
Characteristics and Long-Term Outcome of 535 Patients with Autoimmune Hepatitis—The 20-Year Experience of a High-Volume Tertiary Center
 , ,
, ,  and
and
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Information, Data Collection, and Ethical Considerations
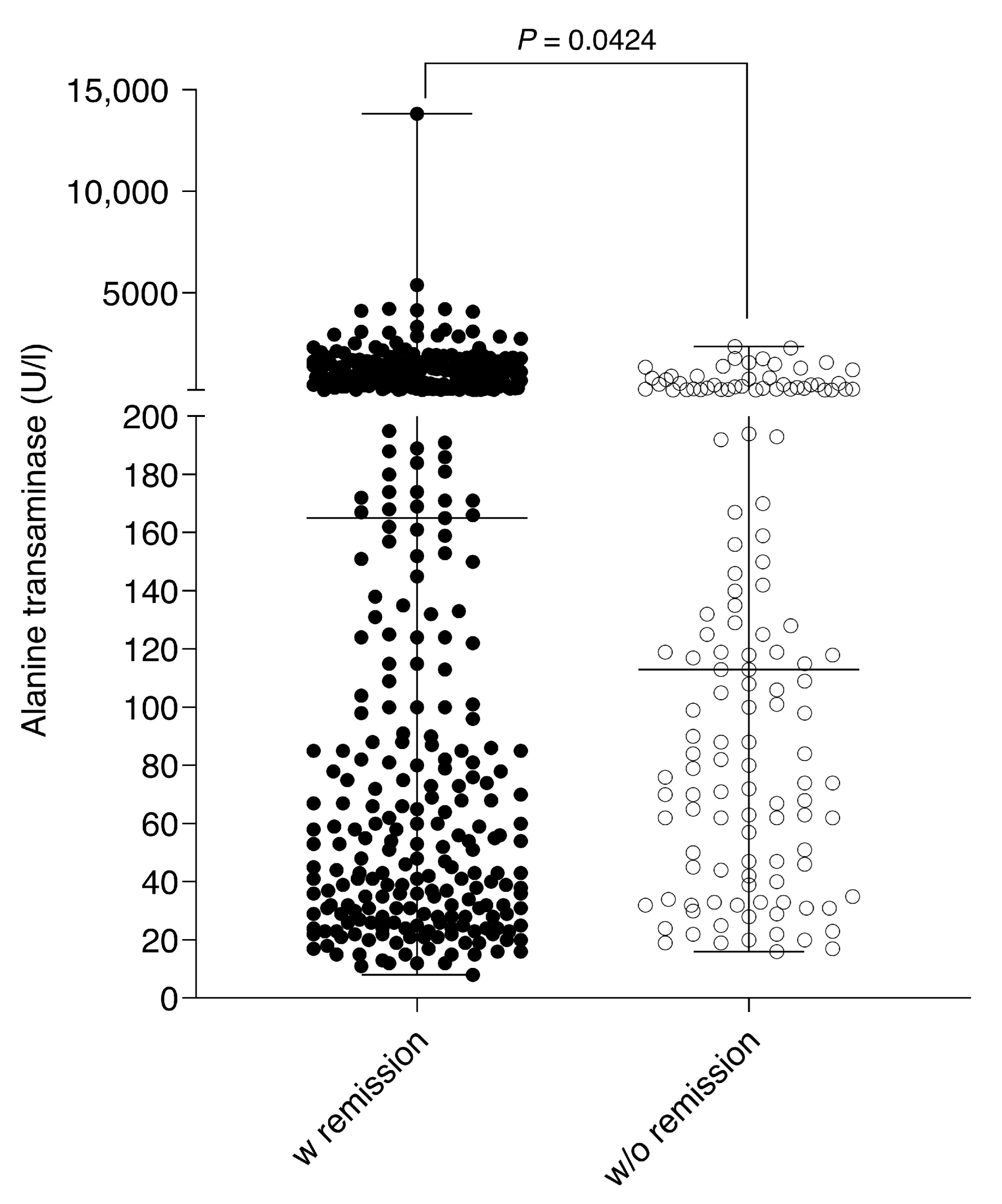
2.2. Laboratory Parameters, Immunosuppressive Therapy, and the Definition of Therapy Response
2.3. Statistical Analysis
3. Results
3.1. Demographic and Laboratory Data
3.2. Autoantibodies and Genetic Background
3.3. Overlap to Other Autoimmune Diseases and Co-Morbidities
3.4. Immunosuppression and Therapy Response
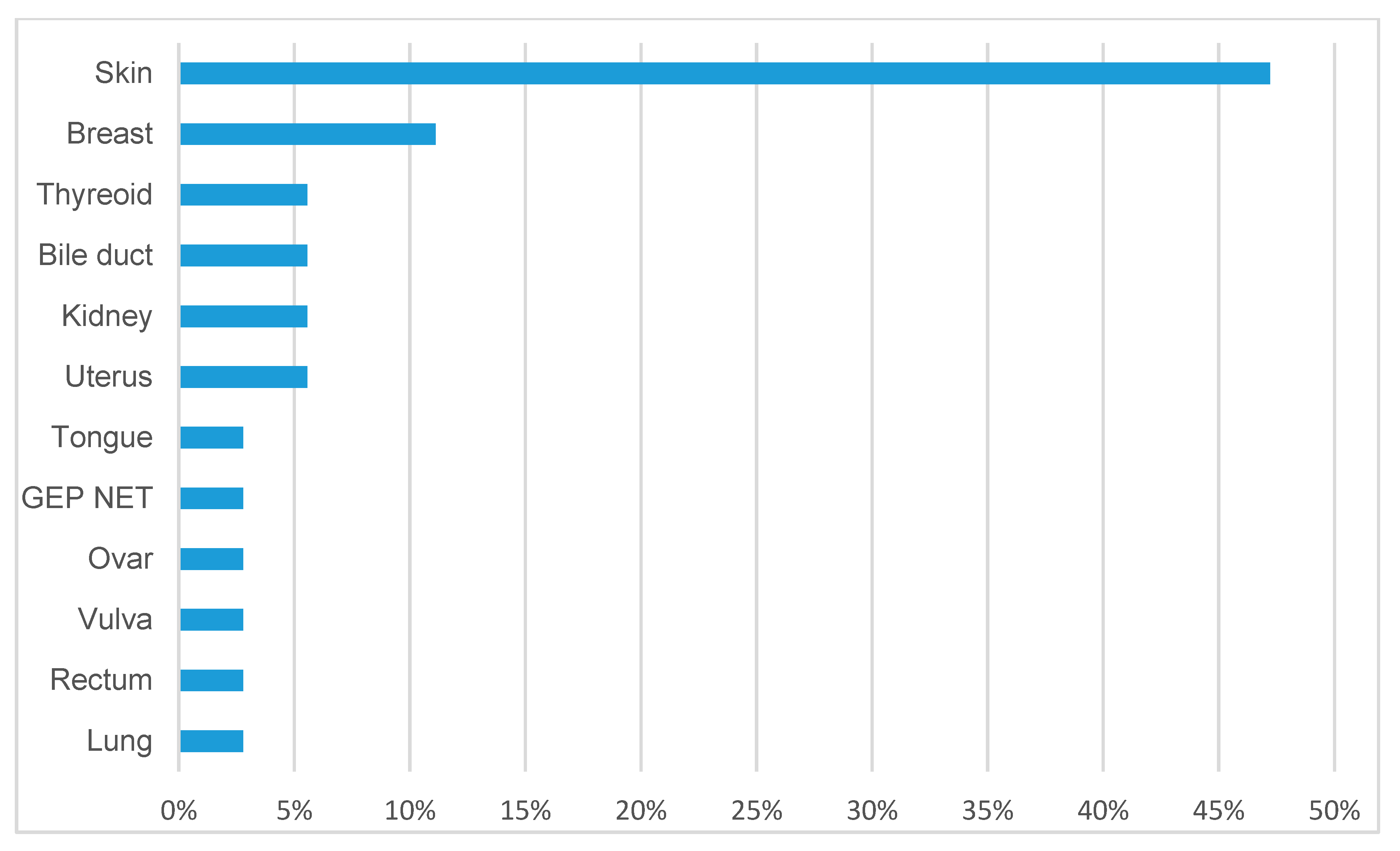
3.5. Tumor Diseases
3.6. Long-Term Outcome and Mortality
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Gatselis, N.K.; Zachou, K.; Koukoulis, G.K.; Dalekos, G.N. Autoimmune hepatitis, one disease with many faces: Etiopathogenetic, clinico-laboratory and histological characteristics. World J. Gastroenterol. 2015, 21, 60–83. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, F.; Miao, Q.; Krawitt, E.L.; Gershwin, M.E.; Ma, X. The clinical phenotypes of autoimmune hepatitis: A comprehensive review. J. Autoimmun. 2015, 66, 98–107. [Google Scholar] [CrossRef]
- van Gerven, N.M.; Verwer, B.J.; Witte, B.I.; van Erpecum, K.J.; van Buuren, H.R.; Maijers, I.; Visscher, A.P.; Verschuren, E.C.; van Hoek, B.; Coenraad, M.J.; et al. Epidemiology and clinical characteristics of autoimmune hepatitis in the Netherlands. Scand. J. Gastroenterol. 2014, 49, 1245–1254. [Google Scholar] [CrossRef]
- Feld, J.J.; Heathcote, E.J. Epidemiology of autoimmune liver disease. J. Gastroenterol. Hepatol. 2003, 18, 1118–1128. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar] [CrossRef]
- Hennes, E.M.; Zeniya, M.; Czaja, A.J.; Parés, A.; Dalekos, G.N.; Krawitt, E.L.; Bittencourt, P.L.; Porta, G.; Boberg, K.M.; Hofer, H.; et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology 2008, 48, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Abraham, J.; Siddiqui, J.; Raina, D.; Wu, G.Y.; Chalasani, N.P.; Bonkovsky, H.L. Autoimmune Hepatitis Triggered by Statins. J. Clin. Gastroenterol. 2006, 40, 757–761. [Google Scholar] [CrossRef]
- Buechter, M.; Manka, P.; Heinemann, F.M.; Lindemann, M.; Baba, H.A.; Schlattjan, M.; Canbay, A.; Gerken, G.; Kahraman, A. Potential triggering factors of acute liver failure as a first manifestation of autoimmune hepatitis-a single center experience of 52 adult patients. World J. Gastroenterol. 2018, 24, 1410–1418. [Google Scholar] [CrossRef]
- Castiella, A.; Zapata, E.; Lucena, M.I.; Andrade, R.J. Drug-induced autoimmune liver disease: A diagnostic dilemma of an increasingly reported disease. World J. Hepatol. 2014, 6, 160–168. [Google Scholar] [CrossRef]
- Liberal, R.; Longhi, M.S.; Mieli-Vergani, G.; Vergani, D. Pathogenesis of autoimmune hepatitis. Best Pract. Res. Clin. Gastroenterol. 2011, 25, 653–664. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, P.T. Genetics of liver disease: Immunogenetics and disease pathogenesis. Gut 2004, 53, 599–608. [Google Scholar] [CrossRef]
- Manns, M.P.; Lohse, A.W.; Vergani, D. Autoimmune hepatitis—Update 2015. J. Hepatol. 2015, 62, S100–S111. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; McFarlane, I.G.; Williams, R. Azathioprine for Long-Term Maintenance of Remission in Autoimmune Hepatitis. N. Engl. J. Med. 1995, 333, 958–963. [Google Scholar] [CrossRef]
- Zachou, K.; Gatselis, N.; Papadamou, G.; Rigopoulou, E.I.; Dalekos, G.N. Mycophenolate for the treatment of autoimmune hepatitis: Prospective assessment of its efficacy and safety for induction and maintenance of remission in a large cohort of treatment-naïve patients. J. Hepatol. 2011, 55, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; Czaja, A.J.; Gorham, J.D.; Krawitt, E.L.; Mieli-Vergani, G.; Vergani, D.; Vierling, J.M. Diagnosis and management of autoimmune hepatitis. Hepatology 2010, 51, 2193–2213. [Google Scholar] [CrossRef]
- Manns, M.P.; Woynarowski, M.; Kreisel, W.; Lurie, Y.; Rust, C.; Zuckerman, E.; Bahr, M.J.; Günther, R.; Hultcrantz, R.W.; Spengler, U.; et al. Budesonide Induces Remission More Effectively Than Prednisone in a Controlled Trial of Patients With Autoimmune Hepatitis. Gastroenterology 2010, 139, 1198–1206. [Google Scholar] [CrossRef]
- Yeoman, A.D.; Westbrook, R.H.; Al-Chalabi, T.; Carey, I.; Heaton, N.D.; Portmann, B.C.; Heneghan, M.A. Diagnostic value and utility of the simplified International Autoimmune Hepatitis Group (IAIHG) criteria in acute and chronic liver disease. Hepatology 2009, 50, 538–545. [Google Scholar] [CrossRef]
- Muratori, P.; Granito, A.; Pappas, G.; Muratori, L. Validation of simplified diagnostic criteria for autoimmune hepatitis in Italian patients. Hepatology 2009, 49, 1782–1783. [Google Scholar] [CrossRef]
- Mileti, E.; Rosenthal, P.; Peters, M.G. Validation and Modification of Simplified Diagnostic Criteria for Autoimmune Hepatitis in Children. Clin. Gastroenterol. Hepatol. 2012, 10, 417–421.e2. [Google Scholar] [CrossRef] [PubMed]
- Pape, S.; Snijders, R.J.; Gevers, T.J.; Chazouilleres, O.; Dalekos, G.N.; Hirschfield, G.M.; Lenzi, M.; Trauner, M.; Manns, M.P.; Vierling, J.M.; et al. Systematic review of response criteria and endpoints in autoimmune hepatitis by the International Autoimmune Hepatitis Group. J. Hepatol. 2022, 76, 841–849. [Google Scholar] [CrossRef]
- Hadem, J.; Tacke, F.; Bruns, T.; Langgartner, J.; Strnad, P.; Denk, G.U.; Fikatas, P.; Manns, M.P.; Hofmann, W.P.; Gerken, G.; et al. Etiologies and outcomes of acute liver failure in Germany. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2012, 10, 664–669.e2. [Google Scholar] [CrossRef]
- Puustinen, L.; Barner-Rasmussen, N.; Pukkala, E.; Färkkilä, M. Incidence, prevalence, and causes of death of patients with autoimmune hepatitis: A nationwide register-based cohort study in Finland. Dig. Liver Dis. 2019, 51, 1294–1299. [Google Scholar] [CrossRef] [PubMed]
- Sucher, E.; Sucher, R.; Gradistanac, T.; Brandacher, G.; Schneeberger, S.; Berg, T. Autoimmune Hepatitis—Immunologically Triggered Liver Pathogenesis—Diagnostic and Therapeutic Strategies. J. Immunol. Res. 2019, 2019, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Kanzler, S.; Löhr, H.; Gerken, G.; Galle, P.R.; Lohse, A.W. Long-term management and prognosis of autoimmune hepatitis (AIH): A single center experience. Z. Gastroenterol. 2001, 39, 339–341, 344–348. [Google Scholar] [CrossRef]
- Roberts, S.K.; Therneau, T.M.; Czaja, A.J. Prognosis of histological cirrhosis in type 1 autoimmune hepatitis. Gastroenterology 1996, 110, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Al-Chalabi, T.; Underhill, J.A.; Portmann, B.C.; McFarlane, I.G.; Heneghan, M.A. Impact of gender on the long-term outcome and survival of patients with autoimmune hepatitis. J. Hepatol. 2008, 48, 140–147. [Google Scholar] [CrossRef]
- Werner, M.; Wallerstedt, S.; Lindgren, S.; Almer, S.; Björnsson, E.; Bergquist, A.; Prytz, H.; Sandberg-Gertzén, H.; Hultcrantz, R.; Sangfelt, P.; et al. Characteristics and long-term outcome of patients with autoimmune hepatitis related to the initial treatment response. Scand. J. Gastroenterol. 2010, 45, 457–467. [Google Scholar] [CrossRef]
- Hoeroldt, B.; McFarlane, E.; Dube, A.; Basumani, P.; Karajeh, M.; Campbell, M.; Gleeson, D. Long-term Outcomes of Patients With Autoimmune Hepatitis Managed at a Nontransplant Center. Gastroenterology 2011, 140, 1980–1989. [Google Scholar] [CrossRef]
- Ngu, J.H.; Gearry, R.B.; Frampton, C.M.; Stedman, C.A. Predictors of poor outcome in patients w ith autoimmune hepatitis: A population-based study. Hepatology 2013, 57, 2399–2406. [Google Scholar] [CrossRef]
- Yoshizawa, K.; Matsumoto, A.; Ichijo, T.; Umemura, T.; Joshita, S.; Komatsu, M.; Tanaka, N.; Tanaka, E.; Ota, M.; Katsuyama, Y.; et al. Long-term outcome of Japanese patients with type 1 autoimmune hepatitis. Hepatology 2012, 56, 668–676. [Google Scholar] [CrossRef]
- Kirstein, M.M.; Metzler, F.; Geiger, E.; Heinrich, E.; Hallensleben, M.; Manns, M.P.; Vogel, A. Prediction of short- and long-term outcome in patients with autoimmune hepatitis. Hepatology 2015, 62, 1524–1535. [Google Scholar] [CrossRef]
- Grønbæk, L.; Vilstrup, H.; Jepsen, P. Autoimmune hepatitis in Denmark: Incidence, prevalence, prognosis, and causes of death. A nationwide registry-based cohort study. J. Hepatol. 2014, 60, 612–617. [Google Scholar] [CrossRef] [PubMed]
- van den Brand, F.F.; van der Veen, K.S.; de Boer, Y.S.; Van Nieuwkerk, C.M.; Mulder, C.J.; Bouma, G. Increased Mortality Among Patients With vs Without Cirrhosis and Autoimmune Hepatitis. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2019, 17, 940–947.e2. [Google Scholar] [CrossRef] [PubMed]
- Malekzadeh, Z.; Haghazali, S.; Sepanlou, S.G.; Vahedi, H.; Merat, S.; Sotoudeh, M.; Nasseri-Moghaddam, S.; Malekzadeh, R. Clinical Features and Long Term Outcome of 102 Treated Autoimmune Hepatitis Patients. Hepat. Mon. 2012, 12, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis: Current Status and Future Directions. Gut Liver 2016, 10, 177–203. [Google Scholar] [CrossRef]
- Maiers, M.; Gragert, L.; Madbouly, A.; Steiner, D.; Marsh, S.G.E.; Gourraud, P.; Oudshoorn, M.; Zanden, H.; Schmidt, A.H.; Pingel, J.; et al. 16 th IHIW: Global analysis of registry HLA haplotypes from 20 Million individuals: Report from the IHIW Registry Diversity Group. Int. J. Immunogenet. 2012, 40, 66–71. [Google Scholar] [CrossRef]
- Teufel, A.; Weinmann, A.; Kahaly, G.J.; Centner, C.; Piendl, A.; Wörns, M.; Lohse, A.W.; Galle, P.R.; Kanzler, S. Concurrent Autoimmune Diseases in Patients With Autoimmune Hepatitis. J. Clin. Gastroenterol. 2010, 44, 208–213. [Google Scholar] [CrossRef]
- Werner, M.; Prytz, H.; Ohlsson, B.; Almer, S.; Björnsson, E.; Bergquist, A.; Wallerstedt, S.; Sandberg-Gertzén, H.; Hultcrantz, R.; Sangfelt, P.; et al. Epidemiology and the initial presentation of autoimmune hepatitis in Sweden: A nationwide study. Scand. J. Gastroenterol. 2008, 43, 1232–1240. [Google Scholar] [CrossRef]
- Schramm, C.; Wahl, I.; Weiler-Normann, C.; Voigt, K.; Wiegard, C.; Glaubke, C.; Brähler, E.; Löwe, B.; Lohse, A.W.; Rose, M. Health-related quality of life, depression, and anxiety in patients with autoimmune hepatitis. J. Hepatol. 2014, 60, 618–624. [Google Scholar] [CrossRef]
- Jones, E.; Watkins, M.; Anderson, E.; Gelow, K.; Green, K.; Draucker, C.; Lammert, C. Overlooked Symptoms in Autoimmune Hepatitis Negatively Impact Many Facets of Life. Dig. Dis. Sci. 2022, 68, 77–86. [Google Scholar] [CrossRef]
- Janik, M.; Wunsch, E.; Moskwa, M.; Raszeja-Wyszomirska, J.; Krawczyk, M.; Milkiewicz, P. Depression in autoimmune hepatitis: A need for detailed psychiatric assessment. Pol. Arch. Intern. Med. 2019, 129, 645–647. [Google Scholar] [CrossRef]
- Feld, J.J.; Dinh, H.; Arenovich, T.; Marcus, V.A.; Wanless, I.R.; Heathcote, E.J. Autoimmune hepatitis: Effect of symptoms and cirrhosis on natural history and outcome. Hepatology 2005, 42, 53–62. [Google Scholar] [CrossRef]
- Buechter, M.; Thimm, J.; Baba, H.A.; Bertram, S.; Willuweit, K.; Gerken, G.; Kahraman, A. Liver Maximum Capacity: A Novel Test to Accurately Diagnose Different Stages of Liver Fibrosis. Digestion 2018, 100, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Heneghan, M.A.; Yeoman, A.D.; Verma, S.; Smith, A.D.; Longhi, M.S. Autoimmune hepatitis. Lancet 2013, 382, 1433–1444. [Google Scholar] [CrossRef]
- Beretta-Piccoli, B.T.; Mieli-Vergani, G.; Vergani, D. Autoimmune hepatitis: Standard treatment and systematic review of alternative treatments. World J. Gastroenterol. 2017, 23, 6030–6048. [Google Scholar] [CrossRef]
- Jiyad, Z.; Olsen, C.M.; Burke, M.T.; Isbel, N.M.; Green, A.C. Azathioprine and Risk of Skin Cancer in Organ Transplant Recipients: Systematic Review and Meta-Analysis. Am. J. Transplant. 2016, 16, 3490–3503. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.G. Long-Term Use of Azathioprine in the Management of Autoimmune Hepatitis. Gastroenterol. Hepatol. 2019, 15, 277–279. [Google Scholar]
- Inman, G.J.; Wang, J.; Nagano, A.; Alexandrov, L.B.; Purdie, K.J.; Taylor, R.G.; Sherwood, V.; Thomson, J.; Hogan, S.; Spender, L.C.; et al. The genomic landscape of cutaneous SCC reveals drivers and a novel azathioprine associated mutational signature. Nat. Commun. 2018, 9, 3667. [Google Scholar] [CrossRef]
- Valean, S.; Acalovschi, M.; Dumitrascu, D.L.; Ciobanu, L.; Nagy, G.; Chira, R. Hepatocellular carcinoma in patients with autoimmune hepatitis—A systematic review of the literature published between 1989–2016. Med. Pharm. Rep. 2019, 92, 99–105. [Google Scholar] [CrossRef]
- Teufel, A.; Weinmann, A.; Centner, C.; Piendl, A.; Lohse, A.W.; Galle, P.R.; Kanzler, S. Hepatocellular carcinoma in patients with autoimmune hepatitis. World J. Gastroenterol. 2009, 15, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Czaja, A.J. Current and prospective pharmacotherapy for autoimmune hepatitis. Expert. Opin. Pharmacother. 2014, 15, 1715–1736. [Google Scholar] [CrossRef] [PubMed]
- Liberal, R.; Krawitt, E.L.; Vierling, J.M.; Manns, M.P.; Mieli-Vergani, G.; Vergani, D. Cutting edge issues in autoimmune hepatitis. J. Autoimmun. 2016, 75, 6–19. [Google Scholar] [CrossRef] [PubMed]
- SSchramm, C.; Bubenheim, M.; Adam, R.; Karam, V.; Buckels, J.; O’Grady, J.G.; Jamieson, N.; Pollard, S.; Neuhaus, P.; Manns, M.M.; et al. Primary liver transplantation for autoimmune hepatitis: A comparative analysis of the European Liver Transplant Registry. Liver Transplant. 2010, 16, 461–469. [Google Scholar] [CrossRef]
- Gleeson, D. Long-Term Outcomes of Autoimmune Hepatitis. Clin. Liver Dis. 2019, 14, 24–28. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | Reference Value |
|---|---|---|
| Mean age (years) | 44.8 (18–81) | |
| Male | 134 (25%) | |
| Female | 401 (75%) | |
| BMI (kg/m2) | 25.63 (16.1–46.6) | 18.5–24.9 |
| INR | 1.07 (0.99;1.28) | |
| Total Bilirubin (mg/dL) | 1.2 (0.7;6.3) | 0.3–1.2 |
| ALT (U/L) | 132.5 (46;712) | <35 |
| Cholinesterase (U/L) | 5.7 (3.9;7.8) | 4.9–11.9 |
| Albumin (%) | 54.8 (49;59.9) | 55.8–66.1 |
| Gamma-Globulin (%) | 21 (16.2;27.6) | 11.1–18.8 |
| Immunoglobulin G (mg/dL) | 15.8 (12;21.1) | 7–16 |
| AIH type 1 | 522 (97.6%) | |
| AIH type 2 | 13 (2.4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buechter, M.; Dorn, D.; Möhlendick, B.; Siffert, W.; Baba, H.A.; Gerken, G.; Kahraman, A. Characteristics and Long-Term Outcome of 535 Patients with Autoimmune Hepatitis—The 20-Year Experience of a High-Volume Tertiary Center. J. Clin. Med. 2023, 12, 4192. https://doi.org/10.3390/jcm12134192
Buechter M, Dorn D, Möhlendick B, Siffert W, Baba HA, Gerken G, Kahraman A. Characteristics and Long-Term Outcome of 535 Patients with Autoimmune Hepatitis—The 20-Year Experience of a High-Volume Tertiary Center. Journal of Clinical Medicine. 2023; 12(13):4192. https://doi.org/10.3390/jcm12134192
Chicago/Turabian StyleBuechter, Matthias, Dominik Dorn, Birte Möhlendick, Winfried Siffert, Hideo A. Baba, Guido Gerken, and Alisan Kahraman. 2023. "Characteristics and Long-Term Outcome of 535 Patients with Autoimmune Hepatitis—The 20-Year Experience of a High-Volume Tertiary Center" Journal of Clinical Medicine 12, no. 13: 4192. https://doi.org/10.3390/jcm12134192
APA StyleBuechter, M., Dorn, D., Möhlendick, B., Siffert, W., Baba, H. A., Gerken, G., & Kahraman, A. (2023). Characteristics and Long-Term Outcome of 535 Patients with Autoimmune Hepatitis—The 20-Year Experience of a High-Volume Tertiary Center. Journal of Clinical Medicine, 12(13), 4192. https://doi.org/10.3390/jcm12134192