
Machine Learning-Based Early Prediction of Sepsis Using Electronic Health Records: A Systematic Review
 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Background and Fundamental Concepts
2.1. Sepsis Definition
- By incorporating organ dysfunction criteria, the Sepsis-3 definition improves the specificity of sepsis diagnosis. This helps differentiate sepsis from other conditions that may present with signs of infection but do not involve organ dysfunction.
- The Sepsis-3 definition simplifies the criteria for sepsis by focusing on organ dysfunction rather than the systemic inflammatory response syndrome (SIRS) criteria used in previous definitions. This simplification reduces the potential for misdiagnosis and facilitates a more targeted approach to sepsis identification.
- The early prediction of sepsis is crucial for timely intervention. The SOFA score, which is part of the Sepsis-3 definition, provides a tool for assessing organ dysfunction and predicting patient outcomes. Higher SOFA scores are associated with increased mortality rates and can help identify patients at higher risk who require immediate attention.
- The Sepsis-3 definition has facilitated the standardization of sepsis diagnosis and research. The use of a consistent definition enables better comparison of studies, data sharing, and the development of evidence-based management strategies.
2.2. Common Machine Learning Models and Performance Metrics
- Classical ML Models:
- Decision Trees (DT)
- Random Forest (RF)
- Support Vector Machine (SVM)
- Logistic Regression (LR)
- Gradient Boosting (GB)
- Naïve Bayes (NB)
- k-Nearest Neighbor (kNN)
- Deep Learning Models:
- Long Short-Term Memory (LSTM) Networks
- Convolutional Neural Network (CNN)
- Gated Recurrent Unit (GRU)
- Neural Network (NN)
- Multitask Gaussian Process and Attention-based Deep Learning Model (MGP-AttTCN)
- Temporal Convolutional Network (TCN)
- Recurrent Neural Network (RNN)
- CNN-LSTM
- CNN-GRU
- Performance Metrics:
- Area Under the Curve (AUC) or AUROC (Receiver Operating Characteristics Curve)
- Sensitivity (Recall)
- Specificity
- Accuracy
- Precision
- F1 score
- Matthews Correlation Coefficient (MCC)
- Mean Average Precision (mAP)
- Positive Predictive Value (PPV)
- Negative Predictive Value (NPV)
- Positive Likelihood Ratio (PLR)
- Negative Likelihood Ratio (NLR)
3. Materials and Methods
3.1. Search Strategy
3.2. Inclusion and Exclusion Criteria
3.2.1. Inclusion Criteria
- Studies that focused on the application of machine learning and deep learning algorithms for the early prediction of sepsis.
- Studies utilizing electronic health records (EHR) data as the primary sources of information.
- Studies that involved adult human subjects (i.e., age ≥ 18).
- Studies that reported on the performance metrics (e.g., sensitivity, specificity, area under the curve) of the machine learning models for sepsis prediction.
- Studies published in peer-reviewed journals.
- Studies available in the English language.
- Studies published within a specific time frame (e.g., Jun 2016 and March 2023).
3.2.2. Exclusion Criteria
- Studies that did not focus on early prediction of sepsis.
- Studies that focused only on using clinical notes.
- Studies that did not involve the use of machine learning/deep learning algorithms.
- Studies that did not utilize electronic health records as data sources.
- Studies that primarily focused on non-human subjects or experimental setups not related to human healthcare.
- Studies that did not report on performance metrics for machine learning models.
- Studies that were not published in peer-reviewed journals.
- Studies published in languages other than English.
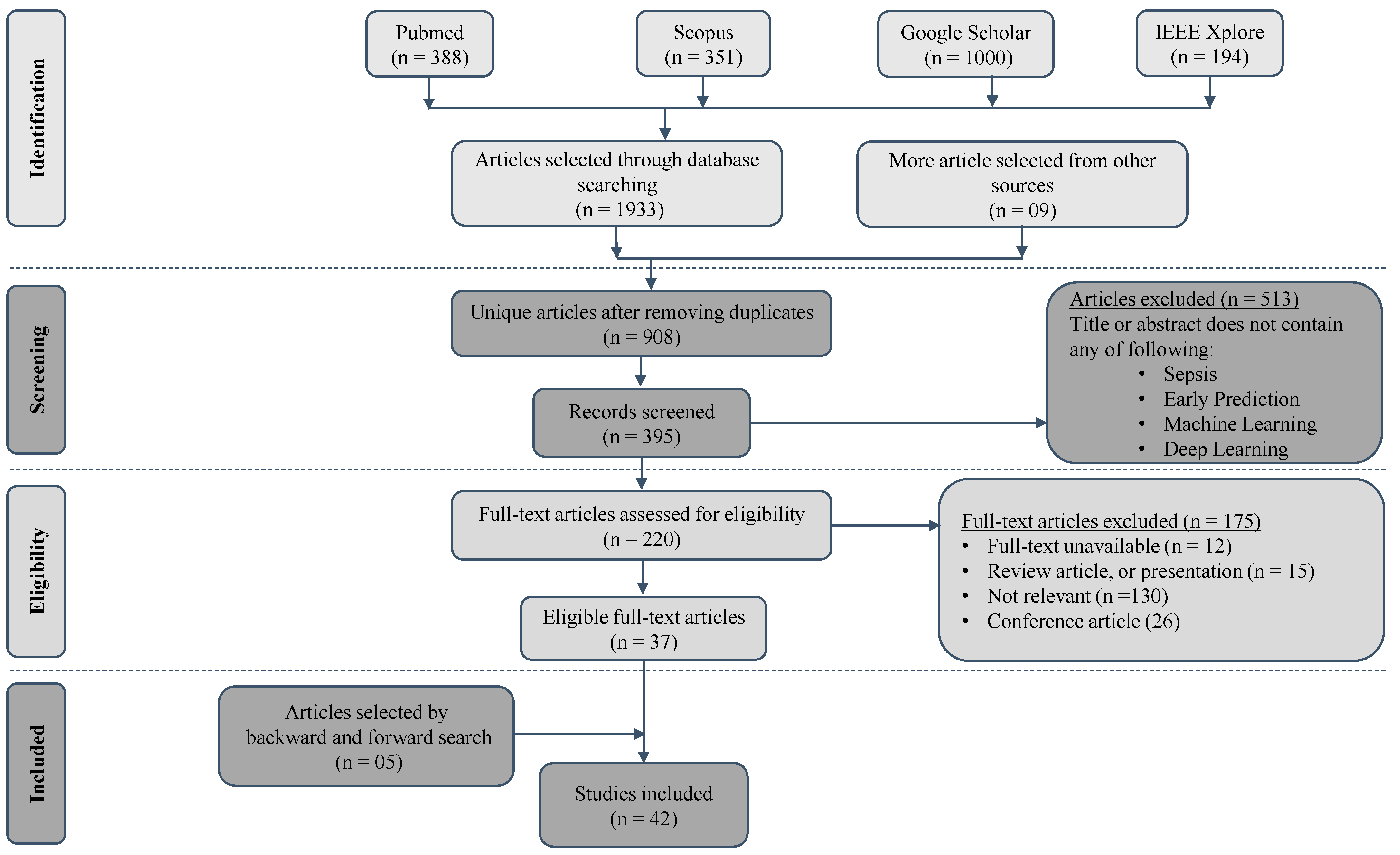
3.3. Study Selection
3.4. Data Extraction
3.5. Quality Assessment
3.6. Impact of Funding Source
4. Results
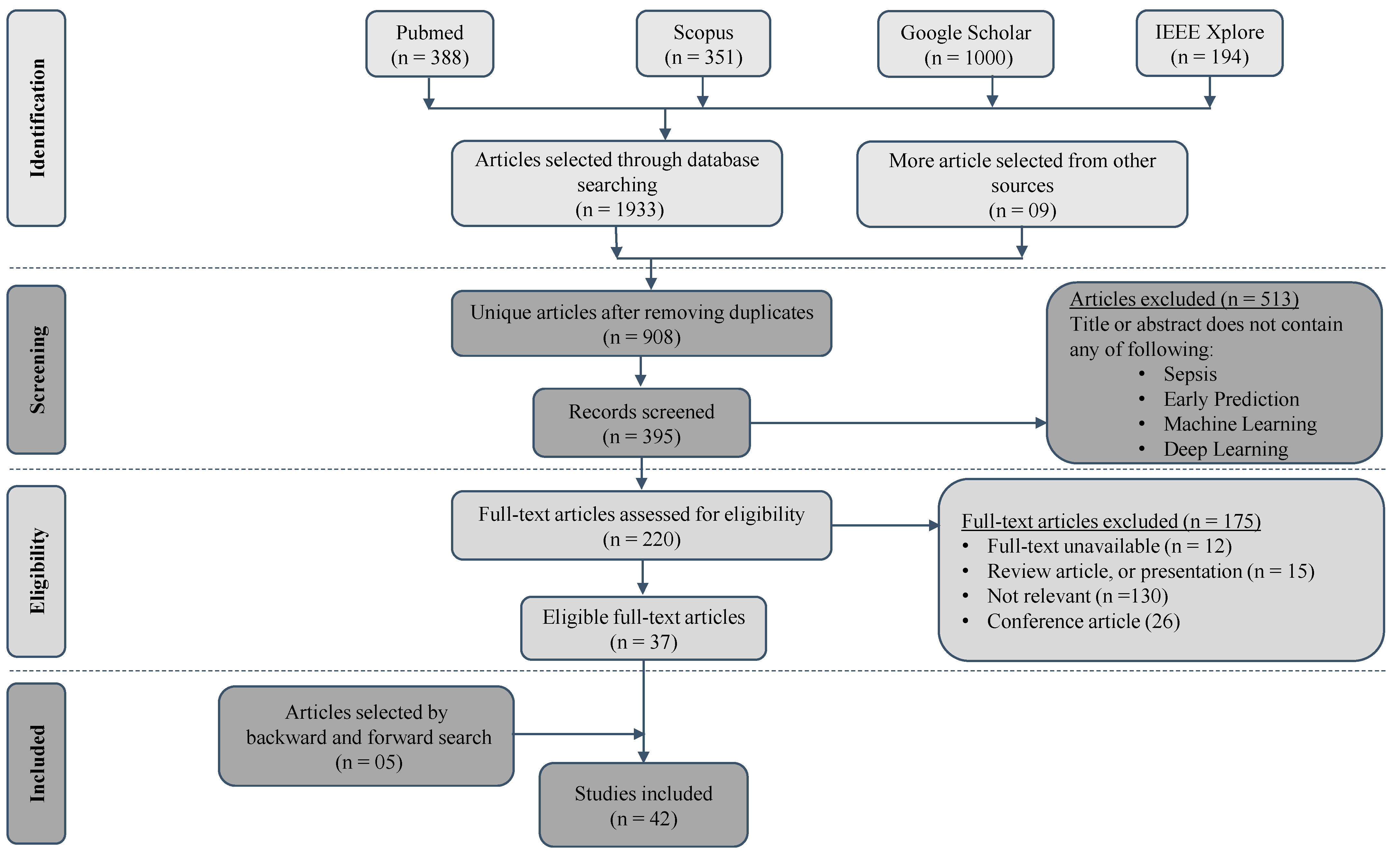
4.1. Selection Process
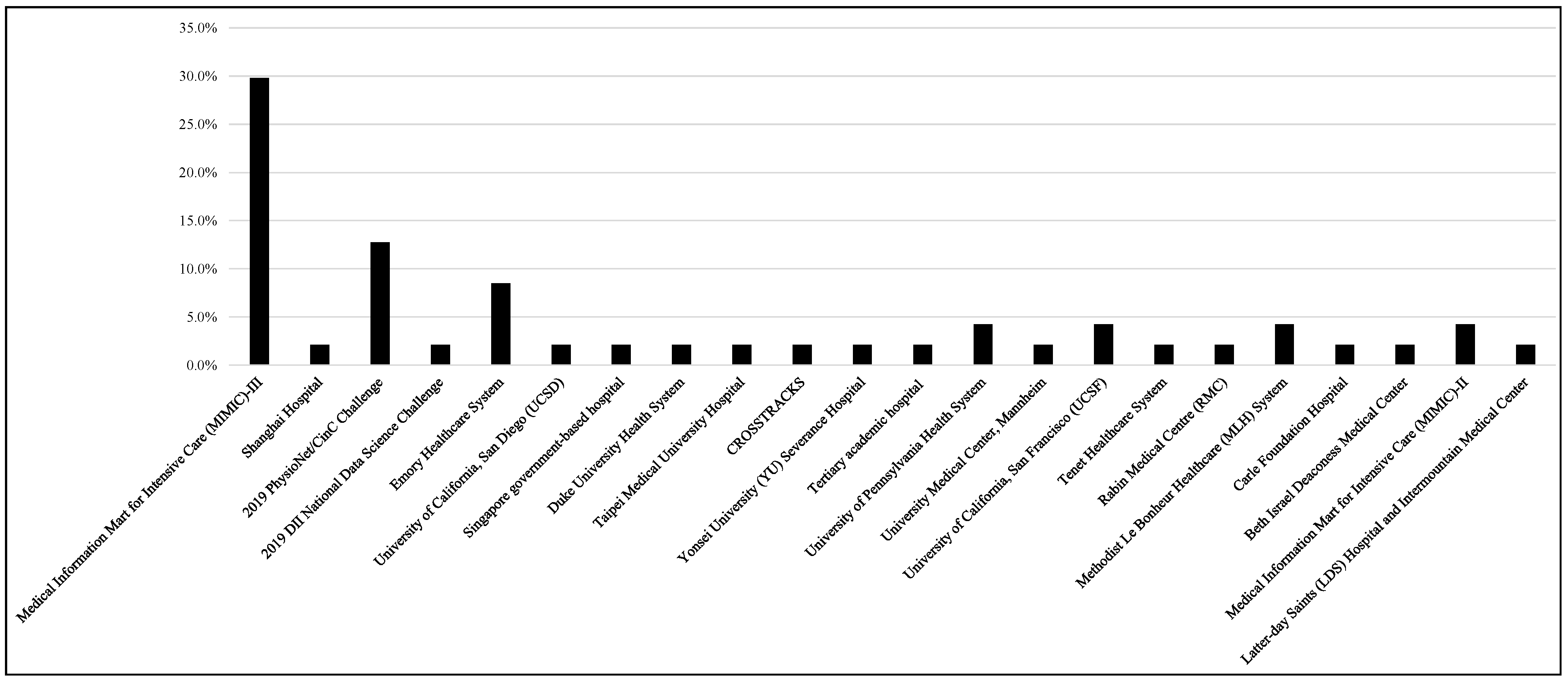
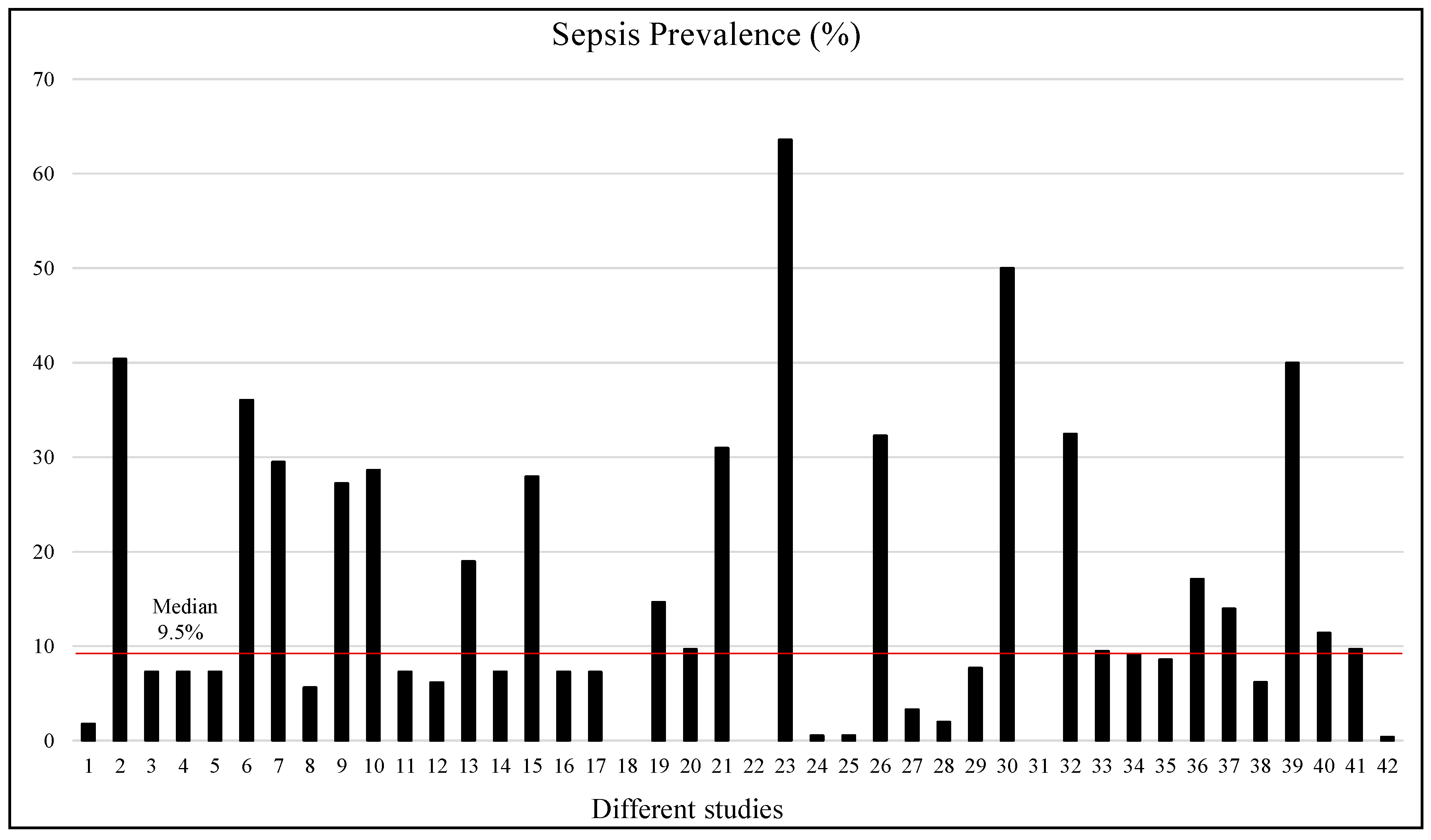
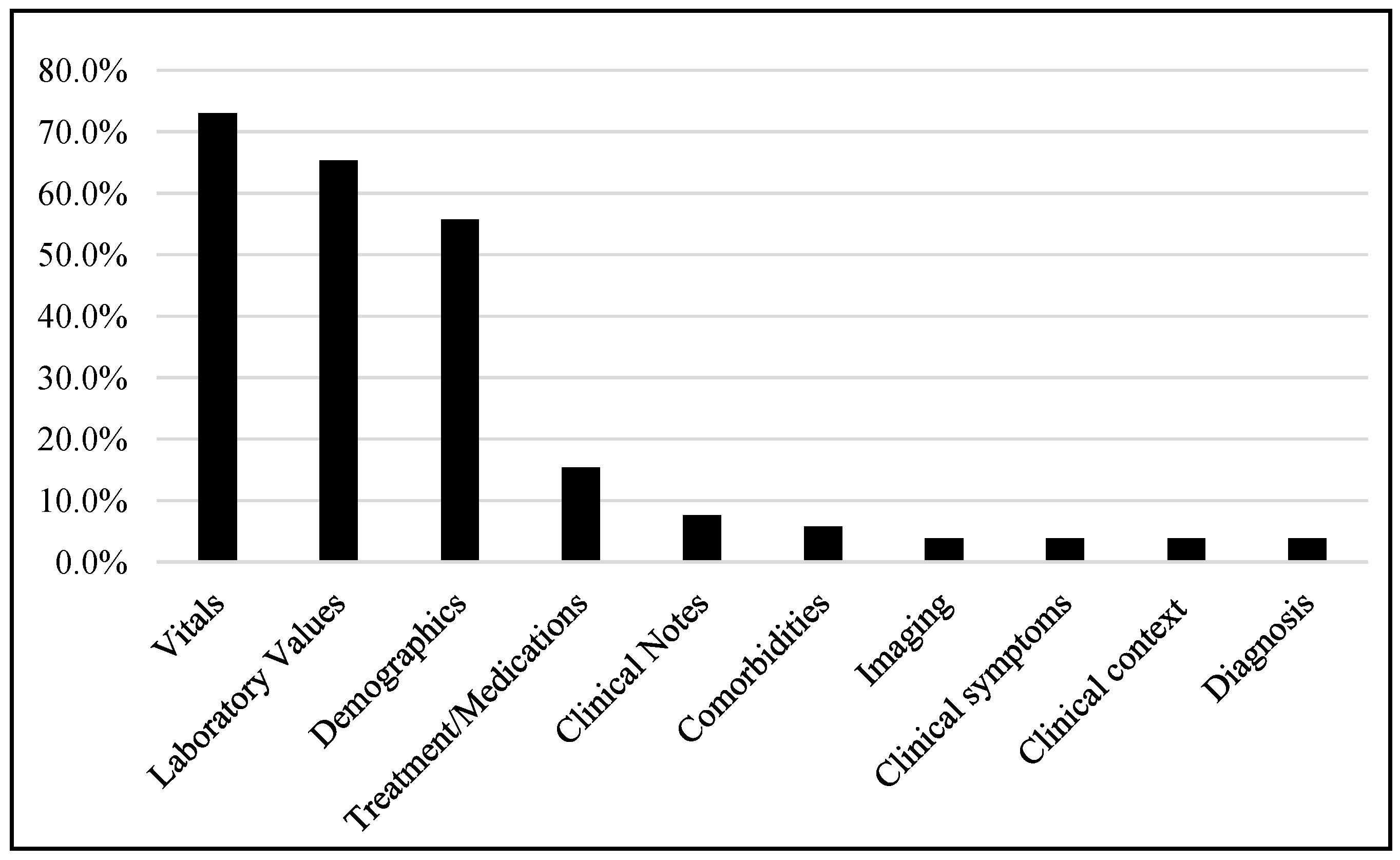
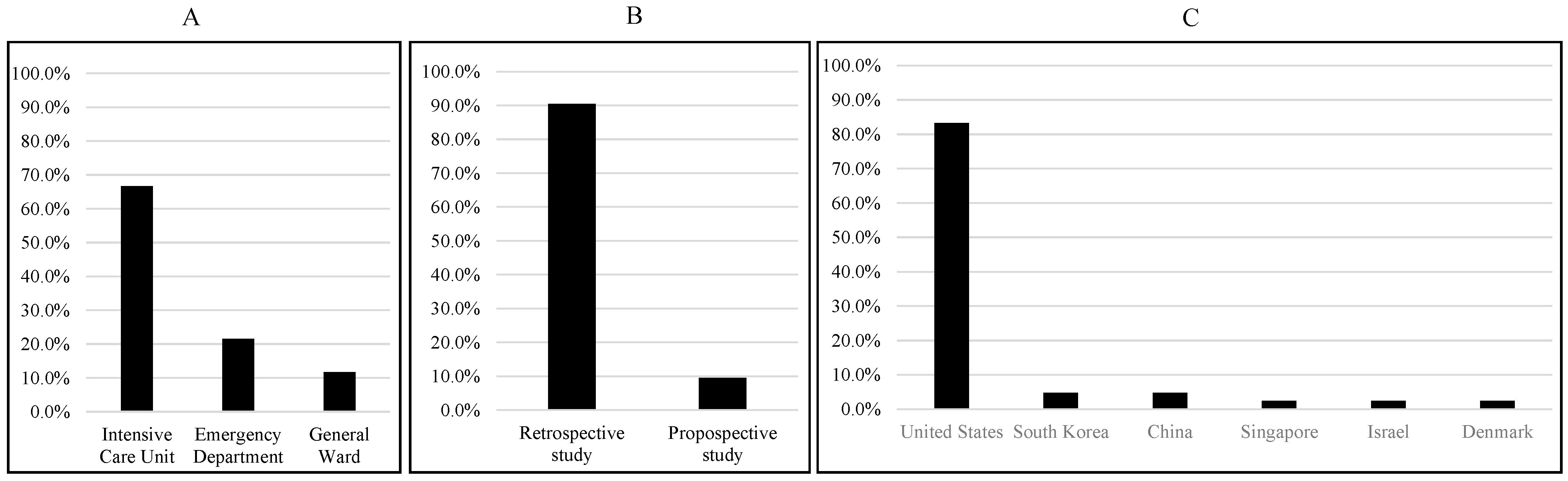
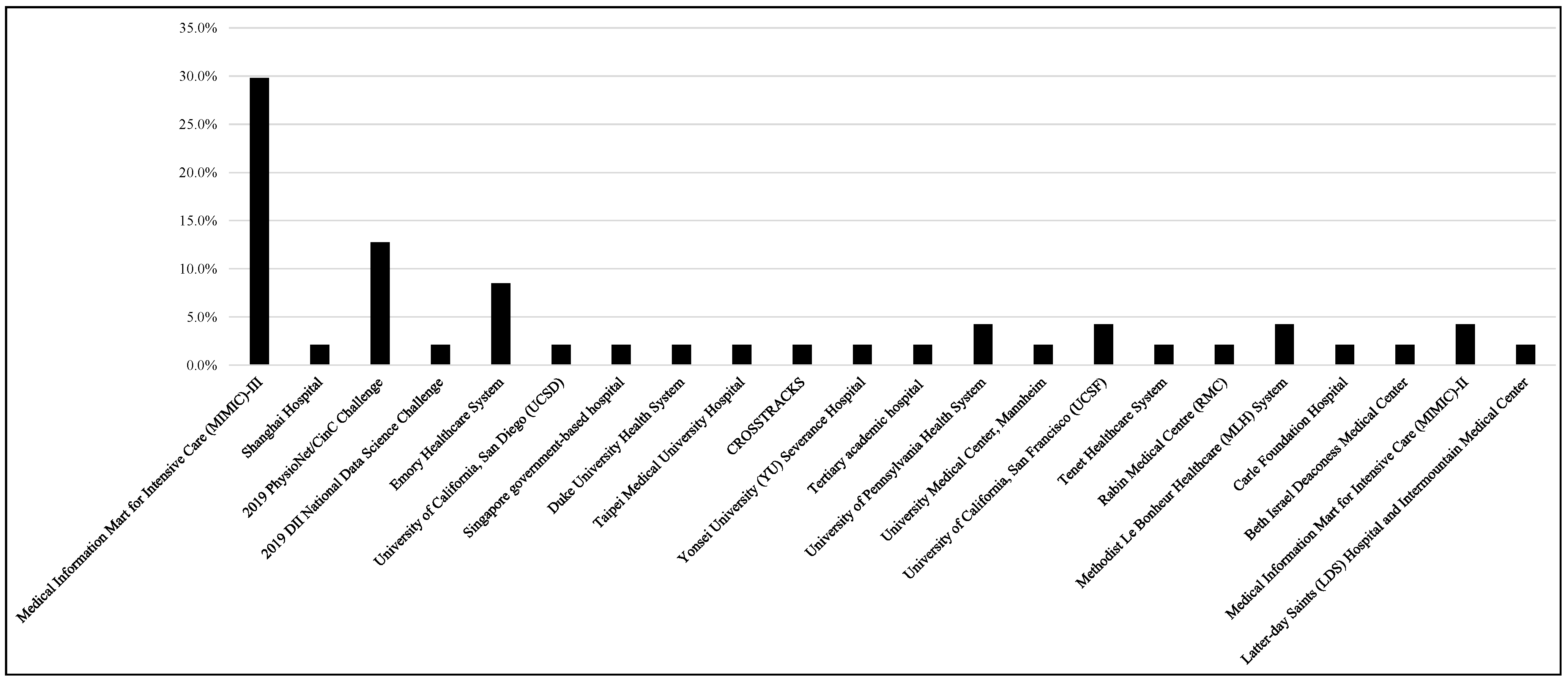
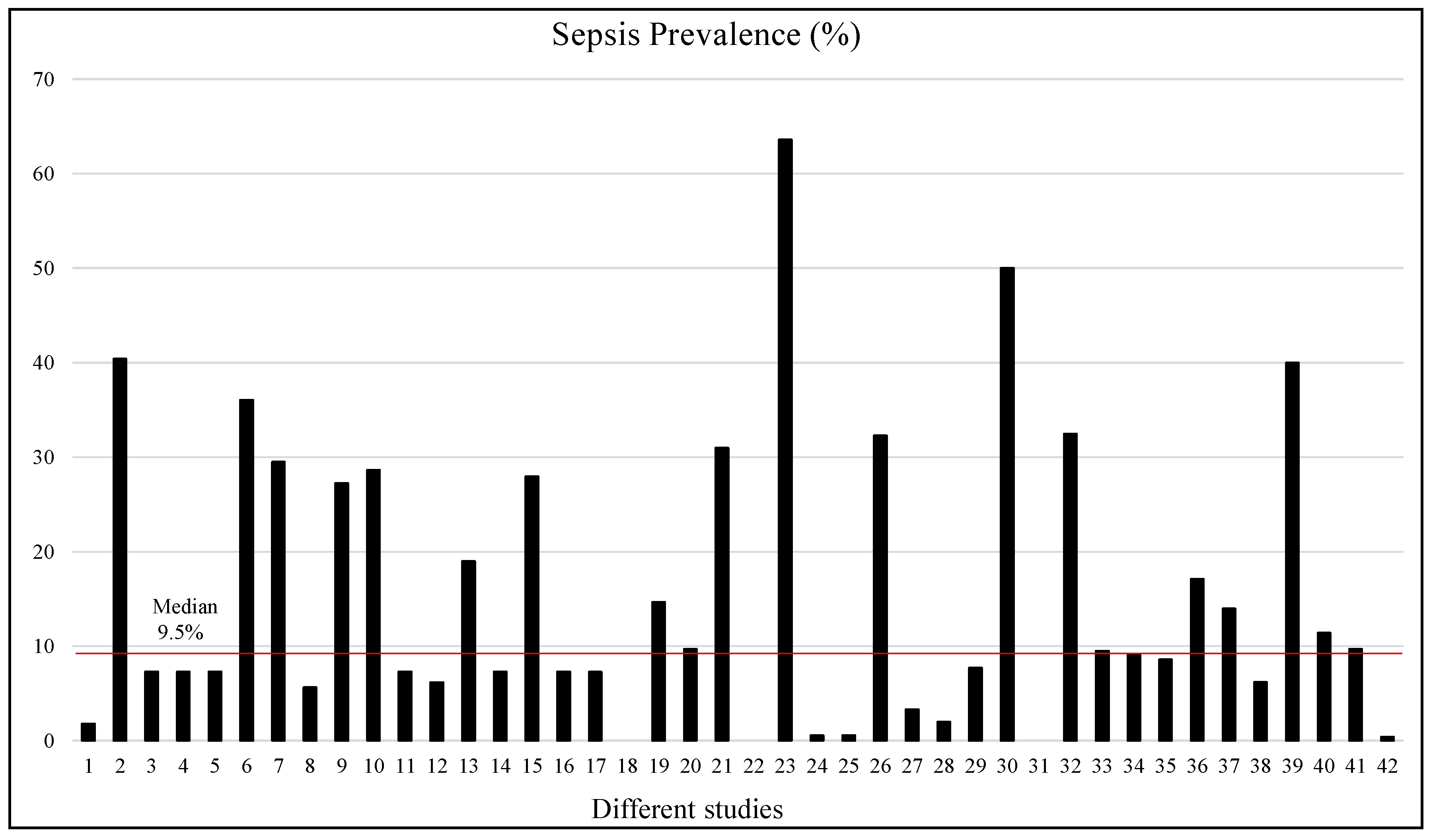
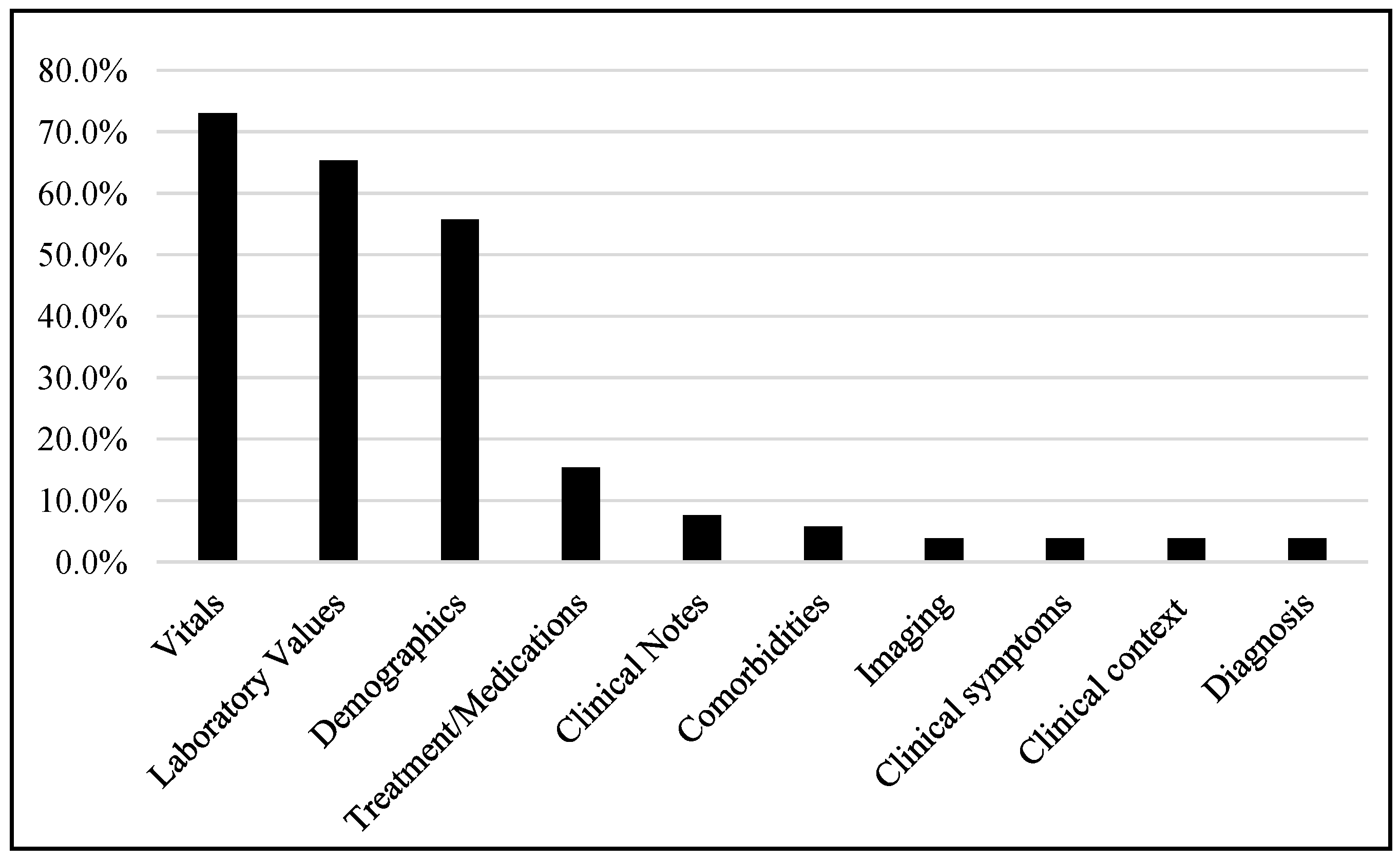
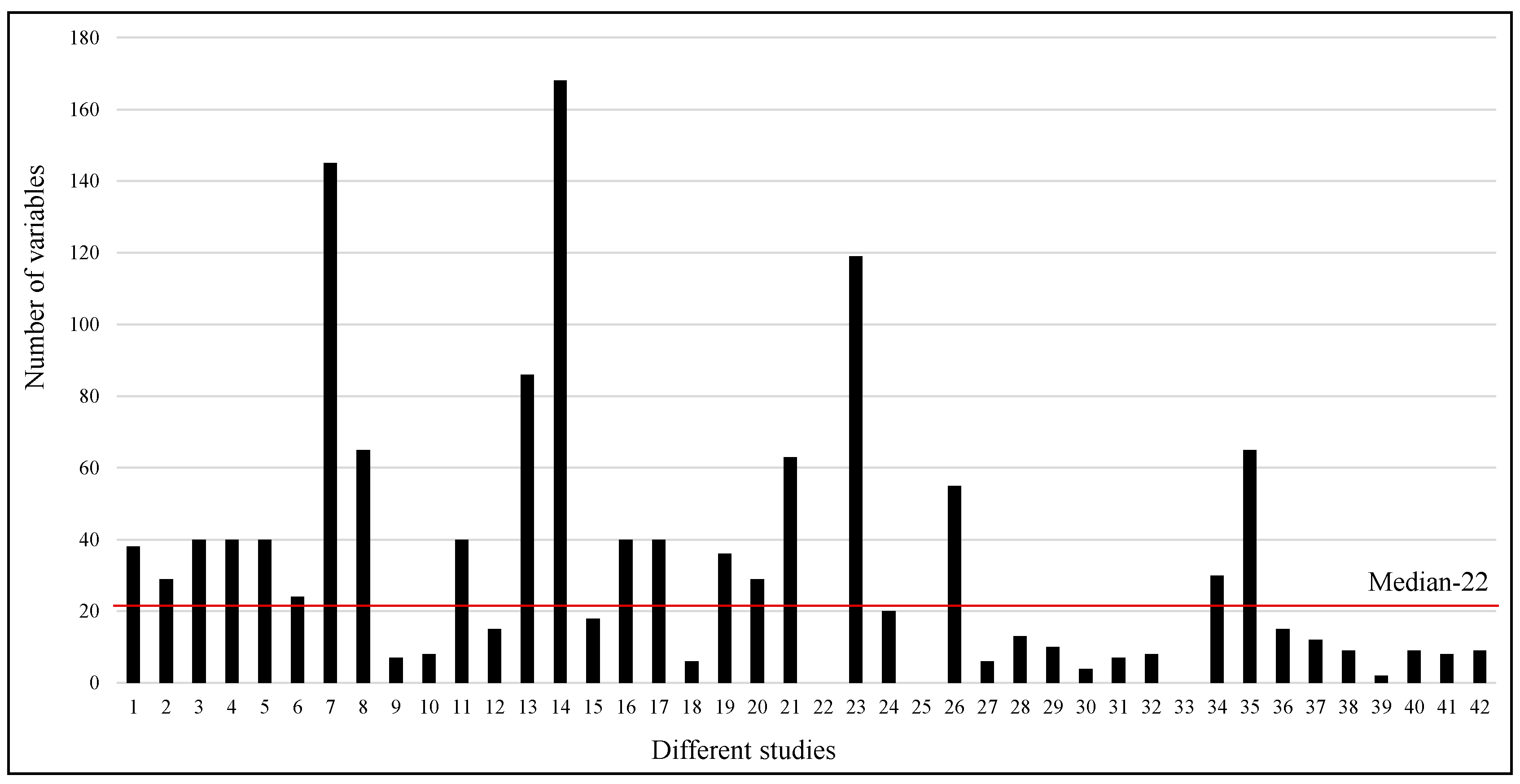
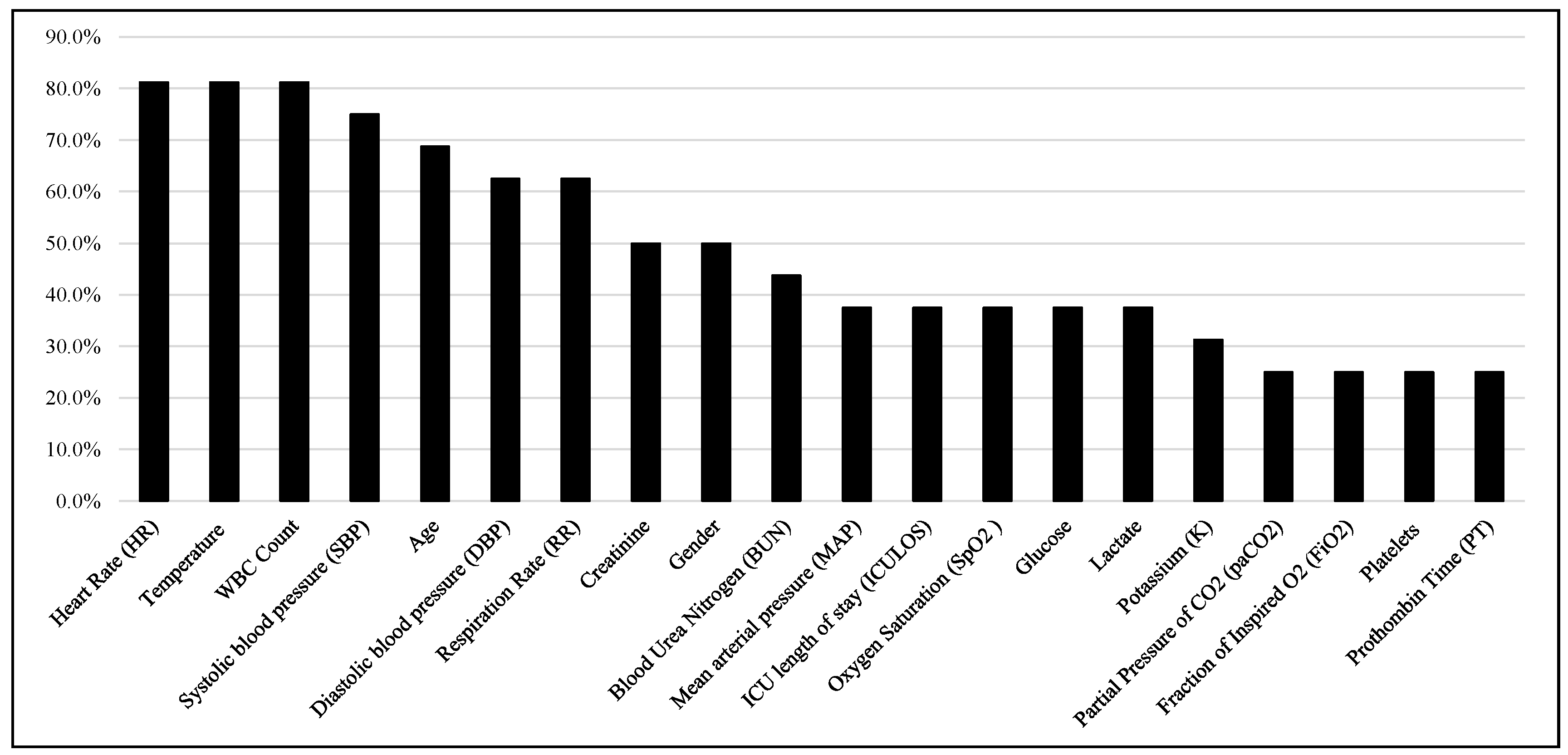
4.2. Study Characteristics
4.3. Machine Learning Models
4.4. Cross-Validation (CV) Techniques
4.5. Performance Metrics
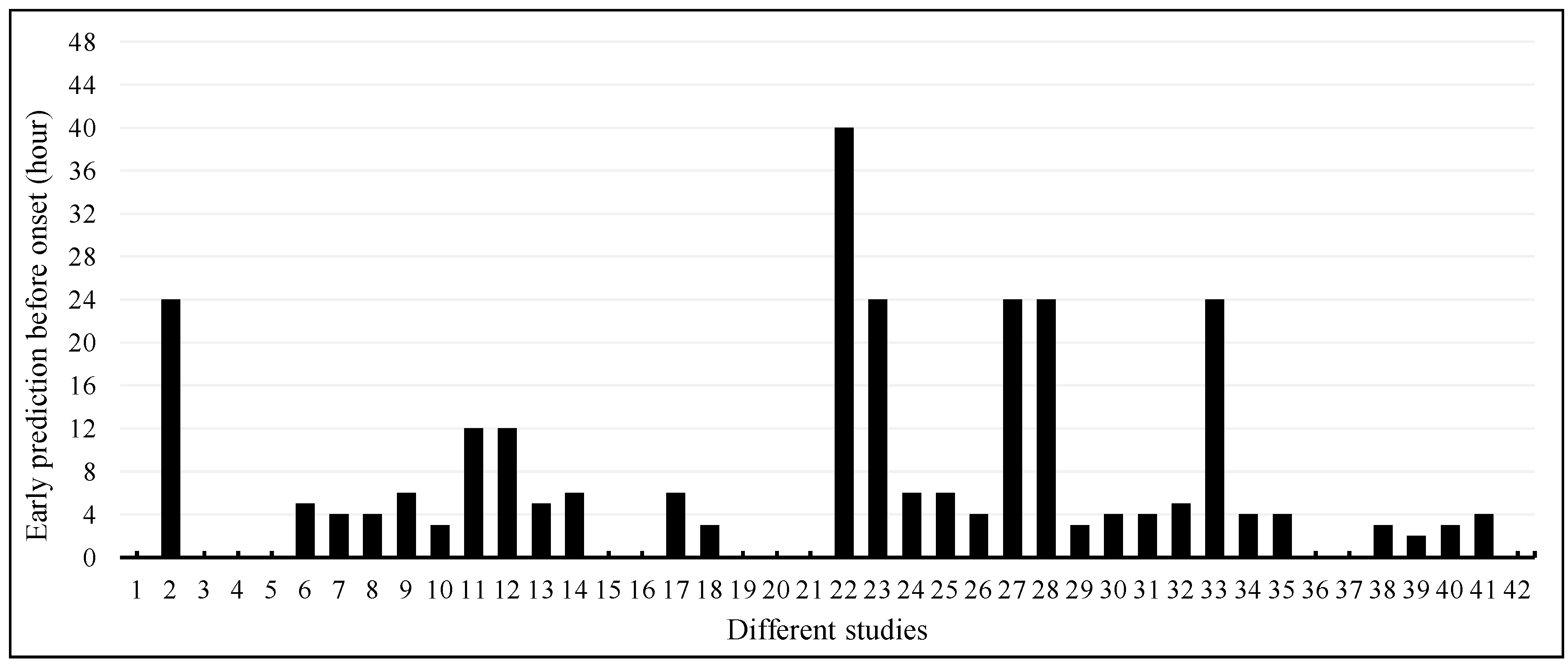
4.6. Early Prediction of Sepsis Onset
4.7. Quality Assessment of Included Studies
4.8. Impact of Funding Source
5. Discussion
5.1. Key Findings
5.2. Summaries of Recent Systematic Reviews in Relevant Fields
5.3. Limitations
5.4. Challenges and Future Directions
- EHR data can be heterogeneous, incomplete, and prone to errors, which poses challenges for accurate prediction models. Future research should focus on improving data quality and standardization, integrating data from multiple sources, and developing techniques to handle missing data effectively.
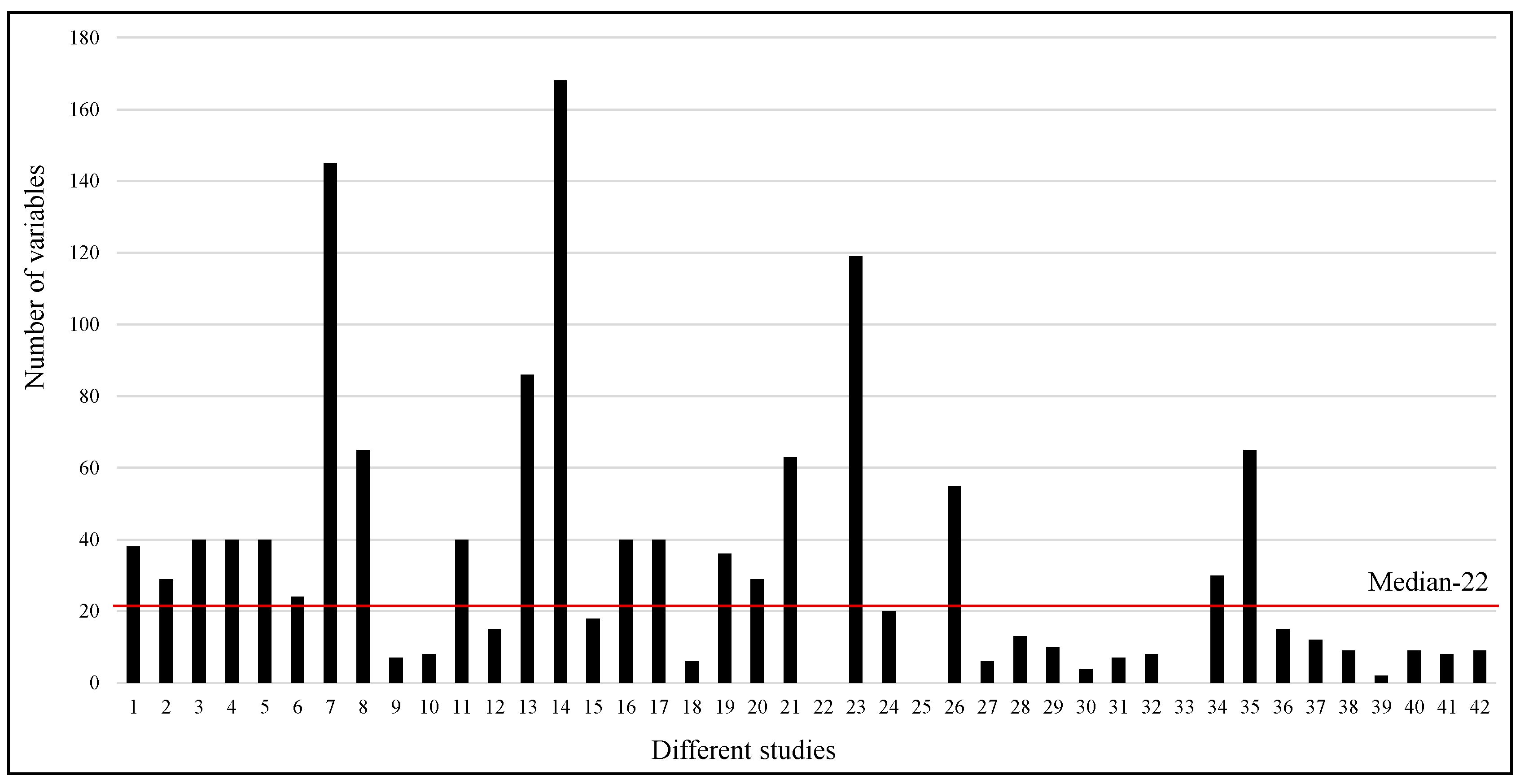
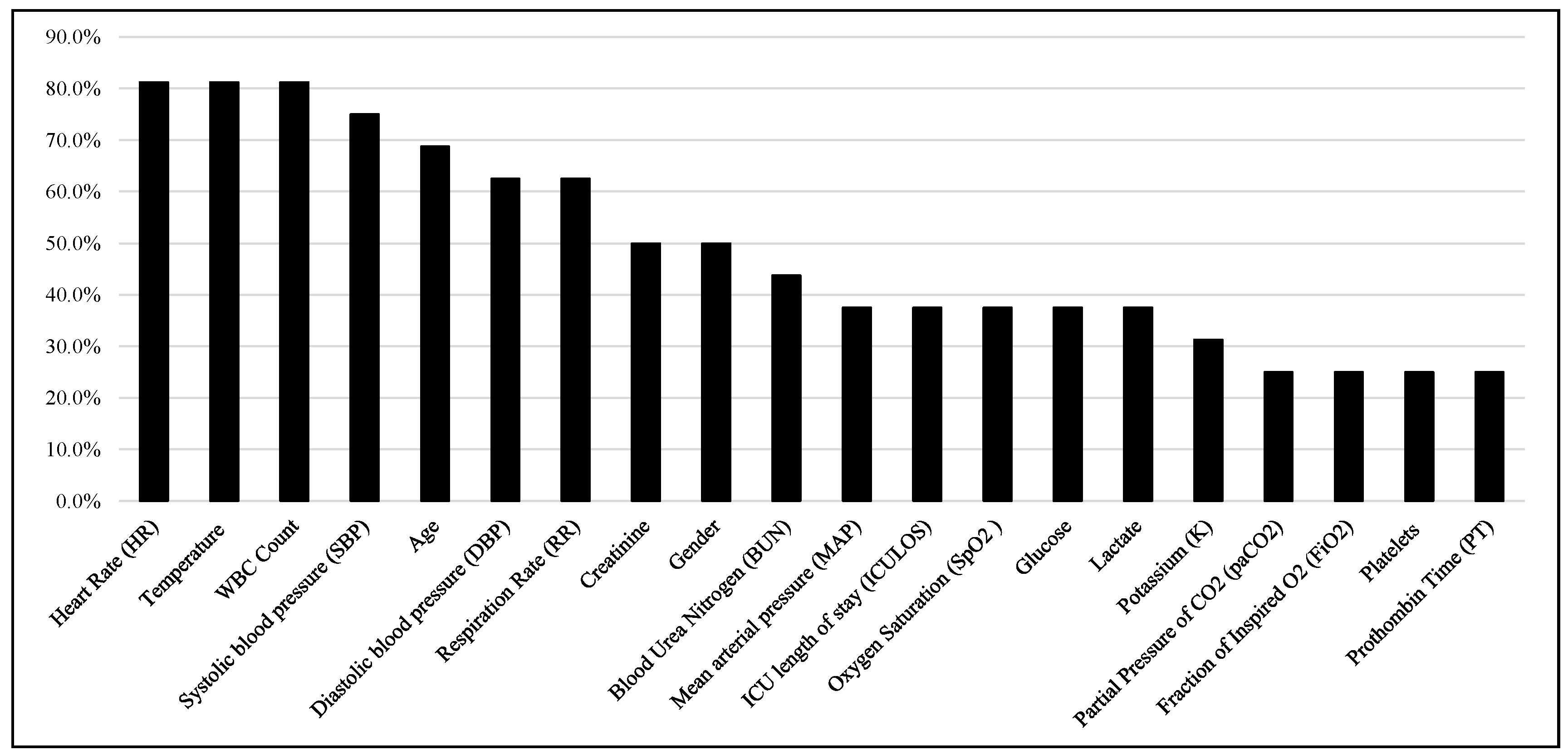
- EHR data contain a vast number of variables, and not all of them may be relevant for sepsis prediction. Feature selection techniques and advanced representation learning methods, such as deep learning, can help identify the most informative features and extract meaningful representations from the EHR data.
- Sepsis is a relatively rare event compared to non-sepsis cases, leading to imbalanced datasets. Class imbalance can affect model performance, and handling this issue requires techniques such as oversampling, under-sampling, or employing advanced algorithms designed for imbalanced data.
- Machine learning models trained on one healthcare system may not be generalized well to other institutions or patient populations. Future research should focus on the external validation and generalizability of sepsis prediction models across diverse healthcare settings to ensure their real-world effectiveness.
- Black-box machine learning models may lack interpretability, which can limit their adoption in clinical practice. Developing interpretable models and providing explanations for model predictions can enhance trust and facilitate clinicians’ understanding of the underlying reasons for sepsis predictions.
- Early detection and timely intervention are crucial for sepsis management. Future research should focus on developing real-time prediction models that integrate seamlessly into clinical workflows, triggering alerts to clinicians and facilitating prompt action.
- Demonstrating the clinical impact of machine learning-based sepsis prediction models is essential. Prospective validation studies in clinical settings are needed to assess these models’ effectiveness, impact on patient outcomes, and cost-effectiveness compared to existing clinical practices.
- EHR datasets defining sepsis onset time becomes crucial for predictive models’ clinical relevance. The challenge lies in aligning model predictions with actual clinical timelines, considering symptoms’ varying occurrence times. Symptoms manifesting hours before hospital arrival or in different healthcare settings pose complexities in early prediction models’ optimization, which necessitates detailed exploration and discussion regarding patient record alignment and optimization.
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vincent, J.L.; Opal, S.M.; Marshall, J.C.; Tracey, K.J. Sepsis definitions: Time for change. Lancet 2013, 381, 774–775. [Google Scholar] [CrossRef] [PubMed]
- Caraballo, C.; Jaimes, F. Focus: Death: Organ dysfunction in sepsis: An ominous trajectory from infection to death. Yale J. Biol. Med. 2019, 92, 629. [Google Scholar] [PubMed]
- Jain, A.; Jain, S.; Rawat, S. Emerging fungal infections among children: A review on its clinical manifestations, diagnosis, and prevention. J. Pharm. Bioallied Sci. 2010, 2, 314. [Google Scholar] [CrossRef]
- Arina, P.; Singer, M. Pathophysiology of sepsis. Curr. Opin. Anesthesiol. 2021, 34, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.Y.; Kumar, A. Empiric antimicrobial therapy in severe sepsis and septic shock: Optimizing pathogen clearance. Curr. Infect. Dis. Rep. 2015, 17, 493. [Google Scholar] [CrossRef] [PubMed]
- Dorsett, M.; Kroll, M.; Smith, C.S.; Asaro, P.; Liang, S.Y.; Moy, H.P. qSOFA has poor sensitivity for prehospital identification of severe sepsis and septic shock. Prehospital Emerg. Care 2017, 21, 489–497. [Google Scholar] [CrossRef]
- Levy, M.M.; Artigas, A.; Phillips, G.S.; Rhodes, A.; Beale, R.; Osborn, T.; Vincent, J.L.; Townsend, S.; Lemeshow, S.; Dellinger, R.P. Outcomes of the Surviving Sepsis Campaign in intensive care units in the USA and Europe: A prospective cohort study. Lancet Infect. Dis. 2012, 12, 919–924. [Google Scholar] [CrossRef]
- Hunt, A. Sepsis: An overview of the signs, symptoms, diagnosis, treatment and pathophysiology. Emerg. Nurse 2019, 27, 32–41. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013, 39, 165–228. [Google Scholar] [CrossRef]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef]
- Angus, D.C.; Linde-Zwirble, W.T.; Lidicker, J.; Clermont, G.; Carcillo, J.; Pinsky, M.R. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001, 29, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. Assessment of global incidence and mortality of hospital-treated sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Iwashyna, T.J.; Ely, E.W.; Smith, D.M.; Langa, K.M. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA 2010, 304, 1787–1794. [Google Scholar] [CrossRef]
- Rhee, C.; Murphy, M.V.; Li, L.; Platt, R.; Klompas, M. Comparison of trends in sepsis incidence and coding using administrative claims versus objective clinical data. Clin. Infect. Dis. 2015, 60, 88–95. [Google Scholar] [CrossRef]
- Shakoor, S.; Warraich, H.J.; Zaidi, A.K. Infection prevention and control in the tropics. In Hunter’s Tropical Medicine and Emerging Infectious Diseases; Elsevier: Amsterdam, The Netherlands, 2020; pp. 159–165. [Google Scholar]
- Luu, S.; Spelman, D.; Woolley, I.J. Post-splenectomy sepsis: Preventative strategies, challenges, and solutions. Infect. Drug Resist. 2019, 12, 2839–2851. [Google Scholar] [CrossRef]
- Moor, M.; Rieck, B.; Horn, M.; Jutzeler, C.R.; Borgwardt, K. Early prediction of sepsis in the ICU using machine learning: A systematic review. Front. Med. 2021, 8, 607952. [Google Scholar] [CrossRef]
- Lauritsen, S.M.; Kalør, M.E.; Kongsgaard, E.L.; Lauritsen, K.M.; Jørgensen, M.J.; Lange, J.; Thiesson, B. Early detection of sepsis utilizing deep learning on electronic health record event sequences. Artif. Intell. Med. 2020, 104, 101820. [Google Scholar] [CrossRef]
- Ramlakhan, S.; Saatchi, R.; Sabir, L.; Singh, Y.; Hughes, R.; Shobayo, O.; Ventour, D. Understanding and interpreting artificial intelligence, machine learning and deep learning in Emergency Medicine. Emerg. Med. J. 2022, 39, 380–385. [Google Scholar] [CrossRef]
- Coggins, S.A.; Glaser, K. Updates in Late-Onset Sepsis: Risk Assessment, Therapy, and Outcomes. Neoreviews 2022, 23, 738–755. [Google Scholar] [CrossRef]
- Schinkel, M.; Paranjape, K.; Panday, R.N.; Skyttberg, N.; Nanayakkara, P.W. Clinical applications of artificial intelligence in sepsis: A narrative review. Comput. Biol. Med. 2019, 115, 103488. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Nasrin, T.; Walther, B.A.; Wu, C.C.; Yang, H.C.; Li, Y.C. Prediction of sepsis patients using machine learning approach: A meta-analysis. Comput. Methods Programs Biomed. 2019, 170, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Komorowski, M.; Green, A.; Tatham, K.C.; Seymour, C.; Antcliffe, D. Sepsis biomarkers and diagnostic tools with a focus on machine learning. EBioMedicine 2022, 86, 104394. [Google Scholar] [CrossRef] [PubMed]
- Jahandideh, S.; Ozavci, G.; Sahle, B.; Kouzani, A.; Magrabi, F.; Bucknall, T. Evaluation of machine learning-based models for prediction of clinical deterioration: A systematic literature review. Int. J. Med. Inform. 2023, 175, 105084. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.F.; Sun, M.W.; Wang, Y.; Zeng, J.; Yuan, T.; Li, T.; Li, D.H.; Chen, W.; Zhou, P.; Wang, Q.; et al. Evaluating machine learning models for sepsis prediction: A systematic review of methodologies. Iscience 2022, 25, 103651. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Signori, A.; Del Puente, F.; Mora, S.; Carmisciano, L.; Briano, F.; Vena, A.; Ball, L.; Robba, C.; Pelosi, P.; et al. Early detection of sepsis with machine learning techniques: A brief clinical perspective. Front. Med. 2021, 8, 617486. [Google Scholar] [CrossRef]
- Yan, M.Y.; Gustad, L.T.; Nytrø, Ø. Sepsis prediction, early detection, and identification using clinical text for machine learning: A systematic review. J. Am. Med. Inform. Assoc. 2022, 29, 559–575. [Google Scholar] [CrossRef]
- Fleuren, L.M.; Klausch, T.L.; Zwager, C.L.; Schoonmade, L.J.; Guo, T.; Roggeveen, L.F.; Swart, E.L.; Girbes, A.R.; Thoral, P.; Ercole, A.; et al. Machine learning for the prediction of sepsis: A systematic review and meta-analysis of diagnostic test accuracy. Intensive Care Med. 2020, 46, 383–400. [Google Scholar] [CrossRef]
- Wang, D.; Li, J.; Sun, Y.; Ding, X.; Zhang, X.; Liu, S.; Han, B.; Wang, H.; Duan, X.; Sun, T. A machine learning model for accurate prediction of sepsis in ICU patients. Front. Public Health 2021, 9, 754348. [Google Scholar] [CrossRef]
- Kijpaisalratana, N.; Sanglertsinlapachai, D.; Techaratsami, S.; Musikatavorn, K.; Saoraya, J. Machine learning algorithms for early sepsis detection in the emergency department: A retrospective study. Int. J. Med. Inform. 2022, 160, 104689. [Google Scholar] [CrossRef]
- Nemati, S.; Holder, A.; Razmi, F.; Stanley, M.D.; Clifford, G.D.; Buchman, T.G. An interpretable machine learning model for accurate prediction of sepsis in the ICU. Crit. Care Med. 2018, 46, 547. [Google Scholar] [CrossRef] [PubMed]
- Singh, Y.V.; Singh, P.; Khan, S.; Singh, R.S. A machine learning model for early prediction and detection of sepsis in intensive care unit patients. J. Healthc. Eng. 2022, 2022, 9263391. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.L.; Ramsay, G.; et al. 2001 sccm/esicm/accp/ats/sis international sepsis definitions conference. Inten-Sive Care Med. 2003, 29, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of clinical criteria for sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef]
- Qiao, N. A systematic review on machine learning in sellar region diseases: Quality and reporting items. Endocr. Connect. 2019, 8, 952–960. [Google Scholar] [CrossRef]
- Gholamzadeh, M.; Abtahi, H.; Safdari, R. Comparison of different machine learning algorithms to classify patients suspected of having sepsis infection in the intensive care unit. Inform. Med. Unlocked 2023, 38, 101236. [Google Scholar] [CrossRef]
- Duan, Y.; Huo, J.; Chen, M.; Hou, F.; Yan, G.; Li, S.; Wang, H. Early prediction of sepsis using double fusion of deep features and handcrafted features. Appl. Intell. 2023, 53, 17903–17919. [Google Scholar] [CrossRef]
- Strickler, E.A.; Thomas, J.; Thomas, J.P.; Benjamin, B.; Shamsuddin, R. Exploring a global interpretation mechanism for deep learning networks when predicting sepsis. Sci. Rep. 2023, 13, 3067. [Google Scholar] [CrossRef]
- Zhou, A.; Beyah, R.; Kamaleswaran, R. OnAI-comp: An online ai experts competing framework for early sepsis detection. IEEE/ACM Trans. Comput. Biol. Bioinform. 2021, 19, 3595–3603. [Google Scholar] [CrossRef]
- Al-Mualemi, B.Y.; Lu, L. A deep learning-based sepsis estimation scheme. IEEE Access 2020, 9, 5442–5452. [Google Scholar] [CrossRef]
- Rosnati, M.; Fortuin, V. MGP-AttTCN: An interpretable machine learning model for the prediction of sepsis. PLoS ONE 2021, 16, e0251248. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Yin, C.; Hunold, K.M.; Jiang, X.; Caterino, J.M.; Zhang, P. An interpretable deep-learning model for early prediction of sepsis in the emergency department. Patterns 2021, 2, 100196. [Google Scholar] [CrossRef] [PubMed]
- Shashikumar, S.P.; Josef, C.S.; Sharma, A.; Nemati, S. DeepAISE–an interpretable and recurrent neural survival model for early prediction of sepsis. Artif. Intell. Med. 2021, 113, 102036. [Google Scholar] [CrossRef] [PubMed]
- Aşuroğlu, T.; Oğul, H. A deep learning approach for sepsis monitoring via severity score estimation. Comput. Methods Programs Biomed. 2021, 198, 105816. [Google Scholar] [CrossRef]
- Oei, S.P.; van Sloun, R.J.; van der Ven, M.; Korsten, H.H.; Mischi, M. Towards early sepsis detection from measurements at the general ward through deep learning. Intell. Based Med. 2021, 5, 100042. [Google Scholar] [CrossRef]
- Rafiei, A.; Rezaee, A.; Hajati, F.; Gheisari, S.; Golzan, M. SSP: Early prediction of sepsis using fully connected LSTM-CNN model. Comput. Biol. Med. 2021, 128, 104110. [Google Scholar] [CrossRef]
- Goh, K.H.; Wang, L.; Yeow, A.Y.; Poh, H.; Li, K.; Yeow, J.J.; Tan, G.Y. Artificial intelligence in sepsis early prediction and diagnosis using unstructured data in healthcare. Nat. Commun. 2021, 12, 711. [Google Scholar] [CrossRef]
- Bedoya, A.D.; Futoma, J.; Clement, M.E.; Corey, K.; Brajer, N.; Lin, A.; Simons, M.G.; Gao, M.; Nichols, M.; Balu, S.; et al. Machine learning for early detection of sepsis: An internal and temporal validation study. JAMIA Open 2020, 3, 252–260. [Google Scholar] [CrossRef]
- Yang, M.; Liu, C.; Wang, X.; Li, Y.; Gao, H.; Liu, X.; Li, J. An explainable artificial intelligence predictor for early detection of sepsis. Crit. Care Med. 2020, 48, e1091-6. [Google Scholar] [CrossRef]
- Yuan, K.C.; Tsai, L.W.; Lee, K.H.; Cheng, Y.W.; Hsu, S.C.; Lo, Y.S.; Chen, R.J. The development an artificial intelligence algorithm for early sepsis diagnosis in the intensive care unit. Int. J. Med. Inform. 2020, 141, 104176. [Google Scholar] [CrossRef] [PubMed]
- Kok, C.; Jahmunah, V.; Oh, S.L.; Zhou, X.; Gururajan, R.; Tao, X.; Cheong, K.H.; Gururajan, R.; Molinari, F.; Acharya, U.R. Automated prediction of sepsis using temporal convolutional network. Comput. Biol. Med. 2020, 127, 103957. [Google Scholar] [CrossRef] [PubMed]
- Reyna, M.A.; Josef, C.S.; Jeter, R.; Shashikumar, S.P.; Westover, M.B.; Nemati, S.; Clifford, G.D.; Sharma, A. Early Prediction of Sepsis from Clinical Data: The PhysioNet/Computing in Cardiology Challenge 2019. Crit. Care Med. 2020, 48, 210–217. [Google Scholar] [CrossRef]
- Choi, J.S.; Trinh, T.X.; Ha, J.; Yang, M.S.; Lee, Y.; Kim, Y.E.; Choi, J.; Byun, H.G.; Song, J.; Yoon, T.H. Implementation of complementary model using optimal combination of hematological parameters for sepsis screening in patients with fever. Sci. Rep. 2020, 10, 273. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Chang, H.; Kim, D.; Jang, D.H.; Park, I.; Kim, K. Machine learning for prediction of septic shock at initial triage in emergency department. J. Crit. Care 2020, 55, 163–170. [Google Scholar] [CrossRef]
- Ibrahim, Z.M.; Wu, H.; Hamoud, A.; Stappen, L.; Dobson, R.J.; Agarossi, A. On classifying sepsis heterogeneity in the ICU: Insight using machine learning. J. Am. Med. Inform. Assoc. 2020, 27, 437–443. [Google Scholar] [CrossRef]
- Fagerström, J.; Bång, M.; Wilhelms, D.; Chew, M.S. LiSep LSTM: A machine learning algorithm for early detection of septic shock. Sci. Rep. 2019, 9, 15132. [Google Scholar] [CrossRef]
- Kaji, D.A.; Zech, J.R.; Kim, J.S.; Cho, S.K.; Dangayach, N.S.; Costa, A.B.; Oermann, E.K. An attention based deep learning model of clinical events in the intensive care unit. PLoS ONE 2019, 14, e0211057. [Google Scholar] [CrossRef]
- Giannini, H.M.; Ginestra, J.C.; Chivers, C.; Draugelis, M.; Hanish, A.; Schweickert, W.D.; Fuchs, B.D.; Meadows, L.; Lynch, M.; Donnelly, P.J.; et al. A machine learning algorithm to predict severe sepsis and septic shock: Development, implementation and impact on clinical practice. Crit. Care Med. 2019, 47, 1485. [Google Scholar] [CrossRef]
- Ginestra, J.C.; Giannini, H.M.; Schweickert, W.D.; Meadows, L.; Lynch, M.J.; Pavan, K.; Chivers, C.J.; Draugelis, M.; Donnelly, P.J.; Fuchs, B.D.; et al. Clinician perception of a machine learning-based early warning system designed to predict severe sepsis and septic shock. Crit. Care Med. 2019, 47, 1477. [Google Scholar] [CrossRef]
- Schamoni, S.; Lindner, H.A.; Schneider-Lindner, V.; Thiel, M.; Riezler, S. Leveraging implicit expert knowledge for non-circular machine learning in sepsis prediction. Artif. Intell. Med. 2019, 100, 101725. [Google Scholar] [CrossRef] [PubMed]
- Barton, C.; Chettipally, U.; Zhou, Y.; Jiang, Z.; Lynn-Palevsky, A.; Le, S.; Calvert, J.; Das, R. Evaluation of a machine learning algorithm for up to 48-hour advance prediction of sepsis using six vital signs. Comput. Biol. Med. 2019, 109, 79–84. [Google Scholar] [CrossRef]
- Delahanty, R.J.; Alvarez, J.; Flynn, L.M.; Sherwin, R.L.; Jones, S.S. Development and evaluation of a machine learning model for the early identification of patients at risk for sepsis. Ann. Emerg. Med. 2019, 73, 334–344. [Google Scholar] [CrossRef]
- Scherpf, M.; Gräßer, F.; Malberg, H.; Zaunseder, S. Predicting sepsis with a recurrent neural network using the MIMIC III database. Comput. Biol. Med. 2019, 113, 103395. [Google Scholar] [CrossRef] [PubMed]
- Bloch, E.; Rotem, T.; Cohen, J.; Singer, P.; Aperstein, Y. Machine learning models for analysis of vital signs dynamics: A case for sepsis onset prediction. J. Healthc. Eng. 2019, 2019, 5930379. [Google Scholar] [CrossRef] [PubMed]
- van Wyk, F.; Khojandi, A.; Kamaleswaran, R. Improving prediction performance using hierarchical analysis of real-time data: A sepsis case study. IEEE J. Biomed. Health Inform. 2019, 23, 978–986. [Google Scholar] [CrossRef]
- van Wyk, F.; Khojandi, A.; Mohammed, A.; Begoli, E.; Davis, R.L.; Kamaleswaran, R. A minimal set of physiomarkers in continuous high frequency data streams predict adult sepsis onset earlier. Int. J. Med. Inform. 2019, 122, 55–62. [Google Scholar] [CrossRef]
- Yee, C.R.; Narain, N.R.; Akmaev, V.R.; Vemulapalli, V. A data-driven approach to predicting septic shock in the intensive care unit. Biomed. Inform. Insights 2019, 11, 1178222619885147. [Google Scholar] [CrossRef]
- Mao, Q.; Jay, M.; Hoffman, J.L.; Calvert, J.; Barton, C.; Shimabukuro, D.; Shieh, L.; Chettipally, U.; Fletcher, G.; Kerem, Y.; et al. Multicentre validation of a sepsis prediction algorithm using only vital sign data in the emergency department, general ward and ICU. BMJ Open 2018, 8, e017833. [Google Scholar] [CrossRef]
- Taneja, I.; Reddy, B.; Damhorst, G.; Dave Zhao, S.; Hassan, U.; Price, Z.; Jensen, T.; Ghonge, T.; Patel, M.; Wachspress, S.; et al. Combining biomarkers with EMR data to identify patients in different phases of sepsis. Sci. Rep. 2017, 7, 10800. [Google Scholar] [CrossRef]
- Horng, S.; Sontag, D.A.; Halpern, Y.; Jernite, Y.; Shapiro, N.I.; Nathanson, L.A. Creating an automated trigger for sepsis clinical decision support at emergency department triage using machine learning. PLoS ONE 2017, 12, e0174708. [Google Scholar] [CrossRef]
- Kam, H.J.; Kim, H.Y. Learning representations for the early detection of sepsis with deep neural networks. Comput. Biol. Med. 2017, 89, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Shashikumar, S.P.; Li, Q.; Clifford, G.D.; Nemati, S. Multiscale network representation of physiological time series for early prediction of sepsis. Physiol. Meas. 2017, 38, 2235. [Google Scholar] [CrossRef] [PubMed]
- Calvert, J.S.; Price, D.A.; Chettipally, U.K.; Barton, C.W.; Feldman, M.D.; Hoffman, J.L.; Jay, M.; Das, R. A computational approach to early sepsis detection. Comput. Biol. Med. 2016, 74, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Desautels, T.; Calvert, J.; Hoffman, J.; Jay, M.; Kerem, Y.; Shieh, L.; Shimabukuro, D.; Chettipally, U.; Feldman, M.D.; Barton, C.; et al. Prediction of sepsis in the intensive care unit with minimal electronic health record data: A machine learning approach. JMIR Med. Inf. 2016, 4, e28. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.M.; Jones, J.; Kuttler, K.G.; Keddington, R.K.; Allen, T.L.; Haug, P. Prospective evaluation of an automated method to identify patients with severe sepsis or septic shock in the emergency department. BMC Emerg. Med. 2016, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Henry, K.E.; Hager, D.N.; Pronovost, P.J.; Saria, S. A targeted real-time early warning score (TREWScore) for septic shock. Sci. Transl. Med. 2015, 7, 299ra122. [Google Scholar] [CrossRef]
- Taylor, S.P.; Bray, B.C.; Chou, S.H.; Burns, R.; Kowalkowski, M.A. Clinical subtypes of sepsis survivors predict readmission and mortality after hospital discharge. Ann. Am. Thorac. Soc. 2022, 19, 1355–1363. [Google Scholar] [CrossRef]
- Tang, B.M.; Eslick, G.D.; Craig, J.C.; McLean, A.S. Accuracy of procalcitonin for sepsis diagnosis in critically ill patients: Systematic review and meta-analysis. Lancet Infect. Dis. 2007, 7, 210–217. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Authors | Year of Publication | Dataset(s) | Sepsis Definition | Sample Size | Sepsis Positive Patients | Sepsis Prevalence (%) | Data Types | Number of Variables | Model(s) | AUROC | Retrospective (R) or Prospective (P) ? | Output Metrics | Hours before Onset |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Gholamzadeh et al. [38] | 2023 | MIMIC-III | Sepsis-3 | 1,552,210 | 27,916 | 1.79 | Demographics, labs, vitals | 38 | DT, RF, XGB | 0.918 | R | AUROC, A, P, R, S, F1 | - |
| 2 | Duan et al. [39] | 2023 | Shanghai Hospital | Sepsis-2 | 282 | 114 | 40.43 | Demographics, labs, vitals | 29 | Double fusion DL framework | 0.92 | R | AUC, A, S, R | 24 |
| 3 | Strickler et al. [40] | 2023 | 2019 PhysioNet/CinC Challenge | Sepsis-3 | 40,336 | 2932 | 7.33 | Demographics, labs, vitals | 40 | CSE, MSC-LSTM, MSC-CSE | - | R | A, P, S, R, F1, MCC, Utility | - |
| 4 | Zhou et al. [41] | 2021 | 2019 PhysioNet/CinC Challenge | Sepsis-3 | 40,336 | 2932 | 7.33 | Demographics, labs, vitals | 40 | RG, XGB, LR, RF, SVC | - | R | Average regret | - |
| 5 | Al-Mualemi and Lu [42] | 2021 | 2019 PhysioNet/CinC Challenge | Sepsis-3 | 40,336 | 2932 | 7.33 | Demographics, labs, vitals | 40 | SVM, RNN-LSTM, Adaptive CNN | - | R | A, S, R | - |
| 6 | Rosnati and Fortuin [43] | 2021 | MIMIC-III | Sepsis-3 | 22,007 | 7936 | 36.06 | Labs, vitals | 24 | MGP-AttTCN | 0.660 | R | AUC | 5 |
| 7 | Zhang et al. [44] | 2021 | 2019 DII National Data Science Challenge | Sepsis-2 | 178,843 | 52,802 | 29.5 | Demographics, labs, vitals | 145 | GRU, RETAIN, Dipole, LSTM | 0.892 | R | AUC | 4 |
| 8 | Shashikumar et al. [45] | 2021 | Emory Healthcare System, UCSD, MIMIC-III | Sepsis-3 | 85,046 | 4794 | 5.64 | Demographics, labs, vitals | 65 | DeepAISE | 0.90 | R | AUC | 4 |
| 9 | Aşuroğlu and Oğul [46] | 2021 | MIMIC-III | Sepsis-3 | 5154 | 1404 | 27.24 | Vitals | 7 | DSPA | 0.97 | R | AUC | 6 |
| 10 | Oei et al. [47] | 2021 | MIMIC-III | Sepsis-3 | 48,632 | 13,935 | 28.65 | Labs, vitals | 8 | Deep learning | 0.86 | R | AUC | 3 |
| 11 | Rafiei et al. [48] | 2021 | 2019 PhysioNet/CinC Challenge | Sepsis-3 | 40,336 | 2932 | 7.33 | Demographics, labs, vitals | 40 | Smart Sepsis Predictor | 0.86 | R | AUC, S, A | 12 |
| 12 | Goh et al. [49] | 2021 | Singapore government-based hospital | Sepsis-3 | 5317 | 327 | 6.15 | Demographic, vitals, notes, labs, treatment | 15 | SERA algorithm | 0.94 | P | AUC, R, S | 12 |
| 13 | Bedoya et al. [50] | 2020 | Duke University Health System | Sepsis-2 | 42,979 | 8160 | 19.0 | Demographics, vital, lab, comorbidities, medications | 86 | RNN, LR, RF | 0.88 | R | AUROC | 5 |
| 14 | Yang et al. [51] | 2020 | 2019 PhysioNet/CinC Challenge | Sepsis-3 | 40,336 | 2932 | 7.33 | Demographics, labs, vitals | 168 | XGB, EASP | 0.85 | R | Utility score, AUROC, R, S | 6 |
| 15 | Yuan et al. [52] | 2020 | Taipei Medical University Hospital | Sepsis-2 | 1588 | 444 | 27.96 | Vitals, lab, exam reports, text and images | 18 | GB | 0.89 | P | F1 score, A, R, S, PPV | - |
| 16 | Kok et al. [53] | 2020 | 2019 PhysioNet/CinC Challenge | Sepsis-3 | 40,000 | 2932 | 7.33 | Demographics, labs, vitals | 40 | TCN | 0.99 | R | A, R, S, AUROC, AUPRC | - |
| 17 | Reyna et al. [54] | 2020 | Emory Healthcare System, MIMIC-III | Sepsis-3 | 60,000 | 2932 | 7.3 | Demographics, labs, vitals | 40 | ML Models | 0.815 | R | AUROC, Utility | 6 |
| 18 | Lauritsen et al. [19] | 2020 | CROSSTRACKS | Sepsis-2 | 3126 | - | - | Diagnoses, labs, vitals, imaging, medications, treatment | 6 | CNN-LSTM | 0.88 | R | AUROC, mAP | 3 |
| 19 | Choi et al. [55] | 2020 | Yonsei University (YU) Severance Hospital | Sepsis (ICD-10) | 7743 | 1136 | 14.67 | laboratory data | 36 | LR | 0.86 | R | A, AUROC, R, S, PPV, NPV | - |
| 20 | Kim et al. [56] | 2020 | Tertiary academic hospital | Sepsis-3 | 49,560 | 4817 | 9.7 | Demographics, labs, vitals | 29 | SVM, GB, MARS, LASSO, Ridge, RF | 0.93 | R | AUROC, R, S, PPV, NPV | - |
| 21 | Ibrahim et al. [57] | 2020 | MIMIC-III | Sepsis-2 | 13,728 | 4256 | 31.0 | Vitals, labs | 63 | RF, GB, SVM | 0.96 | R | R, S, AUC, PLR, NLR | - |
| 22 | Fagerstrom et al. [58] | 2019 | MIMIC-III | Sepsis-2 | 59,000 | - | - | Demographics, labs, vitals, treatment, medications, diagnoses | - | LSTM | 0.83 | R | AUROC | 40 |
| 23 | Kaji et al. [59] | 2019 | MIMIC-III | Sepsis-2 | 36,176 | 23,008 | 63.6 | Demographics, labs, vitals, medications | 119 | LSTM | 0.88 | R | AUROC, R, PPV | 24 |
| 24 | Giannini et al. [60] | 2019 | University of Pennsylvania Health System | Sepsis (ICD-9) | 172,700 | 950 | 0.55 | Demographics, labs, vitals | 20 | RF | 0.88 | R | AUROC, R, S | 6 |
| 25 | Ginestra et al. [61] | 2019 | University of Pennsylvania Health System | Sepsis (ICD-9) | 162,212 | 943 | 0.58 | Vitals, comorbidity, labs | - | Early Warning Systems 2.0 (EWS 2.0) | - | P | Response rate | 6 |
| 26 | Schamoni et al. [62] | 2019 | University Medical Center, Mannheim | Sepsis-3 | 620 | 200 | 32.3 | Demographics, Labs, clinical data | 55 | Non-Linear ordinal regression | 0.84 | R | AUROC | 4 |
| 27 | Barton et al. [63] | 2019 | MIMIC-III, UCSF | Sepsis-3 | 112,952 | 3673 | 3.3 | Vitals | 6 | XGBoost | 0.88 | R | AUROC, R, S | 24 |
| 28 | Delahanty et al. [64] | 2019 | Tenet Healthcare System | Sepsis-3 | 2,759,529 | 54,661 | 1.98 | Demographics, labs, vitals, medications, nursing notes | 13 | GB | 0.97 | R | AUROC, R, S, P | 24 |
| 29 | Scherpf et al. [65] | 2019 | MIMIC-III | Sepsis-2 | 46,520 | 2724 | 7.7 | Lab, vitals | 10 | RNN-GRU, Insight | 0.81 | R | AUROC | 3 |
| 30 | Bloch et al. [66] | 2019 | RMC | Sepsis-2 | 600 | 300 | 50 | Vitals | 4 | NN, SVM, LR | 0.88 | R | AUROC, R, S, PPV, NPV | 4 |
| 31 | VanWyk et al. [67] | 2019 | MLH System | Sepsis (ICD10) | 586 | - | - | Lab, vitals | 7 | RF, RNN | - | R | F2 score, A, R, S, PPV | 4 |
| 32 | van Wyk et al. [68] | 2019 | MLH System | Sepsis-2 | 1161 | 377 | 32.47 | Demographics, vitals | 8 | RF | - | R | R, F1 | 5 |
| 33 | Yee et al. [69] | 2019 | MIMIC-III | Sepsis-3 | 9165 | 872 | 9.5 | Demographics, labs, vitals, diagnosis | Bayesian network | 0.81 | R | AUROC, R, S, PPV, NPV | 24 | |
| 34 | Mao et al. [70] | 2018 | MIMIC-III, UCSF | Sepsis-2 | 90,353 | 1965 | 9.1 | Vitals | 30 | Insight | 0.92 | R | AUROC, R, S | 4 |
| 35 | Nemati et al. [32] | 2018 | Emory Healthcare System | Sepsis-3 | 27,527 | 2375 | 8.6 | Demographics, labs, vitals, clinical data | 65 | AISE | 0.85 | R | A, R, S, AUC | 4 |
| 36 | Taneja et al. [71] | 2017 | Carle Foundation Hospital | Sepsis-3 | 444 | 76 | 17.11 | Demographics, labs, vitals | 15 | SVM | 0.81 | R | R, S, AUC | - |
| 37 | Horng et al. [72] | 2017 | Beth Israel Deaconess Medical Center | Sepsis (ICD-9) | 230,936 | 32,331 | 14 | Vitals, demographics, and notes | 12 | SVM | 0.86 | R | AUROC, R, S, PPV | - |
| 38 | Kam and Kim [73] | 2017 | MIMIC-II | Sepsis-2 | 6362 | 360 | 6.2 | Demographics, labs, vitals | 9 | Sepsis LSTM (SepLSTM) | 0.92 | R | A, R, S, AUC | 3 |
| 39 | Shashikumar et al. [74] | 2017 | Emory Healthcare System | Sepsis-3 | 250 | 100 | 40.0 | Demographics, comorbidity, clinical context, vitals | 2 | SVM | 0.80 | P | AUROC, S | 2 |
| 40 | Calvert et al. [75] | 2016 | MIMIC-II | Sepsis-2 | 1394 | 159 | 11.4 | Demographics, labs, vitals | 9 | InSight | 0.92 | R | A, AUROC, R, S | 3 |
| 41 | Desautels et al. [76] | 2016 | MIMIC-III | Sepsis-3 | 22,853 | 1840 | 9.7 | Demographics, labs, vitals | 8 | InSight | 0.88 | R | AUROC | 4 |
| 42 | Brown et al. [77] | 2016 | LDS Hospital and Intermountain Medical Center | Sepsis (ICD-9) | 132,748 | 549 | 0.41 | Demographics, labs, vitals | 9 | NB | 0.953 | R | AUROC, R, S, PPV, NPV | - |
| Number | Authors | Year of Publication | Sample Size > 50 | Data Availability | Code Availability | Mobile or Web Deployment | Handling of Missing Data | Sepsis Prevalence | Feature Engineering | Machine Learning Models | Hyperparameters | Sepsis Definition Adhered in Study Design | Valid Methods to Prevent Overfitting | Reporting of Performance Matrix | External Data Validation | Explainability | Limitations of the Study | Clinical Applicability Discussion | Score (%) | Quality Category |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Gholamzadeh et al. [38] | 2023 | √ | √ | × | × | √ | √ | √ | √ | × | √ | √ | √ | × | × | √ | √ | 68.75 | AAQ |
| 2 | Duan et al. [39] | 2023 | √ | × | × | × | √ | × | √ | √ | √ | √ | √ | √ | × | × | √ | × | 56.25 | AQ |
| 3 | Strickler et al. [40] | 2023 | √ | √ | × | × | √ | √ | √ | √ | √ | √ | √ | √ | × | √ | √ | × | 75.00 | AAQ |
| 4 | Zhou et al. [41] | 2021 | √ | √ | √ | √ | × | √ | √ | √ | √ | √ | × | √ | × | √ | √ | √ | 81.25 | HQ |
| 5 | Al-Mualemi and Lu [42] | 2021 | √ | √ | × | × | √ | √ | √ | √ | × | √ | × | √ | × | × | √ | √ | 62.50 | AAQ |
| 6 | Rosnati and Fortuin [43] | 2021 | √ | √ | √ | × | √ | √ | √ | √ | √ | √ | × | √ | × | √ | × | × | 68.75 | AAQ |
| 7 | Zhang et al. [44] | 2021 | √ | × | √ | × | √ | √ | √ | √ | √ | √ | √ | √ | × | √ | × | √ | 75.00 | AAQ |
| 8 | Shashikumar et al. [45] | 2021 | √ | √ | × | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | × | √ | 87.50 | HQ |
| 9 | Aşuroğlu and Oğul [46] | 2021 | √ | √ | × | × | √ | √ | √ | √ | √ | √ | × | √ | × | × | √ | √ | 68.75 | AAQ |
| 10 | Oei et al. [47] | 2021 | √ | √ | × | × | √ | √ | √ | √ | √ | √ | √ | √ | × | × | × | × | 62.50 | AAQ |
| 11 | Rafiei et al. [48] | 2021 | √ | √ | × | × | √ | √ | √ | √ | × | √ | √ | √ | × | × | √ | √ | 68.75 | AAQ |
| 12 | Goh et al. [49] | 2021 | √ | × | × | × | × | √ | √ | √ | × | √ | × | √ | √ | × | √ | √ | 56.25 | AQ |
| 13 | Bedoya et al. [50] | 2020 | √ | × | × | × | √ | √ | √ | √ | √ | √ | × | √ | √ | × | √ | × | 62.50 | AAQ |
| 14 | Yang et al. [51] | 2020 | √ | √ | √ | × | √ | √ | √ | √ | × | √ | × | √ | × | √ | √ | × | 68.75 | AAQ |
| 15 | Yuan et al. [52] | 2020 | √ | × | × | × | √ | √ | √ | √ | × | √ | × | √ | × | × | √ | × | 50.00 | AQ |
| 16 | Kok et al. [53] | 2020 | √ | √ | × | × | √ | √ | × | √ | √ | √ | √ | √ | × | × | √ | √ | 68.75 | AAQ |
| 17 | * Reyna et al. [54] | 2020 | √ | √ | √ | × | √ | √ | × | × | × | √ | × | √ | × | × | × | × | 43.75 | AQ |
| 18 | Lauritsen et al. [19] | 2020 | √ | × | × | × | √ | √ | √ | √ | √ | √ | √ | √ | × | × | √ | √ | 68.75 | AAQ |
| 19 | Choi et al. [55] | 2020 | √ | × | × | × | √ | √ | √ | √ | × | √ | × | √ | × | × | √ | × | 50.00 | AQ |
| 20 | Kim et al. [56] | 2020 | √ | × | × | × | √ | √ | √ | √ | √ | √ | √ | √ | × | × | √ | × | 62.50 | AAQ |
| 21 | Ibrahim et al. [57] | 2020 | √ | √ | × | × | √ | √ | √ | √ | √ | √ | √ | √ | × | × | × | × | 62.50 | AAQ |
| 22 | Fagerstrom et al. [58] | 2019 | √ | √ | × | × | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | × | 81.25 | HQ |
| 23 | Kaji et al. [59] | 2019 | √ | √ | √ | × | √ | √ | √ | √ | √ | √ | × | √ | × | √ | √ | √ | 81.25 | HQ |
| 24 | Giannini et al. [60] | 2019 | √ | × | × | × | × | √ | × | × | × | √ | × | √ | × | × | × | √ | 31.25 | LQ |
| 25 | Ginestra et al. [61] | 2019 | √ | × | × | × | × | √ | × | × | × | √ | × | √ | × | × | √ | √ | 37.50 | LQ |
| 26 | Schamoni et al. [62] | 2019 | √ | × | × | × | √ | √ | √ | √ | √ | √ | × | √ | √ | × | × | √ | 62.50 | AAQ |
| 27 | Barton et al. [63] | 2019 | √ | × | × | × | √ | √ | √ | √ | √ | √ | √ | √ | √ | × | √ | √ | 75.00 | AAQ |
| 28 | Delahanty et al. [64] | 2019 | √ | × | × | × | × | √ | √ | √ | × | √ | × | √ | × | × | √ | √ | 50.00 | AQ |
| 29 | Scherpf et al. [65] | 2019 | √ | √ | × | × | √ | √ | √ | √ | × | √ | × | √ | × | × | √ | √ | 62.50 | AAQ |
| 30 | Bloch et al. [66] | 2019 | √ | × | × | × | × | √ | √ | √ | × | √ | × | √ | × | × | √ | × | 43.75 | AQ |
| 31 | VanWyk et al. [67] | 2019 | √ | × | × | × | × | √ | × | √ | √ | √ | × | √ | × | × | √ | √ | 50.00 | AQ |
| 32 | van Wyk et al. [68] | 2019 | √ | × | × | × | × | √ | √ | √ | √ | √ | √ | √ | × | × | √ | × | 56.25 | AQ |
| 33 | Yee et al. [69] | 2019 | √ | √ | × | × | × | √ | × | √ | × | √ | × | √ | × | × | × | √ | 43.75 | AQ |
| 34 | Mao et al. [70] | 2018 | √ | √ | × | × | √ | √ | √ | √ | × | √ | √ | √ | × | × | √ | √ | 68.75 | AAQ |
| 35 | Nemati et al. [32] | 2018 | √ | √ | × | × | √ | √ | √ | √ | × | √ | √ | √ | √ | √ | √ | √ | 81.25 | HQ |
| 36 | Taneja et al. [71] | 2017 | √ | × | × | × | × | √ | √ | √ | × | √ | × | √ | × | × | × | × | 37.50 | LQ |
| 37 | Horng et al. [72] | 2017 | √ | × | × | × | √ | √ | √ | √ | × | √ | × | √ | × | × | √ | × | 50.00 | AQ |
| 38 | Kam and Kim [73] | 2017 | √ | √ | × | × | √ | √ | √ | √ | × | √ | √ | √ | × | × | √ | × | 62.50 | AAQ |
| 39 | Shashikumar et al. [74] | 2017 | √ | × | × | × | × | √ | √ | √ | × | √ | × | √ | × | × | × | × | 37.50 | LQ |
| 40 | Calvert et al. [75] | 2016 | √ | √ | × | × | × | √ | × | √ | × | √ | √ | √ | × | × | √ | × | 50.00 | AQ |
| 41 | Desautels et al. [76] | 2016 | √ | √ | × | × | √ | √ | √ | √ | × | √ | × | √ | × | × | √ | × | 56.25 | AQ |
| 42 | Brown et al. [77] | 2016 | √ | × | × | × | × | × | √ | √ | × | √ | × | √ | × | × | √ | × | 37.50 | LQ |
| % prevalence of each category | 100% | 52% | 14% | 5% | 69% | 95% | 83% | 93% | 46% | 100% | 43% | 100% | 17% | 21% | 74% | 50% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, K.R.; Prithula, J.; Kumar, J.; Tan, T.L.; Reaz, M.B.I.; Sumon, M.S.I.; Chowdhury, M.E.H. Machine Learning-Based Early Prediction of Sepsis Using Electronic Health Records: A Systematic Review. J. Clin. Med. 2023, 12, 5658. https://doi.org/10.3390/jcm12175658
Islam KR, Prithula J, Kumar J, Tan TL, Reaz MBI, Sumon MSI, Chowdhury MEH. Machine Learning-Based Early Prediction of Sepsis Using Electronic Health Records: A Systematic Review. Journal of Clinical Medicine. 2023; 12(17):5658. https://doi.org/10.3390/jcm12175658
Chicago/Turabian StyleIslam, Khandaker Reajul, Johayra Prithula, Jaya Kumar, Toh Leong Tan, Mamun Bin Ibne Reaz, Md. Shaheenur Islam Sumon, and Muhammad E. H. Chowdhury. 2023. "Machine Learning-Based Early Prediction of Sepsis Using Electronic Health Records: A Systematic Review" Journal of Clinical Medicine 12, no. 17: 5658. https://doi.org/10.3390/jcm12175658
APA StyleIslam, K. R., Prithula, J., Kumar, J., Tan, T. L., Reaz, M. B. I., Sumon, M. S. I., & Chowdhury, M. E. H. (2023). Machine Learning-Based Early Prediction of Sepsis Using Electronic Health Records: A Systematic Review. Journal of Clinical Medicine, 12(17), 5658. https://doi.org/10.3390/jcm12175658