Abstract
Immunosuppressants and antifibrotics are currently used to treat patients with various interstitial lung diseases, which may undergo lung transplantation (LTx). The retrospective study aimed to evaluate the potential effects of therapeutic regimen on the perioperative course in patients with idiopathic pulmonary fibrosis (IPF) or progressive pulmonary fibrosis (PPF) undergoing LTx. All patients with IPF and PPF undergoing LTx between January 2014 and December 2021 were included. We retrospectively screened for previous use of immunosuppressants and antifibrotic therapy. We analyzed perioperative courses, short-term outcomes, and safety retrospectively. In total, 286 patients with diagnosis of IPF or PPF were analyzed. According to the treatment regimen before LTx, the study cohort was divided into four groups and compared. No differences between antifibrotic monotherapy, combined antifibrotic and immunosuppressive therapy with regard to postoperative complications were observed. Length of mechanical ventilation was shorter in patients with antifibrotics prior to LTx. Pretreatment with antifibrotic monotherapy and a combination of antifibrotic drugs with immunosuppressive therapy, lower body mass index (BMI) and lower blood loss, were independently associated with primary graft dysfunction grades 0–3 72 hours after LTx (p < 0.001). Finally, patients with antifibrotic monotherapy developed significantly less de novo donor-specific antibodies (DSA) (p = 0.009). Higher intraoperative blood loss, etiology of interstitial lung disease (ILD) and older age were independently associated with shorter survival after LTx. Use of antifibrotic monotherapy and a combination of antifibrotic drugs with immunosuppressive therapy in IPF/PPF patients undergoing LTx, proved to be safe and might lead to beneficial effects after LTx.
1. Introduction
Progressive pulmonary fibrosis (PPF) and idiopathic pulmonary fibrosis (IPF) are associated with irreversible loss of lung function and major reductions in quality of life and survival regardless of the underlying condition [1,2,3]. Therefore, for selected patients, lung transplantation can be offered as the last treatment option after failure of medical therapy in severe ILD.
Survival after lung transplantation is limited by non-allograft-related and allograft-related factors. The major challenge in the postoperative phase is to gain control of immunological reactions and to reduce ischemia-reperfusion injury. Those factors can contribute to acute systemic inflammation, alter the transplanted lungs and lead to primary graft dysfunction (PGD) and thus to prolonged ventilation and adverse outcomes [4].
Recently, the treatment landscape for fibrotic lung diseases has changed after randomized trials demonstrated clinical efficacy of antifibrotic therapy in patients with PPF. Furthermore, two antifibrotic medications, pirfenidone, and nintedanib, first approved for idiopathic pulmonary fibrosis (IPF), have shown consistent effects on lung function decline in several diseases of non-IPF-patients [5,6,7,8]. Therefore, a new treatment pathway for PPF is provided, and combined antifibrotic and immunosuppressant drug therapy has become a relevant treatment option [3].
Still, experience with patients undergoing lung transplantation (LTx) with prior treatment of immunosuppressants, antifibrotics or a combination of both is scarce. Most data are limited to patients pretreated with prednisolone monotherapy or IPF patients pretreated with antifibrotics [9,10,11,12,13,14,15].
This study aimed to evaluate the potential effects of different treatment regimens on post-transplant outcomes and immunology in patients with IPF and PPF after LTx in a retrospective cohort.
2. Methods
2.1. Study Cohort and Design
All transplant candidates with IPF and PPF who underwent LTx from January 2014 until December 2021 were included in the study and analyzed retrospectively. The time point was chosen since, in 2014, nintedanib, the second antifibrotic drug, was approved for IPF. The study was performed at the University of Munich, Germany, and approved by the local ethics committee (UE No. 646-16).
Individuals with a consensus diagnosis of ILD such as IPF, fibrotic hypersensitivity pneumonitis (HP), non-specific interstitial pneumonia (NSIP), autoimmune ILDs such as rheumatoid arthritis-associated ILD, SSc-ILD, mixed connective tissues disease-associated ILD, rare ILDs and unclassified pulmonary fibrosis (uILD) were included. All diagnoses were made in accordance with the current international criteria [16,17,18,19,20]. Diagnosis was verified by histological examination of explanted lungs.
Local databases and medical records were screened for therapy with antifibrotic medication and/or immunosuppression prior to transplantation. The study population was divided into 4 groups according to the treatment regimen prior to LTx: antifibrotic monotherapy (nintedanib or pirfenidone); combination therapy of antifibrotic drugs with immunosuppression; immunosuppressive treatment; and without specific medication. Antifibrotics were applied until at least one week prior to transplantation. Treatment with nintedanib or pirfenidone was not continued after LTx. Immunosuppressive drugs included corticosteroids, azathioprine, mycophenolate mofetil or methotrexate. If indicated, immunosuppressive medication was continued until transplantation. After LTx, all patients received standard immunosuppressive triple therapy including corticosteroids, mycophenolate mofetil and calcineurin inhibitors. [13].
All patients were screened to identify important comorbidities and contraindications before transplantation. To assess the severity of disease, we performed the lung allocation score (LAS) score, gender-age-physiology-ILD-index (GAP-ILD), lung function analysis including blood gas analysis, spirometry, plethysmography and 6-min walking distance (6MWD) according to the German LAS business rules [21]. Baseline characteristics were collected at the time of entering the waiting list.
2.2. Short- and Long-Term Outcomes
We used Narkodata (online-documentation system, Imeso GmbH, Giessen, Germany) to collect perioperative data, including the procedure duration, blood loss and use of extracorporeal membrane oxygenation therapy (ECMO). Further postoperative data included length of intensive care unit (ICU) stay, hours of mechanical ventilation, primary graft dysfunction (PGD), need of reintubation and revision surgeries. We defined revision surgeries as surgery during hospital stay due to postoperative bleeding, wound infection or healing disorder.
PGD was assessed at 72 h after LTx (defined as T72) according to the ISHLT guidelines. PGD was classified into three grades (grade 1 > 300 PaO2/FiO2; grade 2 200 to 300 PaO2/FiO2; grade 3 < 200 PaO2/FiO2) based on the ratio of partial pressure of oxygen (PaO2)/fraction of inspired oxygen (FiO2). Absence of pulmonary edema on chest radiograph of the transplanted lung was defined as grade 0. Any patient using a nasal cannula for oxygen or Venturi mask was graded as 0 or 1, as described previously [13]. Any patient receiving extracorporeal membrane oxygenation or mechanically ventilated with an FiO2 of greater than 0.5 on nitric oxide beyond 72 h after transplantation was considered grade 3 [22].
Transbronchial lung biopsies (TBB) and screening for human leukocyte antigen (HLA)-antibodies against HLA class I and II (Luminex, Life Screen Deluxe, Gen-Probe, USA) were routinely performed within 30 days after LTx and if clinically indicated. TBB were classified as A0 to A4 according to International Society of Heart and Lung Transplantation (ISHLT) guidelines [23,24]. Bronchoalveolar lavage (BAL) was performed after 3, 6 and 12 months if clinically indicated [25]. Additionally, mortality after LTx was recorded during the follow up of at least one year after LTx. Causes of death in the study cohort were assessed based on medical records.
2.3. Statistical Analysis
Continuous variables are presented as the mean ± standard deviation (SD), with categorical variables summarized by frequency and percentage. Analysis of variance (ANOVA) was used to compare continuous variables; significant differences identified on preliminary testing between the groups were analyzed separately by post hoc pairwise comparisons using Tukey’s honest significant difference test. Fisher’s exact test was used to compare categorical variables.
To identify possible associations of certain variables on outcome parameters we first used univariate analysis to compare the distribution of variables between groups. Second, we performed logistic regression analysis to model multivariate associations of possible predictors. Predictors for the regression models were selected with regard to significance in the univariate analysis and under consideration of the rules regarding overfitting and multicollinearity. In addition, multivariate cox regression analysis was used to evaluate the impact of different variables on survival over the entire follow-up. p < 0.05 was considered statistically significant. Data were statistically analyzed by SPSS version 24.0 (IBM SPSS, Armonk, NY, USA) statistical software.
3. Results
3.1. Study Cohort and Baseline Characteristics
A total of 563 lung transplantations were performed during the study period. Thereof, 286 patients (50.8%) had an underlying diagnosis of end-stage ILD, including 170 lung transplant recipients with PPF (59.4%) and 116 patients with IPF (40.6%). The study cohort was divided into four groups as depicted in Figure 1—“antifibrotic monotherapy” (n = 82), “combination of antifibrotic drugs with immunosuppressive therapy” (n = 33), “immunosuppressive treatment” (n = 147) and “without specific treatment” (n = 24)—and analyzed. In the two groups with antifibrotic pretreatment, 108 patients (95.9%) took nintedanib or pirfenidone on the day of transplantation, whereas requirement of mechanical ventilation and/or ECMO therapy after ICU admission led to discontinuation of antifibrotic therapy in 7 patients (6.1%) two to seven days before surgery. In the immunosuppressive treatment group, 17 LTx recipients (5.9%) had previously received antifibrotic agents (13 pirfenidone only, 3 nintedanib only, 1 both). In these cases, antifibrotic medication was stopped due to progression of disease or side effects with a minimum of 2.5 months before transplantation. A detailed overview of the concomitant immunosuppressive therapy prior to LTx is shown in the supplementary material (Table S1). The most common therapy among the study cohort (28.0%) was pretreatment with corticosteroid monotherapy at a median dose of 5 mg/day (2.5–70 mg/day).
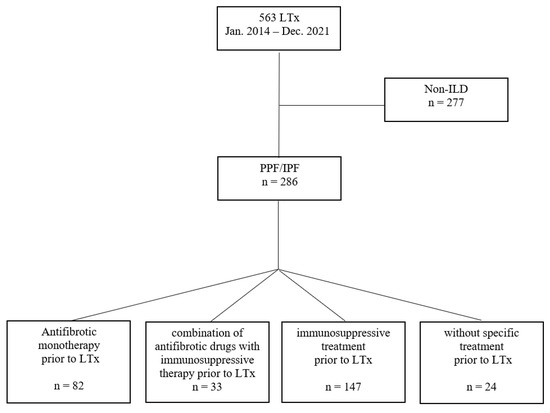
Figure 1.
Description of the study cohort and classification. IPF: idiopathic pulmonary fibrosis; LTx: lung transplantation; PPF: progressive pulmonary fibrosis.
Characteristics of the study cohort, severity of disease and last LAS are demonstrated in Table 1. At the time of LTx, the groups with antifibrotic pretreatment were significantly older and had larger amounts of male patients and past smokers, as well as a higher proportion of IPF as the underlying disease than the immunosuppressive group. Severity of disease did not differ between the study groups. However, comorbidities assessed during transplant evaluation showed a higher prevalence of coronary artery disease (CAD) with a history of revascularization (22.0% vs. 3.0% vs. 8.2% vs. 8.3%, p = 0.007) in the group with antifibrotic monotherapy before LTx (Table S2).

Table 1.
Baseline characteristics of patients with end-stage ILD undergoing LTX at the time of entering the waiting list.
3.2. Perioperative Course, ICU Parameters and Surgery-Related Complications
Acute respiratory worsening led to ICU admission with the need for mechanical ventilation in 15 patients (5.2%) and veno-venous ECMO therapy in 22 patients (7.7%) before LTx, respectively. No significant differences were observed between the groups (Table 2). Intraoperatively, the number of patients supported by venovenous or venoarterial ECMO was similar (4.9% vs. 3.1% vs. 10.3% vs. 12.5%, p = 0.301 and 51.2% vs. 56.3% vs. 58.2% vs. 50.0%, p = 0.718; respectively) as shown in Table 2. Intraoperative blood loss was increased in the study groups with immunosuppressive treatment or without any specific treatment prior to LTx (2105.7 ± 1409.7 mL vs. 2481.8 ± 1432.5 mL vs. 3238.6 ± 2532.2 vs. 3687.5 ± 2758.9 mL, p < 0.001). Operation time was not statistically different between the groups. Most of the patients (70.6%) could be successfully weaned from intraoperative ECMO therapy. In total, 37 patients (13.0%) received vv-ECMO, and 16 patients received va-ECMO (5.6%), respectively.
Table 2.
Perioperative course, lung donor parameters, ICU parameters and surgery-related complications of patients with PPF and IPF undergoing LTx.
Furthermore, revision surgery, pneumothoraces and anastomotic complications were similar in patients with different pretreatments, as depicted in Table 2. Length of mechanical ventilation was shorter (59.1 h vs. 57.4 h vs. 98.0 h vs. 69.3 h, p = 0.019), and severity of PGD at 72 h after transplantation was lower in the groups pretreated with antifibrotic drugs (0.9 ± 0.9 vs. 0.8 ± 0.1 vs. 1.5 ± 1.1 vs. 1.7 ± 1.0, p < 0.001). Seventy-two hours after transplantation, PGD grade 3 was more frequent in the groups with immunosuppressive or no specific treatment before LTx (7.5% vs. 3% vs. 26.4% vs. 29.2%, p < 0.001) (Table 2). There was no difference regarding the rate of reintubation and the use of inhaled nitric oxide between the groups. Additionally, length of ICU stay was shorter (18.1 ± 42.0 vs. 14.0 ± 14.7 vs. 25.6 ± 34.0 vs. 25.6 ± 26.4, p = 0.196) in the group with the combination of antifibrotic drugs and immunosuppressive therapy.
Univariate and multivariate regression analysis was performed to take a deeper view into the diversity of treatment options prior to LTx and to identify the associations of certain variables on post-transplant outcome parameters (Table 3). Pretreatment with antifibrotic therapy, combination of antifibrotic drugs with immunosuppression, lower BMI and less intraoperative blood loss independently correlated with improved primary graft function after 72 h after LTx in multivariate regression analysis (p < 0.001) (Table 3).
Table 3.
Univariate regression (UR, Pearson correlation, coefficient r) and multivariate linear regression (MLR, coefficient beta) analysis factors associated with grade of PGD after 72 h.
3.3. Pre-Transplant Treatment and Outcome
Two patients (1.8%) in the immunosuppressive treatment group and one patient each in the groups with antifibrotic pretreatment (1.9%) received induction therapy with ATG. The number of patients with one or more episodes of acute cellular rejection (≥A1) within 30 days after transplantation was lower after treatment with antifibrotics (7.7% vs. 15.6% vs. 13.8% vs. 31.6%, p = 0.057) (Table 4). The prevalence of de novo donor-specific HLA-antibodies (DSA) within 30 days after transplantation was significantly higher in the groups without antifibrotic pretreatment (12.5% vs. 15.2% vs. 29.6% vs. 34.8%, p = 0.009). Pretreatment with antifibrotic monotherapy (p = 0.034; Coeff. ß: −0.227) was independently associated with lower risk for development of DSA within the first year after LTx while controlling for age, sex, BMI, pre- or postoperative ECMO therapy, etiology of ILD (IPF vs. Non-IPF), CTD-ILD, pulmonary arterial pressure, time from diagnosis to LTx, prednisolone dose > 5 mg, absence of specific treatment prior to LTx, combination of antifibrotic drugs and immunosuppressive therapy, intraoperative blood loss and LAS in regression analysis (p = 0.047).
Table 4.
Immunology and survival of patients with PPF and IPF undergoing LTX.
Analysis of BAL assessed within the first year after LTx regarding neutrophilia was similar between the groups (Table 4).
During the first year after LTx 24 patients (8.4%) died (antifibrotic monotherapy 7.3%, combination of antifibrotic drugs with immunosuppressive therapy 3.0%, immunosuppressive treatment 10.9% and without specific treatment 4.2%; p = 0.516). The most common causes of death were septic shock and multiple-organ failure (n = 11), myocardial infarction or cardiogenic shock (n = 5) and COVID-19 pneumonia (n = 2). Other causes of death were primary transplant failure (n = 2), adenocarcinoma (n = 1), ischemic stroke (n = 1), pneumonia in CLAD (n = 1) and invasive aspergillosis (n = 1). None of the patients with combined antifibrotic and immunosuppressant drug therapy and in the group without specific treatment prior to LTx died during ICU stay. The overall survival rates for the study cohort were 97.9% at one month, 97.2% at six months and 91.6% at 12 months, respectively. Long-term survival over the entire study period, calculated using Kaplan–Meier estimates, showed no significant difference between the 4 treatment groups (p = 0.690) (Figure S1).
Intraoperative blood loss (Odd ratio 1.000, CI 1.000-1.000; p = 0.006), etiology of ILD (IPF vs. PFF) (Odd ratio 3.152, CI 1.463–6.790; p = 0.003), age (Odd ratio 1.072, CI 1.022–1.124; p = 0.004) and LAS score (Odd ratio 1.032, CI 1.010–1.054; p = 0.004) were associated with shorter survival. Still, no significant differences between pretransplant treatment regimens were revealed according to cox regression analysis (Table 5).
Table 5.
COX regression analysis (death 0, survival 1) during the study period with at least one year follow-up.
4. Discussion
Recently, the treatment landscape for the entire field of fibrotic lung diseases has changed after randomized trials demonstrated clinical efficacy of antifibrotic therapy in patients with IPF and PPF [3,5,6,7,8]. As a result, the therapeutic options for ILD patients prior to lung transplantation are constantly increasing. Our cohort study includes a large cohort of ILD patients with various immunomodulatory and antifibrotic therapies.
Except for prednisolone, there are no data on the impact of immunomodulating agents on LTx outcomes in patients with PPF. Prior studies showed that high dose of prednisolone therapy before transplantation might contribute to marked wound healing disorder, anastomotic dehiscence and mortality [14,15]. While the tolerable dose of prednisolone appears to be below 0.30–0.42 mg·kg−1·day−1, most centers consider a maintenance dose of <20 mg as eligible for LTX [14]. Interestingly, according to our data pretreatment with prednisolone (daily dose <10 mg) has no significant impact on PGD after 72 h and survival after LTX in regression analysis.
The effects of treatment with other immunosuppressive agents prior to LTX on lung transplantation outcomes are not well studied. In contrast to earlier studies, we included azathioprine, methotrexate and mycophenolate mofetil used to treat PPF. According to our data, anastomotic complications and operative revision weren’t significantly increased in patients pretreated with immunosuppressive medication. Compared to the other subgroups, patients with immunosuppressive therapy prior to LTx developed significantly more HLA-antibodies one month after LTX and longer duration of mechanical ventilation. These findings might be explained by the pathomechanisms of diseases with autoimmune features.
Previous therapy with the antifibrotic drugs may potentially interfere with immunological reactions and perioperative complications in ILD patients undergoing LTx.
In our cohort study, 40.2% of the lung transplant candidates received antifibrotic medication. In addition, 95.9% of the study cohort with previous antifibrotic treatment have taken nintedanib or pirfenidone until at least one week before transplantation, indicating a good adherence of antifibrotics in patients with end-stage ILD.
Nintedanib and pirfenidone attenuate fibroblast activity and inhibit myofibroblast differentiation and potentially angiogenesis. Therefore, the administration of antifibrotic drugs prior to LTx may theoretically lead to an increased risk of bronchial anastomotic complications, bleeding, and impaired wound healing [11,26]. However, experiences with ILD patients undergoing LTx are mostly limited to data in IPF patients, where antifibrotic drugs were used as monotherapies [9,10,11,12,13]. In line with previous studies of patients with IPF undergoing LTx with antifibrotic drugs our data support that antifibrotics as well as combined antifibrotic and immunosuppressant drug therapy is safe in patients with PPF and IPF listed for lung transplantation [9,10,11,12,13]. This is of interest since nintedanib and pirfenidone might reduce acute exacerbations in PPF and attenuate further disease progression [8,27].
Furthermore, beneficial effects of pretreatment with antifibrotics and combination of antifibrotics with immunosuppressive drugs were observed. In both subgroups, the length of mechanical ventilation was shorter. In addition, occurrence of PGD was significantly decreased in patients with lower BMI, reduced intraoperative blood loss and pretreatment with antifibrotic monotherapy as well as combination of antifibrotic drugs and immunosuppressive therapy according to multivariate regression analysis. This is of interest since several risk factors for the development of severe PGD have been described. PGD is presumed to be a consequence of ischemia-reperfusion injury as well as inflammatory events [28,29]. Nintedanib exerts a potent inhibitory activity on the proliferation and migration of lung fibroblasts mainly through the downstream of growth factors, whereas pirfenidone inhibits inflammatory responses mainly through suppression of tumor necrosis factor (TNF)-α, an early mediator of inflammation [30]. In addition, nintedanib has also shown anti-inflammatory effects in various experimental and clinical settings [31,32,33,34]. The described pleiotropic properties of antifibrotics might potentially lead to less deterioration of pulmonary function in the posttransplant period by suppressing acute inflammation in lung ischemia-reperfusion injury, the main cause of PGD.
Interestingly, the patients of our study cohort pretreated with antifibrotics developed significantly less de novo DSA and tended to have reduced occurrence of acute cellular rejections within 30 days after LTX after applying multivariate regression analysis for various variables. Nintedanib and pirfenidone block T-cell activation, which are important regulators of rejection, inhibit the release of cytokines and reduce neutrophil chemotaxis, indicating important graft protective effects [32,33,35,36]. In addition, pirfenidone treatment results in reduced germinal center B cells and T-follicular helper cell frequencies [37]. However, it is hypothesized that due to the short half-lives of antifibrotic agents the potential perioperative harmful effects are reduced, but also attenuate long-term beneficial immunomodulatory effects [9].
So far, no data regarding the effects of antifibrotics as well as combined antifibrotic and immunosuppressant drug therapy in patients with end-stage ILD undergoing LTx are available. Prior studies mainly focused on patients with IPF [10,11,12]. The results of our study should be interpreted with caution and in view of the study design and its limitations, which include a retrospective, single-center setting and a heterogeneous group of end-stage lung diseases with a high portion of patients with PPF. Although severity of disease, comorbidities and LAS score between the groups didn’t differ, a higher proportion of women and people of younger age were seen in the group pretreated with immunosuppressive drugs and suffering from systemic autoimmune disease and pulmonary hypertension. In addition, allograft related factors (e.g., age or compatibility) were not taken into account completely and antifibrotics were used alone or in combination with other ILD specific medication in a small cohort of the study. Therefore, the beneficial effect on transplant outcome cannot solely attributed to antifibrotics and has to be regarded in the context of previous or simultaneous measures and perioperative conditions.
In conclusion, use of antifibrotics and combined antifibrotic and immunosuppressant drug therapy in patients with end-stage ILD until the moment of LTx proved to be safe, having no significant effects on surgical complications, bleeding or wound healing disorders. Furthermore, patients with pretreatment of antifibrotics as well as combined antifibrotic and immunosuppressant drug therapy had reduced length of mechanical ventilation, improved primary graft function and lower prevalence of de novo donor-specific HLA-antibodies. This is a hypothesis-generating observation warranting further studies.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm12154996/s1, Figure S1: Kaplan–Meier survival in patients undergoing lung transplantation with different previous treatment regimens; Table S1: End-stage ILD of the study cohort and concomitant immunosuppressive and/or antifibrotic therapy prior to LTx; Table S2: Comorbidities assessed during transplant evaluation.
Author Contributions
Participated in research design: D.M., T.V., P.A., S.M., M.I., T.K., N.K., T.V., J.B. and B.M.; Participated in the writing of the paper: T.V., N.K., T.K., D.M., G.L. and J.B.; Participated in the performance of the research: P.A., D.M., J.B., J.B., J.B., N.K. and T.V.; Participated in data analysis: D.M., T.V., P.A., S.M., T.K., N.K., T.V., M.I. and G.L. All authors have read and agreed to the published version of the manuscript.
Funding
Jürgen Behr received honoraria for consulting and lectures from Actelion, Astra-Zeneca, Biogen, BMS, Boehringer-Ingelheim, Ferrer, Galapagos, Novartis, Roche and Sanofi-Genzyme. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the local ethics committee of the University of Munich, Germany (UE No. 646-16).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All relevant data are within the manuscript and its Supporting Information files.
Conflicts of Interest
The authors of this manuscript have conflict of interest to disclose as described by the Journal. J.B., T.V. and N.K. have received honoraria for lectures and consulting fees from Roche and Boehringer-Ingelheim. The other authors have no conflicts of interest to disclose.
Abbreviations
| AZA | azathioprine |
| BLTx | bilateral lung transplantation |
| BMI | body mass index |
| CTD-ILD | connective tissue disease-related ILD |
| DSA | donor specific antibodies |
| ECMO | extracorporeal membrane oxygenation |
| EMA | European Medicines Agency |
| FDA | Food and Drug Administration |
| GAP | gender-age-physiology |
| HP | chronic hypersensitivity pneumonitis |
| ICU | intensive care unit |
| IPF | idiopathic pulmonary fibrosis |
| LAS | lung allocation score |
| LTx | lung transplantation |
| MMF | mycophenolate mofetil |
| NSIP | non-specific interstitial pneumonia |
| PAP | pulmonary arterial pressure |
| PGD | primary graft dysfunction |
| PPF | progressive pulmonary fibrosis |
| SD | standard deviation |
| SLTx | single lung transplantation |
| SSc-ILD | systemic sclerosis-associated ILD |
| TBB | transbronchial biopsies |
| uILD | unclassifiable pulmonary fibrosis |
| UIP | usual interstitial pneumonia |
| 6MWD | 6-minute walking distance |
References
- Kolb, M.; Vašáková, M. The natural history of progressive fibrosing interstitial lung diseases. Respir. Res. 2019, 20, 57. [Google Scholar] [CrossRef] [PubMed]
- Kwon, B.S.; Choe, J.; Chae, E.J.; Hwang, H.S.; Kim, Y.G.; Song, J.W. Progressive fibrosing interstitial lung disease: Prevalence and clinical outcome. Respir. Res. 2021, 22, 282. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Richeldi, L.; Thomson, C.C.; Inoue, Y.; Johkoh, T.; Kreuter, M.; Lynch, D.A.; Maher, T.M.; Martinez, F.J.; et al. Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2022, 205, e18–e47. [Google Scholar] [CrossRef] [PubMed]
- Oto, T.; Griffiths, A.P.; Levvey, B.J.; Pilcher, D.V.; Williams, T.J.; Snell, G.I. Definitions of primary graft dysfunction after lung transplantation: Differences between bilateral and single lung transplantation. J. Thorac. Cardiovasc. Surg. 2006, 132, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Distler, O.; Highland, K.B.; Gahlemann, M.; Azuma, A.; Fischer, A.; Mayes, M.D.; Raghu, G.; Sauter, W.; Girard, M.; Alves, M.; et al. Nintedanib for Systemic Sclerosis-Associated Interstitial Lung Disease. N. Engl. J. Med. 2019, 380, 2518–2528. [Google Scholar] [CrossRef]
- Flaherty, K.R.; Wells, A.U.; Cottin, V.; Devaraj, A.; Walsh, S.L.; Inoue, Y.; Richeldi, L.; Kolb, M.; Tetzlaff, K.; Stowasser, S.; et al. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. N. Engl. J. Med. 2019, 381, 1718–1727. [Google Scholar] [CrossRef]
- Wells, A.U.; Flaherty, K.R.; Brown, K.K.; Inoue, Y.; Devaraj, A.; Richeldi, L.; Moua, T.; Crestani, B.; Wuyts, W.A.; Stowasser, S.; et al. Nintedanib in patients with progressive fibrosing interstitial lung diseases-subgroup analyses by interstitial lung disease diagnosis in the INBUILD trial: A randomised, double-blind, placebo-controlled, parallel-group trial. Lancet Respir. Med. 2020, 8, 453–460. [Google Scholar] [CrossRef]
- Behr, J.; Prasse, A.; Kreuter, M.; Johow, J.; Rabe, K.F.; Bonella, F.; Bonnet, R.; Grohe, C.; Held, M.; Wilkens, H.; et al. Pirfenidone in patients with progressive fibrotic interstitial lung diseases other than idiopathic pulmonary fibrosis (RELIEF): A double-blind, randomised, placebo-controlled, phase 2b trial. Lancet Respir. Med. 2021, 9, 476–486. [Google Scholar] [CrossRef]
- Bos, S.; De Sadeleer, L.J.; Vanstapel, A.; Beeckmans, H.; Sacreas, A.; Yserbyt, J.; Wuyts, W.A.; Vos, R. Antifibrotic drugs in lung transplantation and chronic lung allograft dysfunction: A review. Eur. Respir. Rev. 2021, 30, 210050. [Google Scholar] [CrossRef]
- Lambers, C.; Boehm, P.M.; Lee, S.; Ius, F.; Jaksch, P.; Klepetko, W.; Tudorache, I.; Ristl, R.; Welte, T.; Gottlieb, J. Effect of antifibrotics on short-term outcome after bilateral lung transplantation: A multicentre analysis. Eur. Respir. J. 2018, 51, 1800503. [Google Scholar] [CrossRef]
- Leuschner, G.; Stocker, F.; Veit, T.; Kneidinger, N.; Winter, H.; Schramm, R.; Weig, T.; Matthes, S.; Ceelen, F.; Arnold, P.; et al. Outcome of lung transplantation in idiopathic pulmonary fibrosis with previous anti-fibrotic therapy. J. Heart Lung Transplant. 2017, 37, 268–274. [Google Scholar] [CrossRef]
- Mackintosh, J.A.; Munsif, M.; Ranzenbacher, L.; Thomson, C.; Musk, M.; Snell, G.; Glanville, A.; Chambers, D.C.; Hopkins, P. Risk of anastomotic dehiscence in patients with pulmonary fibrosis transplanted while receiving anti-fibrotics: Experience of the Australian Lung Transplant Collaborative. J. Heart Lung Transplant. 2019, 38, 553–559. [Google Scholar] [CrossRef]
- Veit, T.; Leuschner, G.; Sisic, A.; Ceelen, F.; Munker, D.; Schmitzer, M.; Weig, T.; Michel, S.; Schneider, C.; Meiser, B.; et al. Pirfenidone exerts beneficial effects in patients with IPF undergoing single lung transplantation. Am. J. Transplant. 2019, 19, 2358–2365. [Google Scholar] [CrossRef] [PubMed]
- de Boer, W.J.; Mannes, G.P.; van der Bij, W. Preoperative corticosteroids. A contraindication to lung transplantation? Chest 1994, 105, 1908. [Google Scholar] [CrossRef] [PubMed]
- McAnally, K.J.; Valentine, V.G.; LaPlace, S.G.; McFadden, P.M.; Seoane, L.; Taylor, D.E. Effect of pre-transplantation prednisone on survival after lung transplantation. J. Heart Lung Transplant. 2006, 25, 67–74. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society; European Respiratory Society. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am. J. Respir. Crit. Care Med. 2002, 165, 277–304. [Google Scholar]
- Kondoh, Y.; Makino, S.; Ogura, T.; Suda, T.; Tomioka, H.; Amano, H.; Anraku, M.; Enomoto, N.; Fujii, T.; Fujisawa, T.; et al. 2020 guide for the diagnosis and treatment of interstitial lung disease associated with connective tissue disease. Respir. Investig. 2021, 59, 709–740. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Ryerson, C.J.; Myers, J.L.; Kreuter, M.; Vasakova, M.; Bargagli, E.; Chung, J.H.; Collins, B.F.; Bendstrup, E.; et al. Diagnosis of Hypersensitivity Pneumonitis in Adults. An Official ATS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 202, e36–e69. [Google Scholar] [CrossRef]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef]
- Kneidinger, N.; Winter, H.; Sisic, A.; Preissler, G.; Neurohr, C.; Czerner, S.; Weig, T.; Dolch, M.; Uberfuhr, P.; Schramm, R. Munich lung transplant group: Waiting list during the first 9 months of the lung allocation score era. Thorac. Cardiovasc. Surg. 2014, 62, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Christie, J.D.; Carby, M.; Bag, R.; Corris, P.; Hertz, M.; Weill, D. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction part II: Definition. A consensus statement of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 2005, 24, 1454–1459. [Google Scholar] [CrossRef]
- Kauke, T.; Kneidinger, N.; Martin, B.; Dick, A.; Schneider, C.; Schramm, R.; Meimarakis, G.; Preissler, G.; Eickelberg, O.; von Dossow, V.; et al. Bronchiolitis obliterans syndrome due to donor-specific HLA-antibodies. Tissue Antigens 2015, 86, 178–185. [Google Scholar] [CrossRef]
- A Yousem, S.; Berry, G.J.; Cagle, P.T.; Chamberlain, D.; Husain, A.N.; Hruban, R.H.; Marchevsky, A.; Ohori, N.P.; Ritter, J.; Stewart, S.; et al. Revision of the 1990 working formulation for the classification of pulmonary allograft rejection: Lung Rejection Study Group. J. Heart Lung Transplant. 1996, 15 (1 Pt 1), 1–15. [Google Scholar]
- Vandermeulen, E.; Verleden, S.E.; Ruttens, D.; Moelants, E.; Mortier, A.; Somers, J.; Bellon, H.; Piloni, D.; Dupont, L.J.; Van Raemdonck, D.E.; et al. BAL neutrophilia in azithromycin-treated lung transplant recipients: Clinical significance. Transpl. Immunol. 2015, 33, 37–44. [Google Scholar] [CrossRef]
- Balestro, E.; Solidoro, P.; Parigi, P.; Boffini, M.; Lucianetti, A.; Rea, F. Safety of nintedanib before lung transplant: An Italian case series. Respirol. Case Rep. 2018, 6, e00312. [Google Scholar] [CrossRef]
- Ito, Y.; Tazaki, G.; Kondo, Y.; Takahashi, G.; Sakamaki, F. Therapeutic effect of nintedanib on acute exacerbation of interstitial lung diseases. Respir. Med. Case Rep. 2019, 26, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Bharat, A.; Kuo, E.; Steward, N.; Aloush, A.; Hachem, R.; Trulock, E.P.; Patterson, G.A.; Meyers, B.F.; Mohanakumar, T. Immunological link between primary graft dysfunction and chronic lung allograft rejection. Ann. Thorac. Surg. 2008, 86, 189–195, discussion 196–197. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.J.; Diamond, J.M. Diamond, Primary Graft Dysfunction (PGD) Following Lung Transplantation. Semin. Respir. Crit. Care Med. 2018, 39, 148–154. [Google Scholar] [CrossRef]
- Oku, H.; Nakazato, H.; Horikawa, T.; Tsuruta, Y.; Suzuki, R. Pirfenidone suppresses tumor necrosis factor-alpha, enhances interleukin-10 and protects mice from endotoxic shock. Eur. J. Pharmacol. 2002, 446, 167–176. [Google Scholar] [CrossRef]
- Wollin, L.; Maillet, I.; Quesniaux, V.; Holweg, A.; Ryffel, B. Antifibrotic and anti-inflammatory activity of the tyrosine kinase inhibitor nintedanib in experimental models of lung fibrosis. J. Pharmacol. Exp. Ther. 2014, 349, 209–220. [Google Scholar] [CrossRef]
- Wollin, L.; Wex, E.; Pautsch, A.; Schnapp, G.; Hostettler, K.E.; Stowasser, S.; Kolb, M. Mode of action of nintedanib in the treatment of idiopathic pulmonary fibrosis. Eur. Respir. J. 2015, 45, 1434–1445. [Google Scholar] [CrossRef]
- Chen, W.-C.; Chen, N.-J.; Chen, H.-P.; Yu, W.-K.; Su, V.Y.-F.; Chen, H.; Wu, H.-H.; Yang, K.-Y. Nintedanib Reduces Neutrophil Chemotaxis via Activating GRK2 in Bleomycin-Induced Pulmonary Fibrosis. Int. J. Mol. Sci. 2020, 21, 4735. [Google Scholar] [CrossRef]
- Ubieta, K.; Thomas, M.J.; Wollin, L. The Effect of Nintedanib on T-Cell Activation, Subsets and Functions. Drug. Des. Devel Ther. 2021, 15, 997–1011. [Google Scholar] [CrossRef]
- Lehtonen, S.T.; Veijola, A.; Karvonen, H.; Lappi-Blanco, E.; Sormunen, R.; Korpela, S.; Zagai, U.; Sköld, M.C.; Kaarteenaho, R. Pirfenidone and nintedanib modulate properties of fibroblasts and myofibroblasts in idiopathic pulmonary fibrosis. Respir. Res. 2016, 17, 14. [Google Scholar] [CrossRef]
- Visner, G.A.; Liu, F.; Bizargity, P.; Liu, H.; Liu, K.; Yang, J.; Wang, L.; Hancock, W.W. Pirfenidone inhibits T-cell activation, proliferation, cytokine and chemokine production, and host alloresponses. Transplantation 2009, 88, 330–338. [Google Scholar] [CrossRef]
- Du, J.; Paz, K.; Flynn, R.; Vulic, A.; Robinson, T.M.; Lineburg, K.E.; Alexander, K.A.; Meng, J.; Roy, S.; Panoskaltsis-Mortari, A.; et al. Pirfenidone ameliorates murine chronic GVHD through inhibition of macrophage infiltration and TGF-β production. Blood 2017, 129, 2570–2580. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).