
Risk of Mortality among Patients with Gastrointestinal Bleeding with Early and Late Treatment with Tranexamic Acid: A Population-Based Cohort Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
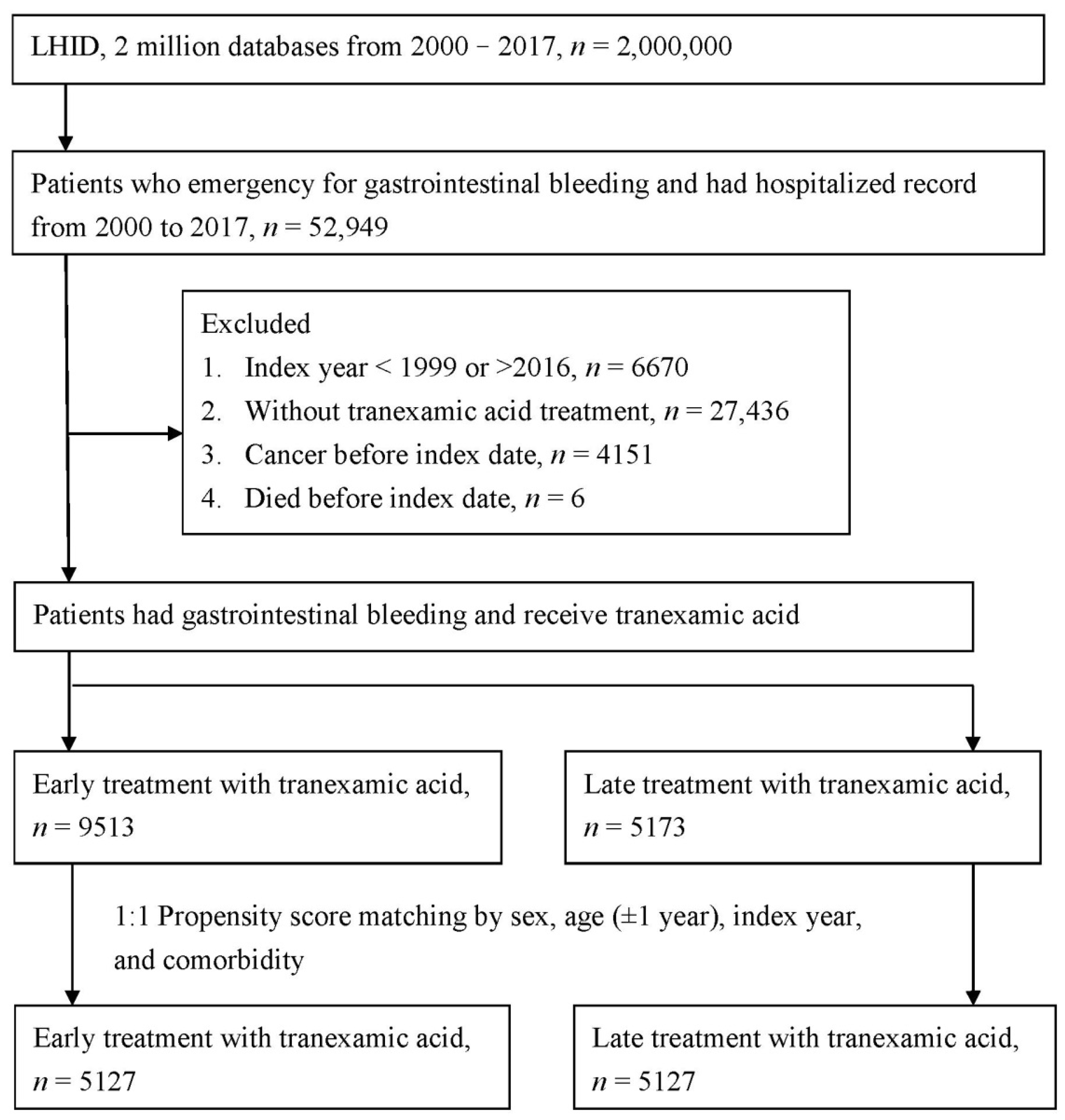
2.1. Study Design and Population
2.2. Study Population
2.3. Characteristics, Comorbidities, and Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
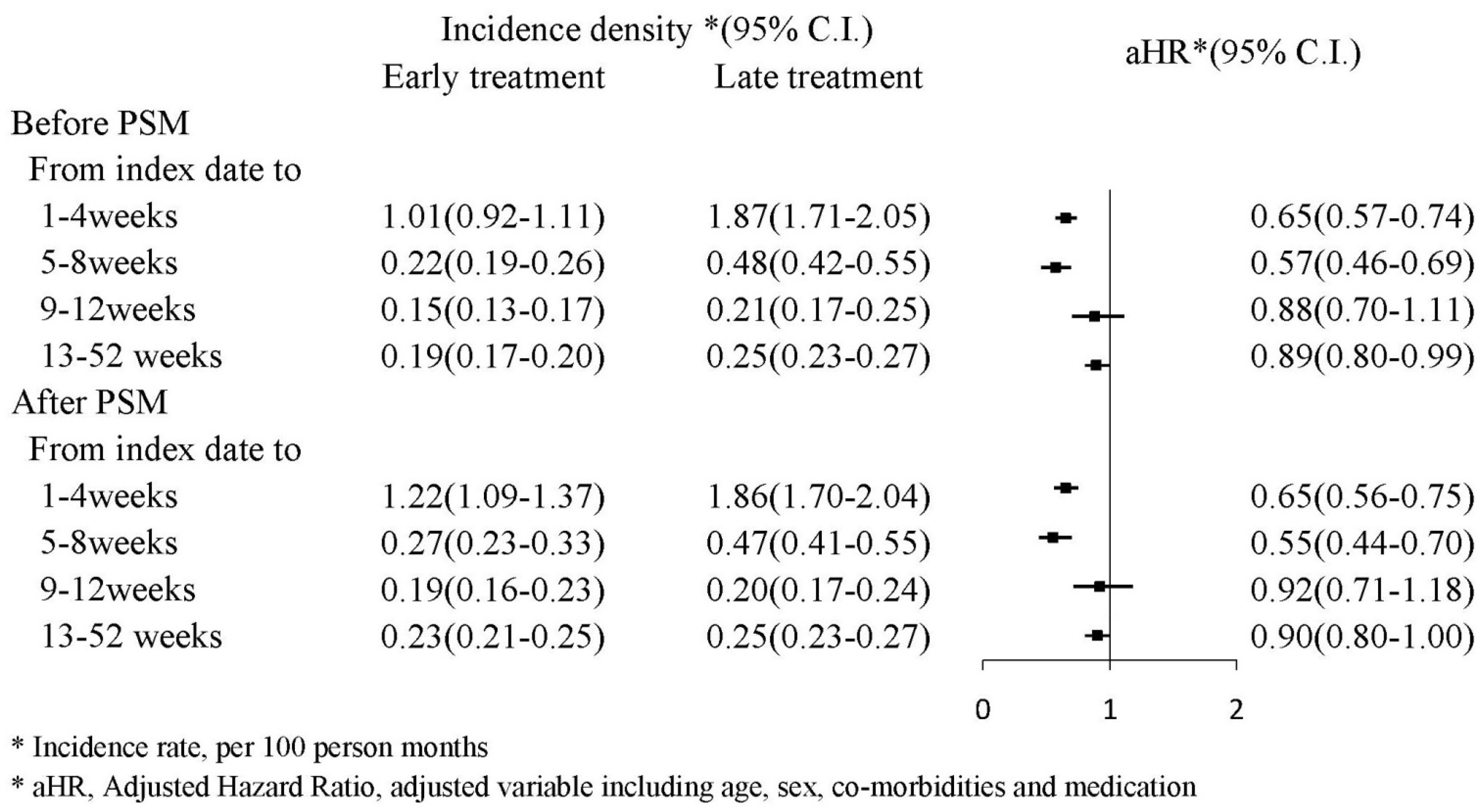
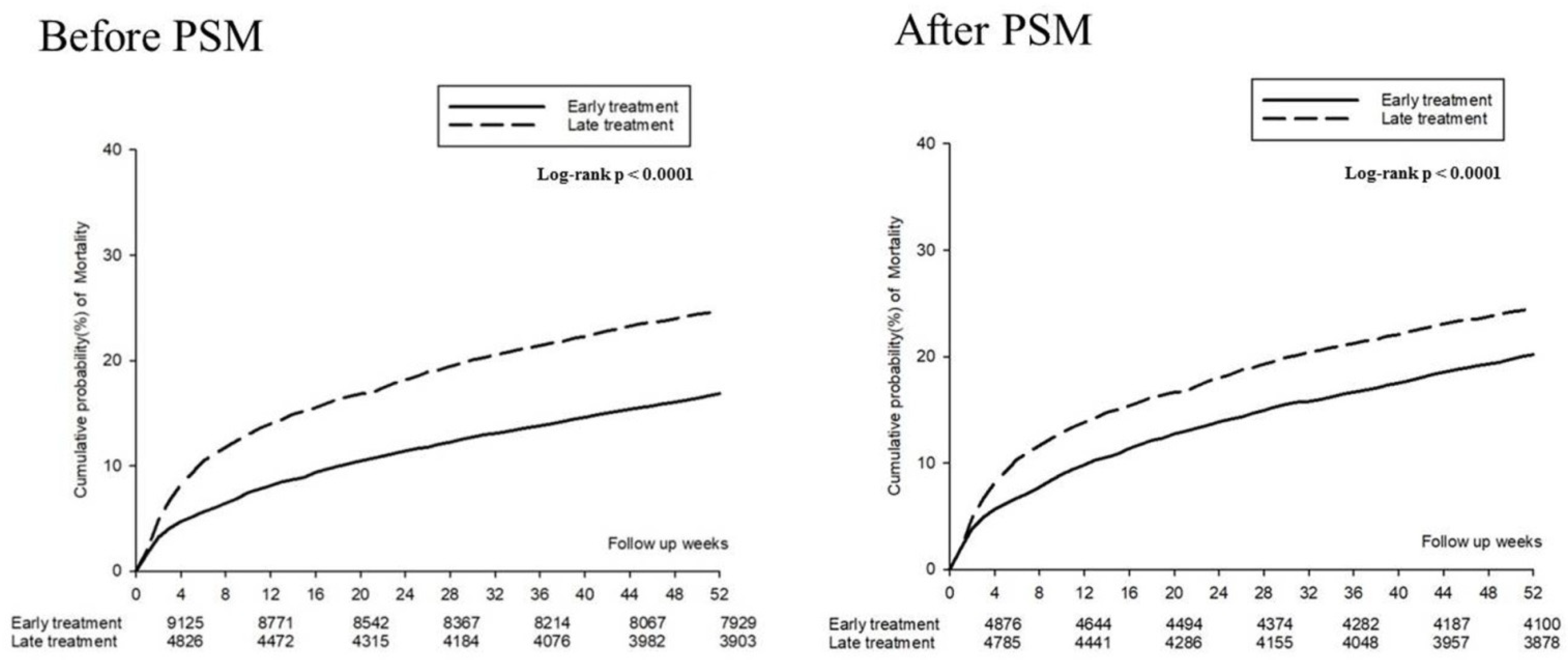
3.2. The Risk of Mortality in the TXA Treatment Group
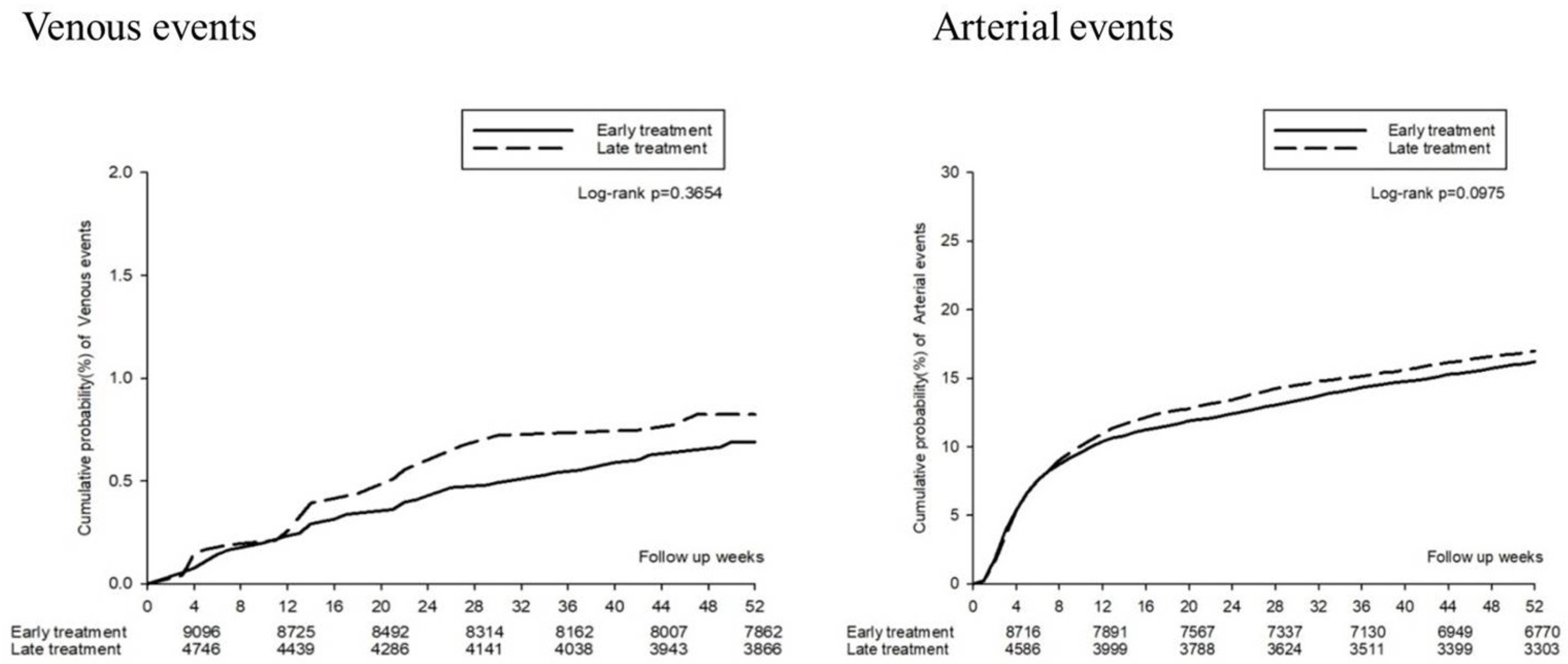
3.3. Thromboembolic Events in the TXA Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Leerdam, M.E. Epidemiology of acute upper gastrointestinal bleeding. Best Pract. Res. Clin. Gastroenterol. 2008, 22, 209–224. [Google Scholar] [CrossRef] [PubMed]
- Rockall, T.A.; Logan, R.F.A.; Devlin, H.B.; Northfield, T.C. Incidence of and mortality from acute upper gastrointestinal haemorrhage in the United Kingdom. BMJ 1995, 311, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Sostres, C.; Lanas, A. Epidemiology and Demographics of Upper Gastrointestinal Bleeding: Prevalence, Incidence, and Mortality. Gastrointest. Endosc. Clin. N. Am. 2011, 21, 567–581. [Google Scholar] [CrossRef] [PubMed]
- Vermylen, J.; Verhaegen-Declercq, M.L.; Fierens, F.; Verstraete, M. A double blind study of the effect of tranexamic acid in essential menorrhagia. Bull. Soc. R. Belg. Gynecol. Obs. 1968, 38, 385–390. [Google Scholar] [CrossRef]
- Brown, J.R.; Birkmeyer, N.J.; O’Connor, G.T. Meta-analysis comparing the effectiveness and adverse outcomes of antifibrinolytic agents in cardiac surgery. Circulation 2007, 115, 2801–2813. [Google Scholar] [CrossRef] [PubMed]
- Myles, P.S.; Smith, J.A.; Forbes, A.; Silbert, B.; Jayarajah, M.; Painter, T.; Cooper, D.J.; Marasco, S.; McNeil, J.; Bussières, J.S.; et al. Tranexamic Acid in Patients Undergoing Coronary-Artery Surgery. N. Engl. J. Med. 2016, 376, 136–148. [Google Scholar] [CrossRef]
- Shakur, H.; Roberts, I.; Fawole, B.; Chaudhri, R.; El-Sheikh, M.; Akintan, A.; Qureshi, Z.; Kidanto, H.; Vwalika, B.; Abdulkadir, A.; et al. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): An international, randomised, double-blind, placebo-controlled trial. Lancet 2017, 389, 2105–2116. [Google Scholar] [CrossRef] [Green Version]
- The CRASH-3 Trial Collaborators. Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): A randomised, placebo-controlled trial. Lancet 2019, 394, 1713–1723. [Google Scholar] [CrossRef] [Green Version]
- Barer, D.; Ogilvie, A.; Henry, D.; Dronfield, M.; Coggon, D.; French, S.; Ellis, S.; Atkinson, M.; Langman, M. Cimetidine and tranexamic acid in the treatment of acute upper-gastrointestinal-tract bleeding. N. Engl. J. Med. 1983, 308, 1571–1575. [Google Scholar] [CrossRef]
- Bennett, C.; Klingenberg, S.L.; Langholz, E.; Gluud, L.L. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst. Rev. 2014, 2014, Cd006640. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.-L.; Yang, K.-S.; Tsai, H.-W.; Hou, S.-K.; Kang, Y.-N.; Chang, C.-C. Tranexamic acid for gastrointestinal bleeding: A systematic review with meta-analysis of randomized clinical trials. Am. J. Emerg. Med. 2021, 45, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, H.-I.T. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): An international randomised, double-blind, placebo-controlled trial. Lancet 2020, 395, 1927–1936. [Google Scholar] [CrossRef]
- Smith, S.R.; Murray, D.; Pockney, P.G.; Bendinelli, C.; Draganic, B.D.; Carroll, R. Tranexamic Acid for Lower GI Hemorrhage: A Randomized Placebo-Controlled Clinical Trial. Dis. Colon Rectum 2018, 61, 99–106. [Google Scholar] [CrossRef]
- Burke, E.; Harkins, P.; Ahmed, I. Is There a Role for Tranexamic Acid in Upper GI Bleeding? A Systematic Review and Meta-Analysis. Surg. Res. Pract. 2021, 2021, 8876991. [Google Scholar] [CrossRef]
- Gayet-Ageron, A.; Prieto-Merino, D.; Ker, K.; Shakur, H.; Ageron, F.-X.; Roberts, I.; Kayani, A.; Geer, A.; Ndungu, B.; Fawole, B.; et al. Effect of treatment delay on the effectiveness and safety of antifibrinolytics in acute severe haemorrhage: A meta-analysis of individual patient-level data from 40 138 bleeding patients. Lancet 2018, 391, 125–132. [Google Scholar] [CrossRef] [Green Version]
- Gralnek, I.M.; Dumonceau, J.-M.; Kuipers, E.J.; Lanas, A.; Sanders, D.S.; Kurien, M.; Rotondano, G.; Hucl, T.; Dinis-Ribeiro, M.; Marmo, R.; et al. Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015, 47, a1–a46. [Google Scholar] [CrossRef] [Green Version]
- Stanley, A.J.; Laine, L. Management of acute upper gastrointestinal bleeding. BMJ 2019, 364, l536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavakoli, N.; Mokhtare, M.; Agah, S.; Azizi, A.; Masoodi, M.; Amiri, H.; Sheikhvatan, M.; Syedsalehi, B.; Behnam, B.; Arabahmadi, M.; et al. Comparison of the efficacy of intravenous tranexamic acid with and without topical administration versus placebo in urgent endoscopy rate for acute gastrointestinal bleeding: A double-blind randomized controlled trial. United Eur. Gastroenterol. J. 2017, 6, 46–54. [Google Scholar] [CrossRef]
- Miyamoto, Y.; Ohbe, H.; Ishimaru, M.; Matsui, H.; Fushimi, K.; Yasunaga, H. Effect of tranexamic acid in patients with colonic diverticular bleeding: A nationwide inpatient database study. J. Gastroenterol. Hepatol. 2021, 36, 999–1005. [Google Scholar] [CrossRef]
- GnanaDev, R.; Dong, F.; Ali, A.; Makkar, G.; Esiobu, P.; Vara, R.; Wong, D.; Neeki, M. RS12. Comparing Mortality and Hospital Length of Stay in the Setting of Truncal and Peripheral Vascular Trauma in Patients Treated with Tranexamic Acid on Initial Presentation. J. Vasc. Surg. 2019, 69, e188–e189. [Google Scholar] [CrossRef] [Green Version]
- Saad, B.N.; Menken, L.G.; Elkattaway, S.; Liporace, F.A.; Yoon, R.S. Tranexamic acid lowers transfusion requirements and hospital length of stay following revision total hip or knee arthroplasty. Patient Saf. Surg. 2021, 15, 21. [Google Scholar] [CrossRef]
- Calapai, G. Systematic Review of Tranexamic Acid Adverse Reactions. J. Pharmacovigil. 2015, 3, 171. [Google Scholar] [CrossRef]
- Murdaca, G.; Greco, M.; Vassallo, C.; Gangemi, S. Tranexamic acid adverse reactions: A brief summary for internists and emergency doctors. Clin. Mol. Allergy 2020, 18, 16. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.E.; Button, L.A.; Williams, J.G. Prognosis following Upper Gastrointestinal Bleeding. PLoS ONE 2012, 7, e49507. [Google Scholar] [CrossRef] [PubMed]
- Hágendorn, R.; Farkas, N.; Vincze, Á.; Gyöngyi, Z.; Csupor, D.; Bajor, J.; Erőss, B.; Csécsei, P.; Vasas, A.; Szakács, Z.; et al. Chronic kidney disease severely deteriorates the outcome of gastrointestinal bleeding: A meta-analysis. World J. Gastroenterol. 2017, 23, 8415–8425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, I. Tranexamic acid in trauma: How should we use it? J. Thromb. Haemost. 2015, 13, S195–S199. [Google Scholar] [CrossRef] [PubMed]
- Wellington, K.; Wagstaff, A.J. Tranexamic Acid. Drugs 2003, 63, 1417–1433. [Google Scholar] [CrossRef]
- Cheriyan, T.; Maier, S.P., II; Bianco, K.; Slobodyanyuk, K.; Rattenni, R.N.; Lafage, V.; Schwab, F.J.; Lonner, B.S.; Errico, T.J. Efficacy of tranexamic acid on surgical bleeding in spine surgery: A meta-analysis. Spine J. 2015, 15, 752–761. [Google Scholar] [CrossRef]
- Ker, K.; Edwards, P.; Perel, P.; Shakur, H.; Roberts, I. Effect of tranexamic acid on surgical bleeding: Systematic review and cumulative meta-analysis. BMJ Br. Med. J. 2012, 344, e3054. [Google Scholar] [CrossRef] [Green Version]
- Sprigg, N.; Flaherty, K.; Appleton, J.P.; Salman, R.A.-S.; Bereczki, D.; Beridze, M.; Christensen, H.; Ciccone, A.; Collins, R.; Czlonkowska, A.; et al. Tranexamic acid for hyperacute primary IntraCerebral Haemorrhage (TICH-2): An international randomised, placebo-controlled, phase 3 superiority trial. Lancet 2018, 391, 2107–2115. [Google Scholar] [CrossRef] [Green Version]
- Hu, W.; Xin, Y.; Chen, X.; Song, Z.; He, Z.; Zhao, Y. Tranexamic Acid in Cerebral Hemorrhage: A Meta-Analysis and Systematic Review. CNS Drugs 2019, 33, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Rowell, S.E.; Meier, E.N.; McKnight, B.; Kannas, D.; May, S.; Sheehan, K.; Bulger, E.M.; Idris, A.H.; Christenson, J.; Morrison, L.J.; et al. Effect of Out-of-Hospital Tranexamic Acid vs Placebo on 6-Month Functional Neurologic Outcomes in Patients with Moderate or Severe Traumatic Brain Injury. JAMA 2020, 324, 961–974. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before PSM | After PSM | |||||
|---|---|---|---|---|---|---|
| Early Treatment | Late Treatment | ASD | Early Treatment | Late Treatment | ASD | |
| N | 9513 | 5173 | 5127 | 5127 | ||
| Index year | 0.2488 | 0.0239 | ||||
| 2000–2005 | 2064 (21.70%) | 1596 (30.85%) | 1516 (29.57%) | 1551 (30.25%) | ||
| 2006–2010 | 2996 (31.49%) | 1692 (32.71%) | 1747 (34.07%) | 1691 (32.98%) | ||
| 2011–2015 | 4453 (46.81%) | 1885 (36.44%) | 1864 (36.36%) | 1885 (36.77%) | ||
| Sex | 0.0025 | 0.0042 | ||||
| Female | 3060 (32.17%) | 1658 (32.05%) | 1633 (31.85%) | 1643 (32.05%) | ||
| Male | 6453 (67.83%) | 3515 (67.95%) | 3494 (68.15%) | 3484 (67.95%) | ||
| Age | 0.0405 | 0.0000 | ||||
| ≤50 | 2443 (25.68%) | 1277 (24.69%) | 1289 (25.14%) | 1268 (24.73%) | ||
| 51–70 | 3060 (32.17%) | 1591 (30.76%) | 1570 (30.62%) | 1583 (30.88%) | ||
| ≥71 | 4010 (42.15%) | 2305 (44.56%) | 2268 (44.24%) | 2276 (44.39%) | ||
| CCI score | 0.0885 | 0.0263 | ||||
| 0 | 2225 (23.39%) | 1009 (19.51%) | 1043 (20.34%) | 1006 (19.62%) | ||
| 1 | 2564 (26.95%) | 1340 (25.90%) | 1265 (24.67%) | 1332 (25.98%) | ||
| 2 | 1848 (19.43%) | 1101 (21.28%) | 1056 (20.6%) | 1088 (21.22%) | ||
| ≥3 | 2876 (30.23%) | 1723 (33.31%) | 1763 (34.39%) | 1701 (33.18%) | ||
| Co-morbidity | ||||||
| Hypertension | 4608 (48.44%) | 2518 (48.68%) | 0.0047 | 2494 (48.64%) | 2495 (48.66%) | 0.0004 |
| Diabetes mellitus | 2862 (30.09%) | 1577 (30.49%) | 0.0087 | 1565 (30.52%) | 1564 (30.51%) | 0.0004 |
| Hyperlipidemia | 1373 (14.43%) | 652 (12.60%) | 0.0535 | 637 (12.42%) | 650 (12.68%) | 0.0077 |
| Kidney disease | 1441 (15.15%) | 965 (18.65%) | 0.0937 | 940 (18.33%) | 946 (18.45%) | 0.0030 |
| Chronic pulmonary diseases | 1715 (18.03%) | 1086 (20.99%) | 0.0749 | 1023 (19.95%) | 1065 (20.77%) | 0.0203 |
| Liver disease | 3233 (33.99%) | 1858 (35.92%) | 0.0405 | 1880 (36.67%) | 1840 (35.89%) | 0.0162 |
| Ischemic heart diseases | 1598 (16.80%) | 839 (16.22%) | 0.0156 | 810 (15.80%) | 834 (16.27%) | 0.0128 |
| Ischemic stroke | 1045 (10.98%) | 615 (11.89%) | 0.0284 | 634 (12.37%) | 606 (11.82%) | 0.0167 |
| Hemorrhage stroke | 239 (2.51%) | 170 (3.29%) | 0.0461 | 161 (3.14%) | 166 (3.24%) | 0.0055 |
| Atrial fibrillation | 487 (5.12%) | 258 (4.99%) | 0.0060 | 252 (4.92%) | 257 (5.01%) | 0.0045 |
| Congestive heart failure | 1103 (11.59%) | 667 (12.89%) | 0.0396 | 647 (12.62%) | 656 (12.80%) | 0.0053 |
| Dementia | 631 (6.63%) | 384 (7.42%) | 0.0309 | 386 (7.53%) | 380 (7.41%) | 0.0045 |
| Peripheral vascular disease | 434 (4.56%) | 213 (4.12%) | 0.0218 | 198 (3.86%) | 212 (4.13%) | 0.0139 |
| Medication | ||||||
| Proton-pump inhibitors | 8140 (85.57%) | 4430 (85.64%) | 0.0020 | 4403 (85.88%) | 4389 (85.61%) | 0.0078 |
| Hemostatic | 3237 (34.03%) | 2085 (40.31%) | 0.1302 | 2069 (40.35%) | 2049 (39.96%) | 0.0080 |
| Drugs for constipation | 5973 (62.79%) | 3554 (68.70%) | 0.1249 | 3489 (68.05%) | 3508 (68.42%) | 0.0080 |
| Furosemide | 3329 (34.99%) | 2326 (44.96%) | 0.2046 | 2291 (44.69%) | 2283 (44.53%) | 0.0031 |
| Metoclopramide | 4008 (42.13%) | 2598 (50.22%) | 0.1628 | 2564 (50.01%) | 2553 (49.80%) | 0.0043 |
| Silicon | 4157 (43.70%) | 2539 (49.08%) | 0.1081 | 2502 (48.80%) | 2500 (48.76%) | 0.0008 |
| Magnesium oxide | 1512 (15.89%) | 910 (17.59%) | 0.0455 | 887 (17.30%) | 890 (17.36%) | 0.0016 |
| Aspirin | 2833 (29.78%) | 1744 (33.71%) | 0.0846 | 1679 (32.75%) | 1708 (33.31%) | 0.0120 |
| Clopidogrel/Ticagrelor | 772 (8.12%) | 398 (7.69%) | 0.0156 | 392 (7.65%) | 397 (7.74%) | 0.0037 |
| NSAIDs | 6403 (67.31%) | 3638 (70.33%) | 0.0652 | 3603 (70.28%) | 3598 (70.18%) | 0.0021 |
| Variable | aHR (95% CI) | |
|---|---|---|
| 1–8 Weeks | 9–52 Weeks | |
| Study group | ||
| Early treatment | 0.64 (0.57–0.73) | 0.90 (0.80–1.00) |
| Late treatment | Reference | Reference |
| Index year | ||
| 2000–2005 | Reference | Reference |
| 2006–2010 | 1.23 (1.05–1.45) | 0.98 (0.85–1.14) |
| 2011–2015 | 1.12 (0.95–1.32) | 1.04 (0.90–1.20) |
| Sex | ||
| Female | Reference | Reference |
| Male | 1.09 (0.95–1.25) | 1.24 (1.10–1.40) |
| Age | ||
| ≤50 | Reference | Reference |
| 51–70 | 1.18 (0.96–1.45) | 0.98 (0.81–1.18) |
| ≥71 | 2.09 (1.70–2.57) | 1.81 (1.51–2.18) |
| Co-morbidity (ref: non) | ||
| Hypertension | 0.74 (0.64–0.85) | 0.94 (0.83–1.07) |
| Diabetes mellitus | 1.07 (0.93–1.23) | 1.24 (1.10–1.39) |
| Hyperlipidemia | 0.76 (0.61–0.94) | 0.73 (0.61–0.88) |
| Kidney disease | 1.41 (1.21–1.63) | 1.52 (1.34–1.73) |
| Chronic pulmonary diseases | 1.09 (0.94–1.26) | 1.22 (1.08–1.39) |
| Liver disease | 1.32 (1.14–1.52) | 1.48 (1.31–1.68) |
| Ischemic heart diseases | 0.95 (0.79–1.13) | 0.86 (0.73–1.00) |
| Ischemic stroke | 1.01 (0.84–1.21) | 1.05 (0.90–1.23) |
| Hemorrhage stroke | 1.88 (1.45–2.44) | 1.64 (1.27–2.11) |
| Atrial fibrillation | 0.88 (0.68–1.13) | 1.08 (0.88–1.33) |
| Congestive heart failure | 1.18 (0.99–1.40) | 1.11 (0.95–1.29) |
| Dementia | 1.17 (0.96–1.42) | 1.43 (1.21–1.69) |
| Peripheral vascular disease | 1.23 (0.94–1.61) | 1.09 (0.85–1.40) |
| Medication (ref: non) | ||
| Proton-pump inhibitors | 0.93 (0.75–1.14) | 1.00 (0.84–1.20) |
| Hemostatic | 1.95 (1.71–2.22) | 1.27 (1.13–1.42) |
| Drugs for constipation | 1.22 (1.02–1.45) | 2.32 (1.93–2.79) |
| Furosemide | 2.71 (2.32–3.16) | 2.41 (2.12–2.74) |
| Metoclopramide | 1.43 (1.25–1.64) | 1.50 (1.33–1.69) |
| Silicon | 0.85 (0.75–0.97) | 0.97 (0.87–1.09) |
| magnesium oxide | 0.95 (0.81–1.12) | 0.92 (0.80–1.05) |
| Aspirin | 1.11 (0.97–1.28) | 1.06 (0.94–1.20) |
| Clopidogrel/Ticagrelor | 1.09 (0.87–1.36) | 1.27 (1.06–1.53) |
| NSAIDs | 0.93 (0.75–1.14) | 1.00 (0.84–1.20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ting, K.-H.; Shiu, B.-H.; Yang, S.-F.; Liao, P.-L.; Huang, J.-Y.; Chen, Y.-Y.; Yeh, C.-B. Risk of Mortality among Patients with Gastrointestinal Bleeding with Early and Late Treatment with Tranexamic Acid: A Population-Based Cohort Study. J. Clin. Med. 2022, 11, 1741. https://doi.org/10.3390/jcm11061741
Ting K-H, Shiu B-H, Yang S-F, Liao P-L, Huang J-Y, Chen Y-Y, Yeh C-B. Risk of Mortality among Patients with Gastrointestinal Bleeding with Early and Late Treatment with Tranexamic Acid: A Population-Based Cohort Study. Journal of Clinical Medicine. 2022; 11(6):1741. https://doi.org/10.3390/jcm11061741
Chicago/Turabian StyleTing, Ke-Hsin, Bei-Hao Shiu, Shun-Fa Yang, Pei-Lun Liao, Jing-Yang Huang, Yin-Yang Chen, and Chao-Bin Yeh. 2022. "Risk of Mortality among Patients with Gastrointestinal Bleeding with Early and Late Treatment with Tranexamic Acid: A Population-Based Cohort Study" Journal of Clinical Medicine 11, no. 6: 1741. https://doi.org/10.3390/jcm11061741
APA StyleTing, K.-H., Shiu, B.-H., Yang, S.-F., Liao, P.-L., Huang, J.-Y., Chen, Y.-Y., & Yeh, C.-B. (2022). Risk of Mortality among Patients with Gastrointestinal Bleeding with Early and Late Treatment with Tranexamic Acid: A Population-Based Cohort Study. Journal of Clinical Medicine, 11(6), 1741. https://doi.org/10.3390/jcm11061741