
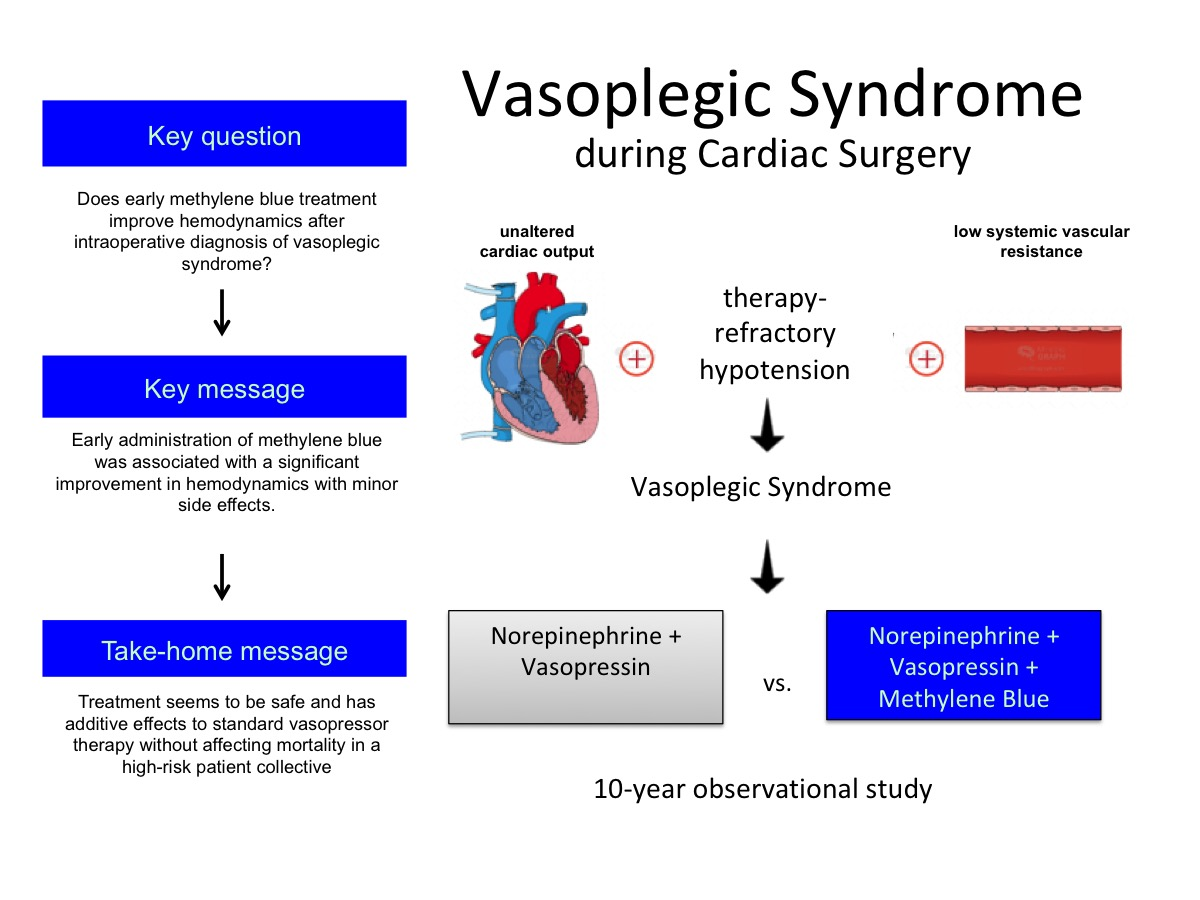
Early Use of Methylene Blue in Vasoplegic Syndrome: A 10-Year Propensity Score-Matched Cohort Study

 , , , , ,
, , , , , 
Abstract
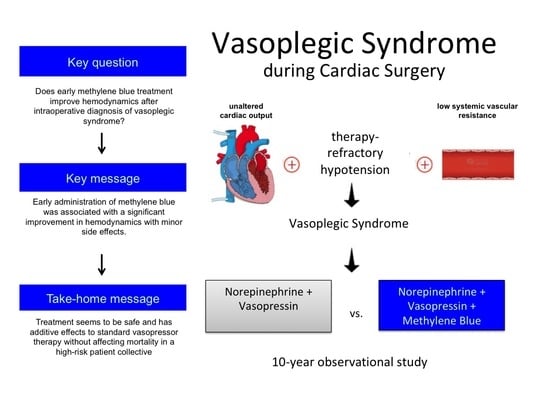
1. Introduction
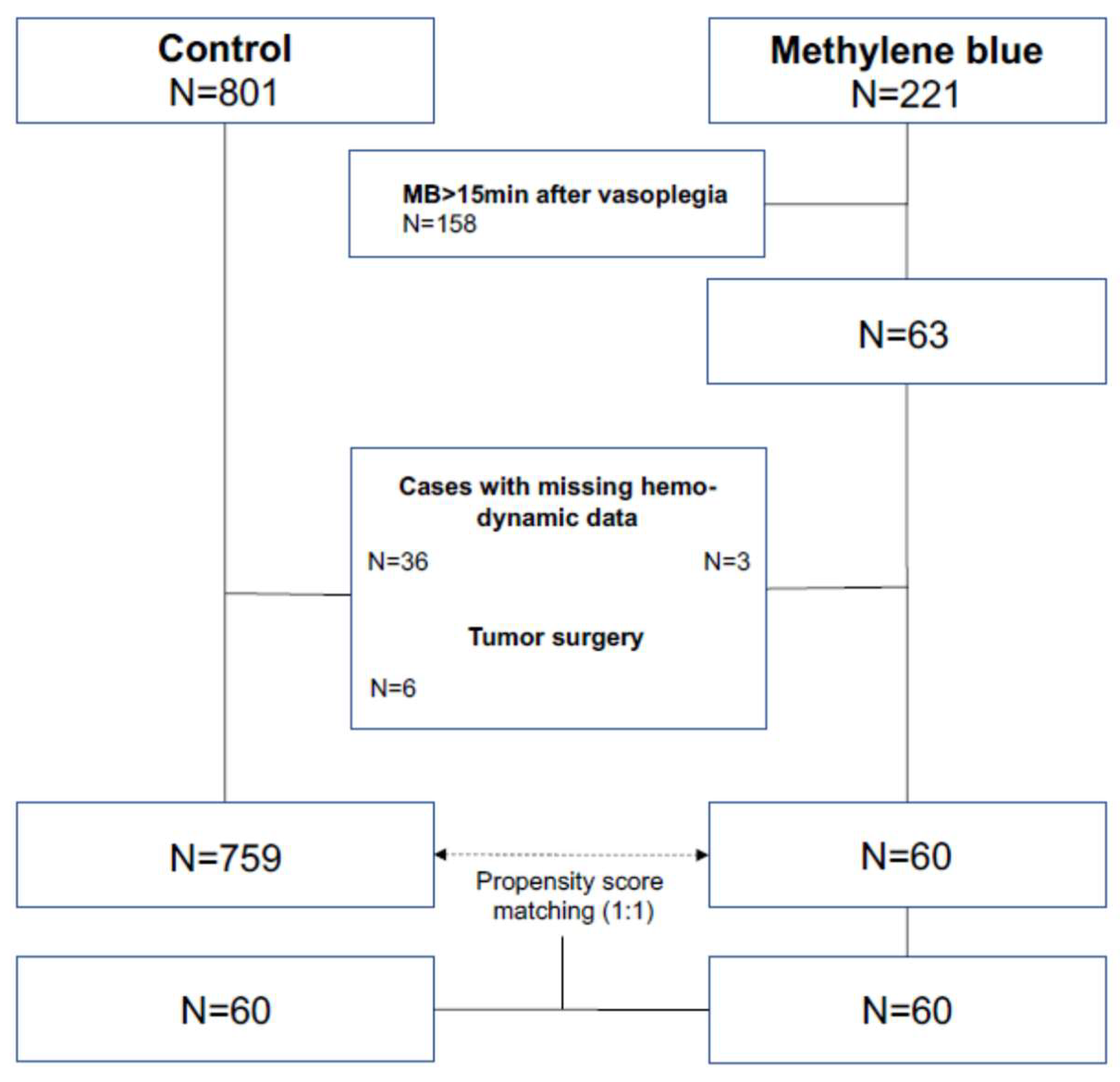
2. Materials and Methods
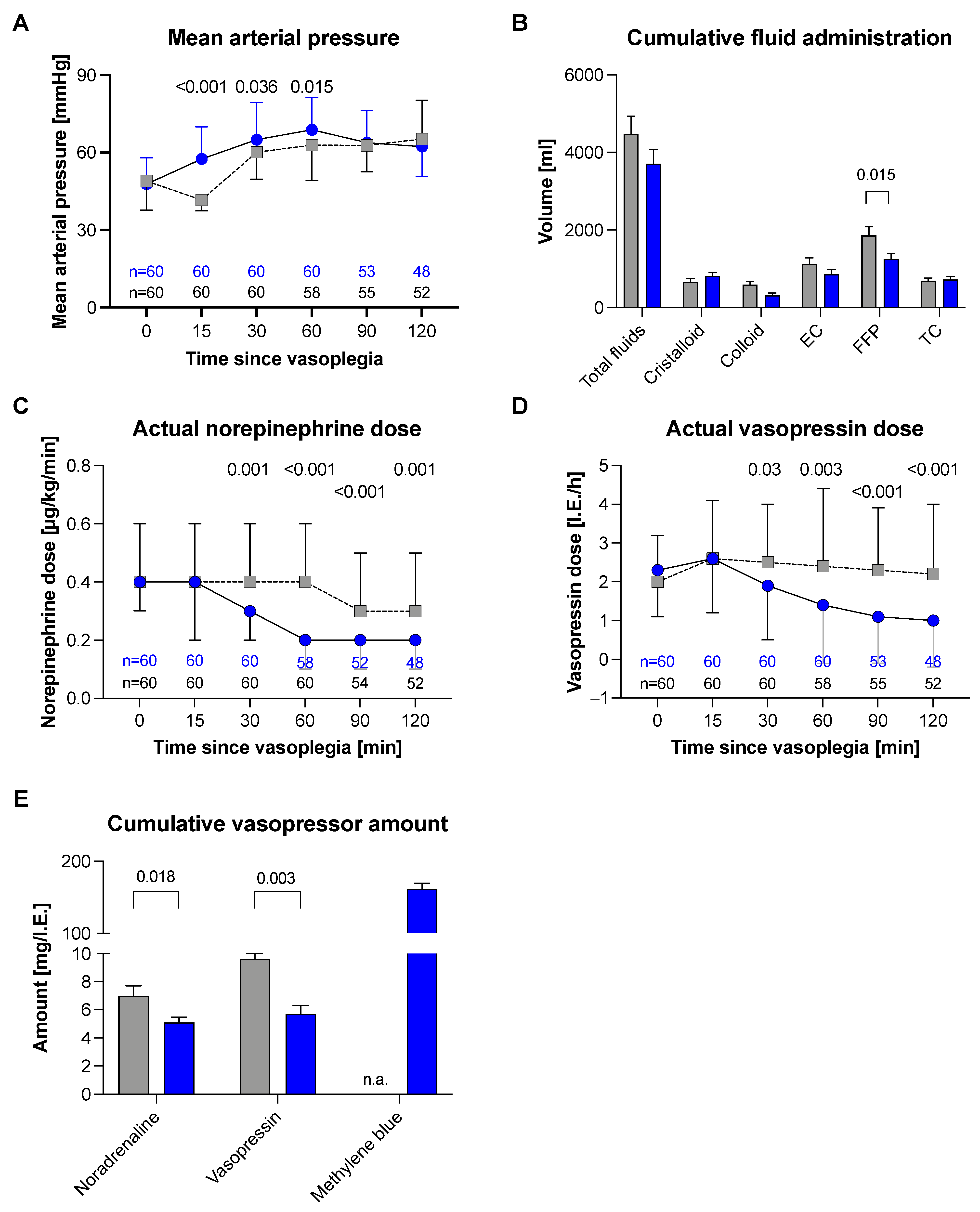
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Gomes, W.J.; Carvalho, A.C.; Palma, J.H.; Gonçalves, I., Jr.; Buffolo, E. Vasoplegic syndrome: A new dilemma. J. Thorac. Cardiovasc. Surg. 1994, 107, 942–943. [Google Scholar] [CrossRef]
- Lambden, S.; Creagh-Brown, B.C.; Hunt, J.; Summers, C.; Forni, L.G. Definitions and pathophysiology of vasoplegic shock. Crit. Care 2018, 22, 174. [Google Scholar] [CrossRef] [PubMed]
- Fischer, G.W.; Levin, M.A. Vasoplegia During Cardiac Surgery: Current Concepts and Management. Semin. Thorac. Cardiovasc. Surg. 2010, 22, 140–144. [Google Scholar] [CrossRef]
- Omar, S.; Zedan, A.; Nugent, K. Cardiac Vasoplegia Syndrome: Pathophysiology, Risk Factors and Treatment. Am. J. Med Sci. 2015, 349, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Byrne, J.G.; Leacche, M.; Paul, S.; Mihaljevic, T.; Rawna, J.D.; Shernan, S.K.; Mudge, G.H.; Stevenson, L.W. Risk factors and outcomes for ’vasoplegia syndrome’ following cardiac transplantation. Eur. J. Cardio-Thoracic Surg. 2004, 25, 327–332. [Google Scholar] [CrossRef]
- Liu, H.; Yu, L.; Yang, L.; Green, M.S. Vasoplegic syndrome: An update on perioperative considerations. J. Clin. Anesth. 2017, 40, 63–71. [Google Scholar] [CrossRef]
- Wu, K.K.; Rossi, E.C. (Eds.) The damaging effects of cardiopulmonary bypass. In Prostaglandins in Clinical Medicine: Cardiovascular and Thrombotic Disorders; Year Book Medical Publishers: Chicago, IL, USA, 1982; p. 355. [Google Scholar]
- Shaefi, S.; Mittel, A.; Klick, J.; Evans, A.; Ivascu, N.S.; Gutsche, J.; Augoustides, J.G. Vasoplegia after cardiovascular procedures-pathophysiology and targeted therapy. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1013–1022. [Google Scholar] [CrossRef]
- Busse, L.W.; Barker, N.; Petersen, C. Vasoplegic syndrome following cardiothoracic surgery—review of pathophysiology and update of treatment options. Crit. Care 2020, 24, 36. [Google Scholar] [CrossRef]
- Kruszyna, H.; Magyar, J.; Rochelle, L.G.; A Russell, M.; Smith, R.P.; E Wilcox, D. Spectroscopic studies of nitric oxide (NO) interactions with cobalamins: Reaction of NO with superoxocobalamin(III) likely accounts for cobalamin reversal of the biological effects of NO. J. Pharmacol. Exp. Ther. 1998, 285, 665–671. [Google Scholar]
- Weinberg, J.B.; Chen, Y.; Jiang, N.; Beasley, B.E.; Salerno, J.C.; Ghosh, D.K. Inhibition of nitric oxide synthase by cobalamins and cobinamides. Free Radic. Biol. Med. 2009, 46, 1626–1632. [Google Scholar] [CrossRef]
- Bakker, J.; Grover, R.; McLuckie, A.; Holzapfel, L.; Andersson, J.; Lodato, R.; Watson, D.; Grossman, S.; Donaldson, J.; Takala, J. Administration of the nitric oxide synthase inhibitor NG-methyl-l-arginine hydrochloride (546C88) by intravenous infusion for up to 72 hours can promote the resolution of shock in patients with severe sepsis: Results of a randomized, double-blind, placebo-controlled multicenter study (study no. 144-002). Crit. Care Med. 2004, 32, 1–12. [Google Scholar] [CrossRef]
- Wieruszewski, P.; Radosevich, M.A.; Kashani, K.B.; Daly, R.C.; Wittwer, E.D. Synthetic Human Angiotensin II for Postcardiopulmonary Bypass Vasoplegic Shock. J. Cardiothorac. Vasc. Anesth. 2019, 33, 3080–3084. [Google Scholar] [CrossRef]
- Evans, A.; McCurdy, M.T.; Weiner, M.; Zaku, B.; Chow, J.H. Use of Angiotensin II for Post Cardiopulmonary Bypass Vasoplegic Syndrome. Ann. Thorac. Surg. 2019, 108, e5–e7. [Google Scholar] [CrossRef] [PubMed]
- Saha, A.; Jennings, D.L.; Ning, Y.; Kurlansky, P.; Miltiades, A.N.; Spellman, J.L.; Sanchez, J.; Yuzefpolskaya, M.; Colombo, P.C.; Takayama, H.; et al. Methylene Blue Does Not Improve Vasoplegia After Left Ventricular Assist Device Implantation. Ann. Thorac. Surg. 2021, 111, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Weiner, M.M.; Lin, H.-M.; Danforth, D.; Rao, S.; Hosseinian, L.; Fischer, G.W. Methylene Blue is Associated With Poor Outcomes in Vasoplegic Shock. J. Cardiothorac. Vasc. Anesth. 2013, 27, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Andritsos, M.J. Con: Methylene Blue Should Not Be Used Routinely for Vasoplegia Perioperatively. J. Cardiothorac. Vasc. Anesth. 2011, 25, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Özal, E.; Kuralay, E.; Yildirim, V.; Kilic, S.; Bolcal, C.; Kücükarslan, N.; Günay, C.; Demirkilic, U.; Tatar, H. Preoperative Methylene Blue Administration in Patients at High Risk for Vasoplegic Syndrome During Cardiac Surgery. Ann. Thorac. Surg. 2005, 79, 1615–1619. [Google Scholar] [CrossRef]
- Evora, P.R.B.; Alves, L.; Ferreira, C.A.; Menardi, A.C.; Bassetto, S.; Rodrigues, A.J.; Scorzoni, A.; Vicente, W. Twenty years of vasoplegic syndrome treatment in heart surgery. Methylene blue revised. Rev. Bras. Cir. Cardiovasc. Órgão Soc. Bras. Cir. Cardiovasc. 2014, 30, 84–92. [Google Scholar] [CrossRef]
- Levin, M.A.; Lin, H.-M.; Castillo, J.G.; Adams, D.H.; Reich, D.L.; Fischer, G.W. Early On–Cardiopulmonary Bypass Hypotension and Other Factors Associated With Vasoplegic Syndrome. Circulation 2009, 120, 1664–1671. [Google Scholar] [CrossRef]
- Gomes, W.J.; Carvalho, A.C.; Palma, J.H.; A Teles, C.; Branco, J.N.; Silas, M.G.; Buffolo, E. Vasoplegic syndrome after open heart surgery. J. Cardiovasc. Surg. 1998, 39, 619–623. [Google Scholar]
- Busse, L.W.; Ostermann, M. Vasopressor Therapy and Blood Pressure Management in the Setting of Acute Kidney Injury. Semin. Nephrol. 2019, 39, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Argenziano, M.; Chen, J.M.; Choudhri, A.F.; Cullinane, S.; Garfein, E.; Weinberg, A.D.; Smith, C.R.; Rose, E.A.; Landry, D.W.; Oz, M.C. Management of vasodilatory shock after cardiac surgery: Identification of predisposing factors and use of a novel pressor agent. J. Thorac. Cardiovasc. Surg. 1998, 116, 973–980. [Google Scholar] [CrossRef]
- Nestler, E.J.; Duman, R.S. Guanylyl cyclase. In Basic Neurochemistry: Molecular, Cellular and Medical Aspects, 6th ed.; Bookshelf ID: NBK28167; American Society for Neurochemistry: Windermere, FL, USA, 1999. [Google Scholar]
- Evora, P.R.B. Methylene Blue Is a Guanylate Cyclase Inhibitor That Does Not Interfere with Nitric Oxide Synthesis. Tex. Heart Inst. J. 2016, 43, 103. [Google Scholar] [CrossRef] [PubMed]
- Wolin, M.S.; Cherry, P.D.; Rodenburg, J.M.; Messina, E.J.; Kaley, G. Methylene blue inhibits vasodilation of skeletal muscle arterioles to acetylcholine and nitric oxide via the extracellular generation of superoxide anion. J. Pharmacol. Exp. Ther. 1990, 254, 872–876. [Google Scholar]
- Levy, B.; Fritz, C.; Tahon, E.; Jacquot, A.; Auchet, T.; Kimmoun, A. Vasoplegia treatments: The past, the present, and the future. Crit. Care 2018, 22, 52. [Google Scholar] [CrossRef]
- Ortoleva, J.P.; Cobey, F.C. A Systematic Approach to the Treatment of Vasoplegia Based on Recent Advances in Pharmacotherapy. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1310–1314. [Google Scholar] [CrossRef]
- Mazzeffi, M.; Hammer, B.; Chen, E.; Caridi-Scheible, M.; Ramsay, J.; Paciullo, C. Methylene blue for postcardiopulmonary bypass vasoplegic syndrome: A cohort study. Ann. Card. Anaesth. 2017, 20, 178–181. [Google Scholar] [CrossRef]
- Mehaffey, J.H.; Johnston, L.E.; Hawkins, R.; Charles, E.J.; Yarboro, L.; Kern, J.A.; Ailawadi, G.; Kron, I.L.; Ghanta, R.K. Methylene Blue for Vasoplegic Syndrome After Cardiac Operation: Early Administration Improves Survival. Ann. Thorac. Surg. 2017, 104, 36–41. [Google Scholar] [CrossRef]
- Levin, R.L.; Degrange, M.A.; Bruno, G.F.; Del Mazo, C.D.; Taborda, D.J.; Griotti, J.J.; Boullon, F.J. Methylene blue reduces mortality and morbidity in vasoplegic patients after cardiac surgery. Ann. Thorac. Surg. 2004, 77, 496–499. [Google Scholar] [CrossRef]
- Blacker, S.A.; Whalen, F.X. Vasoplegic syndrome: Does the timing of methylene blue matter? J. Anesth. Clin. Res. 2013, 4, 333. [Google Scholar]
- Fernandes, D.; Da Silva-Santos, J.E.; Duma, D.; Villela, C.G.; Barja-Fidalgo, C.; Assreuy, J. Nitric Oxide-Dependent Reduction in Soluble Guanylate Cyclase Functionality Accounts for Early Lipopolysaccharide-Induced Changes in Vascular Reactivity. Mol. Pharmacol. 2005, 69, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Ng, B.K.; Cameron, A.J. The role of methylene blue in serotonin syndrome: A systematic review. Psychosomatics 2010, 51, 194–200. [Google Scholar] [CrossRef]
- Grubb, K.J.; Kennedy, J.L.; Bergin, J.D.; Groves, D.S.; Kern, J.A. The role of methylene blue in serotonin syndrome following cardiac transplantation: A case report and review of the literature. J. Thorac. Cardiovasc. Surg. 2012, 144, e113–e116. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hencken, L.; To, L.; Ly, N.; Morgan, J.A. Serotonin Syndrome Following Methylene Blue Administration for Vasoplegic Syndrome. J. Card. Surg. 2016, 31, 208–210. [Google Scholar] [CrossRef]
- Martino, E.A.; Winterton, D.; Nardelli, P.; Pasin, L.; Calabrò, M.G.; Bove, T.; Fanelli, G.; Zangrillo, A.; Landoni, G. The Blue Coma: The Role of Methylene Blue in Unexplained Coma After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2016, 30, 423–427. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methylene Blue N = 60 | Control N = 759 | p-Value | Matched Control N = 60 | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| Male sex | 51 | 85.0 | 580 | 76.4 | 0.082 | 44 | 73.3 | 0.177 |
| Age (y) | 62.3 | ±12.2 | 64.0 | ±13.6 | 0.351 | 62.0 | ±14.2 | 0.891 |
| BMI (kg/m2) | 27.5 | ±4.5 | 26.2 | ±4.3 | 0.024 | 26.7 | ±4.8 | 0.363 |
| ASA class | 0.062 | 0.414 | ||||||
| 1 | 0 | 0 | 1 | 0.1 | 0 | 0.0 | ||
| 2 | 0 | 0 | 1 | 0.1 | 0 | 0.0 | ||
| 3 | 12 | 20.0 | 293 | 38.6 | 10 | 16.7 | ||
| 4 | 42 | 70.0 | 419 | 55.2 | 39 | 65.0 | ||
| 5 | 6 | 10.0 | 45 | 5.9 | 11 | 18.3 | ||
| Procedure | <0.001 | 0.031 | ||||||
| Aorta | 16 | 26.7 | 107 | 14.1 | 7 | 11.7 | ||
| Valve | 21 | 35.0 | 302 | 39.8 | 20 | 33.3 | ||
| Bypass | 8 | 13.3 | 225 | 29.6 | 18 | 30.0 | ||
| Artificial heart | 5 | 8.3 | 69 | 9.1 | 9 | 15.0 | ||
| Combination | 4 | 6.7 | 22 | 2.9 | 0 | 0.0 | ||
| Other | 2 | 3.3 | 25 | 3.3 | 4 | 6.7 | ||
| Revision | 4 | 6.7 | 9 | 1.2 | 2 | 3.3 | ||
| Emergency | 13 | 21.7 | 151 | 19.9 | 0.738 | 16 | 26.7 | 0.335 |
| Methylene Blue N = 60 | Matched Control N = 60 | p-Value | |||
|---|---|---|---|---|---|
| Duration of surgery (min) | 421 | ±152 | 447 | ±169 | 0.373 |
| Bypass duration (min) | 183 | ±104 | 185 | ±109 | 0.915 |
| Duration of mechanical ventilation (h) * | 203 | ±338 | 195 | ±275 | 0.918 |
| Length of hospitalization (d) | 30 | ±33 | 27 | ±35 | 0.620 |
| Length of ICU stay (d) ** | 16 | ±21 | 20 | ±37 | 0.466 |
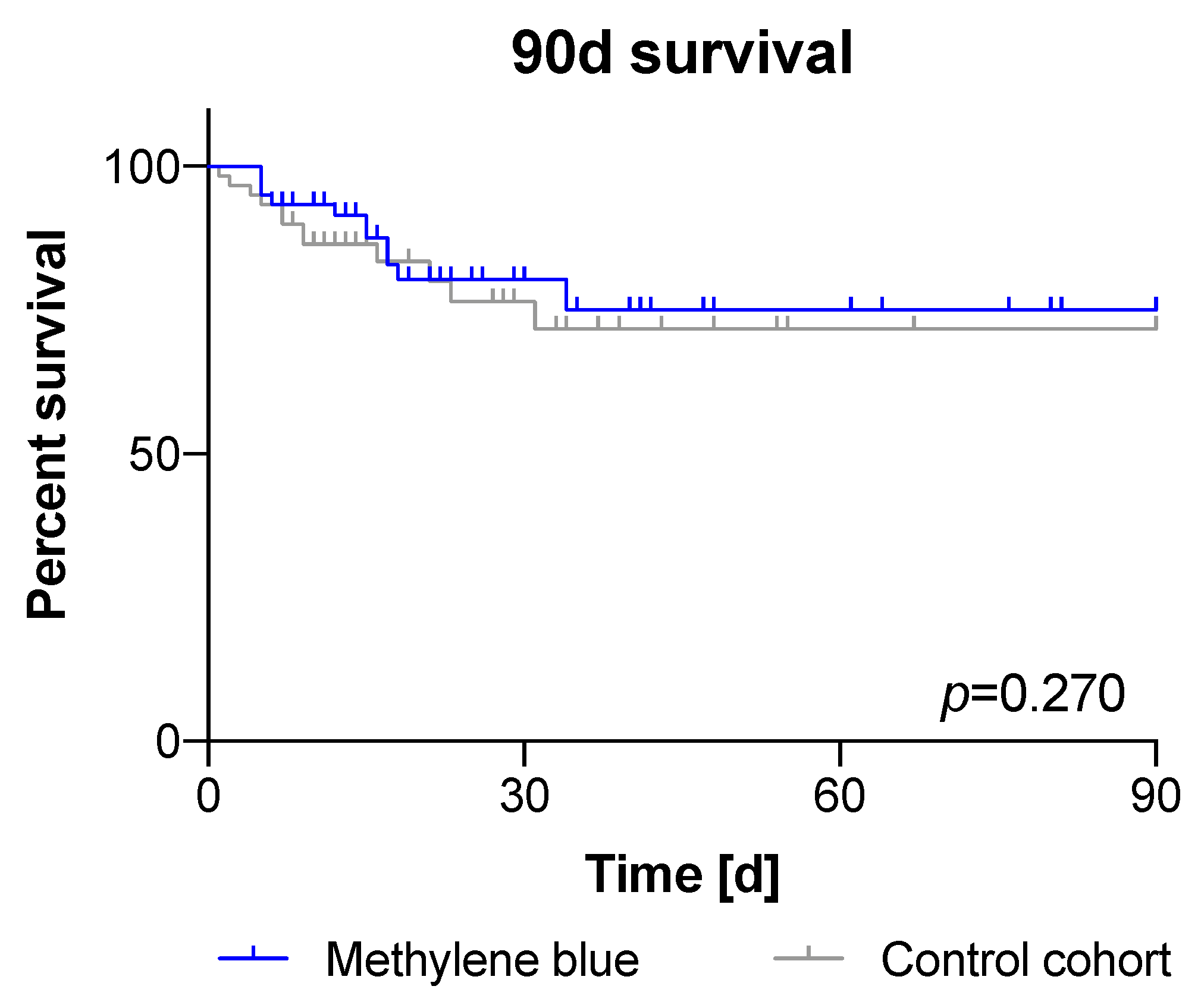
| 90-day survival | 49 | 81.7 | 48 | 80.0 | 0.270 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kofler, O.; Simbeck, M.; Tomasi, R.; Hinske, L.C.; Klotz, L.V.; Uhle, F.; Born, F.; Pichlmaier, M.; Hagl, C.; Weigand, M.A.; et al. Early Use of Methylene Blue in Vasoplegic Syndrome: A 10-Year Propensity Score-Matched Cohort Study. J. Clin. Med. 2022, 11, 1121. https://doi.org/10.3390/jcm11041121
Kofler O, Simbeck M, Tomasi R, Hinske LC, Klotz LV, Uhle F, Born F, Pichlmaier M, Hagl C, Weigand MA, et al. Early Use of Methylene Blue in Vasoplegic Syndrome: A 10-Year Propensity Score-Matched Cohort Study. Journal of Clinical Medicine. 2022; 11(4):1121. https://doi.org/10.3390/jcm11041121
Chicago/Turabian StyleKofler, Othmar, Maximilian Simbeck, Roland Tomasi, Ludwig Christian Hinske, Laura Valentina Klotz, Florian Uhle, Frank Born, Maximilian Pichlmaier, Christian Hagl, Markus Alexander Weigand, and et al. 2022. "Early Use of Methylene Blue in Vasoplegic Syndrome: A 10-Year Propensity Score-Matched Cohort Study" Journal of Clinical Medicine 11, no. 4: 1121. https://doi.org/10.3390/jcm11041121
APA StyleKofler, O., Simbeck, M., Tomasi, R., Hinske, L. C., Klotz, L. V., Uhle, F., Born, F., Pichlmaier, M., Hagl, C., Weigand, M. A., Zwißler, B., & von Dossow, V. (2022). Early Use of Methylene Blue in Vasoplegic Syndrome: A 10-Year Propensity Score-Matched Cohort Study. Journal of Clinical Medicine, 11(4), 1121. https://doi.org/10.3390/jcm11041121