
Prognostic Markers of Ocrelizumab Effectiveness in Multiple Sclerosis: A Real World Observational Multicenter Study

 , ,
, ,  , ,
, ,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Procedures and Participants
2.2. Statistical Analyses
3. Results
3.1. Clinico-Demographic Features
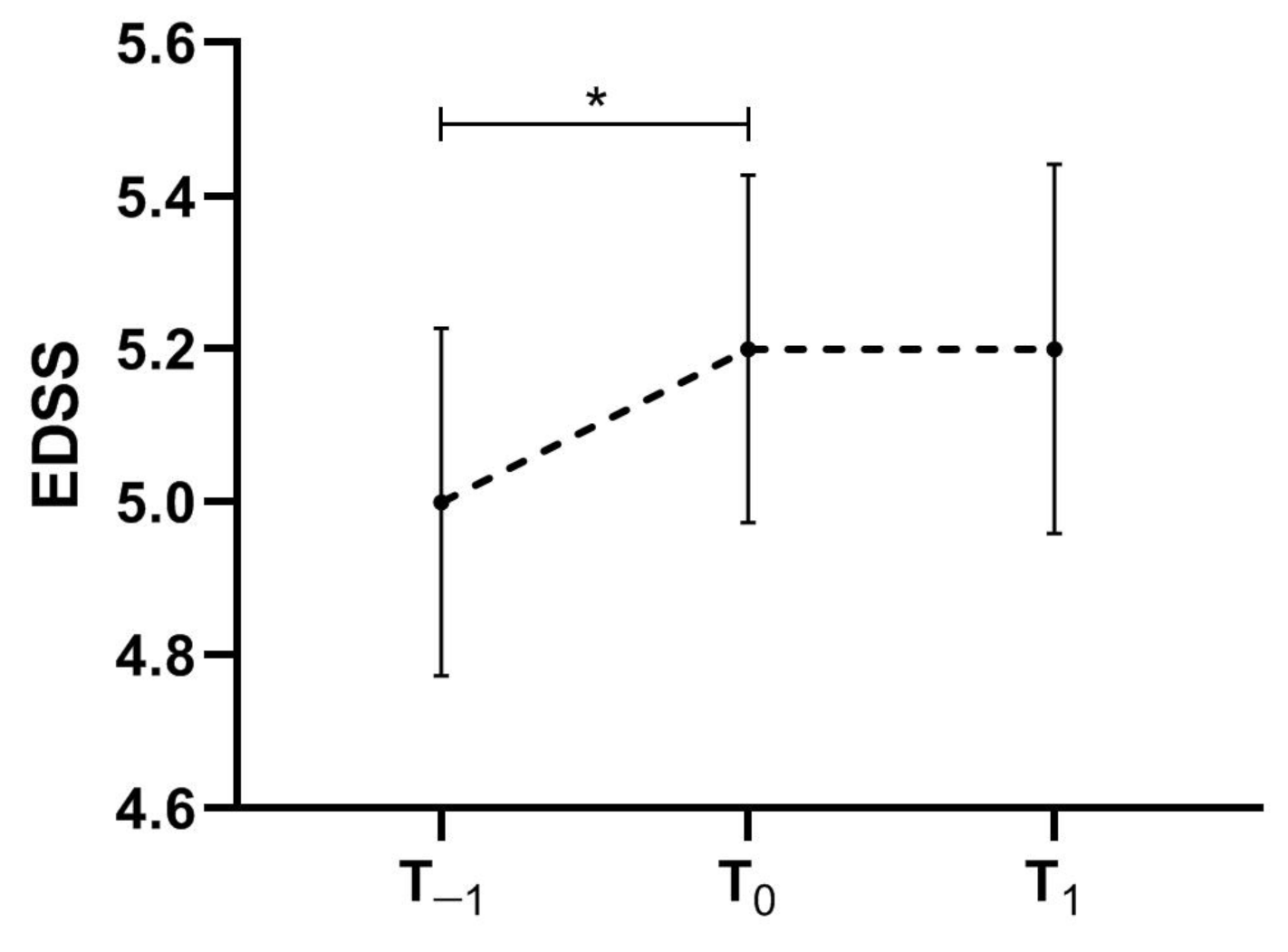
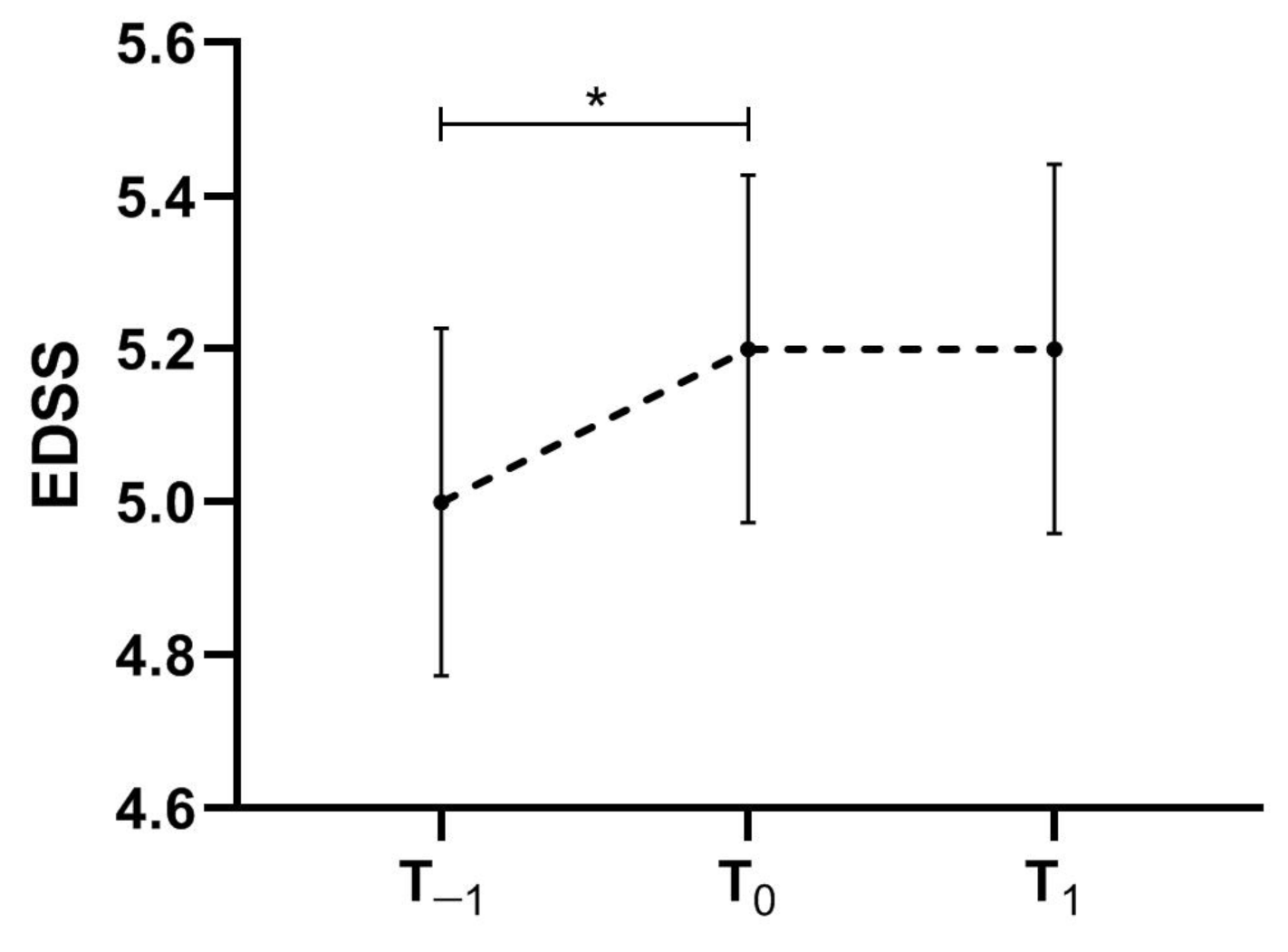
3.2. Effectiveness Analysis
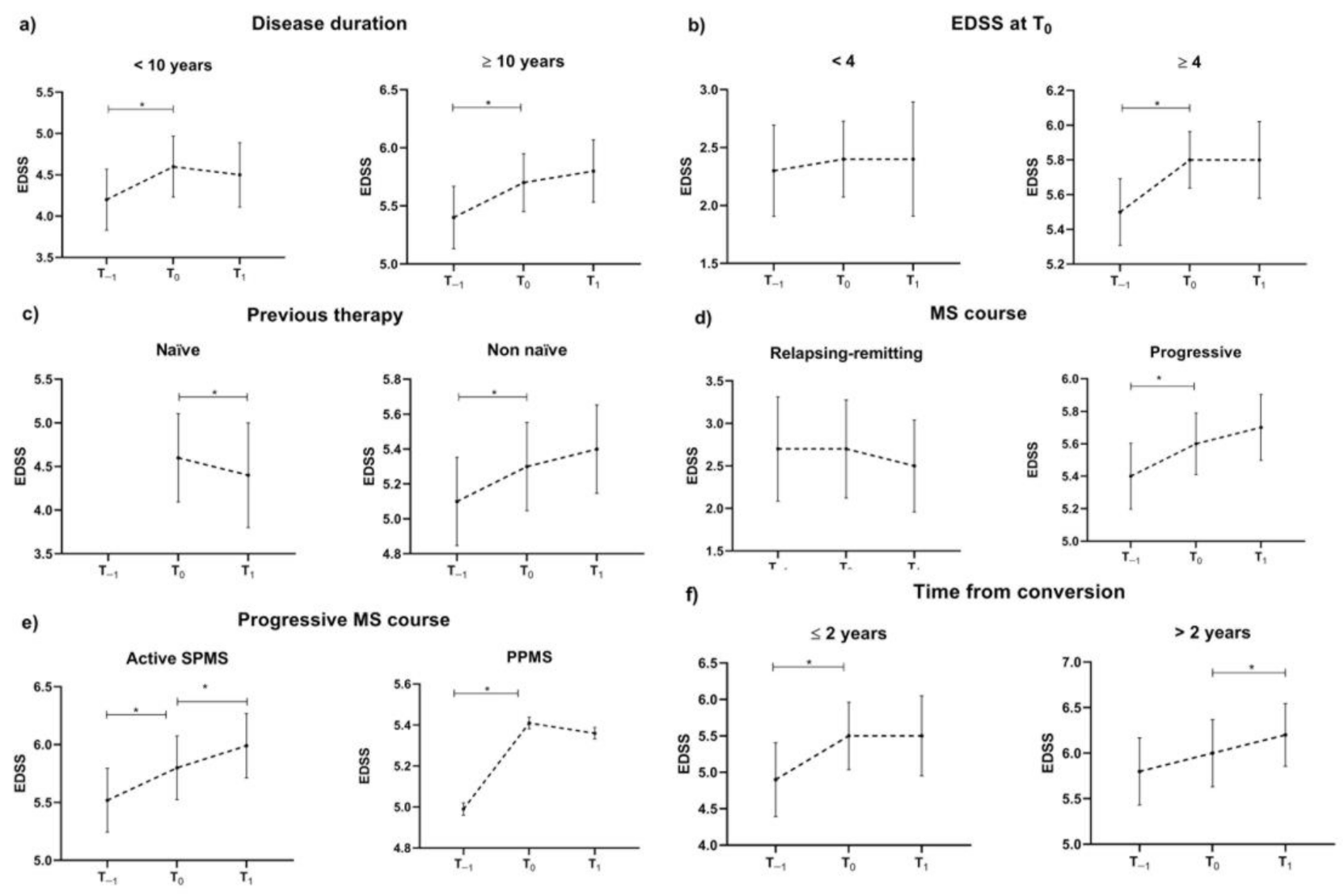
3.3. Post-Hoc Effectiveness Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kappos, L.; Li, D.; Calabresi, P.A.; O’Connor, P.; Bar-Or, A.; Barkhof, F.; Yin, M.; Leppert, D.; Glanzman, R.; Tinbergen, J.; et al. Ocrelizumab in relapsing-remitting multiple sclerosis: A phase 2, randomised, placebo-controlled, multicentre trial. Lancet 2011, 378, 1779–1787. [Google Scholar] [CrossRef]
- Hauser, S.L.; Bar-Or, A.; Comi, G.; Giovannoni, G.; Hartung, H.P.; Hemmer, B.; Lublin, F.; Montalban, X.; Rammohan, K.W.; Selmaj, K.; et al. Ocrelizumab versus Interferon Beta-1a in Relapsing Multiple Sclerosis. N. Engl. J. Med. 2017, 376, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Montalban, X.; Hauser, S.L.; Kappos, L.; Arnold, D.L.; Bar-Or, A.; Comi, G.; de Seze, J.; Giovannoni, G.; Hartung, H.P.; Hemmer, B.; et al. Ocrelizumab versus Placebo in Primary Progressive Multiple Sclerosis. N. Engl. J. Med. 2017, 376, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Cellerino, M.; Boffa, G.; Lapucci, C.; Tazza, F.; Sbragia, E.; Mancuso, E.; Bruschi, N.; Minguzzi, S.; Ivaldi, F.; Poire, I.; et al. Predictors of Ocrelizumab Effectiveness in Patients with Multiple Sclerosis. Neurotherapeutics 2021, 18, 2579–2588. [Google Scholar] [CrossRef]
- Rojas, J.I.; Patrucco, L.; Fruns, M.; Hornung, G.; Flores, J.; Carnero Contentti, E.; Lopez, P.A.; Pettinicchi, J.P.; Caride, A.; Galleguillos, L.; et al. Real-world experience of ocrelizumab in multiple sclerosis patients in Latin America. Arq. Neuro-Psiquiatr. 2021, 79, 305–309. [Google Scholar] [CrossRef]
- Turner, B.; Cree, B.A.C.; Kappos, L.; Montalban, X.; Papeix, C.; Wolinsky, J.S.; Buffels, R.; Fiore, D.; Garren, H.; Han, J.; et al. Ocrelizumab efficacy in subgroups of patients with relapsing multiple sclerosis. J. Neurol. 2019, 266, 1182–1193. [Google Scholar] [CrossRef]
- Kalincik, T.; Kuhle, J.; Pucci, E.; Rojas, J.I.; Tsolaki, M.; Sirbu, C.A.; Slee, M.; Butzkueven, H.; Group, M.S.S.L.; Group, M.S.S. Data quality evaluation for observational multiple sclerosis registries. Mult. Scler. 2017, 23, 647–655. [Google Scholar] [CrossRef]
- Daniels, K.; van der Nat, P.B.; Frequin, S.; van der Wees, P.J.; Biesma, D.H.; Hoogervorst, E.L.J.; van de Garde, E.M.W. Real-World Results of Ocrelizumab Treatment for Primary Progressive Multiple Sclerosis. Mult. Scler. Int 2020, 2020, 5463451. [Google Scholar] [CrossRef]
- Prockl, V.; Nickel, F.T.; Utz, K.S.; Frohlich, K.; Engelhorn, T.; Hilz, M.J.; Lee, D.H.; Linker, R.A.; Huhn, K. Real world application of ocrelizumab in multiple sclerosis: Single-center experience of 128 patients. J. Neurol. Sci. 2020, 415, 116973. [Google Scholar] [CrossRef]
- Sempere, A.P.; Berenguer-Ruiz, L.; Borrego-Soriano, I.; Burgos-San Jose, A.; Concepcion-Aramendia, L.; Volar, L.; Aragones, M.; Palazon-Bru, A. Ocrelizumab in Multiple Sclerosis: A Real-World Study From Spain. Front. Neurol. 2020, 11, 592304. [Google Scholar] [CrossRef]
- Coban, H.; Germaine, S.; Dimaandal, I.; Haberli, N.; Padam, C.; Creed, M.A.; Imitola, J. Real-world experience of ocrelizumab initiation in a diverse multiple sclerosis population. Mult. Scler. Relat. Disord. 2021, 53, 103021. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Diaz, E.; Perez-Vicente, J.A.; Villaverde-Gonzalez, R.; Berenguer-Ruiz, L.; Candeliere Merlicco, A.; Martinez-Navarro, M.L.; Gracia Gil, J.; Romero-Sanchez, C.M.; Alfaro-Saez, A.; Diaz, I.; et al. Real-world experience of ocrelizumab in multiple sclerosis in a Spanish population. Ann. Clin. Transl. Neurol. 2021, 8, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Pontieri, L.; Blinkenberg, M.; Bramow, S.; Papp, V.; Rasmussen, P.V.; Kant, M.; Schafer, J.; Mathiesen, H.K.; Jensen, M.B.; Sirakov, G.; et al. Ocrelizumab treatment in multiple sclerosis: A Danish population-based cohort study. Eur. J. Neurol. 2022, 29, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Wolinsky, J.S.; Engmann, N.J.; Pei, J.; Pradhan, A.; Markowitz, C.; Fox, E.J. An exploratory analysis of the efficacy of ocrelizumab in patients with multiple sclerosis with increased disability. Mult. Scler. J. Exp. Transl. Clin. 2020, 6, 1–7. [Google Scholar] [CrossRef]
- Giovannoni, G.; Kappos, L.; de Seze, J.; Hauser, S.L.; Overell, J.; Koendgen, H.; Manfrini, M.; Wang, Q.; Wolinsky, J.S. Risk of requiring a walking aid after 6.5 years of ocrelizumab treatment in patients with relapsing multiple sclerosis: Data from the OPERA I and OPERA II trials. Eur. J. Neurol. 2021, 29, 1238–1242. [Google Scholar] [CrossRef]
- Chalmer, T.A.; Baggesen, L.M.; Norgaard, M.; Koch-Henriksen, N.; Magyari, M.; Sorensen, P.S.; Danish Multiple Sclerosis, G. Early versus later treatment start in multiple sclerosis: A register-based cohort study. Eur. J. Neurol. 2018, 25, 1262-e1110. [Google Scholar] [CrossRef]
- Lublin, F.D. New multiple sclerosis phenotypic classification. Eur. Neurol. 2014, 72 (Suppl. S1), 1–5. [Google Scholar] [CrossRef]
- Agenzia Italiana del Farmaco (AIFA). Determinazione dell’Agenzia Italiana del Farmaco, 20 Marzo 2008. Gazzetta Ufficiale della Repubblica Italiana 2008, 76, 67–74. Available online: http://www.omceoge.org/newsdoc/AIFA_20_3_2008.pdf (accessed on 2 April 2022).
- Weinshenker, B.G.; Bass, B.; Rice, G.P.; Noseworthy, J.; Carriere, W.; Baskerville, J.; Ebers, G.C. The natural history of multiple sclerosis: A geographically based study. I. Clinical course and disability. Brain 1989, 112 Pt 1, 133–146. [Google Scholar] [CrossRef]
- Runmarker, B.; Andersen, O. Prognostic factors in a multiple sclerosis incidence cohort with twenty-five years of follow-up. Brain 1993, 116 Pt 1, 117–134. [Google Scholar] [CrossRef]
- Carotenuto, A.; Signoriello, E.; Lanzillo, R.; Vaia, Y.; Moccia, M.; Bonavita, S.; Lus, G.; Brescia Morra, V. Unraveling diagnostic uncertainty in transition phase from relapsing-remitting to secondary progressive multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 43, 102211. [Google Scholar] [CrossRef]
- Capasso, N.; Nozzolillo, A.; Scalia, G.; Lanzillo, R.; Carotenuto, A.; De Angelis, M.; Petruzzo, M.; Sacca, F.; Russo, C.V.; Brescia Morra, V.; et al. Ocrelizumab depletes T-lymphocytes more than rituximab in multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 49, 102802. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Total Population | Patients with at Least 1 Year Follow-Up | p-Value | |
|---|---|---|---|
| Number of subjects | 383 | 217 | |
| Sex | |||
| Male, N (%) | 178 (46.5) | 115 (53) | 0.13 |
| Female, N (%) | 205 (53.5) | 102 (47) | |
| Age, mean (SD) (years) | 45.8 (11.2) | 46.6 (10.6) | 0.37 |
| ARR pre-OCR start, mean (SD) | 0.29 (0.3) | 0.28 (0.33) | 0.72 |
| EDSS 1 year pre-OCR start, median (Range) | 5 (0–8) | 5.25 (1–8) | 0.39 |
| EDSS at OCR start, median (Range) | 5.5 (1–8.5) | 5.5 (1–8.5) | 0.27 |
| Disease duration, median (Range) (years) | 11 (0–41) | 11 (1–41) | 0.76 |
| MS course | |||
| Relapsing-remitting, N (%) | 89 (23) | 32 (15) | 0.04 * |
| Active secondary progressive, N (%) | 165 (43) | 100 (46) | |
| Primary progressive, N (%) | 129 (34) | 85 (39) | |
| Previous Therapy | |||
| First-line, N (%) | 154 (40.2) | 96 (44) | 0.78 |
| Second-line, N (%) | 155 (40.5) | 80 (37) | |
| Naïve, N (%) | 74 (19.3) | 41 (19) | |
| Ocrelizumab courses, median (Range) | 2 (1–5) | 4 (2–5) | <0.001 * |
| Features | Number | EDSS (Mean [SD]) | ||||
|---|---|---|---|---|---|---|
| T−1 | T0 | T1 | p-Value (T0 vs. T−1) | p-Value (T1 vs. T0) | ||
| Sex | ||||||
| Male | 115 | 4.9 (1.8) | 5.1 (1.7) | 5.2 (1.8) | <0.001 * | 0.08 |
| Female | 102 | 5.1 (1.7) | 5.3 (1.6) | 5.2 (1.8) | <0.001 * | 0.26 |
| Age | ||||||
| <40 years | 63 | 4.0 (2.0) | 4.3 (2.0) | 4.5 (2.2) | <0.001 * | 0.10 |
| ≥40 years | 154 | 5.3 (1.4) | 5.5 (1.4) | 5.5 (1.5) | <0.001 * | 0.78 |
| Disease duration | ||||||
| <10 years | 94 | 4.2 (1.8) | 4.6 (1.8) | 4.5 (1.9) | <0.001 * | 0.23 |
| ≥10 years | 123 | 5.4 (1.5) | 5.7 (1.4) | 5.8 (1.5) | 0.002 * | 0.05 |
| EDSS at T0 | ||||||
| <4 | 38 | 2.3 (1.2) | 2.4 (1.0) | 2.4 (1.5) | 0.96 | 0.88 |
| ≥4 | 179 | 5.5 (1.3) | 5.8 (1.1) | 5.8 (1.5) | <0.001 * | 0.65 |
| Previous Therapy | ||||||
| Naïve | 41 | - | 4.6 (1.6) | 4.4 (1.9) | - | 0.004 * |
| Non-naïve | 176 | 5.1 (1.7) | 5.3 (1.7) | 5.4 (1.7) | <0.001 * | 0.09 |
| MS course | ||||||
| Relapsing-remitting | 32 | 2.7 (1.7) | 2.7 (1.6) | 2.5 (1.5) | 0.60 | 0.08 |
| Progressive | 185 | 5.4 (1.4) | 5.6 (1.3) | 5.7 (1.4) | <0.001 * | 0.21 |
| Progressive MS course | ||||||
| Active secondary progressive MS | 100 | 5.5 (1.4) | 5.8 (1.4) | 6.0 (1.4) | <0.001* | 0.009* |
| Primary progressive MS | 85 | 5.0 (0.1) | 5.4 (0.1) | 5.4 (0.1) | <0.001* | 0.87 |
| Time from conversion | ||||||
| ≤2 years | 24 | 4.9 (1.2) | 5.5 (1.1) | 5.5 (1.3) | 0.006 * | 0.94 |
| >2 years | 66 | 5.8 (1.5) | 6.0 (1.5) | 6.2 (1.4) | 0.10 | 0.002 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lanzillo, R.; Carotenuto, A.; Signoriello, E.; Iodice, R.; Miele, G.; Bisecco, A.; Maniscalco, G.T.; Sinisi, L.; Romano, F.; Di Gregorio, M.; et al. Prognostic Markers of Ocrelizumab Effectiveness in Multiple Sclerosis: A Real World Observational Multicenter Study. J. Clin. Med. 2022, 11, 2081. https://doi.org/10.3390/jcm11082081
Lanzillo R, Carotenuto A, Signoriello E, Iodice R, Miele G, Bisecco A, Maniscalco GT, Sinisi L, Romano F, Di Gregorio M, et al. Prognostic Markers of Ocrelizumab Effectiveness in Multiple Sclerosis: A Real World Observational Multicenter Study. Journal of Clinical Medicine. 2022; 11(8):2081. https://doi.org/10.3390/jcm11082081
Chicago/Turabian StyleLanzillo, Roberta, Antonio Carotenuto, Elisabetta Signoriello, Rosa Iodice, Giuseppina Miele, Alvino Bisecco, Giorgia Teresa Maniscalco, Leonardo Sinisi, Felice Romano, Maria Di Gregorio, and et al. 2022. "Prognostic Markers of Ocrelizumab Effectiveness in Multiple Sclerosis: A Real World Observational Multicenter Study" Journal of Clinical Medicine 11, no. 8: 2081. https://doi.org/10.3390/jcm11082081
APA StyleLanzillo, R., Carotenuto, A., Signoriello, E., Iodice, R., Miele, G., Bisecco, A., Maniscalco, G. T., Sinisi, L., Romano, F., Di Gregorio, M., Lavorgna, L., Trojsi, F., Moccia, M., Fratta, M., Capasso, N., Dubbioso, R., Petracca, M., Spiezia, A. L., Gallo, A., ... Brescia Morra, V. (2022). Prognostic Markers of Ocrelizumab Effectiveness in Multiple Sclerosis: A Real World Observational Multicenter Study. Journal of Clinical Medicine, 11(8), 2081. https://doi.org/10.3390/jcm11082081