
Combination of High-Density and Coherent Mapping for Ablation of Ventricular Arrhythmia in Patients with Structural Heart Disease

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Peri- and Intraprocedural Management
2.3. Ablation Protocol
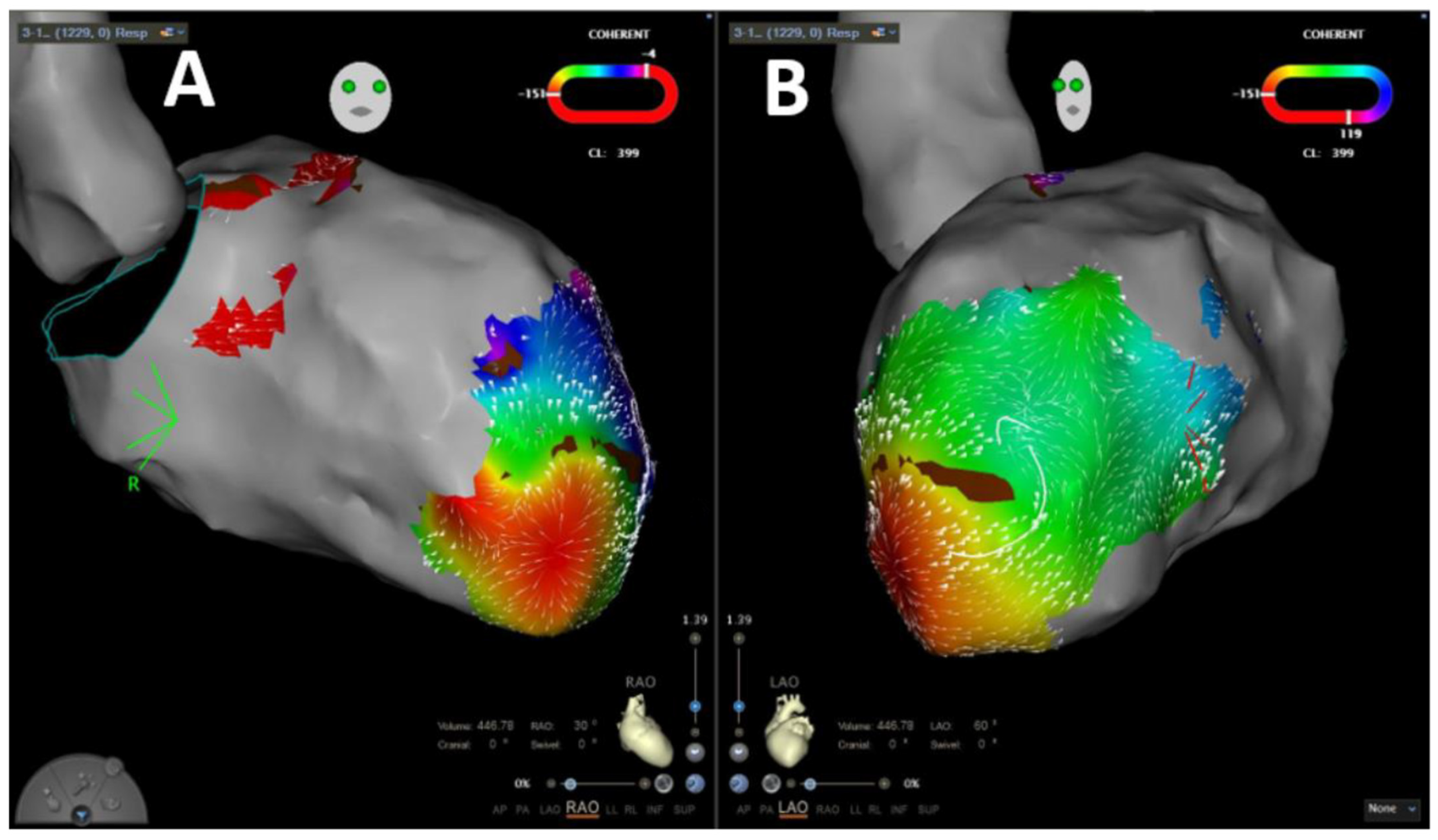
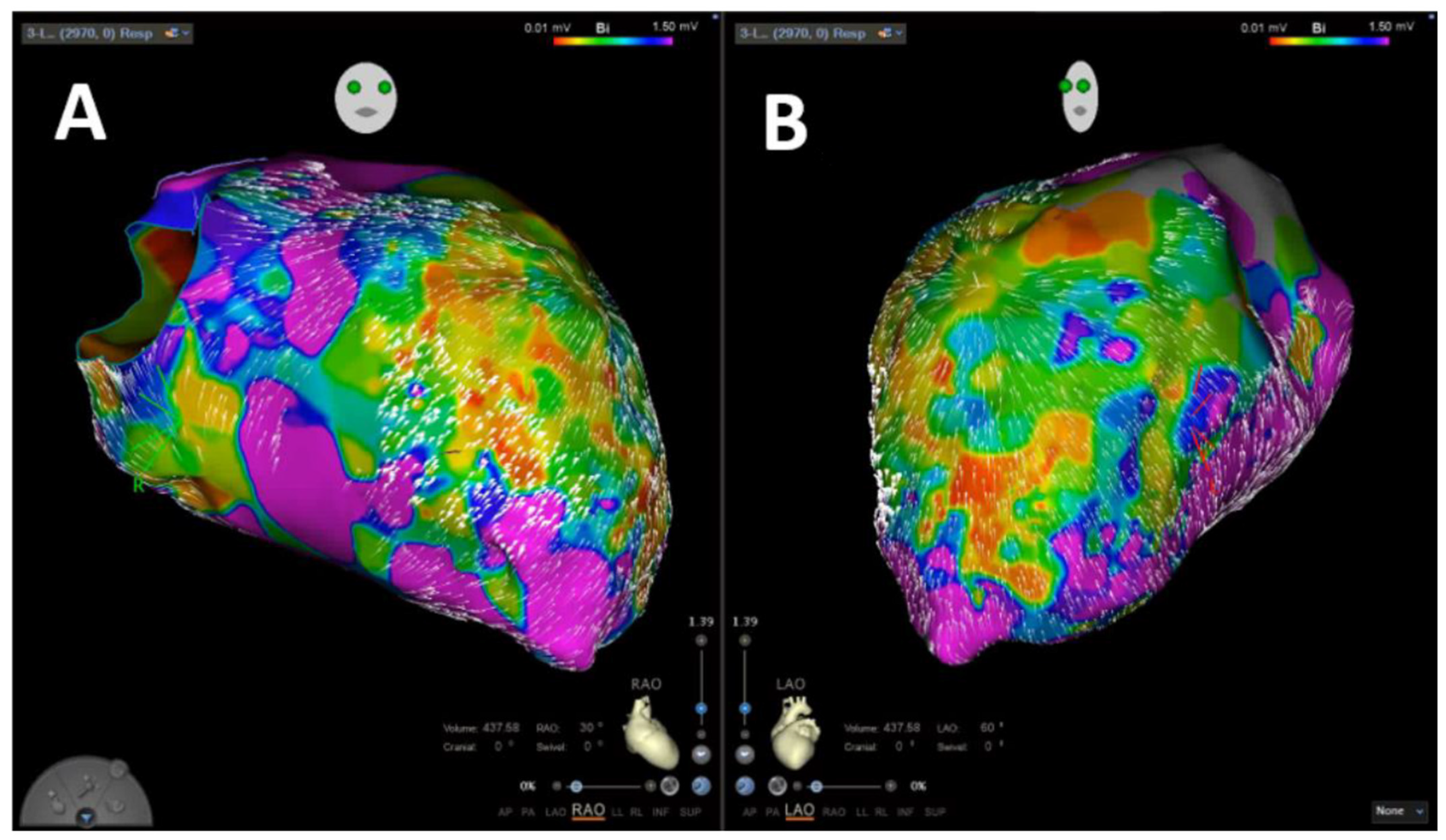
2.4. Coherent Mapping
2.5. Postprocedural Care and Follow Up
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Procedural Data
3.3. Follow Up
3.4. Arrhythmia-Free Survival
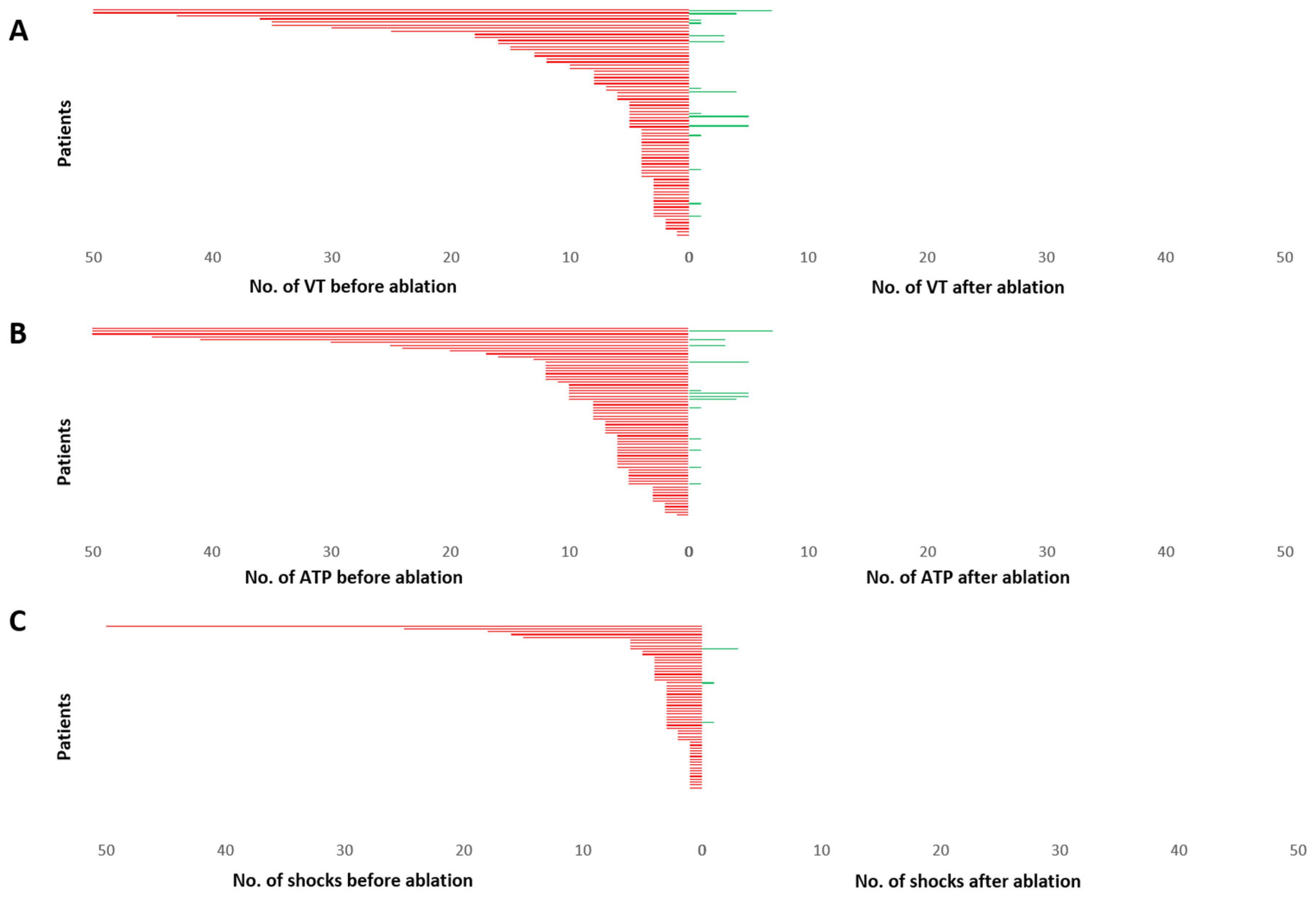
3.5. Ventricular Arrhythmia Burden
4. Discussion
- Ablation of VA based on high-density, velocity-vector-based mapping was performed with short procedural duration and low complication rates.
- Intraprocedural termination of induced VA was achieved in a high number of patients using the novel mapping algorithm.
- Ablation of VA based on the present approach was associated with high acute and mid-term success rates in patients with ICM, as well as in patients with NICM.
- A significant reduction in VA burden and consecutively of ICD therapy burden was observed in all patients after VA ablation.
4.1. Velocity Vector Mapping for Guidance of VA Ablation
4.2. Effectiveness of VA Ablation Implementing Current Mapping Technologies
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- John, R.M.; Tedrow, U.B.; Koplan, B.A.; Albert, C.M.; Epstein, L.M.; Sweeney, M.O.; Miller, A.L.; Michaud, G.F.; Stevenson, W.G. Ventricular arrhythmias and sudden cardiac death. Lancet 2012, 380, 1520–1529. [Google Scholar] [CrossRef]
- Tamburro, P.; Wilber, D. Sudden death in idiopathic dilated cardiomyopathy. Am. Heart J. 1992, 124, 1035–1045. [Google Scholar] [CrossRef]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Europace 2015, 17, 1601–1687. [Google Scholar] [PubMed]
- Kamphuis, H.C.; de Leeuw, J.R.; Derksen, R.; Hauer, R.N.; Winnubst, J.A. Implantable cardioverter defibrillator recipients: Quality of life in recipients with and without ICD shock delivery: A prospective study. Europace 2003, 5, 381–389. [Google Scholar] [CrossRef]
- Poole, J.E.; Johnson, G.W.; Hellkamp, A.S.; Anderson, J.; Callans, D.J.; Raitt, M.H.; Reddy, R.K.; Marchlinski, F.E.; Yee, R.; Guarnieri, T.; et al. Prognostic importance of defibrillator shocks in patients with heart failure. N. Engl. J. Med. 2008, 359, 1009–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, A.J.; Greenberg, H.; Case, R.B.; Zareba, W.; Hall, W.J.; Brown, M.W.; Daubert, J.P.; McNitt, S.; Andrews, M.L.; Elkin, A.D. Multicenter Automatic Defibrillator Implantation Trial-II (MADIT-II) Research Group. Long-term clinical course of patients after termination of ventricular tachyarrhythmia by an implanted defibrillator. Circulation 2004, 21, 3760–3765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, B.K.; Baker, W.L.; Konopka, A.; Giannelli, D.; Coleman, C.I.; Kluger, J.; Cronin, E.M. Systematic review and meta-analysis of catheter ablation of ventricular tachycardia in ischemic heart disease. Heart Rhythm 2020, 17, e206–e219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tung, R.; Vaseghi, M.; Frankel, D.S.; Vergara, P.; Di Biase, L.; Nagashima, K.; Yu, R.; Vangala, S.; Tseng, C.H.; Choi, E.K.; et al. Freedom from recurrent ventricular tachycardia after catheter ablation is associated with improved survival in patients with structural heart disease: An International VT Ablation Center Collaborative Group study. Heart Rhythm 2015, 12, 1997–2007. [Google Scholar] [CrossRef] [Green Version]
- Reddy, V.Y.; Reynolds, M.R.; Neuzil, P.; Richardson, A.W.; Taborsky, M.; Jongnarangsin, K.; Kralovec, S.; Sediva, L.; Ruskin, J.N.; Josephson, M.E. Prophylactic catheter ablation for the prevention of defibrillator therapy. N. Engl. J. Med. 2007, 357, 2657–2665. [Google Scholar] [CrossRef] [Green Version]
- Kuck, K.H.; Schaumann, A.; Eckardt, L.; Willems, S.; Ventura, R.; Delacrétaz, E.; Pitschner, H.F.; Kautzner, J.; Schumacher, B.; Hansen, P.S.; et al. Catheter ablation of stable ventricular tachycardia before defibrillator implantation in patients with coronary heart disease (VTACH): A multicentre randomised controlled trial. Lancet 2010, 375, 31–40. [Google Scholar] [CrossRef]
- Kuck, K.H.; Tilz, R.R.; Deneke, T.; Hoffmann, B.A.; Ventura, R.; Hansen, P.S.; Zarse, M.; Hohnloser, S.H.; Kautzner, J.; Willems, S.; et al. Impact of Substrate Modification by Catheter Ablation on Implantable Cardioverter-Defibrillator Interventions in Patients With Unstable Ventricular Arrhythmias and Coronary Artery Disease: Results From the Multicenter Randomized Controlled SMS (Substrate Modification Study). Circ. Arrhythm. Electrophysiol. 2017, 10, e004422. [Google Scholar] [PubMed]
- Sapp, J.L.; Wells, G.A.; Parkash, R.; Stevenson, W.G.; Blier, L.; Sarrazin, J.F.; Thibault, B.; Rivard, L.; Gula, L.; Leong-Sit, P.; et al. Ventricular Tachycardia Ablation versus Escalation of Antiarrhythmic Drugs. N. Engl. J. Med. 2016, 375, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Vicera, J.J.B.; Lin, Y.-J.; Lee, P.-T.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Chung, F.-P.; Lin, C.-Y.; Chang, T.Y.; Tuan, T.-C.; et al. Identification of critical isthmus using coherent mapping in patients with scar-related atrial tachycardia. J. Cardiovasc. Electrophysiol. 2020, 31, 1436–1447. [Google Scholar] [CrossRef] [PubMed]
- Guckel, D.; Molatta, S.; Imnadze, G.; Bergau, L.; Sommer, P.; Sohns, C. Coherent mapping in adults with congenital heart disease: Role of the novel coherent mapping technique for treatment of atrial tachycardia in adults with congenital heart disease. Herzschrittmacherther. Elektrophysiol. 2021, 32, 119–123. [Google Scholar] [CrossRef]
- Jaïs, P.; Maury, P.; Khairy, P.; Sacher, F.; Nault, I.; Komatsu, Y.; Hocini, M.; Forclaz, A.; Jadidi, A.S.; Weerasooryia, R.; et al. Elimination of local abnormal ventricular activities: A new end point for substrate modification in patients with scar-related ventricular tachycardia. Circulation 2012, 125, 2184–2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2018, 72, 1677–1749, Erratum in: J. Am. Coll. Cardiol. 2018, 72, 1756–1759. [Google Scholar]
- Morady, F.; Harvey, M.; Kalbfleisch, S.J.; el-Atassi, R.; Calkins, H.; Langberg, J.J. Radiofrequency catheter ablation of ventricular tachycardia in patients with coronary artery disease. Circulation 1993, 87, 363–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakagawa, H.; Yamanashi, W.S.; Pitha, J.V.; Arruda, M.; Wang, X.; Ohtomo, K.; Beckman, K.J.; McClelland, J.H.; Lazzara, R.; Jackman, W.M. Comparison of in vivo tissue temperature profile and lesion geometry for radiofrequency ablation with a saline-irrigated electrode versus temperature control in a canine thigh muscle preparation. Circulation 1995, 91, 2264–2273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, W.G.; Wilber, D.J.; Natale, A.; Jackman, W.M.; Marchlinski, F.E.; Talbert, T.; Gonzalez, M.D.; Worley, S.J.; Daoud, E.G.; Hwang, C.; et al. Irrigated radiofrequency catheter ablation guided by electroanatomic mapping for recurrent ventricular tachycardia after myocardial infarction: The multicenter thermocool ventricular tachycardia ablation trial. Circulation 2008, 118, 2773–2782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santangeli, P.; Frankel, D.S.; Marchlinski, F.E. End points for ablation of scar-related ventricular tachycardia. Circ. Arrhythm. Electrophysiol. 2014, 7, 949–960. [Google Scholar] [CrossRef] [Green Version]
- Anter, E.; Duytschaever, M.; Shen, C.; Strisciuglio, T.; Leshem, E.; Contreras-Valdes, F.M.; Waks, J.W.; Zimetbaum, P.J.; Kumar, K.; Spector, P.S.; et al. Activation Mapping With Integration of Vector and Velocity Information Improves the Ability to Identify the Mechanism and Location of Complex Scar-Related Atrial Tachycardias. Circ. Arrhythm. Electrophysiol. 2018, 11, e006536. [Google Scholar] [CrossRef]
- Køber, L.; Thune, J.J.; Nielsen, J.C.; Haarbo, J.; Videbæk, L.; Korup, E.; Jensen, G.; Hildebrandt, P.; Steffensen, F.H.; Bruun, N.E.; et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N. Engl. J. Med. 2016, 9, 1221–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Khatib, S.M.; Daubert, J.P.; Anstrom, K.J.; Daoud, E.G.; Gonzalez, M.; Saba, S.; Jackson, K.P.; Reece, T.; Gu, J.; Pokorney, S.D.; et al. Catheter ablation for ventricular tachycardia in patients with an implantable cardioverter defibrillator (CALYPSO) pilot trial. J. Cardiovasc. Electrophysiol. 2015, 26, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Willems, S.; Tilz, R.R.; Steven, D.; Kääb, S.; Wegscheider, K.; Gellér, L.; Meyer, C.; Heeger, C.H.; Metzner, A.; Sinner, M.F.; et al. Preventive or Deferred Ablation of Ventricular Tachycardia in Patients With Ischemic Cardiomyopathy and Implantable Defibrillator (BERLIN VT): A Multicenter Randomized Trial. Circulation 2020, 141, 1057–1067. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | 65 (87.8) |
| Female | 9 (12.2) |
| Age [years] | 65 ± 11.44 |
| BMI [kg/m²] | 28.57 ± 6.71 |
| GFR [mL/min] | 61 ± 15.4 |
| NICM | 39 (52.7) |
| ICM | 35 (47.3) |
| LV-EF [%] | 33.82 ± 9.88 |
| ICD | 72 (97.3) |
| LVAD | 5 (6.8) |
| Antiarrhythmic medication | 48 (64.9) |
| Amiodaron | 44 (91.7) |
| Sotalol | 4 (8.3) |
| Oral anticoagulation | 46 (62.2) |
| DOAC | 23 (0.5) |
| Vitamin K antagonist | 23 (0.5) |
| Antiplatelet medication | 26 (35.1) |
| VT storm | 15 (20.3) |
| Epicardial access | 10 (13.5) |
| Procedure time [min] | 167 ± 27.68 |
| Fluoroscopy time [min] | 11 ± 5 |
| Fluoroscopy dosage [yGym²] | 1319.04 ± 121.67 |
| Mapping time RV in sinus rhythm [min] | 7 ± 5.18 |
| Mapping time LV in sinus rhythm [min] | 26 ± 9.88 |
| Points voltage mapping LV [n], % | 2044.76 ± 1269.81 |
| Mapping time tachycardia [min] | 9 ± 1.78 |
| Points LAT in tachycardia [n], % | 1286.62 ± 217.29 |
| RV volume [mL] | 132.89 ± 43.11 |
| LV volume [mL] | 281.62 ± 101.75 |
| Low voltage area [%] | 19.6 ± 14.18 |
| Ablation time [min] | 34 ± 16.21 |
| VT inducible [n], % | 65 (87.3) |
| VT mapping possible [n], % | 31 (41.9) |
| Termination of VT by ablation [n], % | 29 (93.5) |
| Pace-mapping performed [n], % | 27 (36.5) |
| Substrate modification performed [n], % | 66 (89.2) |
| Non-inducibility of any VT at end of procedure [n], % | 70 (94.6) |
| Duration [days] | 221.64 ± 25.78 |
| VT recurrence [n], % | 15 (20.3) |
| Mean time to recurrence [days] | 247 ± 183.51 |
| ICD therapy after ablation [n], % | 12 (16.7) |
| ATP [n], % | 11 (15.3) |
| ICD shock [n], % | 7 (9.7) |
| Death during FU [n], % | 9 (12.2) |
| Death due to non-cardiogenic cause [n], % | 7 (77.8) |
| Death due to cardiogenic cause [n], % | 2 (22.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sciacca, V.; Fink, T.; Bergau, L.; Imnadze, G.; El Hamriti, M.; Guckel, D.; Braun, M.; Khalaph, M.; Sommer, P.; Sohns, C. Combination of High-Density and Coherent Mapping for Ablation of Ventricular Arrhythmia in Patients with Structural Heart Disease. J. Clin. Med. 2022, 11, 2418. https://doi.org/10.3390/jcm11092418
Sciacca V, Fink T, Bergau L, Imnadze G, El Hamriti M, Guckel D, Braun M, Khalaph M, Sommer P, Sohns C. Combination of High-Density and Coherent Mapping for Ablation of Ventricular Arrhythmia in Patients with Structural Heart Disease. Journal of Clinical Medicine. 2022; 11(9):2418. https://doi.org/10.3390/jcm11092418
Chicago/Turabian StyleSciacca, Vanessa, Thomas Fink, Leonard Bergau, Guram Imnadze, Mustapha El Hamriti, Denise Guckel, Martin Braun, Moneeb Khalaph, Philipp Sommer, and Christian Sohns. 2022. "Combination of High-Density and Coherent Mapping for Ablation of Ventricular Arrhythmia in Patients with Structural Heart Disease" Journal of Clinical Medicine 11, no. 9: 2418. https://doi.org/10.3390/jcm11092418
APA StyleSciacca, V., Fink, T., Bergau, L., Imnadze, G., El Hamriti, M., Guckel, D., Braun, M., Khalaph, M., Sommer, P., & Sohns, C. (2022). Combination of High-Density and Coherent Mapping for Ablation of Ventricular Arrhythmia in Patients with Structural Heart Disease. Journal of Clinical Medicine, 11(9), 2418. https://doi.org/10.3390/jcm11092418