



Electroanatomical Conduction Characteristics of Pig Myocardial Tissue Derived from High-Density Mapping
 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Electroanatomical Mapping
2.2. Post-Processing in Rhythmia
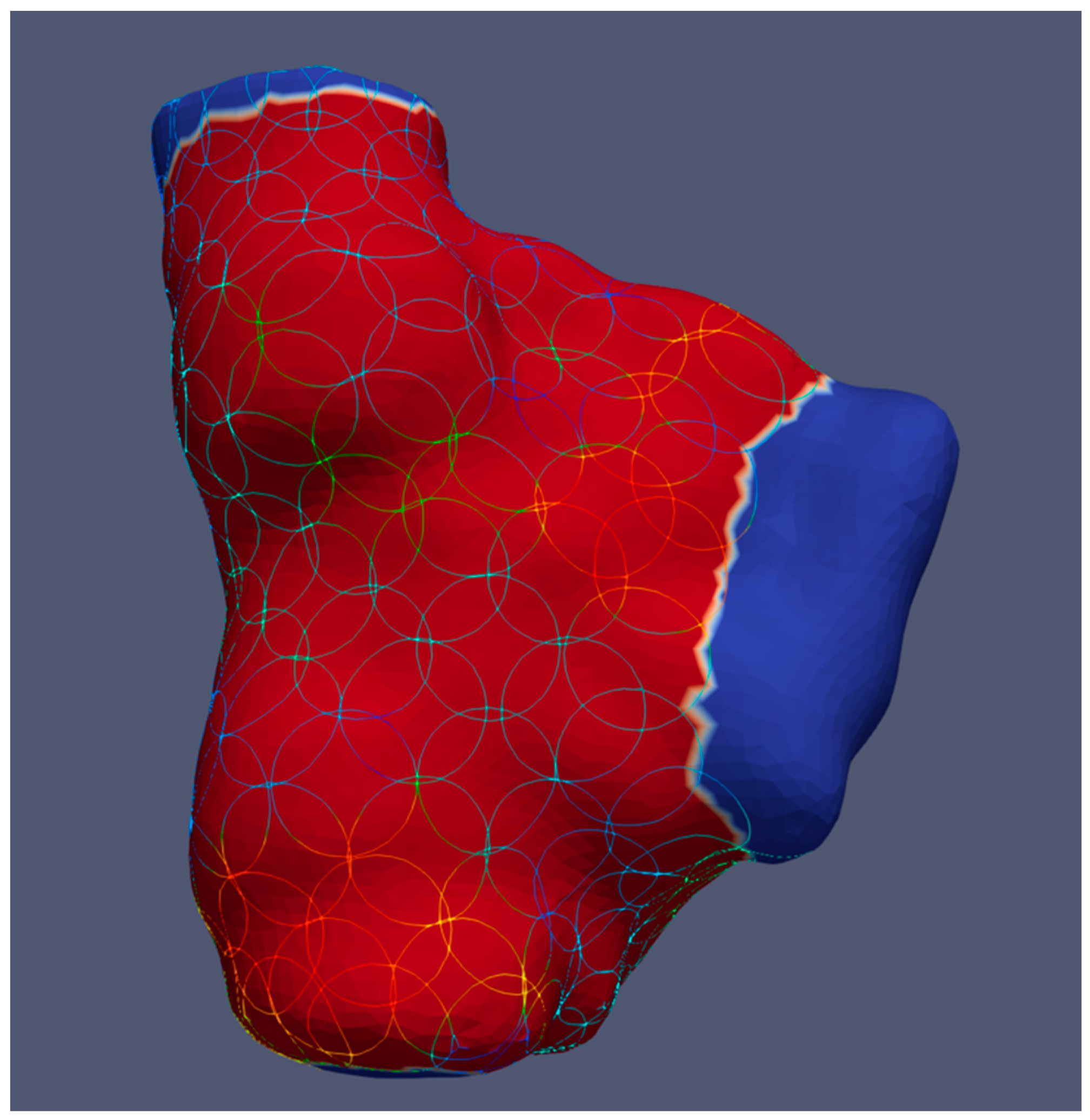
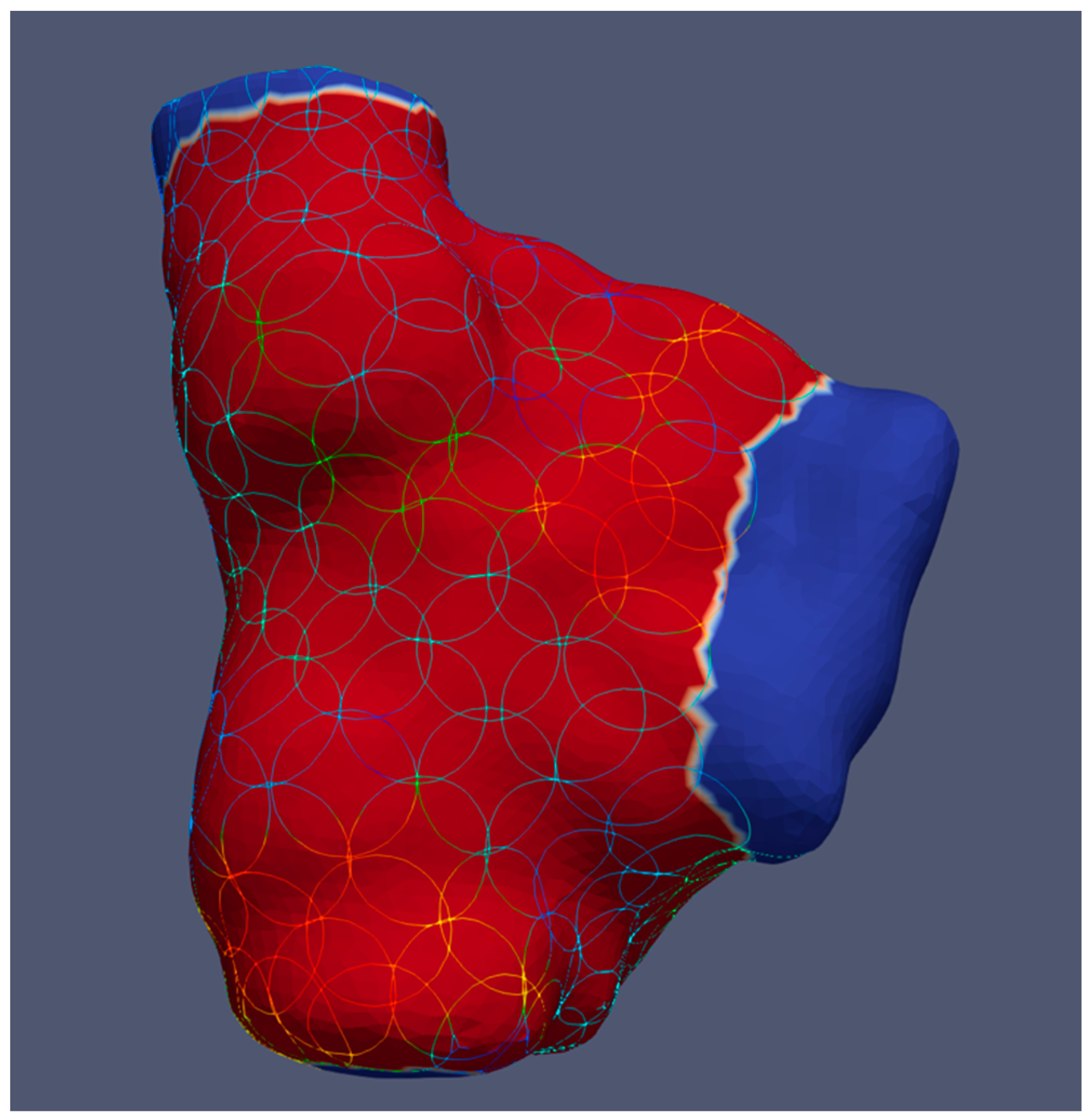
2.3. Calculation of Local Conduction Velocity and Voltage Amplitude
2.4. Statistical Analysis
3. Results
3.1. No Influence of Sex on Conduction Velocity and Voltage Amplitude
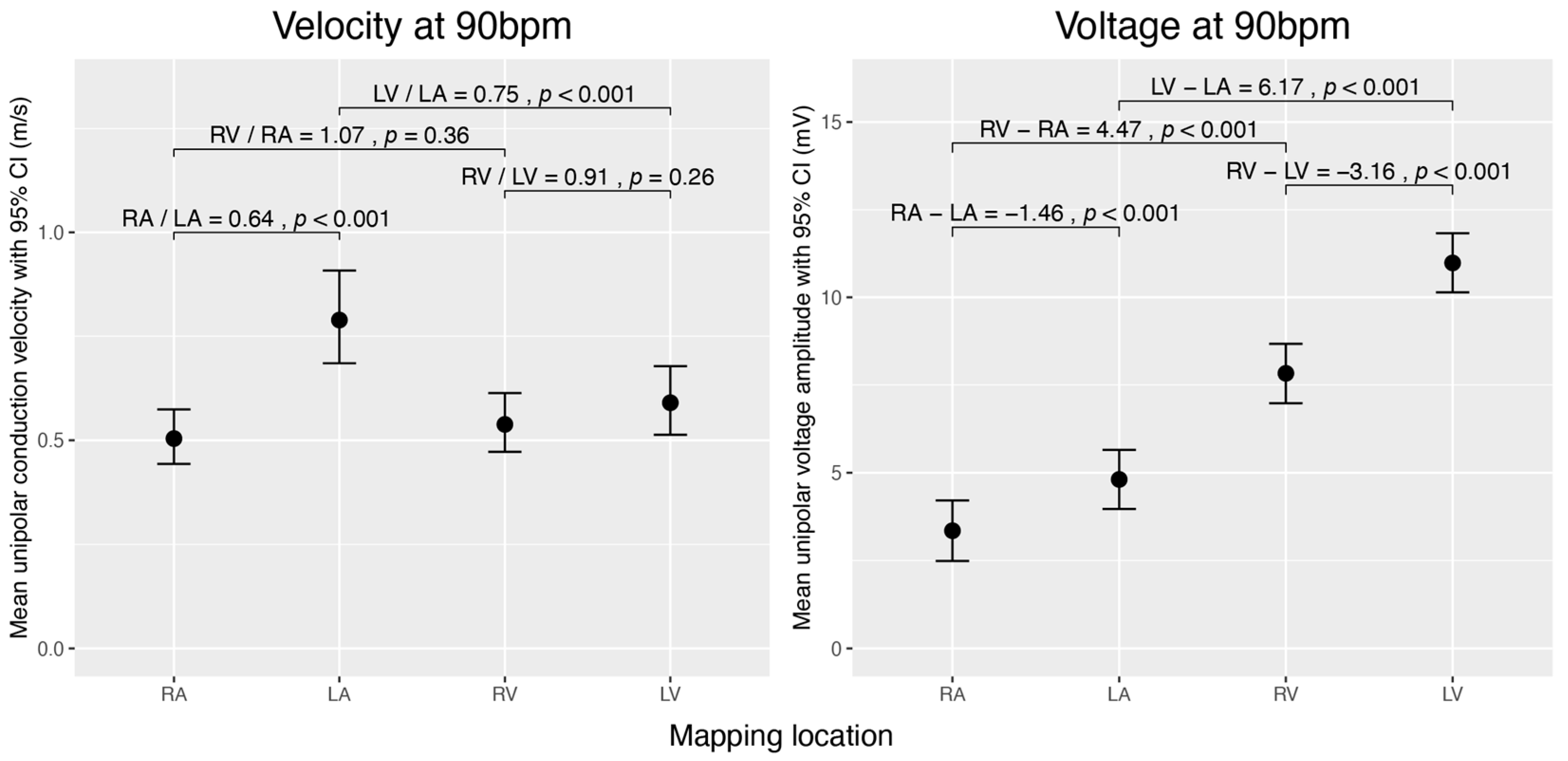
3.2. Mean Velocity and Voltage of Heart Chambers during Sinus Rhythm
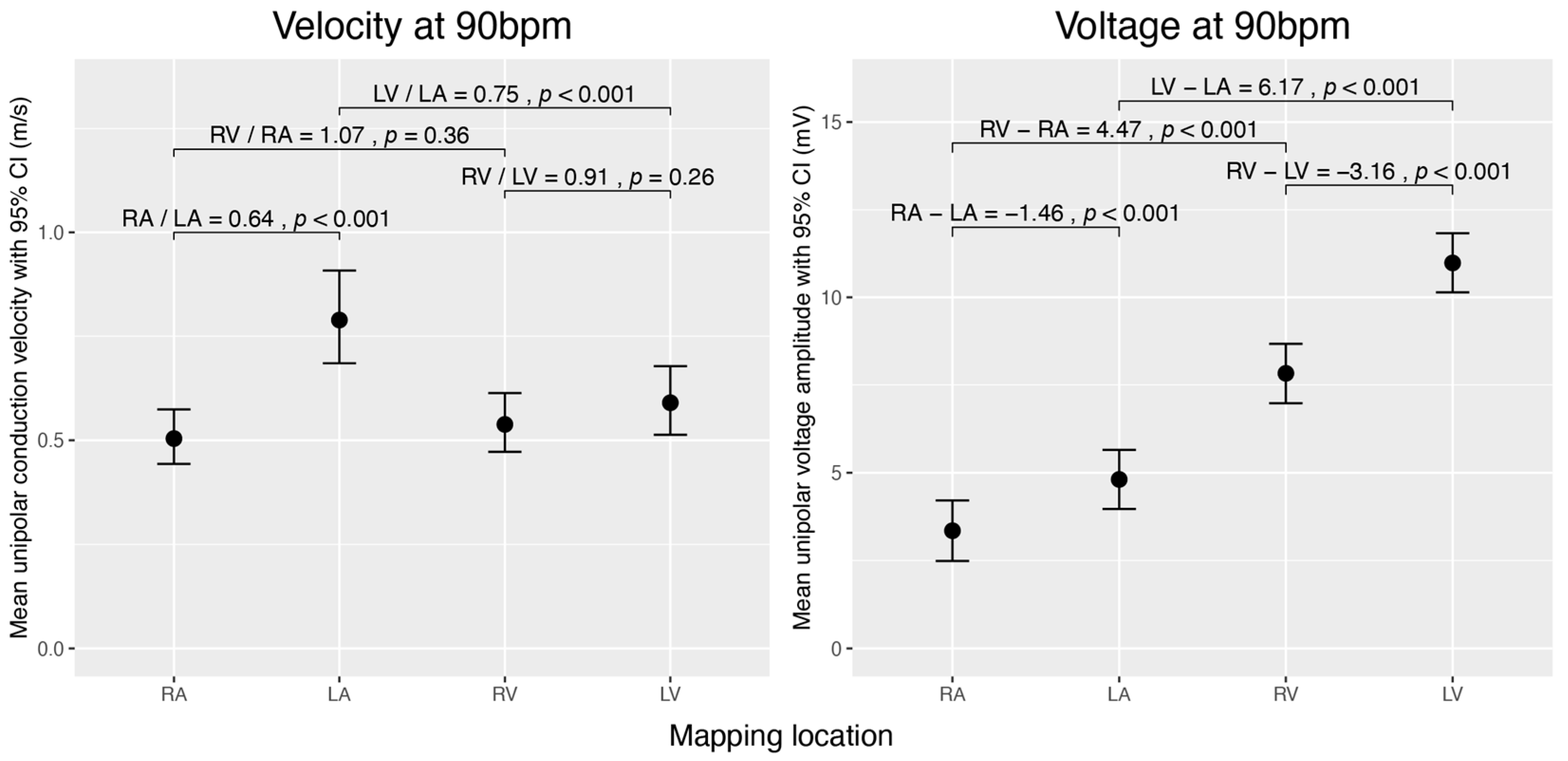
3.3. Velocity and Voltage Differences between Chambers
3.3.1. Inter-Atrial and Inter-Ventricular Comparison
3.3.2. Comparison between Atria and Ventricles of the Left and Right Heart
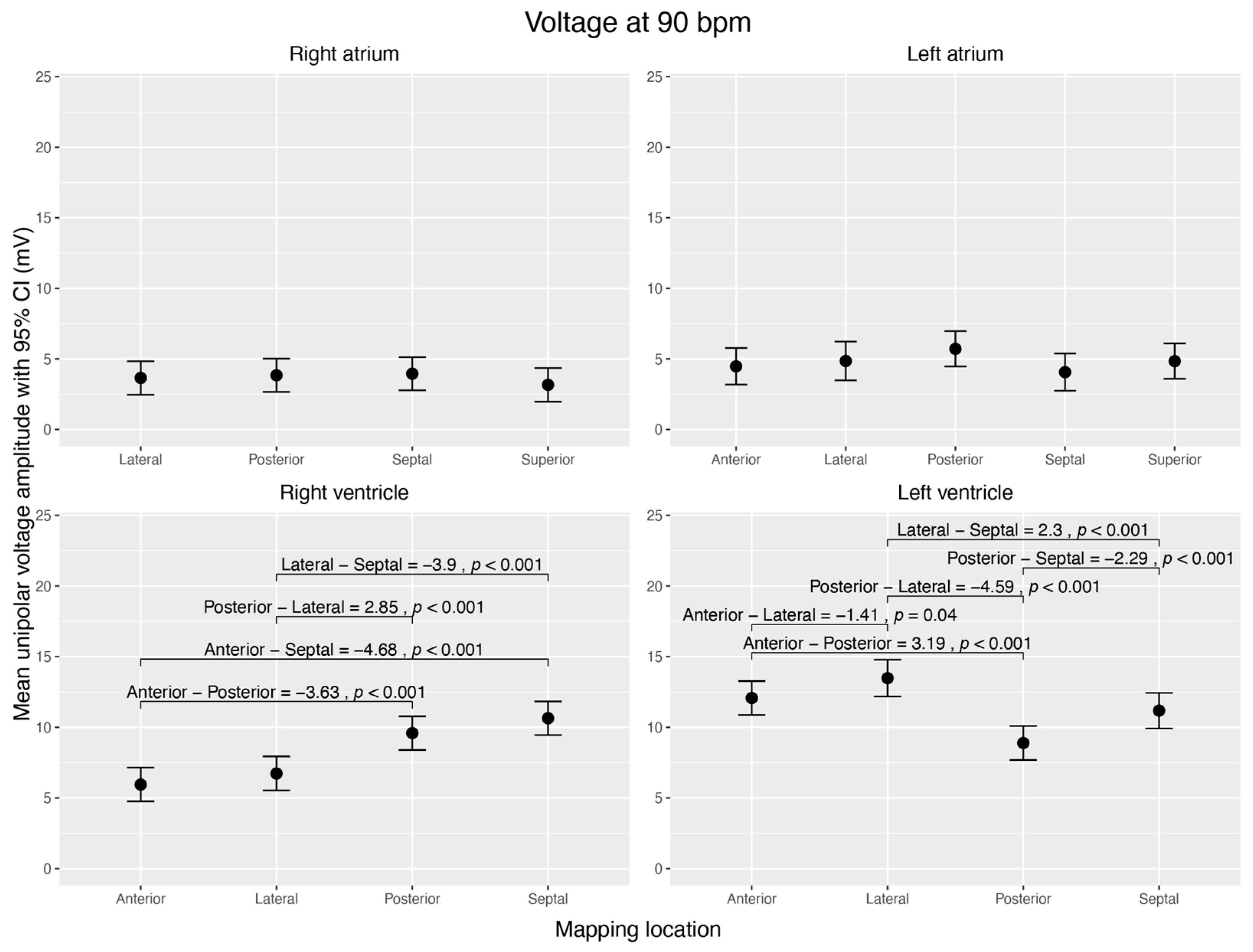
3.4. Regional Velocity and Voltage Characteristics within Each Chamber
3.4.1. Conduction Velocity
3.4.2. Voltage Amplitude
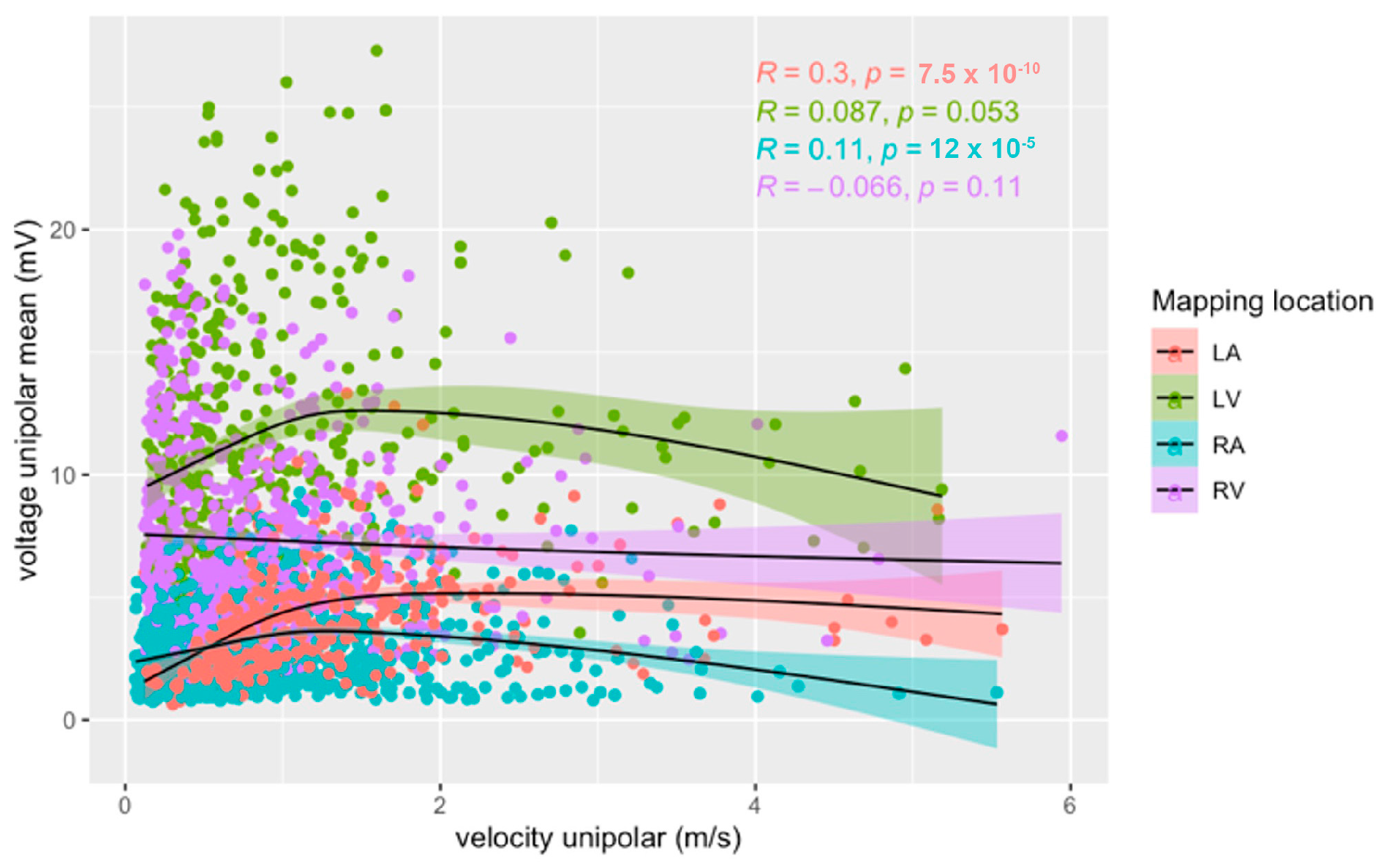
3.5. Correlation of Velocity and Voltage
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Han, B.; Trew, M.L.; Zgierski-Johnston, C.M. Cardiac Conduction Velocity, Remodeling and Arrhythmogenesis. Cells 2021, 10, 2923. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef]
- Shi, R.; Chen, Z.; Butcher, C.; AB Zaman, J.; Boyalla, V.; Wang, Y.K.; Riad, O.; Sathishkumar, A.; Norman, M.; Haldar, S.; et al. Diverse activation patterns during persistent atrial fibrillation by noncontact charge-density mapping of human atrium. J. Arrhythm. 2020, 36, 692–702. [Google Scholar] [CrossRef]
- Jais, P.; Haissaguerre, M.; Shah, D.C.; Chouairi, S.; Clementy, J. Regional Disparities of Endocardial Atrial Activation in Paroxysmal Atrial Fibrillation. Pacing Clin. Electrophysiol. 1996, 19, 1998–2003. [Google Scholar] [CrossRef]
- Martin, R.; Maury, P.; Bisceglia, C.; Wong, T.; Estner, H.; Meyer, C.; Dallet, C.; Martin, C.A.; Shi, R.; Takigawa, M.; et al. Characteristics of Scar-Related Ventricular Tachycardia Circuits Using Ultra-High-Density Mapping. Circ. Arrhythm. Electrophysiol. 2018, 11, e006569. [Google Scholar] [CrossRef]
- Guandalini, G.S.; Liang, J.J.; Marchlinski, F.E. Ventricular Tachycardia Ablation: Past, Present, and Future Perspectives. JACC Clin. Electrophysiol. 2019, 5, 1363–1383. [Google Scholar] [CrossRef]
- Seifert, M.; Erk, J.; Heiderfazel, S.; Georgi, C.; Keil, A.; Butter, C. Impact of mapping points in high-density mapping of the left atrium. J. Interv. Card. Electrophysiol. 2020, 58, 347–353. [Google Scholar] [CrossRef]
- Hansson, A.; Holm, M.; Blomström, P.; Johansson, R.; Lührs, C.; Brandt, J.; Olsson, S. Right atrial free wall conduction velocity and degree of anisotropy in patients with stable sinus rhythm studied during open heart surgery. Eur. Heart J. 1998, 19, 293–300. [Google Scholar] [CrossRef]
- Kleber, A.G.; Janse, M.J.; Wilms-Schopmann, F.J.; Wilde, A.A.; Coronel, R. Changes in conduction velocity during acute ischemia in ventricular myocardium of the isolated porcine heart. Circulation 1986, 73, 189–198. [Google Scholar] [CrossRef]
- Mantziari, L.; Butcher, C.; Kontogeorgis, A.; Panikker, S.; Roy, K.; Markides, V.; Wong, T. Utility of a Novel Rapid High-Resolution Mapping System in the Catheter Ablation of Arrhythmias. JACC Clin. Electrophysiol. 2015, 1, 411–420. [Google Scholar] [CrossRef]
- Ayachit, U. The ParaView Guide: A Parallel Visualization Application; Kitware Inc.: New York, NY, USA, 2015. [Google Scholar]
- Hansen, C.; Johnson, C.R. ParaView: An End-User Tool for Large Data Visualization, Visualization Handbook; Elsevier: Amsterdam, The Netherlands, 2005. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2021. [Google Scholar]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. lme4: Linear Mixed-Effects Models using Eigen and S4. 2022. Available online: https://cran.r-project.org/web/packages/lme4/lme4.pdf (accessed on 20 June 2022).
- Kuznetsova, A.; Bruun Brockhoff, P.; Haubo Bojesen Christensen, R. lmerTest: Tests in Linear Mixed Effects Models. 2020. Available online: https://cran.r-project.org/web/packages/lmerTest/index.html (accessed on 20 June 2022).
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in Linear Mixed Effects Models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef]
- Lenth, R.V. Emmeans: Estimated Marginal Means, Aka Least-Squares Means; CRAN: Iowa-City, IA, USA, 2022. [Google Scholar]
- Kou, S.; Caballero, L.; Dulgheru, R.; Voilliot, D.; De Sousa, C.; Kacharava, G.; Athanassopoulos, G.D.; Barone, D.; Baroni, M.; Cardim, N.; et al. Echocardiographic reference ranges for normal cardiac chamber size: Results from the NORRE study. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 680–690. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, G. The inter-auricular time interval. Am. J. Physiol. 1916, 41, 309–320. [Google Scholar] [CrossRef]
- De Ponti, R.; Ho, S.Y.; Salerno-Uriarte, J.A.; Tritto, M.; Spadacini, G. Electroanatomic Analysis of Sinus Impulse Propagation in Normal Human Atria. J. Cardiovasc. Electrophysiol. 2002, 13, 11–12. [Google Scholar] [CrossRef]
- Latcu, D.G.; Saoudi, N. How Fast Does the Electrical Impulse Travel Within the Myocardium? The Need for a New Clinical Electrophysiology Tool: The Conduction Velocity Mapping. J. Cardiovasc. Electrophysiol. 2014, 25, 395–397. [Google Scholar] [CrossRef]
- Jaïs, P.; Shah, D.C.; Haïssaguerre, M.; Hocini, M.; Peng, J.T.; Takahashi, A.; Garrigue, S.; Le Métayer, P.; Clémenty, J. Mapping and Ablation of Left Atrial Flutters. Circulation 2000, 101, 2928–2934. [Google Scholar] [CrossRef]
- Nairn, D.; Lehrmann, H.; Müller-Edenborn, B.; Schuler, S.; Arentz, T.; Dössel, O.; Jadidi, A.; Loewe, A. Comparison of Unipolar and Bipolar Voltage Mapping for Localization of Left Atrial Arrhythmogenic Substrate in Patients With Atrial Fibrillation. Front. Physiol. 2020, 11, 575846. [Google Scholar] [CrossRef]
- Sanders, P.; Morton, J.B.; Kistler, P.M.; Spence, S.J.; Davidson, N.C.; Hussin, A.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Electrophysiological and electroanatomic characterization of the atria in sinus node disease: Evidence of diffuse atrial remodeling. Circulation 2004, 109, 1514–1522. [Google Scholar] [CrossRef]
- Sanders, P.; Morton, J.B.; Davidson, N.C.; Spence, S.J.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Electrical remodeling of the atria in congestive heart failure: Electrophysiological and electroanatomic mapping in humans. Circulation 2003, 108, 1461–1468. [Google Scholar] [CrossRef]
- Glashan, C.A.; Tofig, B.J.; Beukers, H.; Tao, Q.; Blom, S.A.; Villadsen, P.R.; Lassen, T.R.; de Riva, M.; Kristiansen, S.B.; Zeppenfeld, K. Multielectrode Unipolar Voltage Mapping and Electrogram Morphology to Identify Post-Infarct Scar Geometry. JACC Clin. Electrophysiol. 2022, 8, 437–449. [Google Scholar] [CrossRef]
- van Schie, M.S.; Heida, A.; Taverne, Y.J.H.J.; Bogers, A.J.J.C.; de Groot, N.M.S. Identification of local atrial conduction heterogeneities using high-density conduction velocity estimation. EP Eur. 2021, 23, 1815–1825. [Google Scholar] [CrossRef] [PubMed]
- Milani-Nejad, N.; Janssen, P.M.L. Small and large animal models in cardiac contraction research: Advantages and disadvantages. Pharmacol. Ther. 2014, 141, 235–249. [Google Scholar] [CrossRef] [PubMed]
- Maceira, A.M.; Cosín-Sales, J.; Roughton, M.; Prasad, S.K.; Pennell, D.J. Reference right atrial dimensions and volume estimation by steady state free precession cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2013, 15, 29. [Google Scholar] [CrossRef]
- Khan, F.; Banchs, J.E.; Skibba, J.B.; Grando-Ting, J.; Kelleman, J.; Singh, H.; Gonzalez, M.D. Determination of left atrium volume by fast anatomical mapping and intracardiac echocardiography. The contribution of respiratory gating. J. Interv. Card. Electrophysiol. 2015, 42, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, S.; Zhu, Q.; Wang, Y.; Li, G.; Kong, F.; Yang, J. Reference values of right ventricular volumes and ejection fraction by three-dimensional echocardiography in adults: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2021, 8, 709863. [Google Scholar] [CrossRef]
- Clay, S.; Alfakih, K.; Radjenovic, A.; Jones, T.; Ridgway, J.P. Normal Range of Human Left Ventricular Volumes and Mass Using Steady State Free Precession MRI in the Radial Long Axis Orientation. Magn. Reson. Mater. Phys. Biol. Med. 2006, 19, 41–45. [Google Scholar] [CrossRef]
- Hirata, N.; Kanaya, N.; Kamada, N.; Kimura, S.; Namiki, A. Differential effects of propofol and sevoflurane on ischemia-induced ventricular arrhythmias and phosphorylated connexin 43 protein in rats. Anesthesiology 2009, 110, 50–57. [Google Scholar] [CrossRef]
- Liu, Q.; Kong, A.L.; Chen, R.; Qian, C.; Liu, S.W.; Sun, B.G.; Wang, L.X.; Song, L.S.; Hong, J. Propofol and arrhythmias: Two sides of the coin. Acta Pharmacol. Sin. 2011, 32, 817–823. [Google Scholar] [CrossRef]
- Aya, A.G.; Robert, E.; Bruelle, P.; Lefrant, J.Y.; Juan, J.M.; Peray, P.; Eledjam, J.J.; de La Coussaye, J.E. Effects of ketamine on ventricular conduction, refractoriness, and wavelength: Potential antiarrhythmic effects: A high-resolution epicardial mapping in rabbit hearts. Anesthesiology 1997, 87, 1417–1427. [Google Scholar] [CrossRef]
- Wutzler, A.; Huemer, M.; Boldt, L.-H.; Parwani, A.S.; Attanasio, P.; Tscholl, V.; Haverkamp, W. Effects of deep sedation on cardiac electrophysiology in patients undergoing radiofrequency ablation of supraventricular tachycardia: Impact of propofol and ketamine. EP Eur. 2013, 15, 1019–1024. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pig | Map-Nr. | Mapping Location | Heart Rate | Nr. of Points | Volume (mL) | Nr. of Circles Whole Map | Lateral Circles | Septal Circles | Posterior Circles | Anterior Circles | Superior Circles |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | RA | 115 | 6839 | 77.65 | 184 | 30 | 23 | 26 | - | 9 |
| 1 | 4 | RA | 115 | 6907 | 77.65 | 184 | 30 | 23 | 26 | - | 9 |
| 1 | 5 | LV | 122 | 4806 | 53.16 | 122 | 10 | 14 | 20 | 21 | - |
| 1 | 9 | LV | 130 | 4726 | 53.16 | 122 | 10 | 14 | 20 | 21 | - |
| 2 | 10 | RA | 120 | 7475 | 69.66 | 167 | 21 | 17 | 16 | - | 11 |
| 2 | 12 | RA | 134 | 7475 | 69.66 | 167 | 21 | 17 | 16 | - | 11 |
| 2 | 14 | LV | 120 | 5060 | 50.10 | 129 | 11 | 13 | 26 | 24 | - |
| 2 | 16 | LV | 86 | 5060 | 50.10 | 129 | 11 | 13 | 26 | 24 | - |
| 2 | 18 | LA | 86 | 4835 | 39.95 | 100 | 11 | 10 | 16 | 12 | 15 |
| 2 | 20 | LA | 90 | 4964 | 40.68 | 100 | 11 | 10 | 16 | 12 | 15 |
| 2 | 21 | RV | 104 | 6440 | 68.88 | 138 | 12 | 16 | 17 | 21 | - |
| 2 | 23 | RV | 95 | 6445 | 68.64 | 138 | 12 | 16 | 17 | 21 | - |
| 3 | 25 | RA | 130 | 7815 | 81.00 | 193 | 30 | 35 | 33 | - | 10 |
| 3 | 26 | RV | 135 | 3547 | 33.95 | 74 | 9 | 13 | 9 | 14 | - |
| 3 | 32 | RV | 150 | 4698 | 35.82 | 66 | 10 | 9 | 6 | 6 | - |
| 5 | 36 | RA | 95 | 6848 | 64.54 | 176 | 41 | 21 | 21 | - | 13 |
| 5 | 37 | RV | 110 | 3158 | 25.93 | 84 | 12 | 15 | 16 | 9 | - |
| 5 | 39 | RA | 145 | 6799 | 69.00 | 186 | 45 | 32 | 26 | - | 24 |
| 5 | 42 | RV | 132 | 3420 | 28.04 | 84 | 12 | 15 | 16 | 9 | - |
| 5 | 44 | LA | 145 | 5481 | 40.70 | 105 | 4 | 9 | 10 | 9 | 11 |
| 5 | 45 | LA | 171 | 5481 | 40.70 | 105 | 4 | 9 | 10 | 9 | 11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilhelm, T.I.; Lewalter, T.; Fischer, J.; Reiser, J.; Werner, J.; Baumgartner, C.; Gleirscher, L.; Hoppmann, P.; Kupatt, C.; Tiemann, K.; et al. Electroanatomical Conduction Characteristics of Pig Myocardial Tissue Derived from High-Density Mapping. J. Clin. Med. 2023, 12, 5598. https://doi.org/10.3390/jcm12175598
Wilhelm TI, Lewalter T, Fischer J, Reiser J, Werner J, Baumgartner C, Gleirscher L, Hoppmann P, Kupatt C, Tiemann K, et al. Electroanatomical Conduction Characteristics of Pig Myocardial Tissue Derived from High-Density Mapping. Journal of Clinical Medicine. 2023; 12(17):5598. https://doi.org/10.3390/jcm12175598
Chicago/Turabian StyleWilhelm, Theresa Isabelle, Thorsten Lewalter, Johannes Fischer, Judith Reiser, Julia Werner, Christine Baumgartner, Lukas Gleirscher, Petra Hoppmann, Christian Kupatt, Klaus Tiemann, and et al. 2023. "Electroanatomical Conduction Characteristics of Pig Myocardial Tissue Derived from High-Density Mapping" Journal of Clinical Medicine 12, no. 17: 5598. https://doi.org/10.3390/jcm12175598
APA StyleWilhelm, T. I., Lewalter, T., Fischer, J., Reiser, J., Werner, J., Baumgartner, C., Gleirscher, L., Hoppmann, P., Kupatt, C., Tiemann, K., & Jilek, C. (2023). Electroanatomical Conduction Characteristics of Pig Myocardial Tissue Derived from High-Density Mapping. Journal of Clinical Medicine, 12(17), 5598. https://doi.org/10.3390/jcm12175598