac implantable devices. Int. J. Cardiol. 2019, 279, 72–78. [Google Scholar] [CrossRef]
- Kocyigit, D.; Abozeed, M.; Kwon, D.H.; Flamm, S.D.; Wilkoff, B.L.; Jellis, C.L. Predictors of Cardiac Implantable Electronic Device Artifact on Cardiac MRI: The Utility of a Device Related Score. Heart Lung Circ. 2021, 30, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Pavon, A.G.; Porretta, A.P.; Arangalage, D.; Domenichini, G.; Rutz, T.; Hugelshofer, S.; Pruvot, E.; Monney, P.; Pascale, P.; Schwitter, J. Feasibility of adenosine stress cardiovascular magnetic resonance perfusion imaging in patients with MR-conditional transvenous permanent pacemakers and defibrillators. J. Cardiovasc. Magn. Reson. 2022, 24, 9. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.; Airapetov, S.; Pillai, A.; Kalahasty, G.; Ellenbogen, K.A.; Gregory Hundley, W.; Trankle, C.R. Hemodynamic response and safety of vasodilator stress cardiovascular magnetic resonance in patients with permanent pacemakers or implantable cardioverter-defibrillators. J. Cardiovasc. Electrophysiol. 2022, 33, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Kiblboeck, D.; Reiter, C.; Kammler, J.; Schmit, P.; Blessberger, H.; Kellermair, J.; Fellner, F.; Steinwender, C. Artefacts in 1.5 Tesla and 3 Tesla cardiovascular magnetic resonance imaging in patients with leadless cardiac pacemakers. J. Cardiovasc. Magn. Reson. 2018, 20, 47. [Google Scholar] [CrossRef]
- Vuorinen, A.M.; Lehmonen, L.; Karvonen, J.; Holmström, M.; Kivistö, S.; Kaasalainen, T. Reducing cardiac implantable electronic device-induced artefacts in cardiac magnetic resonance imaging. Eur. Radiol. 2023, 33, 1229–1242. [Google Scholar] [CrossRef] [PubMed]
- Penso, M.; Babbaro, M.; Moccia, S.; Guglielmo, M.; Carerj, M.L.; Giacari, C.M.; Chiesa, M.; Maragna, R.; Rabbat, M.G.; Barison, A.; et al. Cardiovascular magnetic resonance images with susceptibility artifacts: Artificial intelligence with spatial-attention for ventricular volumes and mass assessment. J. Cardiovasc. Magn. Reson. 2022, 24, 62. [Google Scholar] [CrossRef] [PubMed]
- Rod Gimbel, J.; Bello, D.; Schmitt, M.; Merkely, B.; Schwitter, J.; Hayes, D.L.; Sommer, T.; Schloss, E.J.; Chang, Y.; Willey, S.; et al. Randomized trial of pacemaker and lead system for safe scanning at 1.5 Tesla. Heart Rhythm 2013, 10, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.R.; Sommer, T.; Schwitter, J.; Kanal, E.; Bernabei, M.A.; Love, C.J.; Surber, R.; Ramza, B.; Cerkvenik, J.; Merkely, B. Impact of magnetic resonance imaging on ventricular tachyarrhythmia sensing: Results of the Evera MRI Study. Heart Rhythm 2016, 13, 1631–1635. [Google Scholar] [CrossRef]
- Shah, A.D.; Morris, M.A.; Hirsh, D.S.; Warnock, M.; Huang, Y.; Mollerus, M.; Merchant, F.M.; Patel, A.M.; Delurgio, D.B.; Patel, A.U.; et al. Magnetic resonance imaging safety in nonconditional pacemaker and defibrillator recipients: A meta-analysis and systematic review. Heart Rhythm 2018, 15, 1001–1008. [Google Scholar] [CrossRef]
- Munawar, D.A.; Chan, J.E.Z.; Emami, M.; Kadhim, K.; Khokhar, K.; O’shea, C.; Iwai, S.; Pitman, B.; Linz, D.; Munawar, M.; et al. Magnetic resonance imaging in non-conditional pacemakers and implantable cardioverter-defibrillators: A systematic review and meta-analysis. EP Eur. 2020, 22, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Bhuva, A.N.; Moralee, R.; Brunker, T.; Lascelles, K.; Cash, L.; Patel, K.P.; Lowe, M.; Sekhri, N.; Alpendurada, F.; Pennell, D.J.; et al. Evidence to support magnetic resonance conditional labelling of all pacemaker and defibrillator leads in patients with cardiac implantable electronic devices. Eur. Heart J. 2022, 43, 2469–2478. [Google Scholar] [CrossRef]
- Ma, Y.D.; Watson, R.E.; Olson, N.E.; Birgersdotter-Green, U.; Patel, K.; Mulpuru, S.K.; Madhavan, M.; Deshmukh, A.J.; Killu, A.M.; Friedman, P.A.; et al. Safety of magnetic resonance imaging in patients with surgically implanted permanent epicardial leads. Heart Rhythm 2023, 20, 1111–1118. [Google Scholar] [CrossRef]
- Vuorinen, A.M.; Paakkanen, R.; Karvonen, J.; Sinisalo, J.; Holmström, M.; Kivistö, S.; Peltonen, J.I.; Kaasalainen, T. Magnetic resonance imaging safety in patients with abandoned or functioning epicardial pacing leads. Eur. Radiol. 2022, 32, 3830–3838. [Google Scholar] [CrossRef] [PubMed]
- Gakenheimer-Smith, L.; Etheridge, S.P.; Niu, M.C.; Ou, Z.; Presson, A.P.; Whitaker, P.; Su, J.; Puchalski, M.D.; Asaki, S.Y.; Pilcher, T. MRI in pediatric and congenital heart disease patients with CIEDs and epicardial or abandoned leads. Pacing Clin. Electrophysiol. 2020, 43, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Schaller, R.D.; Brunker, T.; Riley, M.P.; Marchlinski, F.E.; Nazarian, S.; Litt, H. Magnetic Resonance Imaging in Patients with Cardiac Implantable Electronic Devices with Abandoned Leads. JAMA Cardiol. 2021, 6, 549–556. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
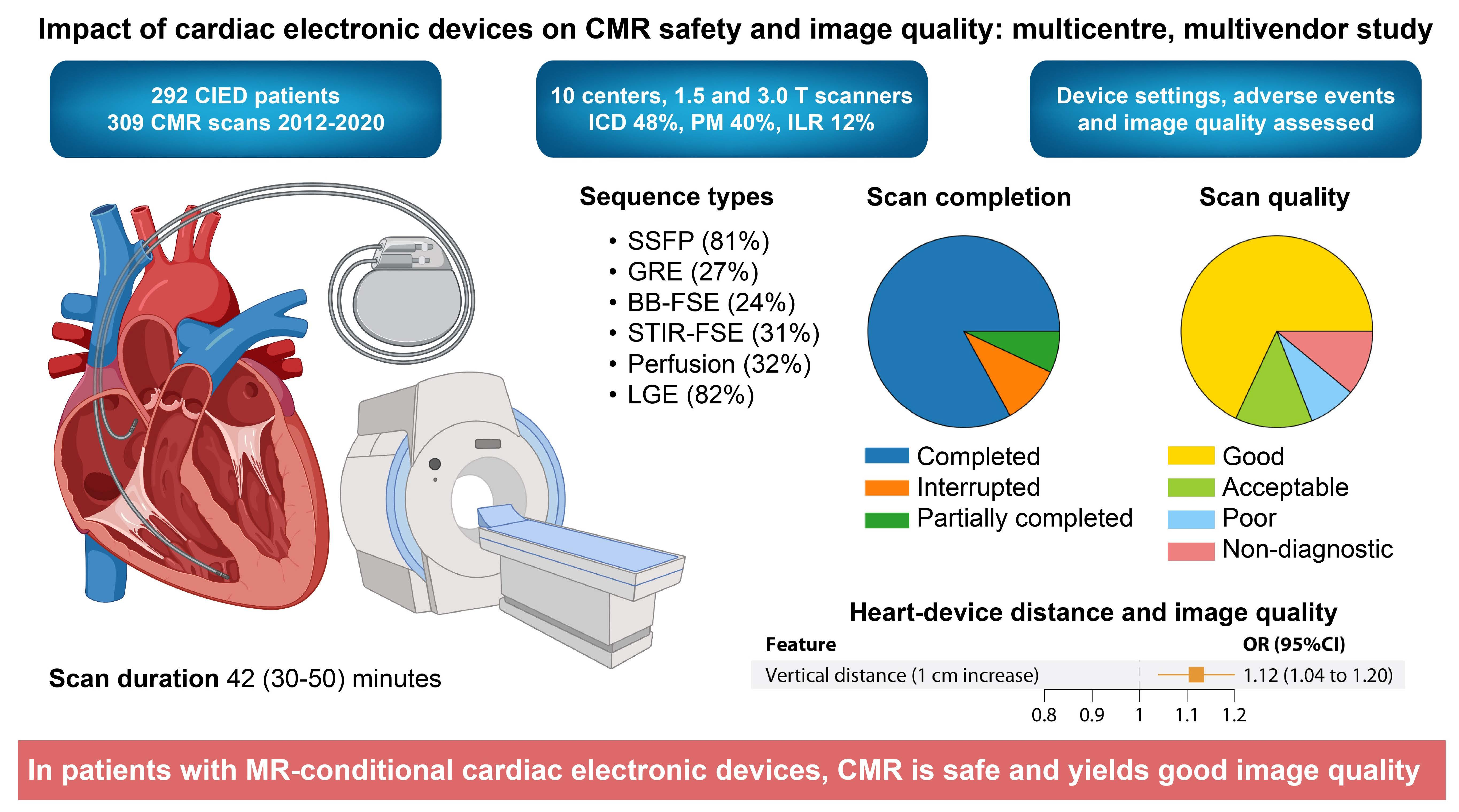
| Sample Size, n | 309 |
|---|---|
| Age, years | 60 (48–70) |
| Male, n (%) | 144 (74.6%) |
| BSA, Kg/m2 | 1.91 (1.71–2.04) |
| Hypertension, n (%) | 122 (42.1%) |
| Dyslipidemia, n (%) | 107 (34.6%) |
| Diabetes, n (%) | 58 (20.0%) |
| Implant to CMR time, months | 12.3 (5.7–29.4) |
| Etiology | |
| Non-ischemic heart disease, n (%) | 169 (54.9%) |
| Conduction disorders, n (%) | 53 (17.2%) |
| Ischemic heart disease, n (%) | 76 (24.7%) |
| Valvular heart disease, n (%) | 10 (3.2%) |
| Sequences, n (%) | Overall Scans | ICD | PM | ILR |
|---|---|---|---|---|
| 309 (100%) | 149 (48.2%) | 122 (39.5%) | 38 (12.3%) | |
| SSFP | 250 (80.9%) | 107 (71.8%) | 106 (86.9%) | 37 (97.4%) |
| GRE | 82 (26.5%) | 56 (37.6%) | 24 (19.7%) | 2 (5.3%) |
| BB-FSE | 73 (23.6%) | 33 (22.1%) | 12 (9.8%) | 28 (73.7%) |
| STIR-FSE | 95 (30.7%) | 44 (29.5%) | 39 (32.0%) | 12 (31.6%) |
| Perfusion | 98 (31.7%) | 48 (32.2%) | 46 (37.7%) | 4 (10.5%) |
| LGE | 252 (81.6%) | 114 (76.5%) | 107 (87.7%) | 31 (81.6%) |
| Scan duration, min | 42 (30–50) | 40 (25–50) | 43 (34–50) | 44 (29–56) |
| Overall Quality | Non-Diagnostic | Poor | Acceptable | Good | p |
|---|---|---|---|---|---|
| Number of CMR scans | 34 | 25 | 40 | 210 | |
| Age, years | 54 (42–65) | 58 (43–67) | 58 (45–70) | 61 (50–72) | 0.107 |
| BSA, Kg/m2 | 1.90 (1.71–20.7) | 1.91 (1.73–2.06) | 1.94 (1.72–2.10) | 1.90 (1.71–2.04) | 0.924 |
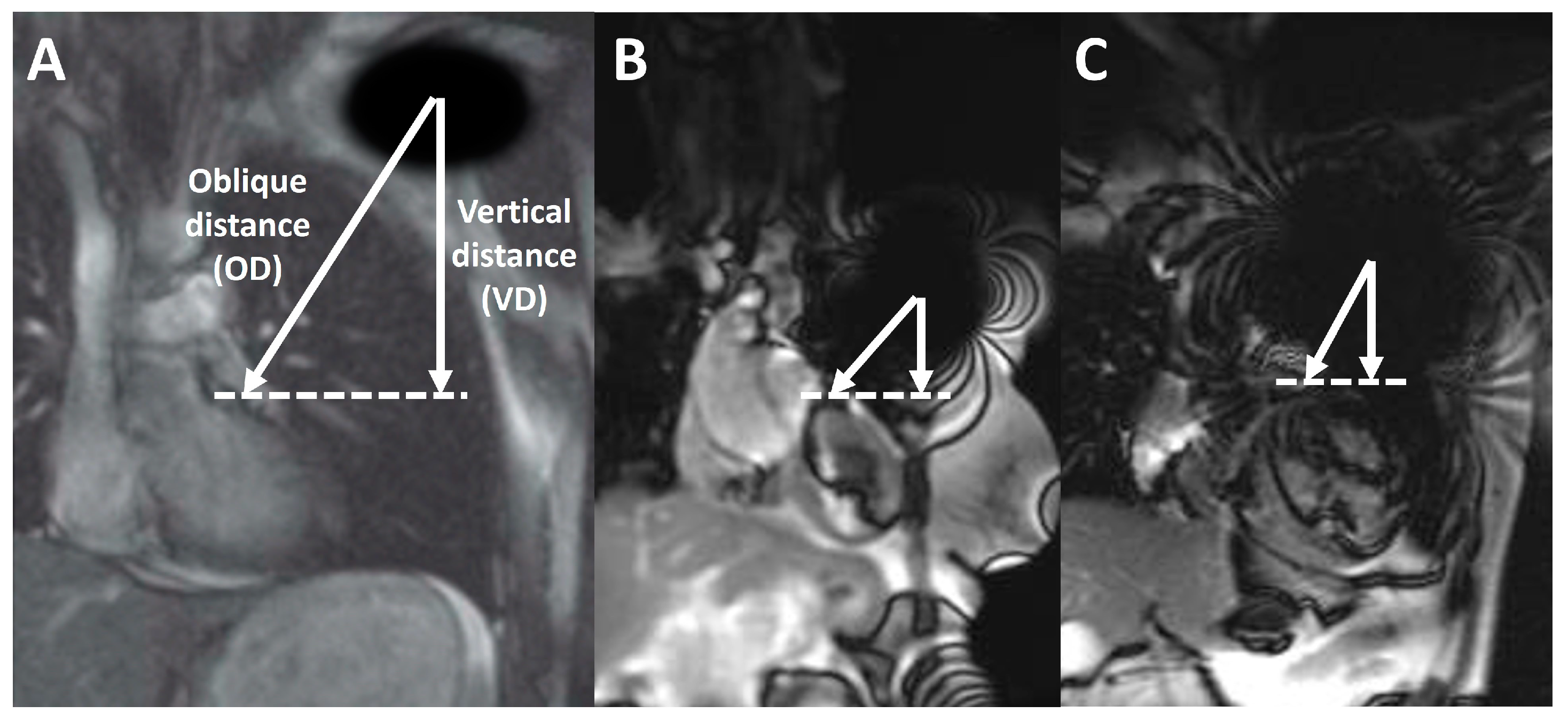
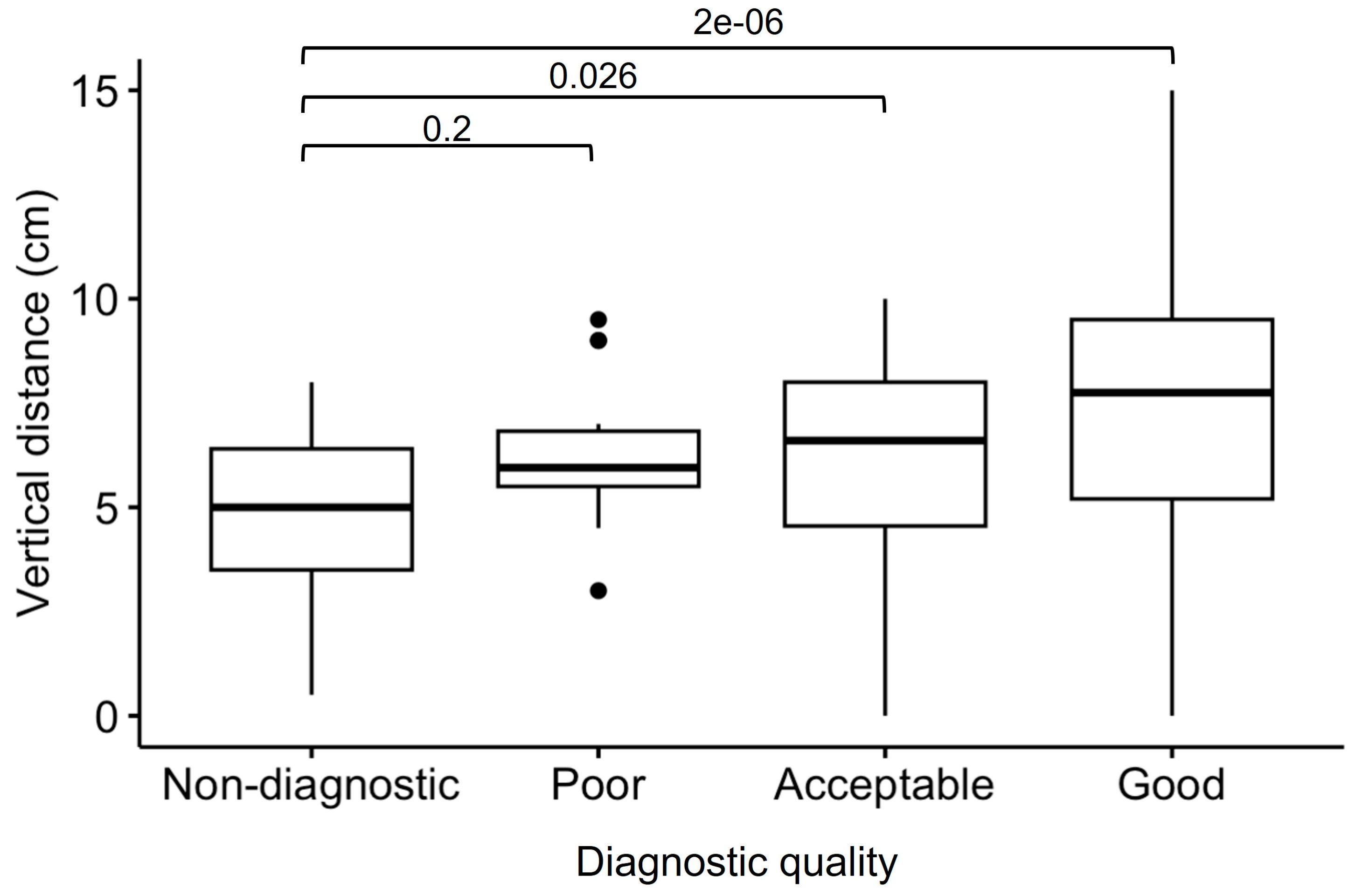
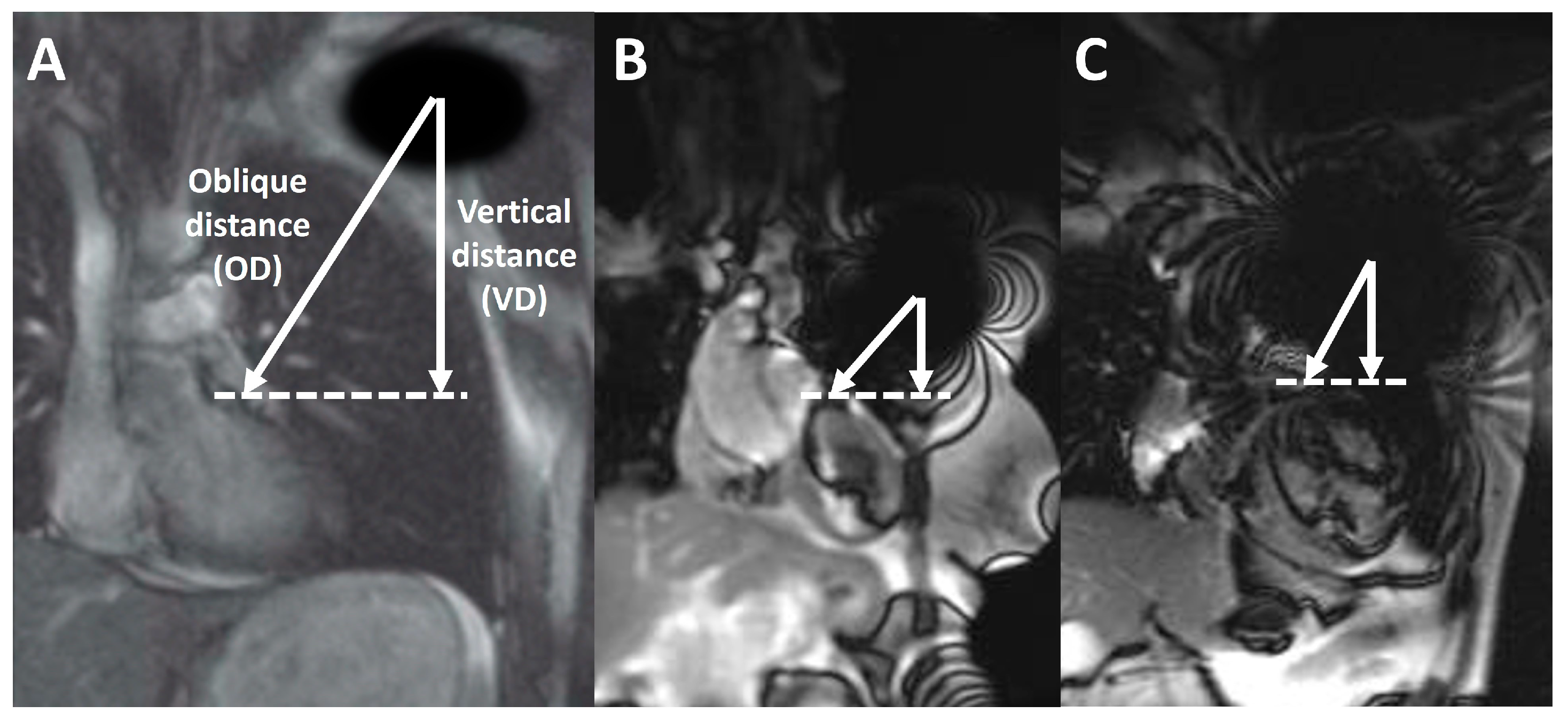
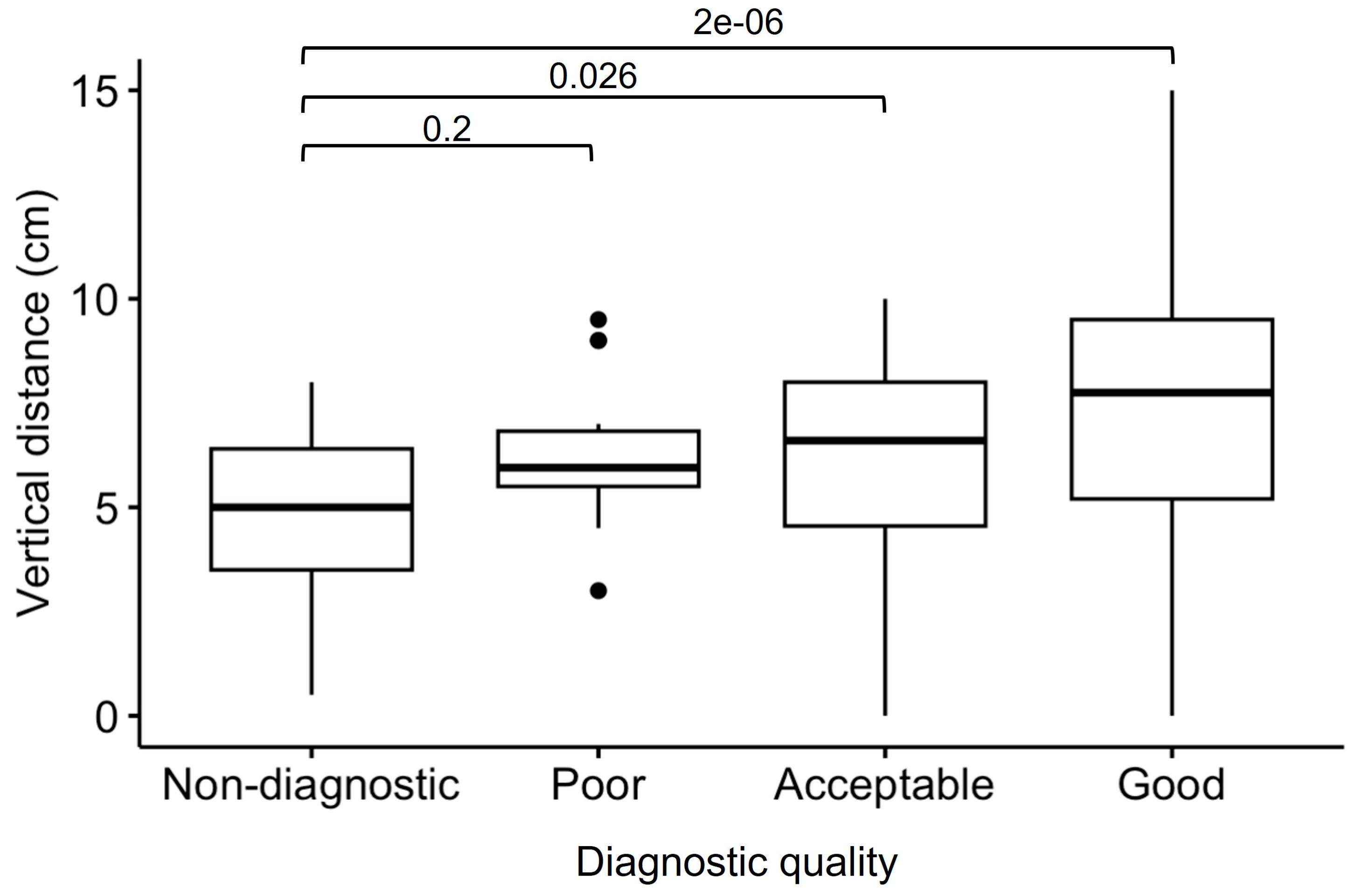
| Vertical distance, cm | 4.3 (1.6–6.2) | 5.5 (3.8–6.8) | 6.5 (3.1–8.0) | 7.5 (4.8–9.5) | <0.001 |
| Oblique distance, cm | 7.9 (6.6–8.7) | 9.2 (7.9–10.7) | 9.2 (8.4–10.8) | 9.3 (7.2–11.0) | 0.553 |
| Overall Quality, n (%) | ICD (n = 149) | ILR (n = 38) | PM (n = 22) | p-Value |
|---|---|---|---|---|
| Non-diagnostic | 25 (16.8) | 6 (15.8) | 3 (2.5) | <0.001 |
| Poor | 23 (15.4) | 1 (2.6) | 1 (0.8) | |
| Acceptable | 32 (21.5) | 1 (2.6) | 7 (5.7) | |
| Good | 69 (46.3) | 30 (78.9) | 111 (91.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barison, A.; Ricci, F.; Pavon, A.G.; Muscogiuri, G.; Bisaccia, G.; Camastra, G.; De Lazzari, M.; Lanzillo, C.; Raguso, M.; Monti, L.; et al. Cardiovascular Magnetic Resonance in Patients with Cardiac Electronic Devices: Evidence from a Multicenter Study. J. Clin. Med. 2023, 12, 6673. https://doi.org/10.3390/jcm12206673
Barison A, Ricci F, Pavon AG, Muscogiuri G, Bisaccia G, Camastra G, De Lazzari M, Lanzillo C, Raguso M, Monti L, et al. Cardiovascular Magnetic Resonance in Patients with Cardiac Electronic Devices: Evidence from a Multicenter Study. Journal of Clinical Medicine. 2023; 12(20):6673. https://doi.org/10.3390/jcm12206673
Chicago/Turabian StyleBarison, Andrea, Fabrizio Ricci, Anna Giulia Pavon, Giuseppe Muscogiuri, Giandomenico Bisaccia, Giovanni Camastra, Manuel De Lazzari, Chiara Lanzillo, Mario Raguso, Lorenzo Monti, and et al. 2023. "Cardiovascular Magnetic Resonance in Patients with Cardiac Electronic Devices: Evidence from a Multicenter Study" Journal of Clinical Medicine 12, no. 20: 6673. https://doi.org/10.3390/jcm12206673
APA StyleBarison, A., Ricci, F., Pavon, A. G., Muscogiuri, G., Bisaccia, G., Camastra, G., De Lazzari, M., Lanzillo, C., Raguso, M., Monti, L., Vargiu, S., Pedrotti, P., Piacenti, M., Todiere, G., Pontone, G., Indolfi, C., Dellegrottaglie, S., Lombardi, M., Schwitter, J., ... on behalf of the Working Group on Cardiovascular Magnetic Resonance of the Italian Society of Cardiology. (2023). Cardiovascular Magnetic Resonance in Patients with Cardiac Electronic Devices: Evidence from a Multicenter Study. Journal of Clinical Medicine, 12(20), 6673. https://doi.org/10.3390/jcm12206673