


Evaluation of Tropicamide–Phenylephrine Mydriatic Eye Drop Instillation on Choroidal Thickness

 , ,
, ,  , , , and
, , , and 
Abstract
:1. Introduction
- -
- Phenylephrine [7], a selective sympathetic mimetic receptor agonist 1, available in different formulations (2.5% and 10%) as mydriatic eye drops.
- -
- Tropicamide [7], a muscarinic antagonist available in various formulations (0.5% and 1%) which is used in the ophthalmic field for cycloplegia and mydriasis.
2. Materials and Methods
2.1. Patient Selection
2.2. Clinical and Instrumental Examinations
- -
- The hole-in-the-card test: The subject holds, with two hands and extended arms, a sheet with a central hole of 3 cm in diameter. The task of the examinee is to look at a target through the hole. The eye looking at the target is the dominant one [27].
- -
- The convergence test: An object, a pen, is slowly brought close to the subject in the median plane at nose level, inviting him to fixate on it. The eye that loses fixation is the nondominant one [28]. The distance of the pen to the nose that determines the loss of fixation of the nondominant eye was variable depending on the subject.
- -
- The sighting test: The subject is asked to bring his hands together with palms outward and arms extended so that a small space remains between the thumbs and fingers. The examinee is asked to look at a target through this space. The eye visible to the examiner through the space between the fingers is the dominant eye [29].
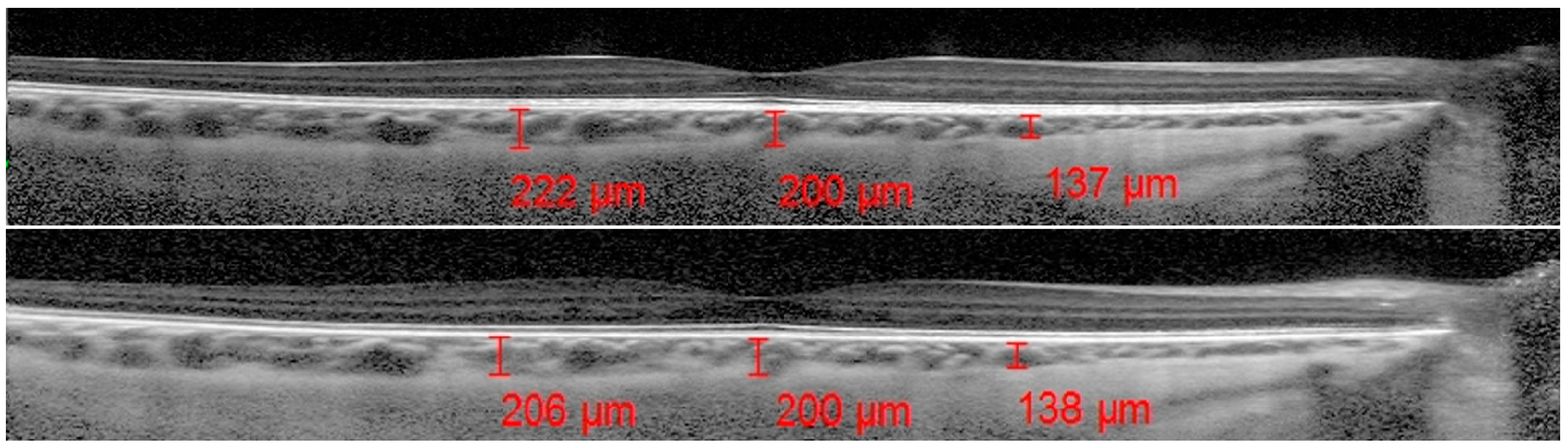
2.3. OCT Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- (1)
- The presence of the optic nerve in the nasal choroidal side could influence the ChT, causing a failed ChT reduction due to a “clutter effect”;
- (2)
- An asymmetric choroidal watershed system between the temporal choroid and other areas could cause a different response to mydriatic drops [35];
- (3)
- An asymmetrical distribution of choroidal vessels with thicker vessels on the temporal side could justify the major thinning of the temporal ChT [35].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sellheyer, K. Development of the choroid and related structures. Eye 1990, 4, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Nickla, D.L.; Wallman, J. The multifunctional choroid. Prog. Retin. Eye Res. 2010, 29, 144–168. [Google Scholar] [CrossRef] [PubMed]
- Laviers, H.; Zambarakji, H. Enhanced depth imaging-OCT of the choroid: A review of the current literature. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 1871–1883. [Google Scholar] [CrossRef]
- Reiner, A.; Fitzgerald, M.E.; Del Mar, N.; Li, C. Neural control of choroidal blood flow. Prog. Retin. Eye Res. 2018, 64, 96–130. [Google Scholar] [CrossRef]
- Booij, J.C.; Baas, D.C.; Beisekeeva, J.; Gorgels, T.G.M.F.; Bergen, A.A.B. The dynamic nature of Bruch’s membrane. Prog. Retin. Eye Res. 2010, 29, 1–18. [Google Scholar] [CrossRef]
- Lütjen-Drecoll, E. Choroidal innervation in primate eyes. Exp. Eye Res. 2006, 82, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Lodhi, S.A.K.; Ramsali, M.V.; Kulkarni, D.K.; Surender, P.; Murty, S. Safety of tropicamide and phenylephrine in pupillary mydriasis for cataract surgery. Saudi J. Ophthalmol. 2022, 35, 108–111. [Google Scholar] [CrossRef]
- Casado, A.; López-de-Eguileta, A.; Gaitán, J.; Fonseca, S.; Gordo-Vega, M.A. Peripapillary and macular choroidal thickness before and after phenylephrine instillation. Eye 2019, 33, 1741–1747. [Google Scholar] [CrossRef]
- Sander, B.P.; Collins, M.J.; Read, S.A. The effect of topical adrenergic and anticholinergic agents on the choroidal thickness of young healthy adults. Exp. Eye Res. 2014, 128, 181–189. [Google Scholar] [CrossRef]
- Kara, N.; Demircan, A.; Karatas, G.; Ozgurhan, E.B.; Tatar, G.; Karakucuk, Y.; Basci, A.; Demirok, A. Effects of two commonly used mydriatics on choroidal thickness: Direct and crossover effects. J. Ocul. Pharmacol. Ther. 2014, 30, 366–370. [Google Scholar] [CrossRef]
- Yuvac, I.; Pangal, E.; Yuvac, S.; Bayram, N.; Ataş, M.; Başkan, B.; Demircan, S.; Akal, A. An evaluation of effects of different mydriatics on choroidal thick- ness by examining anterior chamber parameters: The scheimpflug imaging and enhanced depth imaging-OCT study. J. Ophthalmol. 2015, 2015, 981274. [Google Scholar]
- Iovino, C.; Chhablani, J.; Rasheed, M.A.; Tatti, F.; Bernabei, F.; Pellegrini, M.; Giannaccare, G.; Peiretti, E. Effects of different mydriatics on the choroidal vascularity in healthy subjects. Eye 2021, 35, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kwon, H.J.; Lee, S.C. Influence of mydriatics on choroidal thickness measurement using enhanced depth imaging-OCT. Optom. Vis. Sci. 2012, 89, 1150–1155. [Google Scholar] [CrossRef] [PubMed]
- Wong, I.Y.; Koizumi, H.; Lai, W.W. Enhanced depth imaging optical coherence tomography. Ophthalmic Surg. Lasers Imaging 2011, 42, S75–S84. [Google Scholar] [CrossRef] [PubMed]
- De Bernardo, M.; Salerno, G.; Gioia, M.; Capasso, L.; Russillo, M.C.; Picillo, M.; Erro, R.; Amboni, M.; Barone, P.; Rosa, N.; et al. Intraocular pressure and choroidal thickness postural changes in multiple system atrophy and Parkinson’s disease. Sci. Rep. 2021, 11, 8936. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Xu, L.; Du, K.F.; Shao, L.; Chen, C.X.; Zhou, J.Q.; Wang, Y.X.; You, Q.S.; Jonas, J.B.; Wei, W.B. Subfoveal choroidal thickness in diabetes and diabetic retinopathy. Ophthalmology 2013, 120, 2023–2028. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, K.A.; Kazantzis, D.; Vrachatis, D.A.; Giotaki, S.G.; Papaconstantinou, E.; Kanakis, M.; Avramides, D.; Deftereos, S.; Chatziralli, I.; Georgalas, I. Choroidal thickness in patients with systemic arterial hypertension: A systematic review and meta-analysis. Ther. Adv. Ophthalmol. 2022, 14, 25158414221132825. [Google Scholar] [CrossRef]
- Yang, T.K.; Huang, X.G.; Yao, J.Y. Effects of Cigarette Smoking on Retinal and Choroidal Thickness: A Systematic Review and Meta-Analysis. J. Ophthalmol. 2019, 2019, 8079127. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, Y.L.; Li, H.Y. Subfoveal choroidal thickness and volume in severe internal carotid artery stenosis patients. Int. J. Ophthalmol. 2017, 10, 1870–1876. [Google Scholar]
- Robbins, C.B.; Thompson, A.C.; Bhullar, P.K.; Koo, H.Y.; Agrawal, R.; Soundararajan, S.; Yoon, S.P.; Polascik, B.W.; Scott, B.L.; Grewal, D.S.; et al. Characterization of Retinal Microvascular and Choroidal Structural Changes in Parkinson Disease. JAMA Ophthalmol. 2021, 139, 182–188, Erratum in: JAMA Ophthalmol. 2021, 139, 256. [Google Scholar] [CrossRef]
- Bulut, M.; Yaman, A.; Erol, M.K.; Kurtuluş, F.; Toslak, D.; Doğan, B.; Turgut Çoban, D.; Kaya Başar, E. Choroidal Thickness in Patients with Mild Cognitive Impairment and Alzheimer’s Type Dementia. J. Ophthalmol. 2016, 2016, 7291257. [Google Scholar] [CrossRef] [PubMed]
- Goktas, S.; Sakarya, Y.; Ozcimen, M.; Sakarya, R.; Bukus, A.; Ivacik, I.S.; Erdogan, E. Choroidal thinning in pseudoexfoliation syndrome detected by enhanced depth imaging optical coherence tomography. Eur. J. Ophthalmol. 2014, 24, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Dong, Y.; Zhao, K. A Meta-Analysis of Choroidal Thickness Changes in Unilateral Amblyopia. J. Ophthalmol. 2017, 2017, 2915261. [Google Scholar] [CrossRef] [PubMed]
- De Bernardo, M.; Cione, F.; Capasso, L.; Coppola, A.; Rosa, N. A formula to improve the reliability of optical axial length measurement in IOL power calculation. Sci. Rep. 2022, 12, 18845. [Google Scholar] [CrossRef]
- Fink, W.H. The dominant eye: Its clinical significance. Arch. Ophthalmol. 1938, 4, 555–582. [Google Scholar] [CrossRef]
- Miles, W.R. Ocular dominance in human adults. J. Gen. Psychol. 1930, 3, 412–430. [Google Scholar] [CrossRef]
- Suttle, C.; Alexander, J.; Liu, M.; Ng, S.; Poon, J.; Tran, T. Sensory ocular dominance based on resolution acuity, contrast sensitivity and alignment sensitivity. Clin. Exp. Optom. 2009, 92, 2–8. [Google Scholar] [CrossRef]
- Riffenburgh, R.S. Ocular dominance. Ophthalmology 1999, 106, 3. [Google Scholar] [CrossRef]
- Laby, D.M.; Kirschen, D.G. Thoughts on ocular dominance—Is it actually a preference? Eye Contact Lens 2011, 37, 140–144. [Google Scholar] [CrossRef]
- Tamaki, Y.; Araie, M.; Nagahara, M.; Tomita, K. Acute effects of cigarette smoking on tissue circulation in human optic nerve head and choroid-retina. Ophthalmology 1999, 106, 564–569. [Google Scholar] [CrossRef]
- Altinkaynak, H.; Ceylan, E.; Kartal, B.; Keleş, S.; Ekinci, M.; Olcaysu, O.O. Measurement of Choroidal Thickness Following Caffeine Intake in Healthy Subjects. Curr. Eye Res. 2016, 41, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Pan, Y.; Xu, J.; Li, X.; Spiegel, D.P.; Bao, J.; Chen, H. Effects of physical exercise on macular vessel density and choroidal thickness in children. Sci. Rep. 2021, 11, 2015. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.S.; Ouyang, Y.; Ruiz, H.; Sadda, S.R. Diurnal variation of choroidal thickness in normal, healthy subjects measured by spectral domain optical coherence tomography. Investig. Opthalmology Vis. Sci. 2012, 53, 261–266. [Google Scholar] [CrossRef]
- De Bernardo, M.; Altieri, V.; Coppola, A.; Gioia, M.; Rosa, N. Choroidal evaluation in patients under alpha-lytic therapy. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2729–2736. [Google Scholar] [CrossRef] [PubMed]
- Touhami, S.; Philippakis, E.; Mrejen, S.; Couturier, A.; Casteran, C.; Levent, P.; Tadayoni, R.; Gaudric, A. Topographic Variations of Choroidal Thickness in Healthy Eyes on Swept-Source Optical Coherence Tomography. Investig. Opthalmology Vis. Sci. 2020, 61, 38. [Google Scholar] [CrossRef]
- Rosa, N.; Cione, F.; Pepe, A.; Musto, S.; De Bernardo, M. An Advanced Lens Measurement Approach (ALMA) in post refractive surgery IOL power calculation with unknown preoperative parameters. PLoS ONE 2020, 15, e0237990. [Google Scholar] [CrossRef]
- Cione, F.; De Bernardo, M.; Gioia, M.; Oliviero, M.; Santoro, A.G.; Caputo, A.; Capasso, L.; Pagliarulo, S.; Rosa, N. A No-History Multi-Formula Approach to Improve the IOL Power Calculation after Laser Refractive Surgery: Preliminary Results. J. Clin. Med. 2023, 12, 2890. [Google Scholar] [CrossRef]
- Cione, F.; Gioia, M.; Pagliarulo, S. Bias That Should Be Avoided to Obtain a Reliable Study of IOL Power Calculation After Myopic Refractive Surgery. J. Refract. Surg. 2023, 39, 68. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preadministration (Micron) | Postadministration (Micron) | p Value | ||
|---|---|---|---|---|
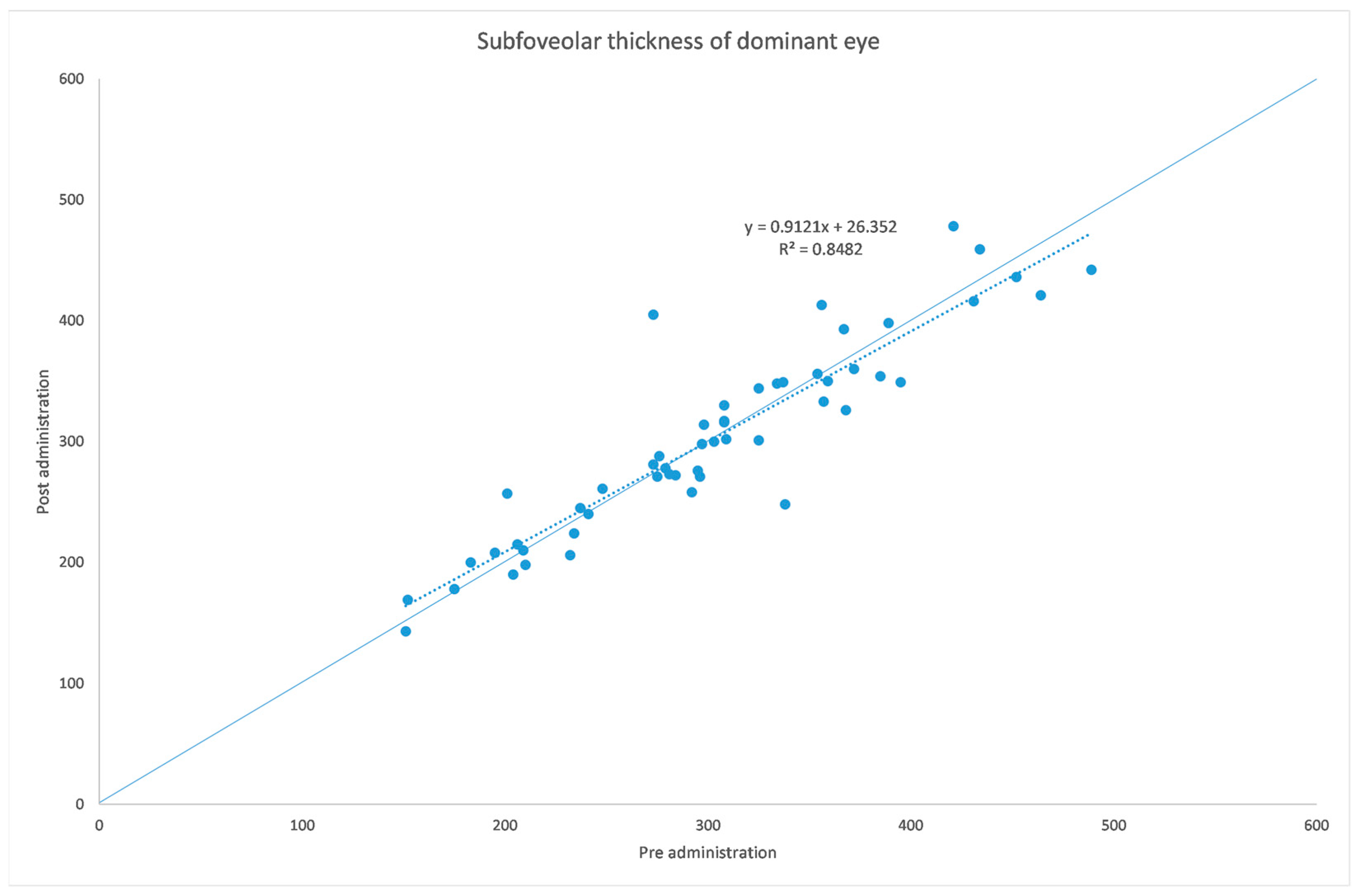
| Fovea | Mean SD Median Range | 303.49 81.24 298.00 151.00–489.00 | 303.17 80.46 300.00 143.00–478.00 | 0.94 |
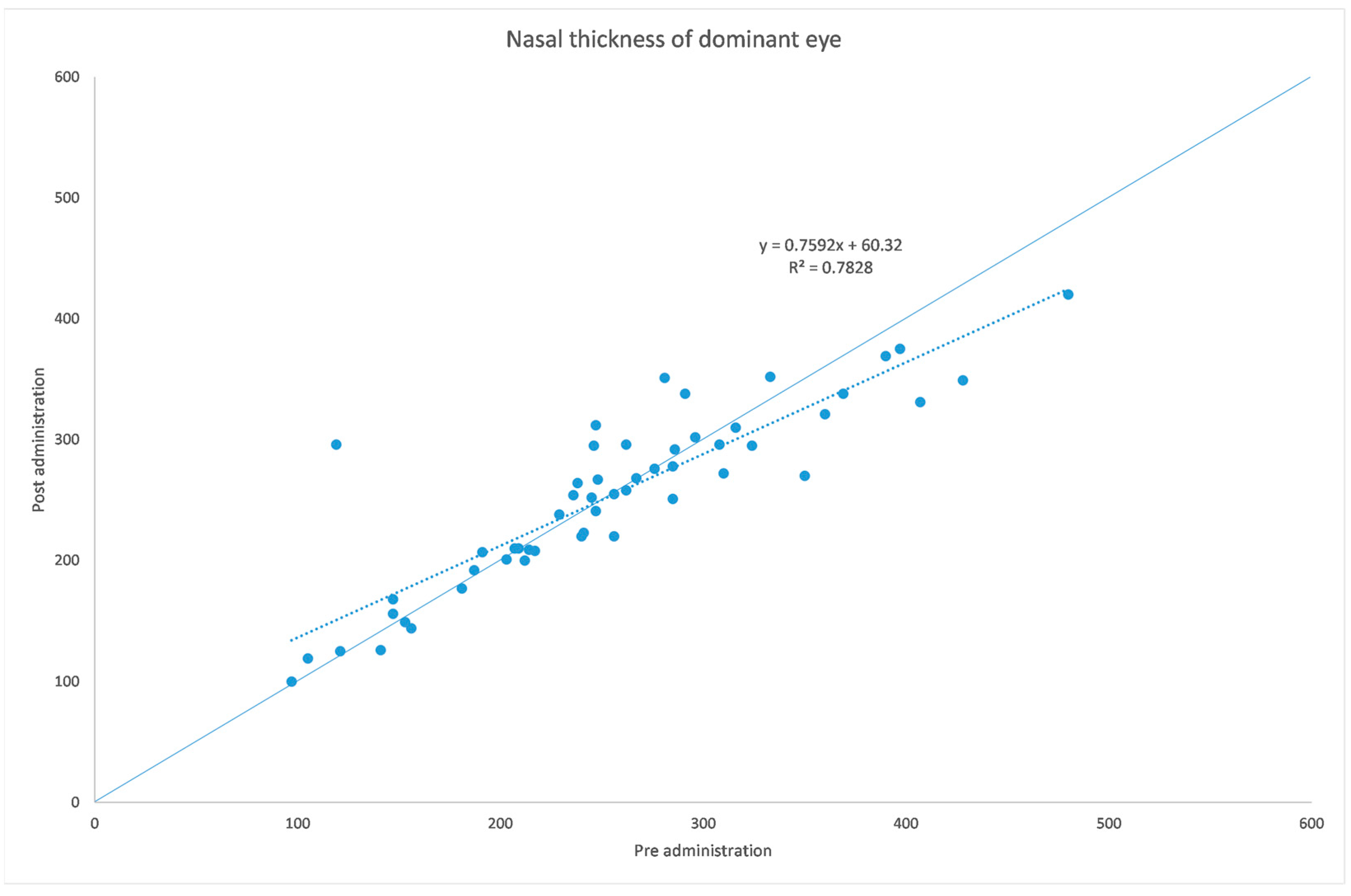
| Nasal sector | Mean SD Median Range | 254.70 84.52 247.00 97.00–480.00 | 253.70 72.53 258.00 100.00–420.00 | 0.85 |
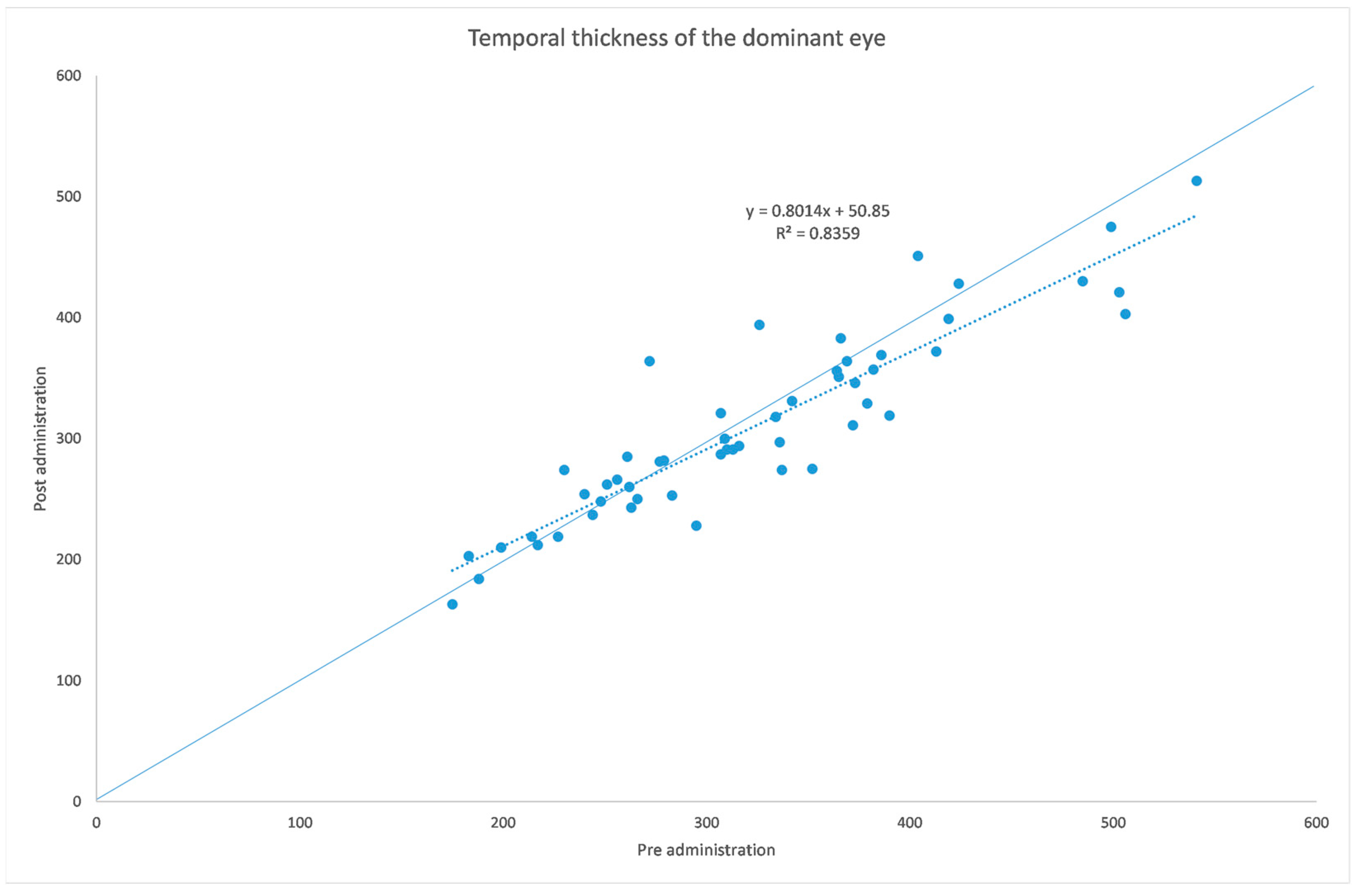
| Temporal sector | Mean SD Median Range | 323.75 88.01 313.00 175.00–541.00 | 310.32 77.15 294.00 163.00–513.00 | 0.009 |
| Preadministration (Micron) | Postadministration (Micron) | p Value | ||
|---|---|---|---|---|
| Fovea | Mean SD Median Range | 295.64 85.75 304.00 140.00–514.00 | 295.92 87.97 301.00 116.00–504.00 | 0.94 |
| Nasal sector | Mean SD Median Range | 244.28 90.24 236.00 98.00–497.00 | 239.72 86.15 241.00 98.00–479.00 | 0.41 |
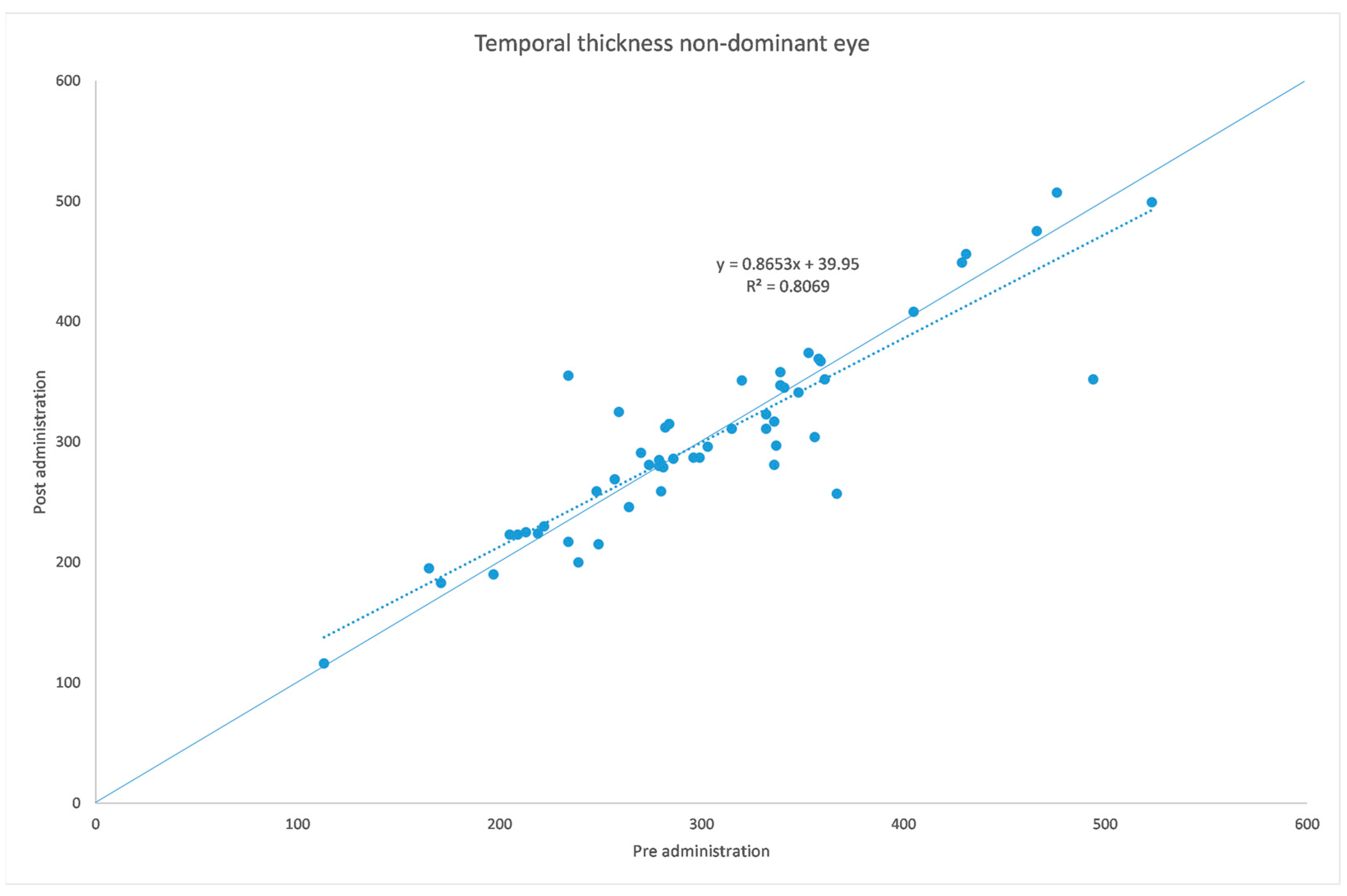
| Temporal sector | Mean SD Median Range | 304.98 84.20 296.00 113.00–523.00 | 303.85 81.11 296.00 116.00–507.00 | 0.83 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gioia, M.; De Bernardo, M.; Pagliarulo, S.; Cione, F.; Mottola, F.F.; La Marca, A.; De Pascale, I.; Albano, G.; Rosa, N. Evaluation of Tropicamide–Phenylephrine Mydriatic Eye Drop Instillation on Choroidal Thickness. J. Clin. Med. 2023, 12, 6355. https://doi.org/10.3390/jcm12196355
Gioia M, De Bernardo M, Pagliarulo S, Cione F, Mottola FF, La Marca A, De Pascale I, Albano G, Rosa N. Evaluation of Tropicamide–Phenylephrine Mydriatic Eye Drop Instillation on Choroidal Thickness. Journal of Clinical Medicine. 2023; 12(19):6355. https://doi.org/10.3390/jcm12196355
Chicago/Turabian StyleGioia, Marco, Maddalena De Bernardo, Sergio Pagliarulo, Ferdinando Cione, Francesco Ferdinando Mottola, Aniello La Marca, Ilaria De Pascale, Giovanni Albano, and Nicola Rosa. 2023. "Evaluation of Tropicamide–Phenylephrine Mydriatic Eye Drop Instillation on Choroidal Thickness" Journal of Clinical Medicine 12, no. 19: 6355. https://doi.org/10.3390/jcm12196355
APA StyleGioia, M., De Bernardo, M., Pagliarulo, S., Cione, F., Mottola, F. F., La Marca, A., De Pascale, I., Albano, G., & Rosa, N. (2023). Evaluation of Tropicamide–Phenylephrine Mydriatic Eye Drop Instillation on Choroidal Thickness. Journal of Clinical Medicine, 12(19), 6355. https://doi.org/10.3390/jcm12196355