
Abnormal Intrinsic Functional Hubs in Corneal Ulcer: Evidence from a Voxel-Wise Degree Centrality Analysis

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. MRI Parameters
2.3. fMRI Data Processing
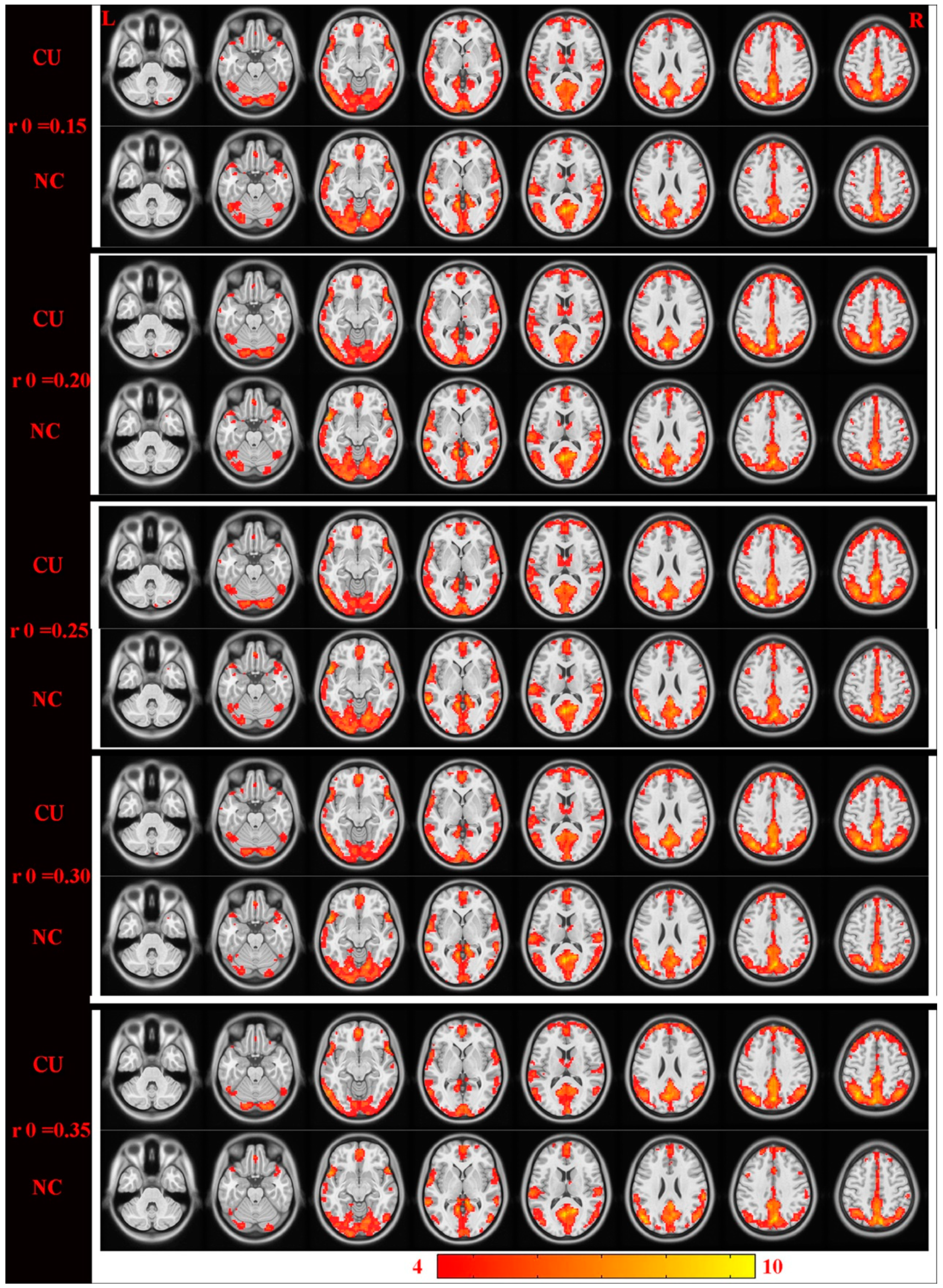
2.4. DC
2.5. Statistical Analysis
3. Results
3.1. Demographic Information and Visual Measurements
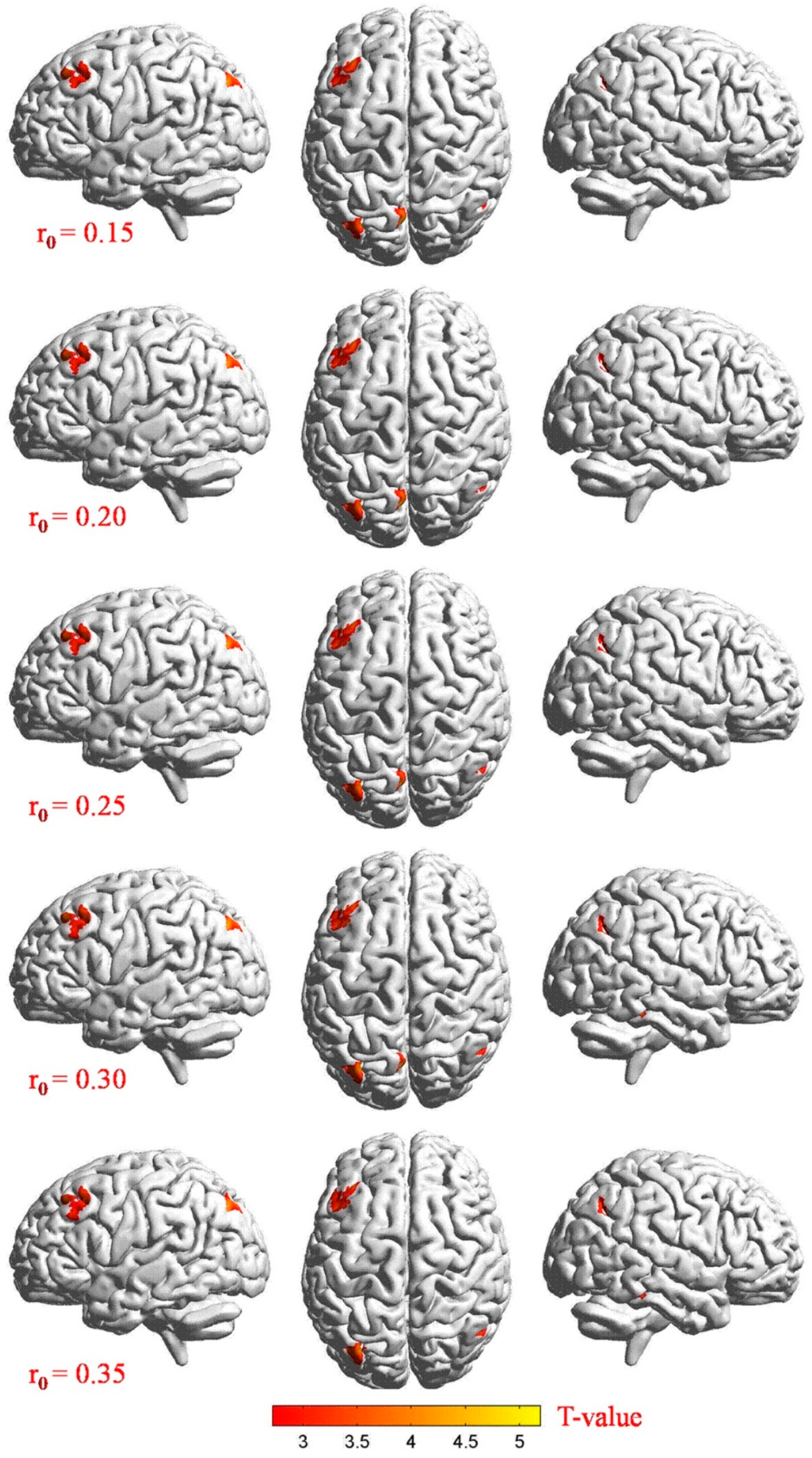
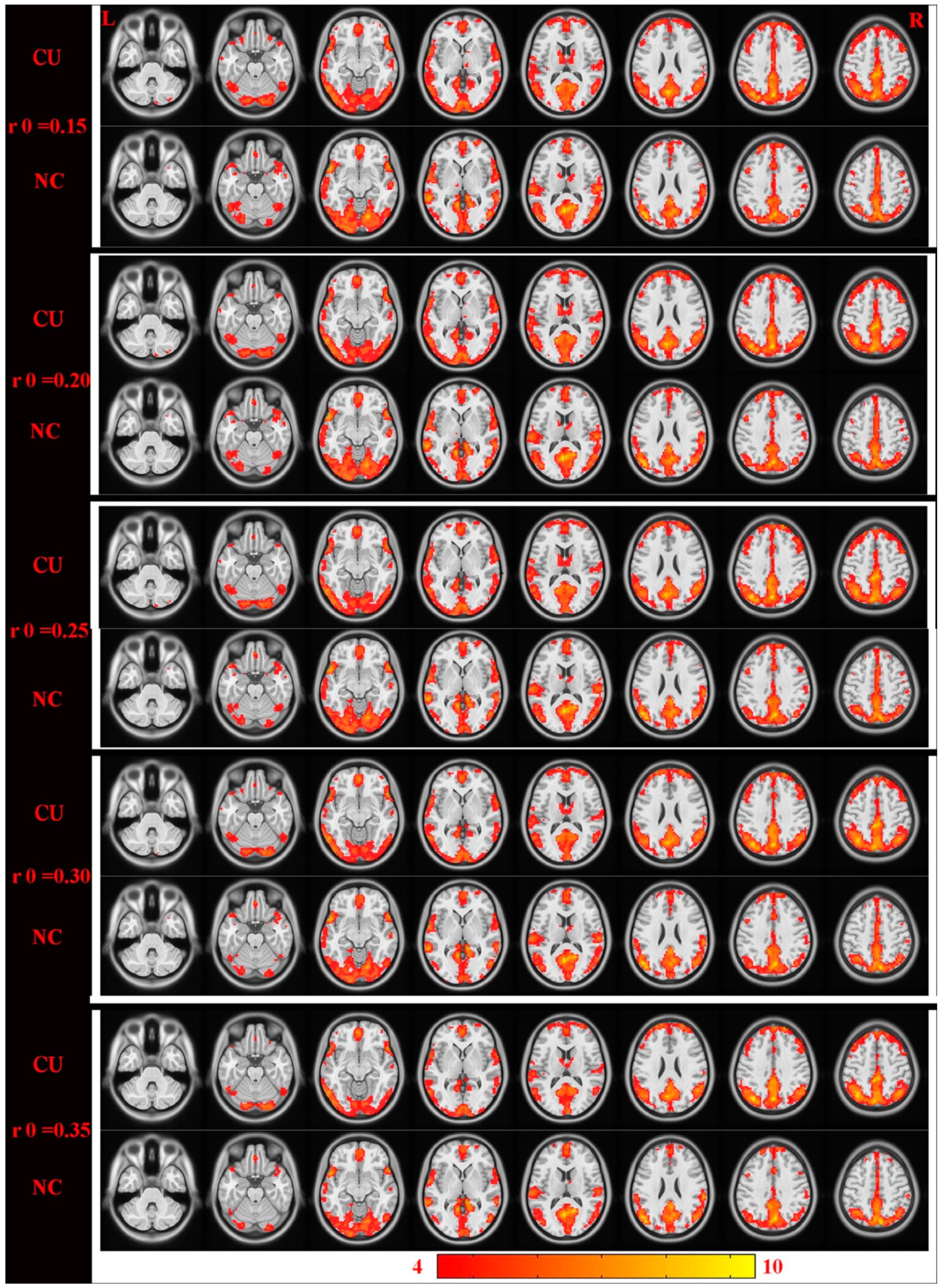
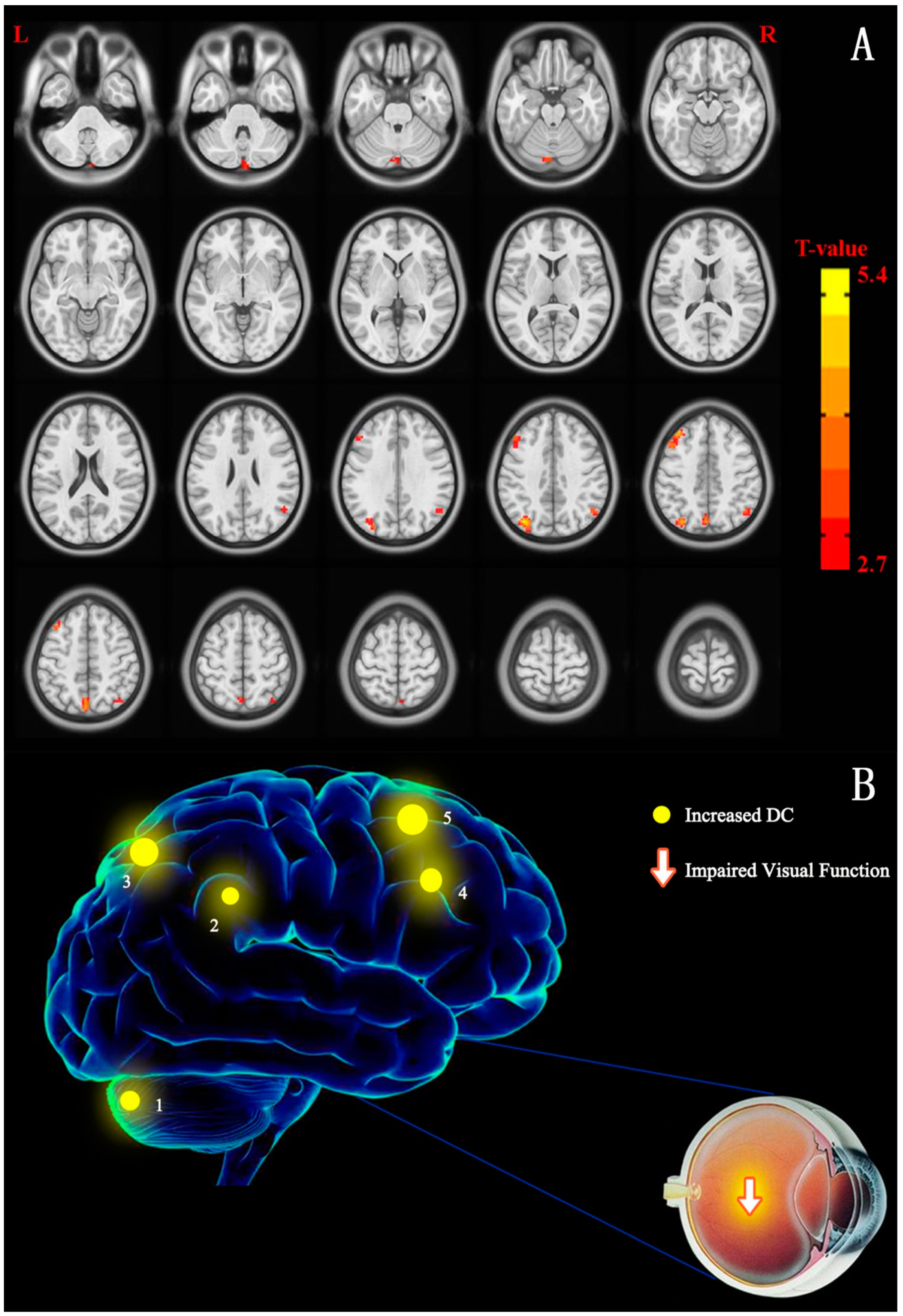
3.2. Differences in DC
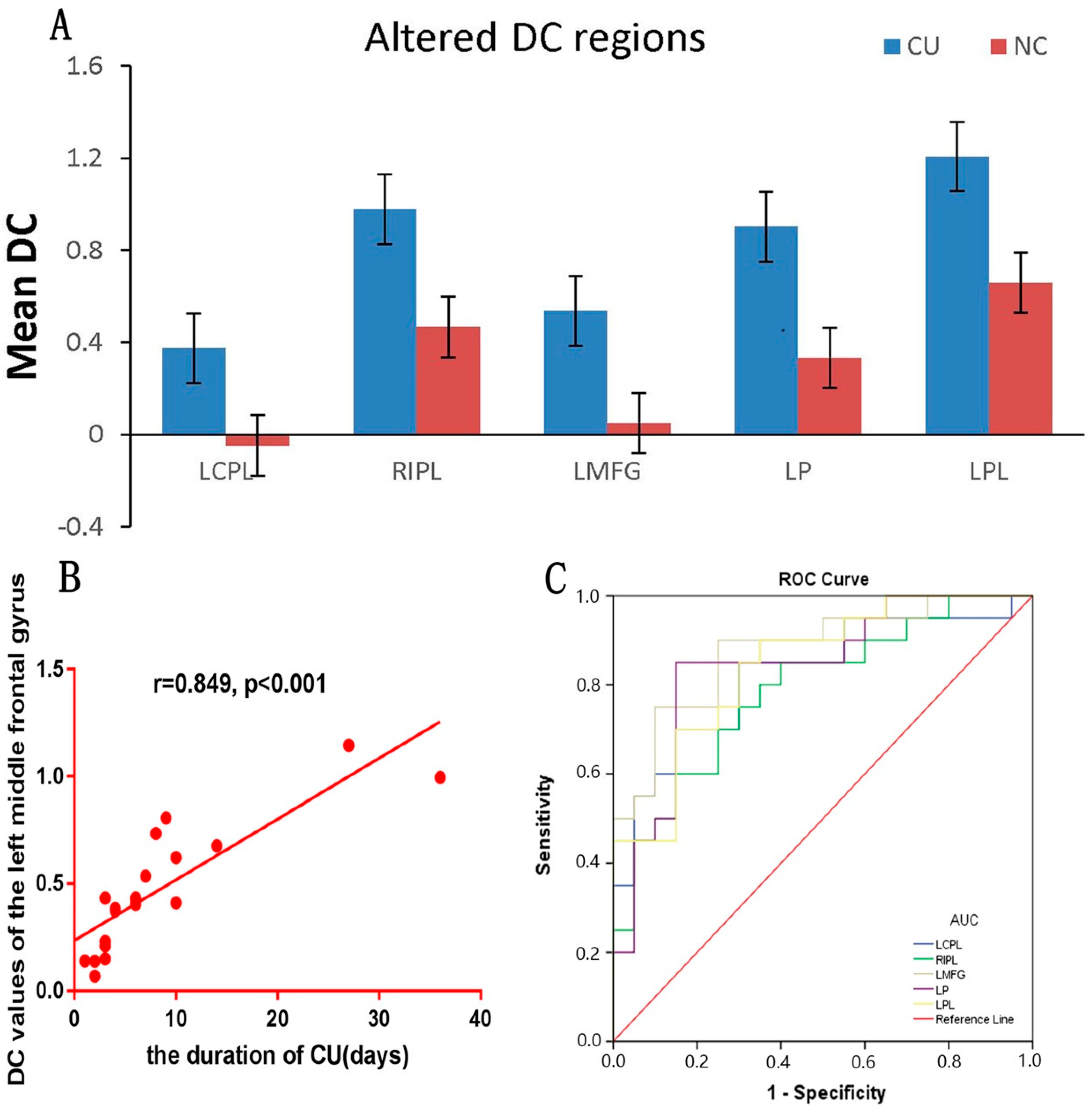
3.3. Correlation Analysis
3.4. Receiver Operating Characteristic (ROC) Curve
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Whitcher, J.P.; Srinivasan, M.; Upadhyay, M.P. Corneal blindness: A global perspective. Bull. World Health Organ. 2001, 79, 214–221. [Google Scholar] [PubMed]
- Vyas, H.; Patel, M. Microbiological study in cases of corneal ulcer and clinical outcome. Indian J. Clin. Exp. Ophthalmol. 2017, 3, 454–457. [Google Scholar]
- Lin, A.; Rhee, M.K.; Akpek, E.K.; Amescua, G.; Farid, M.; Garcia-Ferrer, F.J.; Varu, D.M.; Musch, D.C.; Dunn, S.P.; Mah, F.S. American Academy of Ophthalmology preferred practice pattern cornea and external disease panel. Bacterial keratitis preferred practice pattern®. Ophthalmology 2019, 126, P1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekiesińska-Figatowska, M.; Helwich, E.; Rutkowska, M.; Stankiewicz, J.; Terczyńska, I. Magnetic resonance imaging of neonates in the magnetic resonance compatible incubator. Arch. Med. Sci. 2016, 12, 1064–1070. [Google Scholar] [CrossRef] [Green Version]
- Courrier, E.; Lepine, T.; Hor, G.; Fournier, C.; He, Z.; Chikh, M.; Urrea, C.; Al Anazi, F.-F.; Thuret, G.; Gain, P. Size of the lesions of superficial punctate keratitis in dry eye syndrome observed with a slit lamp. Cornea 2016, 35, 1004–1007. [Google Scholar] [CrossRef]
- Borroni, D.; Rachwani-Anil, R.; González, J.M.S.; Rodríguez-Calvo-de-Mora, M.; de Lossada, C.R. Metagenome techniques to reduce diagnostic delay in Acanthamoeba keratitis. Rom. J. Ophthalmol. 2021, 65, 307–308. [Google Scholar] [CrossRef]
- Gallon, P.; Parekh, M.; Ferrari, S.; Fasolo, A.; Ponzin, D.; Borroni, D. Metagenomics in ophthalmology: Hypothesis or real prospective? Biotechnol. Rep. 2019, 23, e00355. [Google Scholar] [CrossRef]
- Borroni, D.; Romano, V.; Kaye, S.B.; Somerville, T.; Napoli, L.; Fasolo, A.; Gallon, P.; Ponzin, D.; Esposito, A.; Ferrari, S. Metagenomics in ophthalmology: Current findings and future prospectives. BMJ Open Ophthalmol. 2019, 4, e000248. [Google Scholar] [CrossRef]
- Ouyang, J.; Yang, L.; Huang, X.; Zhong, Y.-L.; Hu, P.-H.; Zhang, Y.; Pei, C.-G.; Shao, Y. The atrophy of white and gray matter volume in patients with comitant strabismus: Evidence from a voxel-based morphometry study. Mol. Med. Rep. 2017, 16, 3276–3282. [Google Scholar] [CrossRef] [Green Version]
- Shao, Y.; Huang, X.; Cai, F.-Q.; Hu, P.-H.; Zhong, Y.-L.; Zhang, Y.; Pei, C.-G.; Zhou, F.-Q.; Wei, R. Disturbed spontaneous brain-activity pattern in patients with optic neuritis using amplitude of low-frequency fluctuation: A functional magnetic resonance imaging study. Neuropsychiatr. Dis. Treat. 2015, 11, 3075–3083. [Google Scholar] [CrossRef] [Green Version]
- Di Martino, A.; Zuo, X.N.; Kelly, C.; Grzadzinski, R.; Mennes, M.; Schvarcz, A.; Rodman, J.; Lord, C.; Castellanos, F.X.; Milham, M.P. Shared and distinct intrinsic functional network centrality in autism and attention-deficit/hyperactivity disorder. Biol. Psychiatry 2013, 74, 623–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, I.G.; Jurado, M.Á.; Garolera, M.; Marqués-Iturria, I.; Horstmann, A.; Segura, B.; Pueyo, R.; Sender-Palacios, M.J.; Vernet-Vernet, M.; Villringer, A.; et al. Functional network centrality in obesity: A resting-state and task fMRI study. Psychiatry Res. Neuroimaging 2015, 233, 331–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lou, Y.; Huang, P.; Li, D.; Cen, Z.; Wang, B.; Gao, J.; Xuan, M.; Yu, H.; Zhang, M.; Luo, W. Altered brain network centrality in depressed Parkinson’s disease patients. Mov. Disord. 2015, 30, 1777–1784. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-C.; Cai, G.-Q.; Yang, Q.-C.; Li, B.; Ge, Q.-M.; Li, Q.-Y.; Shi, W.-Q.; Min, Y.-L.; Liang, R.-B.; Shao, Y. Brain functional connectivity changes in patients with acute eye pain: A resting-state functional magnetic resonance imaging (fMRI) study. Med. Sci. Monit. 2021, 27, 930588. [Google Scholar] [CrossRef]
- Cai, F.; Gao, L.; Gong, H.; Jiang, F.; Pei, C.; Zhang, X.; Zeng, X.; Huang, R. Network centrality of resting-state fMRI in primary angle-closure glaucoma before and after surgery. PLoS ONE 2015, 10, e0141389. [Google Scholar] [CrossRef]
- Hu, Y.X.; He, J.R.; Yang, B.; Huang, X.; Li, Y.P.; Zhou, F.Q.; Xu, X.X.; Zhong, Y.L.; Wang, J.; Wu, X.R. Abnormal resting-state functional network centrality in patients with high myopia: Evidence from a voxel-wise degree centrality analysis. Int. J. Ophthalmol. 2018, 11, 1814–1820. [Google Scholar]
- Herzfeld, D.J.; Kojima, Y.; Soetedjo, R.; Shadmehr, R. Encoding of action by the Purkinje cells of the cerebellum. Nature 2015, 526, 439–442. [Google Scholar] [CrossRef] [Green Version]
- Joshi, A.C.; Das, V.E. Muscimol inactivation of caudal fastigial nucleus and posterior interposed nucleus in monkeys with stra-bismus. J. Neurophysiol. 2013, 110, 1882–1891. [Google Scholar] [CrossRef] [Green Version]
- Strick, P.L.; Dum, R.P.; Fiez, J.A. Cerebellum and nonmotor function. Annu. Rev. Neurosci. 2009, 32, 413–434. [Google Scholar] [CrossRef] [Green Version]
- Adamaszek, M.; D’Agata, F.; Ferrucci, R.; Habas, C.; Keulen, S.; Kirkby, K.C.; Leggio, M.; Mariën, P.; Molinari, M.; Moulton, E.; et al. Consensus paper: Cerebellum and emotion. Cerebellum 2017, 16, 552–576. [Google Scholar] [CrossRef]
- Liu, W.; Liu, H.; Wei, D.; Sun, J.; Yang, J.; Meng, J.; Wang, L.; Qiu, J. Abnormal degree centrality of functional hubs associated with negative coping in older Chinese adults who lost their only child. Biol. Psychol. 2015, 112, 46–55. [Google Scholar] [CrossRef]
- Zhang, S.; Li, C.S.R. Functional clustering of the human inferior parietal lobule by whole-brain connectivity mapping of rest-ing-state functional magnetic resonance imaging signals. Brain Connect. 2014, 4, 53–69. [Google Scholar]
- Zhu, X.; Wang, X.; Xiao, J.; Liao, J.; Zhong, M.; Wang, W.; Yao, S. Evidence of a dissociation pattern in resting-state default mode network connectivity in first-episode, treatment-naive major depression patients. Biol. Psychiatry 2012, 71, 611–617. [Google Scholar] [CrossRef]
- Goffaux, P.; Girard-Tremblay, L.; Marchand, S.; Daigle, K.; Whittingstall, K. Individual differences in pain sensitivity vary as a function of precuneus reactivity. Brain Topogr. 2014, 27, 366–374. [Google Scholar] [CrossRef]
- Wallentin, M.; Weed, E.; Østergaard, L.; Mouridsen, K.; Roepstorff, A. Accessing the mental space—Spatial working memory processes for language and vision overlap in precuneus. Hum. Brain Mapp. 2008, 29, 524–532. [Google Scholar] [CrossRef] [Green Version]
- Wenderoth, N.; Debaere, F.; Sunaert, S.; Swinnen, S.P. The role of anterior cingulate cortex and precuneus in the coordination of motor behaviour. Eur. J. Neurosci. 2005, 22, 235–246. [Google Scholar] [CrossRef]
- Raichle, M.E.; MacLeod, A.M.; Snyder, A.Z.; Powers, W.J.; Gusnard, D.A.; Shulman, G.L. A default mode of brain function. Proc. Natl. Acad. Sci. USA 2001, 98, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Egner, T.; Monti, J.M.P.; Trittschuh, E.H.; Wieneke, C.A.; Hirsch, J.; Mesulam, M.-M. Neural integration of top-down spatial and feature-based information in visual search. J. Neurosci. 2008, 28, 6141–6151. [Google Scholar] [CrossRef] [Green Version]
- Moretti, D.V. Increase of EEG Alpha3/Alpha2 power ratio detects inferior parietal lobule atrophy in mild cognitive im-pairment. Curr. Alzheimer Res. 2018, 15, 443–451. [Google Scholar] [CrossRef]
- Reed, T.; Pierce, W.M., Jr.; Turner, D.M.; Markesbery, W.R.; Butterfield, D.A. Proteomic identification of nitrated brain proteins in early Alzheimer’s disease inferior parietal lobule. J. Cell. Mol. Med. 2009, 13, 2019–2029. [Google Scholar] [CrossRef]
- Sliwinska, M.W.; James, A.; Devlin, J.T. Inferior parietal lobule contributions to visual word recognition. J. Cogn. Neurosci. 2015, 27, 593–604. [Google Scholar] [CrossRef]
- Song, P.; Lin, H.; Liu, C.; Jiang, Y.; Lin, Y.; Xue, Q.; Xu, P.; Wang, Y. Transcranial magnetic stimulation to the middle frontal gyrus during attention modes induced dynamic module reconfiguration in brain networks. Front. Neuroinform. 2019, 13, 22. [Google Scholar] [CrossRef]
- Groenewold, N.A.; Opmeer, E.M.; de Jonge, P.; Aleman, A.; Costafreda, S.G. Emotional valence modulates brain functional abnormalities in depression: Evidence from a meta-analysis of fMRI studies. Neurosci. Biobehav. Rev. 2013, 37, 152–163. [Google Scholar] [CrossRef]
- Han, S.B.; Yang, H.K.; Hyon, J.Y.; Wee, W.R. Association of dry eye disease with psychiatric or neurological disorders in elderly patients. Clin. Interv. Aging 2017, 12, 785–792. [Google Scholar] [CrossRef] [Green Version]
- Ioannides, A.A.; Liu, L.; Poghosyan, V.; Saridis, G.A.; Gjedde, A.; Ptito, M.; Kupers, R. MEG reveals a fast pathway from somatosensory cortex to occipital areas via posterior parietal cortex in a blind subject. Front. Hum. Neurosci. 2013, 7, 429. [Google Scholar] [CrossRef] [Green Version]
- Felician, O.; Romaiguère, P.; Anton, J.-L.; Nazarian, B.; Roth, M.; Poncet, M.; Roll, J.-P. The role of human left superior parietal lobule in body part localization. Ann. Neurol. 2004, 55, 749–751. [Google Scholar] [CrossRef]
- Iacoboni, M.; Zaidel, E. Interhemispheric visuo-motor integration in humans: The role of the superior parietal cortex. Neuropsychologia 2004, 42, 419–425. [Google Scholar] [CrossRef]
- Caminiti, R.; Ferraina, S.; Johnson, P.B. The sources of visual information to the primate frontal lobe: A novel role for the superior parietal lobule. Cereb. Cortex 1996, 6, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Segal, E.; Petrides, M. The anterior superior parietal lobule and its interactions with language and motor areas during writing. Eur. J. Neurosci. 2012, 35, 309–322. [Google Scholar] [CrossRef]
- Yang, H.; Wang, N.; Luo, X.; Lv, H.; Liu, H.; Li, Y.; Fan, G. Cerebellar atrophy and its contribution to motor and cognitive performance in multiple system atrophy. NeuroImage Clin. 2019, 23, 101891. [Google Scholar] [CrossRef]
- Jia, Z.; Peng, W.; Chen, Z.; Sun, H.; Zhang, H.; Kuang, W.; Huang, X.; Lui, S.; Gong, Q. Magnetization transfer imaging of treatment-resistant depression. Radiology 2017, 284, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Morita, T.; Saito, D.N.; Ban, M.; Shimada, K.; Okamoto, Y.; Kosaka, H.; Okazawa, H.; Asada, M.; Naito, E. Self-face recognition begins to share active region in right inferior parietal lobule with proprioceptive illusion during adolescence. Cereb. Cortex 2018, 28, 1532–1548. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Zhu, W.; Xiao, M.; Zhang, Q.; Zhao, Y.; Zhang, H.; Chen, X.; Zheng, Y.; Xia, L.-X. Hostile attribution bias mediates the relationship between structural variations in the left middle frontal gyrus and trait angry rumination. Front. Psychol. 2018, 9, 526. [Google Scholar] [CrossRef]
- Yuan, C.; Zhu, H.; Ren, Z.; Yuan, M.; Gao, M.; Zhang, Y.; Li, Y.; Meng, Y.; Gong, Q.; Lui, S.; et al. Precuneus-related regional and network functional deficits in social anxiety disorder: A resting-state functional MRI study. Compr. Psychiatry 2018, 82, 22–29. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | CUs | NCs | T | p-Value * |
|---|---|---|---|---|
| Male/female | 26/14 | 26/14 | N/A | >0.99 |
| Age (years) | 51.25 ± 5.46 | 51.98 ± 5.18 | 0.251 | 0.824 |
| Weight (kg) | 63.12 ± 7.35 | 63.89 ± 6.73 | 0.181 | 0.892 |
| Handedness | 40R | 40R | N/A | >0.99 |
| Duration of CU (days) | 8.10 ± 3.57 | N/A | N/A | N/A |
| Condition | L/R | Brain Regions | MNI Coordinates | Cluster Size | t-Value | ||
|---|---|---|---|---|---|---|---|
| X | Y | Z | |||||
| CU > NC | L | Cerebellum Posterior Lobe | −9 | −84 | −24 | 49 | 3.604 |
| CU > NC | R | Inferior Parietal Lobule | 48 | −63 | 42 | 72 | 3.526 |
| CU > NC | L | Middle Frontal Gyrus | −36 | 36 | 45 | 104 | 4.239 |
| CU > NC | L | Precuneus | −33 | −75 | 42 | 93 | 4.746 |
| CU > NC | L | superior parietal lobule | −3 | −75 | 48 | 61 | 4.975 |
| Brain Regions | Experimental Result | Brain Function | Anticipated Results |
|---|---|---|---|
| left cerebellum posterior lobe | CU > NC | sensorimotor, affective, and cognitive information [36] | Impairing both sensory and motor function; depression and anxiety [37] |
| right inferior parietal lobule | CU > NC | identify cognitive function, proprioception, and selective auditory attention [38] | Negative behavior and cognitive dysfunction. |
| left middle frontal gyrus | CU > NC | inhibition control, working memory, and emotional regulation [39] | Depression and anxiety |
| left precuneus | CU > NC | associated with pain perception and emotional control [40] | depression and anxiety |
| left superior parietal lobule | CU > NC | multiple cognitive processes and transmit visual information | impair the visual-motor integration and coordination |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, M.-J.; Huang, R.; Liang, R.-B.; Pan, Y.-C.; Shu, H.-Y.; Liao, X.-L.; Xu, S.-H.; Ying, P.; Kang, M.; Zhang, L.-J.; et al. Abnormal Intrinsic Functional Hubs in Corneal Ulcer: Evidence from a Voxel-Wise Degree Centrality Analysis. J. Clin. Med. 2022, 11, 1478. https://doi.org/10.3390/jcm11061478
Chen M-J, Huang R, Liang R-B, Pan Y-C, Shu H-Y, Liao X-L, Xu S-H, Ying P, Kang M, Zhang L-J, et al. Abnormal Intrinsic Functional Hubs in Corneal Ulcer: Evidence from a Voxel-Wise Degree Centrality Analysis. Journal of Clinical Medicine. 2022; 11(6):1478. https://doi.org/10.3390/jcm11061478
Chicago/Turabian StyleChen, Min-Jie, Rong Huang, Rong-Bin Liang, Yi-Cong Pan, Hui-Ye Shu, Xu-Lin Liao, San-Hua Xu, Ping Ying, Min Kang, Li-Juan Zhang, and et al. 2022. "Abnormal Intrinsic Functional Hubs in Corneal Ulcer: Evidence from a Voxel-Wise Degree Centrality Analysis" Journal of Clinical Medicine 11, no. 6: 1478. https://doi.org/10.3390/jcm11061478
APA StyleChen, M.-J., Huang, R., Liang, R.-B., Pan, Y.-C., Shu, H.-Y., Liao, X.-L., Xu, S.-H., Ying, P., Kang, M., Zhang, L.-J., Ge, Q.-M., & Shao, Y. (2022). Abnormal Intrinsic Functional Hubs in Corneal Ulcer: Evidence from a Voxel-Wise Degree Centrality Analysis. Journal of Clinical Medicine, 11(6), 1478. https://doi.org/10.3390/jcm11061478