
Platelet-to-White Blood Cell Ratio Is Associated with Adverse Outcomes in Cirrhotic Patients with Acute Deterioration

 ,
,  , , , ,
, , , ,  , , , , , ,
, , , , , ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. Data Collection and the Definition of Clinical Parameters
2.3. Primary Outcomes and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Comparison of Baseline Characteristics
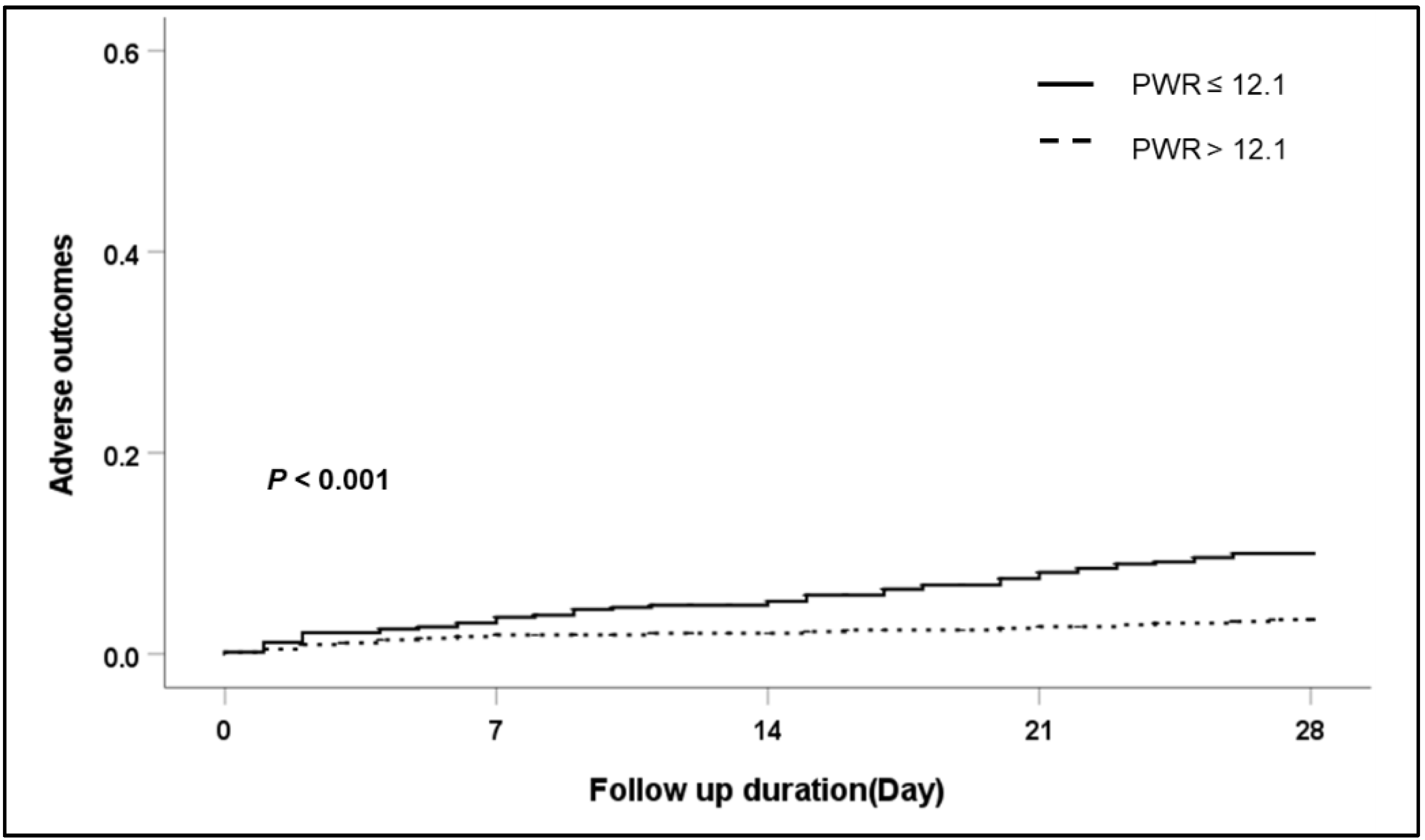
3.2. Associated Factors for 28-Day and Overall Adverse Outcomes of AD of Liver Cirrhosis
3.3. Subgroup Analysis: Effects of the PWR Level on the 28-Day Adverse Outcomes According to the Etiology of Cirrhosis and the Type of AD
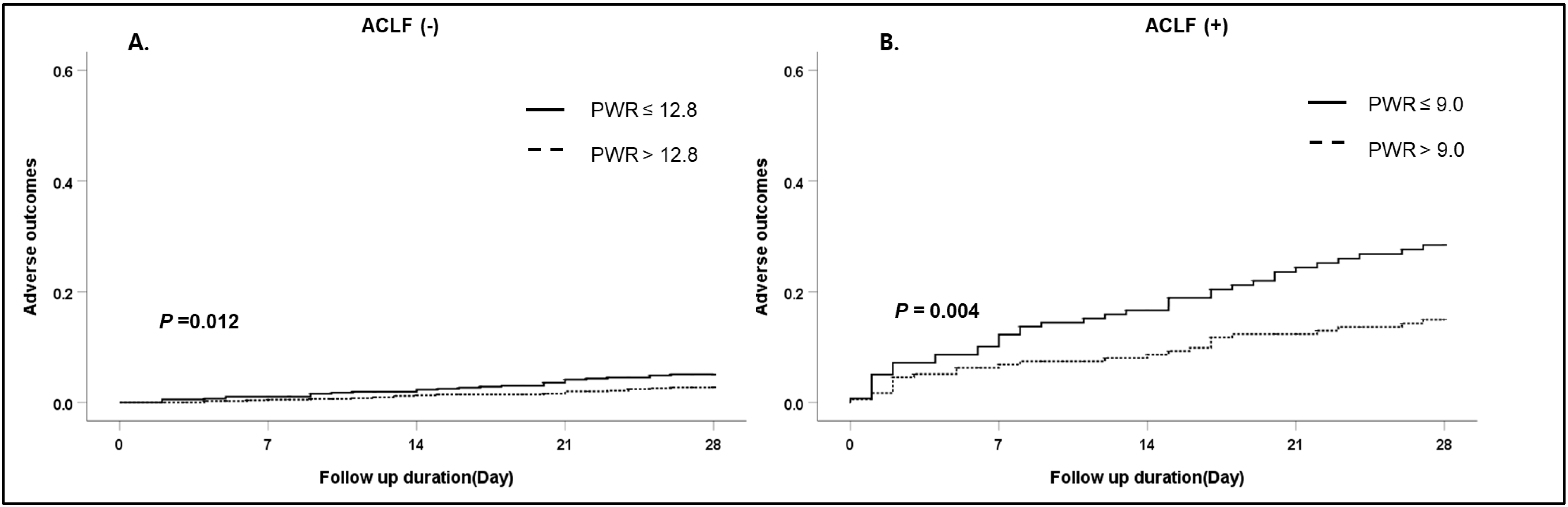
3.4. Subgroup Analysis: Effects of the PWR Level on the 28-Day Adverse Outcomes According to the Presence of ACLF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- European Association for The Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-Chronic Liver Failure Is a Distinct Syndrome That Develops in Patients With Acute Decompensation of Cirrhosis. Gastroenterology 2013, 144, 1426–1437.e9. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Choudhury, A.; Sharma, M.K.; Maiwall, R.; Al Mahtab, M.; Rahman, S.; Saigal, S.; Saraf, N.; Soin, A.S.; Devarbhavi, H.; et al. Acute-on-chronic liver failure: Consensus recommendations of the Asian Pacific association for the study of the liver (APASL): An update. Hepatol. Int. 2019, 13, 353–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalan, R.; Williams, R. Acute-on-chronic liver failure: Pathophysiological basis of therapeutic options. Blood Purif. 2002, 20, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Clària, J.; Stauber, R.E.; Coenraad, M.J.; Moreau, R.; Jalan, R.; Pavesi, M.; Amorós, À.; Titos, E.; Alcaraz-Quiles, J.; Oettl, K.; et al. Systemic inflammation in decompensated cirrhosis: Characterization and role in acute-on-chronic liver failure. Hepatology 2016, 64, 1249–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arroyo, V.; Angeli, P.; Moreau, R.; Jalan, R.; Clària, J.; Trebicka, J.; Fernández, J.; Gustot, T.; Caraceni, P.; Bernardi, M. The systemic inflammation hypothesis: Towards a new paradigm of acute decompensation and multiorgan failure in cirrhosis. J. Hepatol. 2021, 74, 670–685. [Google Scholar] [CrossRef]
- Biyik, M.; Ucar, R.; Solak, Y.; Gungor, G.; Polat, I.; Gaipov, A.; Cakir, O.O.; Ataseven, H.; Demir, A.; Turk, S.; et al. Blood neutrophil-to-lymphocyte ratio independently predicts survival in patients with liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2013, 25, 435–441. [Google Scholar] [CrossRef]
- Zhang, J.; Feng, G.; Zhao, Y.; Zhang, J.; Feng, L.; Yang, J. Association between lymphocyte-to-monocyte ratio (LMR) and the mortality of HBV-related liver cirrhosis: A retrospective cohort study. BMJ Open 2015, 5, e008033. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Sun, Q.; Mao, W.; Fan, J.; Ye, B. Neutrophil-to-Lymphocyte Ratio Predicts Early Mortality in Patients with HBV-Related Decompensated Cirrhosis. Gastroenterol. Res. Pract. 2016, 2016, 4394650. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.J.; Dong, J.J.; Dong, J.Z.; Chen, Y.; Lin, Z.; Song, M.; Wang, Y.Q.; Chen, Y.P.; Shi, K.Q.; Zhou, M.T. A nomogram for predicting prognostic value of inflammatory response biomarkers in decompensated cirrhotic patients without acute-on-chronic liver failure. Aliment. Pharmacol. Ther. 2017, 45, 1413–1426. [Google Scholar] [CrossRef]
- Mao, W.; Wu, J. Haematologic indices in hepatitis B virus-related liver disease. Clin. Chim. Acta 2020, 500, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Qiu, Y.; He, X.; Mao, W.; Han, Z. Platelet-to-white blood cell ratio: A novel and promising prognostic marker for HBV-associated decompensated cirrhosis. J. Clin. Lab. Anal. 2020, 34, e23556. [Google Scholar] [CrossRef] [PubMed]
- Jie, Y.; Gong, J.; Xiao, C.; Zhu, S.; Zhou, W.; Luo, J.; Chong, Y.; Hu, B. Low Platelet to White Blood Cell Ratio Indicates Poor Prognosis for Acute-On-Chronic Liver Failure. BioMed Res. Int. 2018, 2018, 7394904. [Google Scholar] [CrossRef] [PubMed]
- Suk, K.T.; Baik, S.K.; Yoon, J.H.; Cheong, J.Y.; Paik, Y.H.; Lee, C.H.; Kim, Y.S.; Lee, J.W.; Kim, D.J.; Cho, S.W.; et al. Revision and update on clinical practice guideline for liver cirrhosis. Korean J. Hepatol. 2012, 18, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.R.; Mannalithara, A.; Heimbach, J.K.; Kamath, P.S.; Asrani, S.K.; Biggins, S.W.; Wood, N.L.; Gentry, S.E.; Kwong, A.J. MELD 3.0: The Model for End-Stage Liver Disease Updated for the Modern Era. Gastroenterology 2021, 161, 1887–1895.e4. [Google Scholar] [CrossRef]
- Wasmuth, H.E.; Kunz, D.; Yagmur, E.; Timmer-Stranghöner, A.; Vidacek, D.; Siewert, E.; Bach, J.; Geier, A.; Purucker, E.A.; Gressner, A.M.; et al. Patients with acute on chronic liver failure display “sepsis-like” immune paralysis. J. Hepatol. 2005, 42, 195–201. [Google Scholar] [CrossRef]
- Rolando, N.; Wade, J.; Davalos, M.; Wendon, J.; Philpott-Howard, J.; Williams, R. The systemic inflammatory response syndrome in acute liver failure. Hepatology 2000, 32, 734–739. [Google Scholar] [CrossRef]
- Leithead, J.A.; Rajoriya, N.; Gunson, B.K.; Ferguson, J.W. Neutrophil-to-lymphocyte ratio predicts mortality in patients listed for liver transplantation. Liver Int. 2015, 35, 502–509. [Google Scholar] [CrossRef]
- Kwon, J.H.; Jang, J.W.; Kim, Y.W.; Lee, S.W.; Nam, S.W.; Jaegal, D.; Lee, S.; Bae, S.H. The usefulness of C-reactive protein and neutrophil-to-lymphocyte ratio for predicting the outcome in hospitalized patients with liver cirrhosis. BMC Gastroenterol. 2015, 15, 146. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Lou, Y.; Chen, Y.; Yang, J. Prognostic value of the neutrophil-to-lymphocyte ratio in patients with acute-on-chronic liver failure. Int. J. Clin. Pract. 2014, 68, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, O.; Feldman, D.M.; Diakow, M.; Sigal, S.H. The pathophysiology of thrombocytopenia in chronic liver disease. Hepatic Med. Evid. Res. 2016, 8, 39–50. [Google Scholar] [CrossRef] [Green Version]
- Moore, A.H. Thrombocytopenia in Cirrhosis: A Review of Pathophysiology and Management Options. Clin. Liver Dis. 2019, 14, 183–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krogh-Madsen, R.; Møller, K.; Dela, F.; Kronborg, G.; Jauffred, S.; Pedersen, B.K. Effect of hyperglycemia and hyperinsulinemia on the response of IL-6, TNF-alpha, and FFAs to low-dose endotoxemia in humans. Am. J. Physiol. Endocrinol. Metab. 2004, 286, E766–E772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, K.H.; Potts, J.R.; Chetwood, J.; Goubet, S.; Verma, S. Long-term outcomes after hospitalization with spontaneous bacterial peritonitis. J. Dig. Dis. 2015, 16, 228–240. [Google Scholar] [CrossRef]
- Deutsch, M.; Manolakopoulos, S.; Andreadis, I.; Giannaris, M.; Kontos, G.; Kranidioti, H.; Pirounaki, M.; Koskinas, J. Bacterial infections in patients with liver cirrhosis: Clinical characteristics and the role of C-reactive protein. Ann. Gastroenterol. 2018, 31, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, R.; Li, H.; Xia, J.; Wang, X.; Zheng, X.; Huang, Y.; Meng, Z.; Gao, Y.; Qian, Z.; Liu, F.; et al. Lower platelet counts were associated with 90-day adverse outcomes in acute-on-chronic liver disease patients. Ann. Palliat. Med. 2021, 10, 9342–9353. [Google Scholar] [CrossRef]
- Li, H.; Chen, L.Y.; Zhang, N.N.; Li, S.T.; Zeng, B.; Pavesi, M.; Amorós, À.; Mookerjee, R.P.; Xia, Q.; Xue, F.; et al. Characteristics, Diagnosis and Prognosis of Acute-on-Chronic Liver Failure in Cirrhosis Associated to Hepatitis B. Sci. Rep. 2016, 6, 25487. [Google Scholar] [CrossRef]
- Yoon, E.L.; Kim, T.Y.; Lee, C.H.; Kim, T.H.; Cho, H.C.; Lee, S.S.; Kim, S.E.; Kim, H.Y.; Kim, C.W.; Song, D.S.; et al. Long-term Prognosis of Acute-on-Chronic Liver Failure Survivors. J. Clin. Gastroenterol. 2019, 53, 134–141. [Google Scholar] [CrossRef]
- Kim, T.Y.; Song, D.S.; Kim, H.Y.; Sinn, D.H.; Yoon, E.L.; Kim, C.W.; Jung, Y.K.; Suk, K.T.; Lee, S.S.; Lee, C.H.; et al. Characteristics and Discrepancies in Acute-on-Chronic Liver Failure: Need for a Unified Definition. PLoS ONE 2016, 11, e0146745. [Google Scholar] [CrossRef] [Green Version]
- Korean Association for the Study of the Liver. KASL Clinical Practice Guidelines: Management of chronic hepatitis B. Clin. Mol. Hepatol. 2012, 18, 109–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| ALL (n = 1670) | PWR ≤ 12.1 (n = 709) | PWR > 12.1 (n = 961) | p Value | |
|---|---|---|---|---|
| Age (years) | 55.2 ± 11.4 | 53.4 ± 10.9 | 56.5 ± 11.6 | <0.001 |
| Male (%) | 1226 (73.4) | 535 (75.5) | 691 (71.9) | 0.104 |
| Etiology of cirrhosis, n (%) | <0.001 | |||
| Viral infection (HBV/HCV) | 196 (163/33, 11.7) | 70 (56/14, 9.8) | 126 (107/19, 13.1) | |
| Alcohol use | 1164 (69.7) | 552 (73.6) | 642 (66.8) | |
| Viral infection + alcohol use | 140 (8.4) | 68 (9.6) | 72 (7.5) | |
| Others + | 170 (10.2) | 49 (6.9) | 121 (12.6) | |
| Acute decompensation, n (%) | ||||
| Ascites | 483 (28.9) | 181 (25.5) | 302 (31.4) | 0.009 |
| Bacterial infection | 172 (10.3) | 105 (14.8) | 67 (7.0) | <0.001 |
| SBP | 27 (1.6) | 20 (2.1) | 7 (1.0) | |
| Intra-abdominal infection | 17 (1.0) | 12 (1.2) | 5 (0.7) | |
| Pneumonia | 12 (0.7) | 8 (0.8) | 4 (0.6) | |
| Urinary tract infection | 14 (0.8) | 13 (1.3) | 1 (0.1) | |
| Skin infection | 6 (0.4) | 5 (0.5) | 1 (0.1) | |
| Unknown origin | 96 (5.7) | 70 (7.2) | 26 (3.7) | |
| GI bleeding | 534 (32) | 252 (35.5) | 282 (29.3) | 0.007 |
| HE | 274 (16.4) | 112 (15.8) | 162 (16.9) | 0.563 |
| Jaundice | 491 (29.4) | 232 (32.7) | 259 (27.0) | 0.011 |
| CVD, n (%) | 70 (4.2) | 27 (3.8) | 43 (4.5) | 0.502 |
| DM, n (%) | 458 (27.4) | 180 (25.4) | 278 (28.9) | 0.109 |
| HTN, n (%) | 353 (21.1) | 130 (18.3) | 223 (23.2) | 0.016 |
| Precipitating events, n (%) | ||||
| Active alcoholism | 748 (44.8) | 354 (49.9) | 394 (41.0) | <0.001 |
| Bacterial infection | 134 (8.0) | 85 (12.0) | 49 (5.1) | <0.001 |
| GI bleeding | 474 (28.4) | 230 (32.4) | 244 (25.4) | 0.002 |
| Viral reactivation | 31 (1.9) | 8 (1.1) | 23 (2.4) | 0.058 |
| Toxic | 19 (1.1) | 4 (0.6) | 15 (1.6) | 0.058 |
| Others | 88 (5.3) | 25 (3.5) | 63 (6.6) | 0.006 |
| ACLF, n (%) | 315 (18.9) | 196 (27.6) | 119 (12.4) | <0.001 |
| SIRS, n (%) | 411 (24.6) | 239 (33.7) | 172 (17.9) | <0.001 |
| HCC, n (%) | 76 (4.6) | 27 (3.9) | 49 (5.2) | 0.206 |
| PWR | 13.5 (8.8–19.8) | 8.2 (6.2–10.1) | 18.6 (14.7–25.1) | <0.001 |
| PNR | 21.3 (12.8–36.9) | 11.7 (8.2–15.9) | 31.4 (22.8–49.4) | <0.001 |
| Laboratory data | ||||
| WBC count ×109/L | 8.21 (4.75–10.10) | 9.14 (6.56–13.10) | 5.75 (4.09–7.92) | <0.001 |
| Hemoglobin, g/dL | 10.3 (8.4–12.1) | 10.0 (8.2–11.9) | 10.5 (8.5–12.2) | 0.015 |
| Platelet, mg/L | 94 (63–137) | 69 (48–99.5) | 114 (82–161) | <0.001 |
| Bilirubin mg/dL | 3.3 (1.5–7.7) | 4.7 (2.3–9.9) | 2.4 (1.1–5.5) | <0.001 |
| Albumin, g/dL | 2.8 (2.5–3.3) | 2.7 (2.4–3.1) | 2.9 (2.6–3.4) | <0.001 |
| INR | 1.5 (1.3–1.8) | 1.6 (1.4–2.0) | 1.4 (1.2–1.7) | <0.001 |
| Creatinine, mg/dL | 0.9 (0.7–1.3) | 0.9 (0.7–1.5) | 0.9 (0.7–1.1) | <0.001 |
| Sodium, mEq/L | 136 (132–139) | 135 (130–139) | 136 (133–140) | <0.001 |
| Child–Pugh score | 8.0 (7.0–11.0) | 10.0 (8.0–11.0) | 9.0 (7.0–10.0) | <0.001 |
| MELD score | 17.0 (12.8–22.3) | 19.6 (15.3–25.4) | 15.2 (11.2–19.7) | <0.001 |
| MELD-Na score | 19.9 (14.8–26.0) | 23.4 (17.3–29.0) | 18.1 (13.1–23.2) | <0.001 |
| MELD-3 score | 16.9 (10.0–23.8) | 20.5 (13.3–27.6) | 14.6 (8.3–20.7) | <0.001 |
| CLIF-SOFA score | 5.0 (4.0–7.0) | 6.0 (5.0–8.0) | 5.0 (3.0–6.0) | <0.001 |
| Adverse outcome, n (%) | ||||
| 28-day follow-up | 111 (6.6) | 68 (9.6) | 43 (4.5) | <0.001 |
| LT | 12 (0.7) | 7 (1.0) | 5 (0.5) | |
| Overall follow-up | 424 (25.4) | 220 (31.0) | 204 (21.2) | <0.001 |
| LT | 47 (2.8) | 22 (3.1) | 25 (2.6) |
| Univariate HR (95% CI) | p Value | PWR | ||
|---|---|---|---|---|
| Multivariate HR | p Value | |||
| Age | 1.003 (0.984–1.020) | 0.691 | ||
| Sex | 1.099 (0.716–1.686) | 0.667 | ||
| Cirrhosis etiology | Ref. (others) | Ref. (others) | ||
| Viral infection | 2.835 (1.038–7.738) | 0.042 | 2.169 (0.787–5.981) | 0.135 |
| Alcohol use | 2.175 (0.878–5.386) | 0.093 | 1.155 (0.459–2.905) | 0.759 |
| Viral infection and alcohol use | 4.985 (1.861–13.35) | 0.001 | 2.407 (0.884–6.557) | 0.086 |
| Active alcoholism | 1.140 (0.786–1.655) | 0.490 | ||
| Bacterial infection | 2.118 (1.264–3.551) | 0.004 | 1.156 (0.676–1.976) | 0.596 |
| GI bleeding | 0.847 (0.552–1.300) | 0.488 | ||
| Toxic | 0.806 (0.113–5.774) | 0.830 | ||
| Bilirubin | 1.072 (1.056–1.089) | <0.001 | ||
| Albumin | 0.294 (0.207–0.418) | <0.001 | ||
| INR | 1.315 (1.242–1.392) | <0.001 | ||
| Na | 0.944 (0.920–0.968) | <0.001 | ||
| PWR | 3.157 (1.963–5.077) | <0.001 | 1.707 (1.042–2.975) | 0.034 |
| ACLF | 6.374 (4.378–9.281) | <0.001 | 1.729 (1.013–2.950) | 0.045 |
| HCC | 0.569 (0.181–1.792) | 0.335 | ||
| MELD score | 1.130 (1.110–1.150) | <0.001 | 1.101 (1.072–1.131) | <0.001 |
| Univariate HR (95% CI) | p Value | PWR | ||
|---|---|---|---|---|
| Multivariate HR | p Value | |||
| Age | 1.003 (0.995–1.0101) | 0.490 | ||
| Sex | 1.024 (0.824–1.271) | 0.833 | ||
| Cirrhosis etiology | Ref. (others) | Ref. (others) | ||
| Viral infection | 1.003 (0.652–1.544) | 0.989 | ||
| Alcohol use | 1.191 (0.853–1.664) | 0.304 | ||
| Viral infection and alcohol use | 1.670 (1.092–2.577) | 0.018 | ||
| Active alcoholism | 1.098 (0.907–1.330) | 0.337 | ||
| Bacterial infection | 1.641 (1.201–2.244) | 0.002 | 1.051 (0.759–1.455) | 0.771 |
| GI bleeding | 0.670 (0.535–0.839) | <0.001 | 0.841 (0.666–1.063) | 0.143 |
| Toxic | 0.412 (0.103–1.654) | 0.211 | ||
| Bilirubin | 1.052 (1.042–1.063) | <0.001 | ||
| Albumin | 0.420 (0.353–0.499) | <0.001 | ||
| INR | 1.357 (1.297–1.419) | <0.001 | ||
| Na | 0.941 (0.928–0.953) | <0.001 | ||
| PWR | 0.610 (0.498–0.748) | <0.001 | 0.852 (0.687–1.056) | 0.413 |
| ACLF | 2.863 (2.333–3.515) | <0.001 | 1.177 (0.881–1.571) | 0.270 |
| HCC | 0.853 (0.544–1.338) | 0.489 | ||
| MELD score | 1.088 (1.076–1.100) | <0.001 | 1.088 (1.076–1.100) | <0.001 |
| PWR ≤ 12.1 | PWR > 12.1 | ||||
|---|---|---|---|---|---|
| Total | Event | Total | Event | p Value | |
| Etiology of cirrhosis | |||||
| Viral infection | 70 | 7 | 126 | 9 | 0.519 |
| Alcohol use | 522 | 50 | 642 | 21 | <0.001 |
| Viral infection + alcohol use | 68 | 7 | 72 | 12 | 0.282 |
| Others | 49 | 4 | 121 | 1 | 0.010 |
| Acute decompensation | |||||
| Ascites | |||||
| No | 528 | 48 | 659 | 31 | 0.002 |
| Yes | 181 | 20 | 302 | 12 | 0.003 |
| Infection | |||||
| No | 604 | 57 | 894 | 34 | <0.001 |
| Yes | 105 | 11 | 67 | 9 | 0.524 |
| GI bleeding | |||||
| No | 403 | 45 | 627 | 33 | <0.001 |
| Yes | 306 | 23 | 334 | 10 | 0.011 |
| HE | |||||
| No | 597 | 50 | 799 | 33 | 0.001 |
| Yes | 112 | 18 | 162 | 10 | 0.008 |
| Jaundice | |||||
| No | 477 | 35 | 702 | 30 | 0.027 |
| Yes | 232 | 33 | 259 | 13 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.H.; Kim, S.-E.; Song, D.-S.; Kim, H.-Y.; Yoon, E.L.; Kim, T.-H.; Jung, Y.-K.; Suk, K.T.; Jun, B.-G.; Yim, H.-J.; et al. Platelet-to-White Blood Cell Ratio Is Associated with Adverse Outcomes in Cirrhotic Patients with Acute Deterioration. J. Clin. Med. 2022, 11, 2463. https://doi.org/10.3390/jcm11092463
Kim JH, Kim S-E, Song D-S, Kim H-Y, Yoon EL, Kim T-H, Jung Y-K, Suk KT, Jun B-G, Yim H-J, et al. Platelet-to-White Blood Cell Ratio Is Associated with Adverse Outcomes in Cirrhotic Patients with Acute Deterioration. Journal of Clinical Medicine. 2022; 11(9):2463. https://doi.org/10.3390/jcm11092463
Chicago/Turabian StyleKim, Jung Hee, Sung-Eun Kim, Do-Seon Song, Hee-Yeon Kim, Eileen L. Yoon, Tae-Hyung Kim, Young-Kul Jung, Ki Tae Suk, Baek-Gyu Jun, Hyung-Joon Yim, and et al. 2022. "Platelet-to-White Blood Cell Ratio Is Associated with Adverse Outcomes in Cirrhotic Patients with Acute Deterioration" Journal of Clinical Medicine 11, no. 9: 2463. https://doi.org/10.3390/jcm11092463
APA StyleKim, J. H., Kim, S.-E., Song, D.-S., Kim, H.-Y., Yoon, E. L., Kim, T.-H., Jung, Y.-K., Suk, K. T., Jun, B.-G., Yim, H.-J., Kwon, J.-H., Lee, S.-W., Kang, S.-H., Kim, M.-Y., Jeong, S.-W., Jang, J.-Y., Yoo, J.-J., Kim, S.-G., Jin, Y.-J., ... Kim, D. J. (2022). Platelet-to-White Blood Cell Ratio Is Associated with Adverse Outcomes in Cirrhotic Patients with Acute Deterioration. Journal of Clinical Medicine, 11(9), 2463. https://doi.org/10.3390/jcm11092463