


Relationship between Prostate Inflammation and Periodontal Disease—A Systematic Review and Meta-Analysis


 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Focused Question
2.3. Databases and Search Strategy
2.4. Study Selection
2.5. Data Extraction and Study Outcomes
2.6. Methodological Quality Assessment
2.7. Quantitative Synthesis—Meta-Analysis
3. Results
3.1. Flow Diagram
3.2. Qualitative Analysis
3.3. Quality Assessment
3.4. Quantitative Analysis
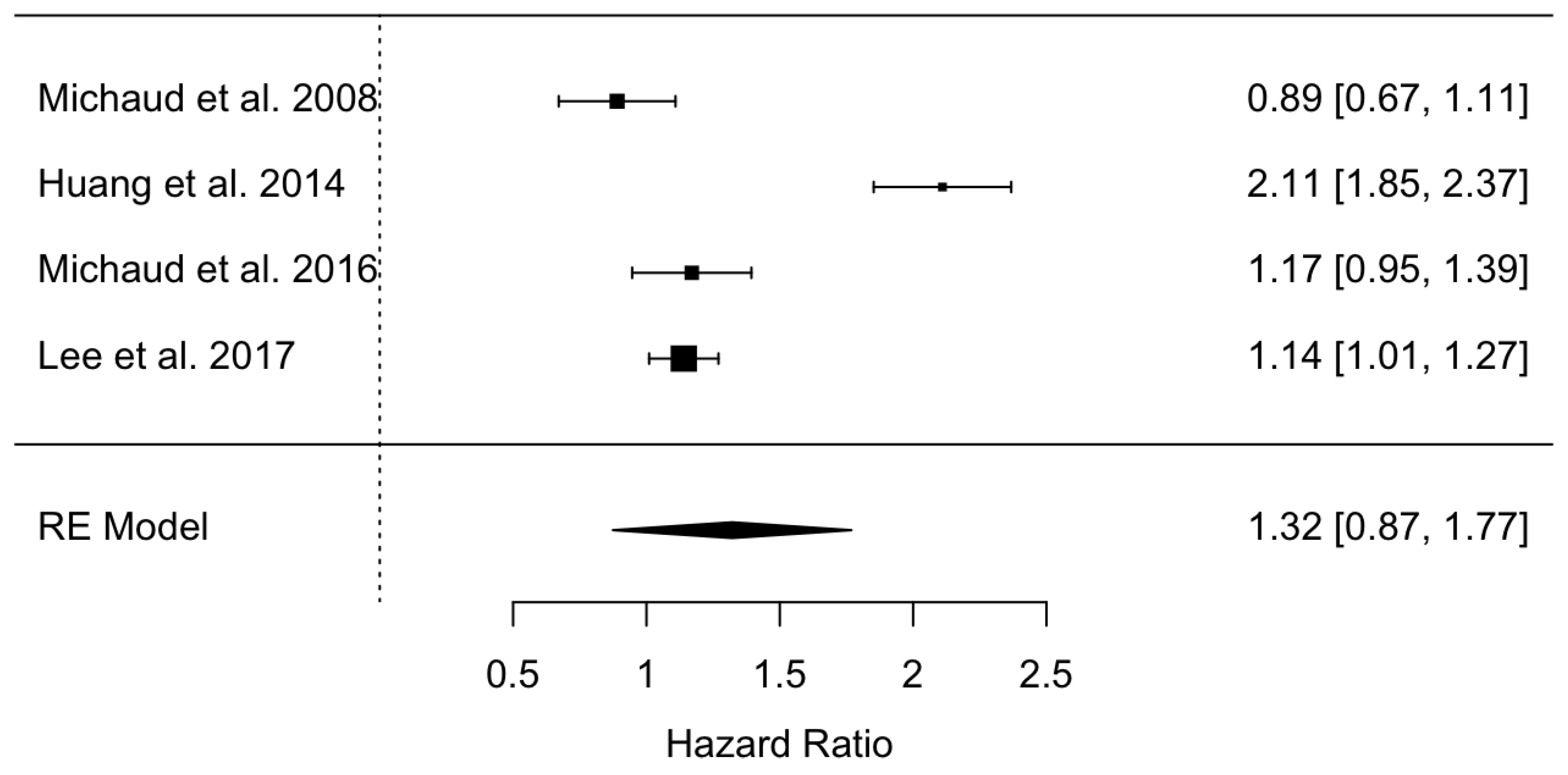
3.4.1. Hazard Ratio of Prostate Inflammation in Patients Affected by Periodontal Disease
3.4.2. Odds Ratio of Prostate Inflammation in Patients Affected by Periodontal Disease
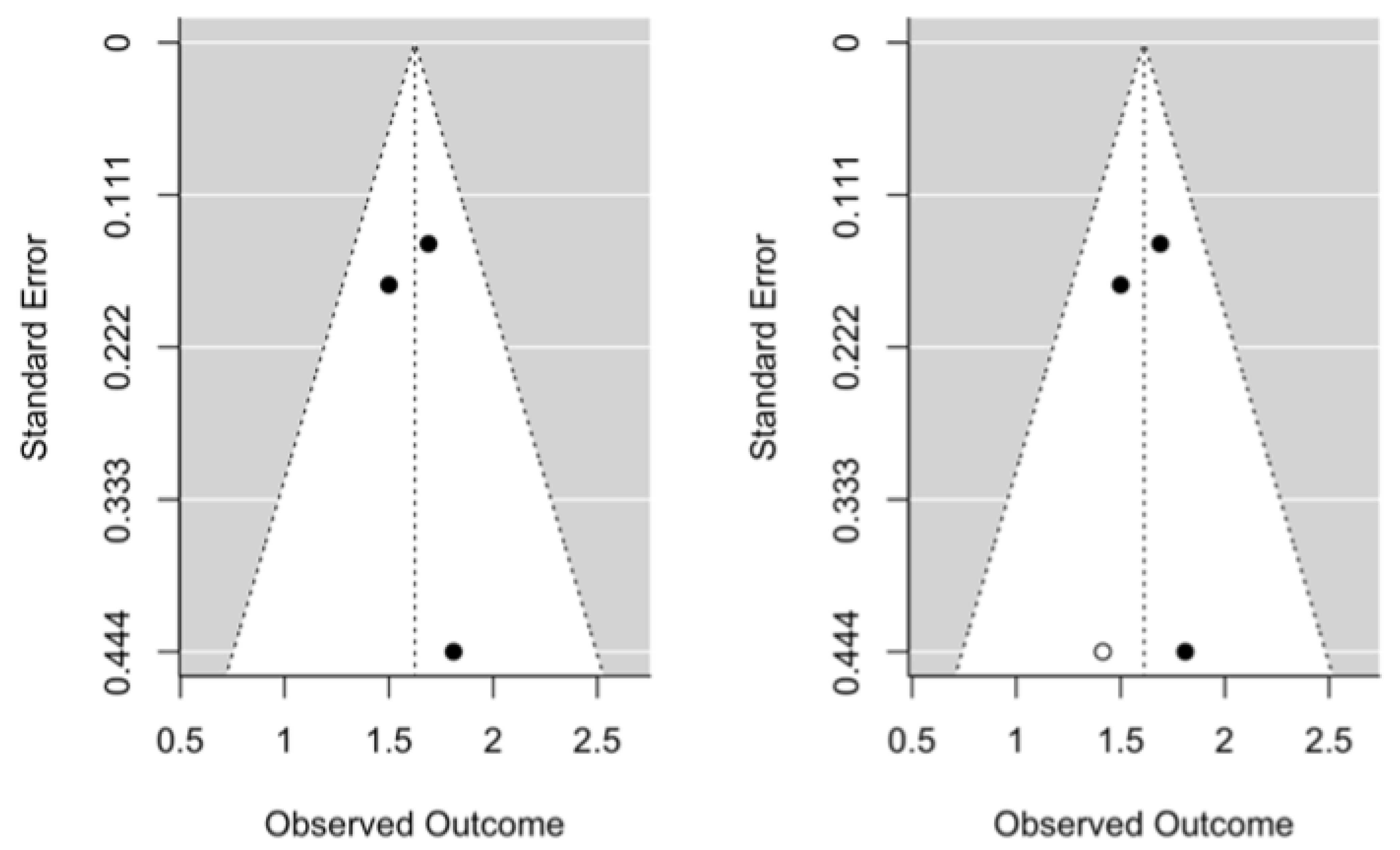
3.5. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barone, B.; Mirto, B.F.; Falcone, A.; Del Giudice, F.; Aveta, A.; Napolitano, L.; Del Biondo, D.; Ferro, M.; Busetto, G.M.; Manfredi, C.; et al. The Efficacy of Flogofilm® in the Treatment of Chronic Bacterial Prostatitis as an Adjuvant to Antibiotic Therapy: A Randomized Prospective Trial. J. Clin. Med. 2023, 12, 2784. [Google Scholar] [CrossRef]
- De Luca, L.; Crocetto, F.; Barone, B.; Creta, M.; Pesce, S.; Aveta, A.; Campanino, M.R.; Imbimbo, C.; Longo, N. Granulomatous prostatitis mimicking prostate cancer in a patient with psoriatic arthritis: A case report. Future Sci. 2020, 6, FSO591. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Karim-Kos, H.E.; Coebergh, J.W.; Byrnes, G.; Antilla, A.; Ferlay, J.; Renehan, A.G.; Forman, D.; Soerjomataram, I. Recent trends in incidence of five common cancers in 26 European countries since 1988: Analysis of the European Cancer Observatory. Eur J Cancer. 2015, 51, 1164–1187. [Google Scholar] [CrossRef] [PubMed]
- Flores-Fraile, M.C.; Padilla-Fernández, B.Y.; Valverde-Martínez, S.; Marquez-Sanchez, M.; García-Cenador, M.B.; Lorenzo-Gómez, M.F.; Flores-Fraile, J. The Association between Prostate-Specific Antigen Velocity (PSAV), Value and Acceleration, and of the Free PSA/Total PSA Index or Ratio, with Prostate Conditions. J. Clin. Med. 2020, 9, 3400. [Google Scholar] [CrossRef]
- Polackwich, A.S.; Shoskes, D.A. Chronic prostatitis/chronic pelvic pain syndrome: A review of evaluation and therapy. Prostate Cancer Prostatic Dis. 2016, 19, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Kolenbrander, P.E.; Palmer, R.J., Jr.; Rickard, A.H.; Jakubovics, N.S.; Chalmers, N.I.; Díaz, P.I. Bacterial interactions and successions during plaque development. Periodontol. 2000 2006, 42, 47–79. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D. Controlling the oral biofilm with antimicrobials. J. Dent. 2010, 38 (Suppl. 1), S11–S15. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D. Evidence of bacterial etiology: A historical perspective. Periodontol. 2000 1994, 5, 7–25. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Socransky, S.S. Introduction to microbial aspects of periodontal biofilm communities. development and treatment. Periodontol. 2000 2006, 42, 7–12. [Google Scholar] [CrossRef]
- Paster, B.J.; Olsen, I.; Aas, J.A.; Dewhirst, F.E. The breadth of bacterial diversity in the human periodontal pocket and other oral sites. Periodontol. 2000 2006, 42, 80–87. [Google Scholar] [CrossRef]
- Albandar, J.M.; Rams, T.E. Global epidemiology of periodontal diseases: An overview. Periodontol. 2000 2002, 29, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Quirynen, M.; Teughels, W.; De Soete, M.; van Steenberghe, D. Topical antiseptics and antibiotics in the initial therapy of chronic adult periodontitis: Microbiological aspects. Periodontol. 2000 2002, 28, 72–90. [Google Scholar] [CrossRef] [PubMed]
- Socransky, S.S.; Haffajee, A.D. The bacterial etiology of destructive periodontal disease: Current concepts. J. Periodontol. 1992, 63 (Suppl. 4), 322–331. [Google Scholar] [CrossRef] [PubMed]
- Bascones, A.; Morante, S.; Mateos, L.; Mata, M.; Poblet, J. Influence of additional active ingredients on the effectiveness of non-alcoholic chlorhexidine mouth washes: A randomized controlled trial. J. Periodontol. 2005, 76, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Corbet, E.F.; Davies, W.I. The role of supragingival plaque in the control of progressive periodontal disease. A review. J. Clin. Periodontol. 1993, 20, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Matsuda, M.; Takekawa, M.; Okada, M.; Hashizume, K.; Wada, N.; Hori, J.; Kita, M.; Iwata, T.; Kakizaki, H. Association between Chronic Periodontal Disease and Lower Urinary Tract Symptoms in Both Sexes. Low. Urin. Tract Symptoms 2015, 7, 17–21. [Google Scholar] [CrossRef]
- Estemalik, J.; Demko, C.; Bissada, N.F.; Joshi, N.; Bodner, D.; Shankar, E.; Gupta, S. Simultaneous Detection of Oral Pathogens in Subgingival Plaque and Prostatic Fluid of Men with Periodontal and Prostatic Diseases. J. Periodontol. 2017, 88, 823–829. [Google Scholar] [CrossRef]
- Davies, R.M. Toothpaste in the control of plaque/gingivitis and periodontitis. Periodontol. 2000 2008, 48, 23–30. [Google Scholar] [CrossRef]
- Liberati, A.; Banzi, R.; Moja, L. Measuring the impact of evidence: The Cochrane systematic review of organized stroke care. Intern. Emerg. Med. 2009, 4, 507–510. [Google Scholar]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef]
- Michaud, D.S.; Liu, Y.; Meyer, M.; Giovannucci, E.; Joshipura, K. Periodontal disease, tooth loss, and cancer risk in male health professionals: A prospective cohort study. Lancet Oncol. 2008, 9, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Kelsey, K.T.; Papathanasiou, E.; Genco, C.A.; Giovannucci, E. Periodontal disease and risk of all cancers among male never smokers: An updated analysis of the Health Professionals Follow-up Study. Ann. Oncol. 2016, 27, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Michaud, D.S.; Lu, J.; Carter, H.B.; Platz, E.A. The association between clinically determined periodontal disease and prostate-specific antigen concentration in men without prostate cancer: The 2009–2010 National Health and Nutrition Examination Survey. Cancer Causes Control 2019, 30, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kweon, H.H.; Choi, J.K.; Kim, Y.T.; Choi, S.H. Association between Periodontal disease and Prostate cancer: Results of a 12-year Longitudinal Cohort Study in South Korea. J. Cancer 2017, 8, 2959–2965. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Li, B.H.; Wang, Y.Y.; Wang, C.Y.; Zi, H.; Weng, H.; Huang, Q.; Zhu, Y.J.; Zeng, X.T. Periodontal disease and risk of benign prostate hyperplasia: A cross-sectional study. Mil. Med. Res. 2019, 6, 34. [Google Scholar] [CrossRef] [PubMed]
- Boland, M.R.; Hripcsak, G.; Albers, D.J.; Wei, Y.; Wilcox, A.B.; Wei, J.; Li, J.; Lin, S.; Breene, M.; Myers, R.; et al. Discovering medical conditions associated with periodontitis using linked electronic health records. J. Clin. Periodontol. 2013, 40, 474–482. [Google Scholar] [CrossRef]
- Hujoel, P.P.; Drangsholt, M.; Spiekerman, C.; Weiss, N.S. An exploration of the periodontitis-cancer association. Ann. Epidemiol. 2003, 13, 312–316. [Google Scholar] [CrossRef]
- Boyapati, R.; Swarna, C.; Devulapalli, N.; Sanivarapu, S.; Katuri, K.K.; Kolaparthy, L. Unveiling the Link between Prostatitis and Periodontitis. Contemp. Clin. Dent. 2018, 9, 524–529. [Google Scholar] [CrossRef]
- Muhsin, J.M.; Al-Sayyid, M.M. The possible Connection of periodontal diseases (PD) with cardiovascular disease (CVD) and prostatitis in sample of Iraqi patients. Muthanna Med. J. 2019, 6, 1–12. [Google Scholar] [CrossRef]
- da Silva, A.P.B.; Alluri, L.S.C.; Bissada, N.F.; Gupta, S. Association between oral pathogens and prostate cancer: Building the relationship. Am. J. Clin. Exp. Urol. 2019, 7, 1–10. [Google Scholar]
- Joshi, N.; Bissada, N.F.; Bodner, D.; Maclennan, G.T.; Narendran, S.; Jurevic, R.; Skillicorn, R. Association between periodontal disease and prostate-specific antigen levels in chronic prostatitis patients. J. Periodontol. 2010, 81, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Coker, T.J.; Dierfeldt, D.M. Acute Bacterial Prostatitis: Diagnosis and Management. Am. Fam. Physician. 2016, 93, 114–120. [Google Scholar] [PubMed]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef]
- Kulhánová, I.; Bray, F.; Fadhil, I.; Al-Zahrani, A.S.; El-Basmy, A.; Anwar, W.A.; Al-Omari, A.; Shamseddine, A.; Znaor, A.; Soerjomataram, I. Profile of cancer in the Eastern Mediterranean region: The need for action. Cancer Epidemiol. 2017, 47, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Han, G.; Chen, J.; Yi, S.; Feng, X. Effect of periodontitis on rats with chronic bacterial prostatitis. Anticancer. Res. 2015, 11, 22–30. [Google Scholar]
- Endo, M.; Yoshida, F.; Mori, M.; Nakano, M.; Morimura, T.; Ohno, Y.; Komura, M. Role of Helicobacter pylori in causing repeated Reinfection from Oral cavity in Chronic Prostatitis. Arch. Surg. Clin. Res. 2018, 2, 5–12. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. EFP Workshop Participants and Methodological Consultants. Treatment of stage I–III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 4–60, Erratum in J. Clin. Periodontol. 2021, 48, 163. [Google Scholar] [CrossRef]
- Kruck, S.; Hennenlotter, J.; Amend, B.; Geiger, M.; Filipova, E.; Neumann, T.; Stühler, V.; Schubert, T.; Todenhöfer, T.; Rausch, S.; et al. Chronic Periodontitis Does Not Impact Serum Levels of Prostate-specific Antigen. Anticancer. Res. 2017, 37, 3163–3167. [Google Scholar] [CrossRef]
- Alwithanani, N.; Bissada, N.F.; Joshi, N.; Bodner, D.; Demko, C.; MacLennan, G.T.; Skillicorn, R.; Ponsky, L.; Gupta, S. Periodontal Treatment Improves Prostate Symptoms and Lowers Serum PSA in Men with High PSA and Chronic Periodontitis. Dentistry 2015, 5, 284–288. [Google Scholar] [CrossRef]
- Fang, C.; Wu, L.; Zhao, M.J.; Deng, T.; Gu, J.M.; Guo, X.P.; Li, C.; Li, W.; Zeng, X.T. Periodontitis Exacerbates Benign Prostatic Hyperplasia through Regulation of Oxidative Stress and Inflammation. Oxid. Med. Cell. Longev. 2021, 2021, 2094665. [Google Scholar] [CrossRef]
- Fu, E.; Cheng, C.M.; Chung, C.H.; Lee, W.C.; Chen, W.L.; Sun, G.H.; Chien, W.C. Association of chronic periodontitis with prostatic hyperplasia and prostatitis: A population-based cohort study in Taiwan. J. Periodontol. 2021, 92, 72–86. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Study Design | N_Control Group | HN_Control Group | IC_Control Group |
|---|---|---|---|---|
| Michaud et al., 2008 [21] | Cohort | 48,275 | 0.89 | 0.71–1.10 |
| Huang et al., 2019 [23] | Cohort | 38,092 | 2.11 | 1.63–2.73 |
| Michaud et al., 2016 [22] | Cohort | 19,933 | 1.17 | 0.94–1.47 |
| Lee et al., 2017 [24] | Cohort | 1235 | 1.5 | 1.05–2.10 |
| Wu et al., 2019 [25] | Case-control | 2171 | 1.81 | 0.76–4.34 |
| Hujoel et al., 2003 [27] | Case-control | 5240 | 0.49 | 0.19–1.26 |
| Boland et al., 2013 [26] | Case-control | 1240 | 1.5 | 1.05–2.10 |
| Author/Year | Selection | Comparability | Outcome | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Representative of the Exposed Cohort | Selection of External Control | Ascertainment of Exposure | Outcome of Interest Not Present at the Start of the Study | Main Factor | Additional Factor | Assessment of Outcomes | Sufficient Follow-Up Time | Adequacy of Follow-Up | Total | |
| Michaud et al., 2008 [21] | * | * | * | * | * | * | 6/9 | |||
| Huang et al., 2019 [23] | * | * | * | * | * | * | * | * | 8/9 | |
| Michaud et al., 2016 [22] | * | * | * | * | * | * | 6/9 | |||
| Lee et al., 2017 [24] | * | * | * | * | * | * | 6/9 | |||
| Author/Year | Selection | Comparability | Outcome | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Representative of the Exposed Cohort | Selection of External Control | Ascertainment of Exposure | Outcome of Interest Not Present at the Start of the Study | Main Factor | Additional Factor | Assessment of Outcomes | Sufficient Follow-Up Time | Adequacy of Follow-Up | Total | |
| Boland et al., 2013 [26] | * | * | * | * | * | * | 6/9 | |||
| Wu et al., 2019 [25] | * | * | * | * | * | * | 6/9 | |||
| Hujoel et al., 2003 [27] | * | * | * | * | * | * | 6/9 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortíz de Urbina Comerón, P.; Zubizarreta-Macho, Á.; Lobo Galindo, A.B.; Montiel-Company, J.M.; Lorenzo-Gómez, M.-F.; Flores Fraile, J. Relationship between Prostate Inflammation and Periodontal Disease—A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 6070. https://doi.org/10.3390/jcm12186070
Ortíz de Urbina Comerón P, Zubizarreta-Macho Á, Lobo Galindo AB, Montiel-Company JM, Lorenzo-Gómez M-F, Flores Fraile J. Relationship between Prostate Inflammation and Periodontal Disease—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(18):6070. https://doi.org/10.3390/jcm12186070
Chicago/Turabian StyleOrtíz de Urbina Comerón, Pablo, Álvaro Zubizarreta-Macho, Ana Belén Lobo Galindo, José María Montiel-Company, María-Fernanda Lorenzo-Gómez, and Javier Flores Fraile. 2023. "Relationship between Prostate Inflammation and Periodontal Disease—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 18: 6070. https://doi.org/10.3390/jcm12186070
APA StyleOrtíz de Urbina Comerón, P., Zubizarreta-Macho, Á., Lobo Galindo, A. B., Montiel-Company, J. M., Lorenzo-Gómez, M.-F., & Flores Fraile, J. (2023). Relationship between Prostate Inflammation and Periodontal Disease—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(18), 6070. https://doi.org/10.3390/jcm12186070