
Improvements in Maximum Bite Force with Gum-Chewing Training in Older Adults: A Randomized Controlled Trial

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
- (1)
- Individuals aged 65–85 years.
- (2)
- Complaints about the inability to masticate stiff foods in comparison to 6 months ago.
- (3)
- Independence in daily living activities, including toileting, bathing, walking, eating, and dressing.
- (4)
- No previous history of masticatory disorders secondary to muscular disease.
- (5)
- No cognitive issues.
- (6)
- Did not receive any dental treatment during participation in the trial.
- (7)
- At least 20 functional teeth (current number of teeth + number of prosthetic teeth).
- (8)
- Able to masticate chewing gum and granular food.
- (9)
- No gelatin allergies.
- (1)
- The participant did not meet the eligibility criteria.
- (2)
- The participant wanted to retract his/her agreement.
- (3)
- Problems that would prevent the study’s continuation occurred during the intervention period.
- (4)
- The intake rate of test samples during the intervention period was <80%.
- (5)
- The test samples were not consumed for more than five consecutive days.
2.3. Intervention
2.4. Outcomes
2.4.1. Maximum Bite Force and Occlusal Contact Areas
2.4.2. Oral Dryness
2.4.3. Tongue Pressure
2.4.4. Tongue and Lip Functions
2.4.5. Masticatory Function
2.4.6. Gum-Chewing Time
2.5. Sample Size
2.6. Randomization and Blinding
2.7. Statistical Analysis
3. Results
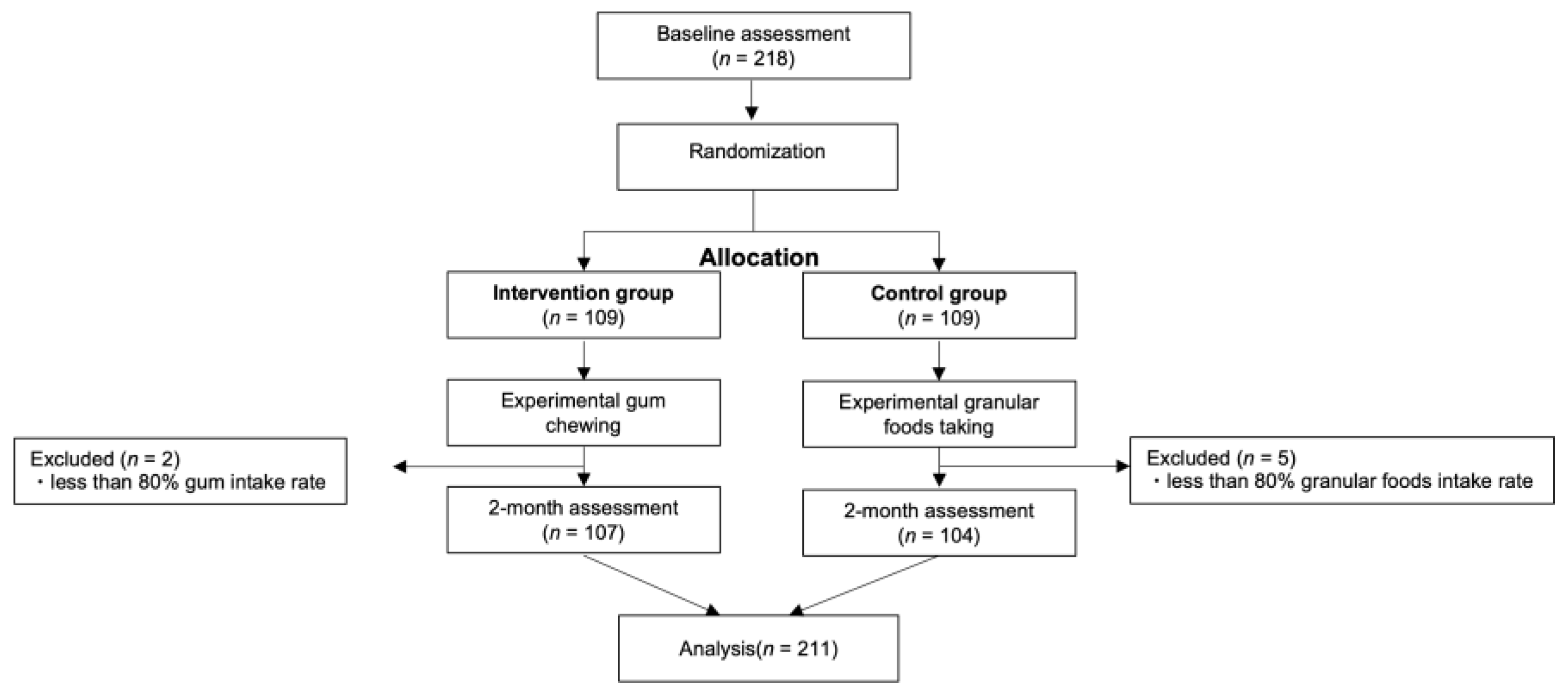
3.1. Participants
3.2. Measurement of Oral Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Minakuchi, S. Philosophy of oral hypofunction. Gerodontology 2022, 39, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K. Oral hypofunction: Management and future direction. Jpn. J. Gerodontol. 2018, 33, 304–311. [Google Scholar]
- Ohara, Y.; Yoshida, N.; Kono, Y.; Hirano, H.; Yoshida, H.; Mataki, S.; Sugimoto, K. Effectiveness of an oral health educational program on community-dwelling older people with xerostomia. Geriatr. Gerontol. Int. 2015, 15, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Matsuo, K.; Takagi, D.; Morita, Y.; Ooka, T.; Hironaka, S.; Mukai, Y. Effects of gum chewing exercises on saliva secretion and occlusal force in community-dwelling elderly individuals: A preliminary study. Geriatr. Gerontol. Int. 2017, 17, 48–53. [Google Scholar] [CrossRef]
- Kim, M.J.; Hong, J.Y.; Lee, G.; Yoon, T.; Hwang, S.H.; Kim, H.H.; Jung, Y.; Park, J.S. Effects of chewing exercises on the occlusal force and masseter muscle thickness in community-dwelling Koreans aged 65 years and older: A randomised assessor-blind trial. J. Oral Rehabil. 2020, 47, 1103–1109. [Google Scholar] [CrossRef]
- Kim, H.-J.; Lee, J.-Y.; Lee, E.-S.; Jung, H.-J.; Ahn, H.-J.; Kim, B.-I. Improvements in oral functions of elderly after simple oral exercise. Clin. Interv. Aging 2019, 14, 915–924. [Google Scholar] [CrossRef]
- Nakazawa, M.; Mori, H.; Handa, J.; Sato, T.; Kojima, T.; Ooki, S.; Hama, Y.; Tohara, H. Simple training for maintaining and improving chewing ability. Jpn. J. Gerodontol. 2018, 33, 63–69. [Google Scholar]
- Shirai, M.; Kawai, N.; Hichijo, N.; Watanabe, M.; Mori, H.; Mitsui, S.N.; Yasue, A.; Tanaka, E. Effects of gum chewing exercise on maximum bite force according to facial morphology. Clin. Exp. Dent. Res. 2018, 4, 48–51. [Google Scholar] [CrossRef]
- Takahashi, M.; Satoh, Y. Effects of gum chewing training on oral function in normal adults: Part 1 investigation of perioral muscle pressure. J. Dent. Sci. 2019, 14, 38–46. [Google Scholar] [CrossRef]
- Cho, E.-P.; Hwang, S.-J.; Clovis, J.B.; Lee, T.-Y.; Paik, D.-I.; Hwang, Y.-S. Enhancing the quality of life in elderly women through a programme to improve the condition of salivary hypofunction. Gerodontology 2012, 29, e972–e980. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, S.; Hori, K.; Shitara, S.; Okawa, J.; Kodama, S.; Murakami, K.; Ono, T. Effect of hard gummy candy chewing on masticatory function. J. Oral Rehabil. 2021, 48, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Kanno, S.; Ando, T.; Churei, H.; Matsumoto, M.; Suzuki, K.; Sasaki, R.; Yamashita, K.; Satou, H.; Ebihara, K.; Ooshima, N.; et al. Intervention effects of gum-chewing training on occlusal force and physical fitness in junior high school students. J. Sports Dent. 2020, 24, 12–17. [Google Scholar]
- Kim, H.-J.; Lee, J.-Y.; Lee, E.-S.; Jung, H.-J.; Ahn, H.-J.; Jung, H.I.; Kim, B.-I. Simple oral exercise with chewing gum for improving oral function in older adults. Aging Clin. Exp. Res. 2021, 33, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Hama, Y.; Hosoda, A.; Komagamine, Y.; Gotoh, S.; Kubota, C.; Kanazawa, M.; Minakuchi, S. Masticatory performance-related factors in preschool children: Establishing a method to assess masticatory performance in preschool children using colour-changeable chewing gum. J. Oral Rehabil. 2017, 44, 948–956. [Google Scholar] [CrossRef]
- Hirano, Y.; Onozuka, M. Chewing and attention: A positive effect on sustained attention. BioMed Res. Int. 2015, 2015, 367026. [Google Scholar] [CrossRef]
- Schimmel, M.; Christou, P.; Herrmann, F.; Müller, F. A two-colour chewing gum test for masticatory efficiency: Development of different assessment methods. J. Oral Rehabil. 2007, 34, 671–678. [Google Scholar] [CrossRef]
- Kashiwazaki, K.; Komagamine, Y.; Uehara, Y.; Yamamoto, M.; Nakai, H.; Bui, N.H.T.; Liu, H.; Namano, S.; Tonprasong, W.; Kanazawa, M.; et al. Effect of gum-chewing exercise on maintaining and improving oral function in older adults: A preliminary randomized controlled trial. J. Dent. Sci. 2023. [Google Scholar] [CrossRef]
- Iwasaki, M.; Yoshihara, A.; Sato, N.; Sato, M.; Minagawa, K.; Shimada, M.; Nishimuta, M.; Ansai, T.; Yoshitake, Y.; Ono, T.; et al. A 5-year longitudinal study of association of maximum bite force with development of frailty in community-dwelling older adults. J. Oral Rehabil. 2018, 45, 17–24. [Google Scholar] [CrossRef]
- Suzuki, T.; Kumagai, H.; Watanabe, T.; Uchida, T.; Nagao, M. Evaluation of complete denture occlusal contacts using pressure-sensitive sheets. Int. J. Prosthodont. 1997, 10, 386–391. [Google Scholar]
- Hidaka, O.; Iwasaki, M.; Saito, M.; Morimoto, T. Influence of clenching intensity on bite force balance, occlusal contact area, and average bite pressure. J. Dent. Res. 1999, 78, 1336–1344. [Google Scholar] [CrossRef] [PubMed]
- Kanehira, T.; Yamaguchi, T.; Takehara, J.; Kashiwazaki, H.; Abe, T.; Morita, M.; Asano, K.; Fujii, Y.; Sakamoto, W. A preliminary study of a simple screening technique for estimation of salivary flow. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Alves, C.; Brandão, M.; Andion, J.; Menezes, R. Use of graduated syringes for measuring salivary flow rate: A preliminary study. Braz. Dent. J. 2010, 21, 401–404. [Google Scholar] [CrossRef]
- Utanohara, Y.; Hayashi, R.; Yoshikawa, M.; Yoshida, M.; Tsuga, K.; Akagawa, Y. Standard values of maximum tongue pressure taken using newly developed disposable tongue pressure measurement device. Dysphagia 2008, 23, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Umemoto, G.; Tsuboi, Y.; Kitashima, A.; Furuya, H.; Kikuta, T. Impaired food transportation in parkinson’s disease related to lingual bradykinesia. Dysphagia 2011, 26, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Mano, T.; Katsuno, M.; Banno, H.; Suzuki, K.; Suga, N.; Hashizume, A.; Araki, A.; Watanabe, H.; Tanaka, S.; Yamamoto, M.; et al. Tongue pressure as a novel biomarker of spinal and bulbar muscular atrophy. Neurology 2014, 82, 255–262. [Google Scholar] [CrossRef]
- Adams, V.; Mathisen, B.; Baines, S.; Lazarus, C.; Callister, R. A systematic review and meta-analysis of measurements of tongue and hand strength and endurance using the Iowa oral performance instrument (IOPI). Dysphagia 2013, 28, 350–369. [Google Scholar] [CrossRef]
- Ito, K.; Yoshihara, A.; Takano, N.; Ishigami, K.; Seida, Y.; Inoue, M.; Kitahara, M.; Miyazaki, H. A comparison of methods for the measurement of oral diadochokinesis. Ronen Shika Igaku 2009, 24, 48–54. [Google Scholar]
- Hama, Y.; Kanazawa, M.; Minakuchi, S.; Uchida, T.; Sasaki, Y. Properties of a color-changeable chewing gum used to evaluate masticatory performance. J. Prosthodont. Res. 2014, 58, 102–106. [Google Scholar] [CrossRef]
- Sato, Y.; Ishida, E.; Minagi, S.; Akagawa, Y.; Tsuru, H. The aspect of dietary intake of full denture wearers. Nihon Hotetsu Shika Gakkai Zasshi 1988, 32, 774–779. [Google Scholar] [CrossRef]
- Uchida, T.; Shimoyama, K.; Nagao, M.; Odagiri, K. Questionnaire for evaluation of masticatory function complete denture wearer. Nihon Hotetsu Shika Gakkai Zasshi 1992, 36, 766–771. [Google Scholar] [CrossRef]
- Hara, K.; Namiki, C.; Yamaguchi, K.; Kobayashi, K.; Saito, T.; Nakagawa, K.; Ishii, M.; Okumura, T.; Tohara, H. Association between myotonometric measurement of masseter muscle stiffness and maximum bite force in healthy elders. J. Oral Rehabil. 2020, 47, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhao, Z.; Zhou, M.; Zheng, X.; An, N.; Niu, L.; Tay, F.R.; Ma, C.; Wang, F. In vivo evaluation of the reliability and validity of three digital occlusion analysis methods. J. Dent. 2022, 127, 104355. [Google Scholar] [CrossRef]
- Shiga, H.; Komino, M.; Uesugi, H.; Sano, M.; Yokoyama, M.; Nakajima, K.; Ishikawa, A. Comparison of two dental prescale systems used for the measurement of occlusal force. Odontology 2020, 108, 676–680. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-F.; Wang, C.-M.; Shieh, W.-Y.; Liao, Y.-F.; Hong, H.-H.; Chang, C.-T. The correlation between two occlusal analyzers for the measurement of bite force. BMC Oral Health 2022, 22, 472. [Google Scholar] [CrossRef]
- Hatch, J.P.; Shinkai, R.S.; Sakai, S.; Rugh, J.D.; Paunovich, E.D. Determinants of masticatory performance in dentate adults. Arch. Oral Biol. 2001, 46, 641–648. [Google Scholar] [CrossRef]
- Fontijn-Tekamp, F.A.; Slagter, A.P.; Van Der Bilt, A.; Van ’T Hof, M.; Witter, D.J.; Kalk, W.; Jansen, J.A. Biting and chewing in overdentures, full dentures, and natural dentitions. J. Dent. Res. 2000, 79, 1519–1524. [Google Scholar] [CrossRef]
- Julien, K.C.; Buschang, P.H.; Throckmorton, G.S.; Dechow, P.C. Normal masticatory performance in young adults and children. Arch. Oral Biol. 1996, 41, 69–75. [Google Scholar] [CrossRef]
- Lujan-Climent, M.; Martinez-Gomis, J.; Palau, S.; Ayuso-Montero, R.; Salsench, J.; Peraire, M. Influence of static and dynamic occlusal characteristics and muscle force on masticatory performance in dentate adults. Eur. J. Oral Sci. 2008, 116, 229–236. [Google Scholar] [CrossRef]
- Yoshida, E.; Fueki, K.; Igarashi, Y. Association between food mixing ability and mandibular movements during chewing of a wax cube. J. Oral Rehabil. 2007, 34, 791–799. [Google Scholar] [CrossRef]
- Wilding, R.J.; Lewin, A. The determination of optimal human jaw movements based on their association with chewing performance. Arch. Oral Biol. 1994, 39, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Ow, R.K.; Carlsson, G.E.; Karlsson, S. Relationship of masticatory mandibular movements to masticatory performance of dentate adults: A method study. J. Oral Rehabil. 1998, 25, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Wilding, R.J.; Shaikh, M. Muscle activity and jaw movements as predictors of chewing performance. J. Orofac. Pain 1997, 11, 24–36. [Google Scholar] [PubMed]
- Beecher, H.K. The powerful placebo. J. Am. Med. Assoc. 1955, 159, 1602–1606. [Google Scholar] [CrossRef] [PubMed]
- Hróbjartsson, A.; Gøtzsche, P.C. Is the Placebo Powerless? An analysis of clinical trials comparing placebo with no treatment. N. Engl. J. Med. 2001, 344, 1594–1602. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Sforza, C.; Zanotti, G.; Tartaglia, G.M. Maximal bite forces in healthy young adults as predicted by surface electromyography. J. Dent. 2004, 32, 451–457. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention (n = 107) | Control (n = 104) | p-Value | |
|---|---|---|---|
| Age, years a | 70.0 (7.0) | 69.0 (6.0) | 0.97 b |
| Sex (%) | 0.83 e | ||
| Female | 53 (49%) | 50 (48%) | |
| Male | 54 (51%) | 54 (52%) | |
| Body height, cm c | 161.3 (8.4) | 162.6 (8.4) | 0.25 d |
| Body weight, kg c | 59.5 (11.4) | 60.4 (11.7) | 0.58 d |
| Number of teeth a | 26.0 (4.0) | 26.0 (3.0) | 0.57 b |
| Number of functional teeth a | 28.0 (1.0) | 28.0 (1.0) | 0.69 b |
| Number of denture wearers | 33 (31%) | 29 (28%) | 0.64 e |
| Baseline | 2M | |||||
|---|---|---|---|---|---|---|
| Intervention (n = 107) | Control (n = 104) | p-Value | Intervention (n = 107) | Control (n = 104) | p-Value | |
| Maximum bite force (N) | 457.8 (442.1) | 512.1 (447.8) | 0.25 | 663.8 (509.1) | 507.0 (411.3) | 0.013 * |
| Occlusal contact areas (mm2) | 11.8 (13.1) | 12.8 (13.2) | 0.28 | 16.2 (14.4) | 15.0 (10.9) | 0.08 |
| Unstimulated saliva flow (g) | 1.8 (1.5) | 1.7 (1.8) | 0.53 | 1.7 (1.4) | 1.8 (1.6) | 0.06 |
| Tongue pressure (kPa) | 35.5 (11.2) | 33.7 (9.6) | 0.12 | 37.6 (12.9) | 36.2 (8.0) | 0.21 |
| Tongue and lip functions | ||||||
| /pa/ (times) | 6.2 (1.0) | 6.0 (1.0) | 0.94 | 6.2 (1.0) | 6.4 (1.0) | 0.33 |
| /ta/ (times) | 6.2 (1.0) | 6.2 (1.0) | 0.92 | 6.2 (1.0) | 6.2 (1.0) | 0.69 |
| /ka/ (times) | 5.8 (1.0) | 5.6 (1.0) | 0.42 | 5.8 (1.0) | 5.8 (1.0) | 0.96 |
| Color-changing chewing gum | ||||||
| Color scale | 9.0 (2.0) | 9.0 (2.0) | 0.33 | 10.0 (1.0) | 10.0 (1.0) | 0.63 |
| ΔE | 48.2 (5.8) | 47.0 (6.5) | 0.27 | 49.2 (6.6) | 50.4 (6.1) | 0.24 |
| Mastication score | 90.3 (14.0) | 91.5 (15.0) | 0.40 | 93.5 (14.0) | 94.8 (13.0) | 0.28 |
| Masticatory time (mins) | 4.7 (1.9) | 4.5 (1.8) | 0.30 | 4.4 (2.2) | 4.5 (2.6) | 0.30 |
| Intervention (n = 107) | Control (n = 104) | |||||
|---|---|---|---|---|---|---|
| Baseline | 2M | p-Value | Baseline | 2M | p-Value | |
| Maximum bite force (N) | 457.8 (442.1) | 663.8 (509.1) | <0.001 * | 512.1 (447.8) | 507.0 (411.3) | 0.97 |
| Occlusal contact areas (mm2) | 11.8 (13.1) | 16.2 (14.4) | <0.001 * | 12.8 (13.2) | 15.0 (10.9) | 0.10 |
| Unstimulated saliva flow (g) | 1.8 (1.5) | 1.7 (1.4) | 0.85 | 1.7 (1.8) | 1.8 (1.6) | 0.79 |
| Tongue pressure (kPa) | 35.5 (11.2) | 37.6 (12.9) | <0.001 * | 33.7 (9.6) | 36.2 (8.0) | 0.021 * |
| Tongue and lip functions | ||||||
| /pa/ (times) | 6.2 (1.0) | 6.2 (1.0) | 0.30 | 6.0 (1.0) | 6.4 (1.0) | 0.50 |
| /ta/ (times) | 6.2 (1.0) | 6.2 (1.0) | 0.88 | 6.2 (1.0) | 6.2 (1.0) | 0.92 |
| /ka/ (times) | 5.8 (1.0) | 5.8 (1.0) | 0.22 | 5.6 (1.0) | 5.8 (1.0) | 0.70 |
| Color-changing chewing gum | ||||||
| Color scale | 9.0 (1.0) | 10.0 (1.0) | <0.001 * | 9.0 (2.0) | 10.0 (1.0) | <0.001 * |
| ΔE | 48.2 (5.8) | 49.2 (6.6) | <0.001 * | 47.0 (6.5) | 50.4 (6.1) | <0.001 * |
| Mastication score | 90.3 (14.0) | 93.5 (14.0) | <0.001 * | 91.5 (15.0) | 94.8 (13.0) | <0.001 * |
| Masticatory time (mins) | 4.7 (1.9) | 4.4 (2.2) | 0.031 * | 4.5 (1.8) | 4.5 (2.6) | 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashiwazaki, K.; Komagamine, Y.; Shanglin, W.; Ren, X.; Hayashi, N.; Nakayama, M.; Namano, S.; Kanazawa, M.; Minakuchi, S. Improvements in Maximum Bite Force with Gum-Chewing Training in Older Adults: A Randomized Controlled Trial. J. Clin. Med. 2023, 12, 6534. https://doi.org/10.3390/jcm12206534
Kashiwazaki K, Komagamine Y, Shanglin W, Ren X, Hayashi N, Nakayama M, Namano S, Kanazawa M, Minakuchi S. Improvements in Maximum Bite Force with Gum-Chewing Training in Older Adults: A Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(20):6534. https://doi.org/10.3390/jcm12206534
Chicago/Turabian StyleKashiwazaki, Kenta, Yuriko Komagamine, Wu Shanglin, Xiangyu Ren, Nanaka Hayashi, Mirai Nakayama, Sahaprom Namano, Manabu Kanazawa, and Shunsuke Minakuchi. 2023. "Improvements in Maximum Bite Force with Gum-Chewing Training in Older Adults: A Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 20: 6534. https://doi.org/10.3390/jcm12206534
APA StyleKashiwazaki, K., Komagamine, Y., Shanglin, W., Ren, X., Hayashi, N., Nakayama, M., Namano, S., Kanazawa, M., & Minakuchi, S. (2023). Improvements in Maximum Bite Force with Gum-Chewing Training in Older Adults: A Randomized Controlled Trial. Journal of Clinical Medicine, 12(20), 6534. https://doi.org/10.3390/jcm12206534