
Evaluation of Risk Prediction Models to Identify Cancer Therapeutics Related Cardiac Dysfunction in Women with HER2+ Breast Cancer

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Cancer Therapeutics Related Cardiac Dysfunction (CTRCD)
2.3. Risk Models
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Incidence of CTRCD within Risk Score Categories
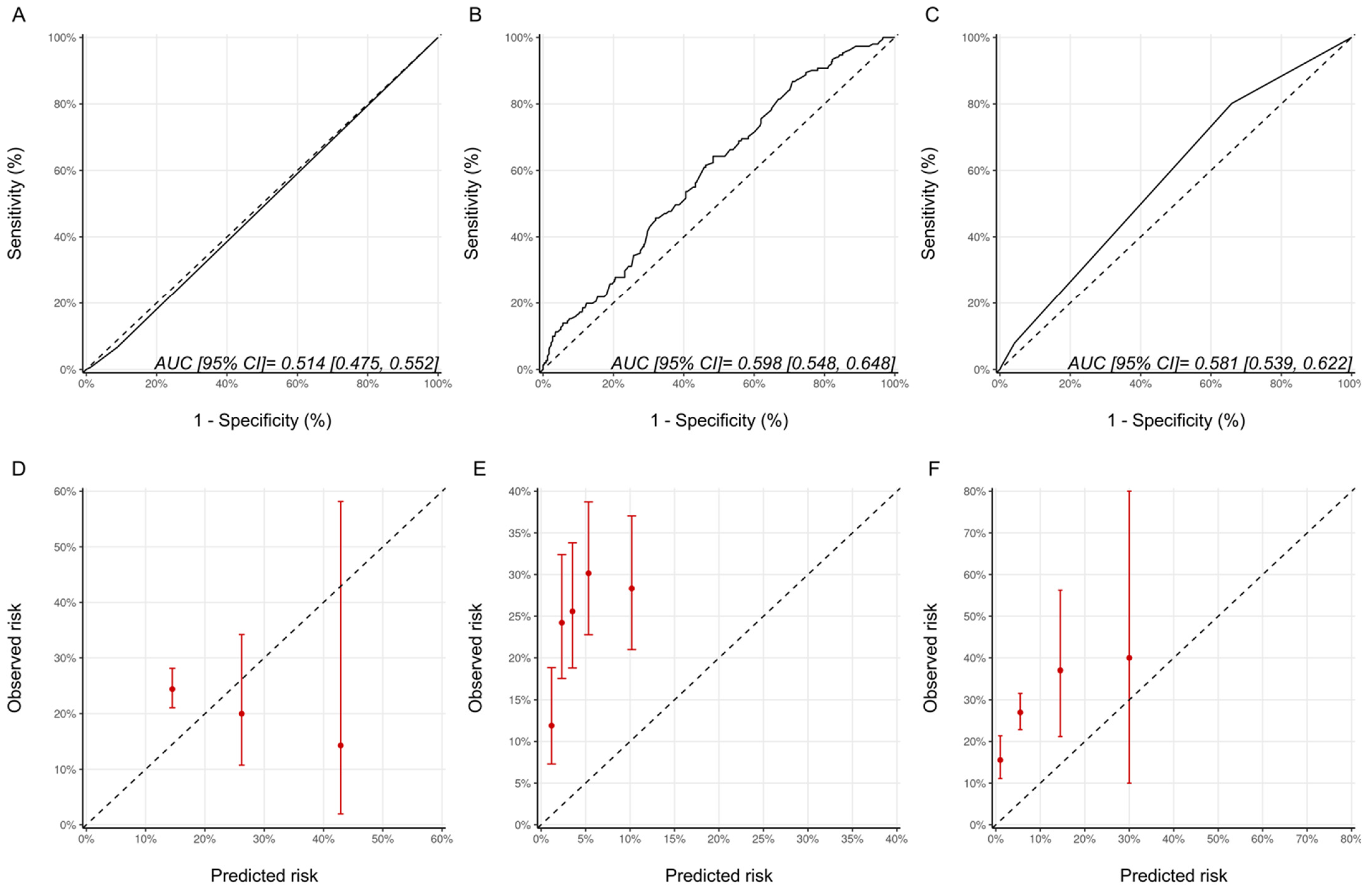
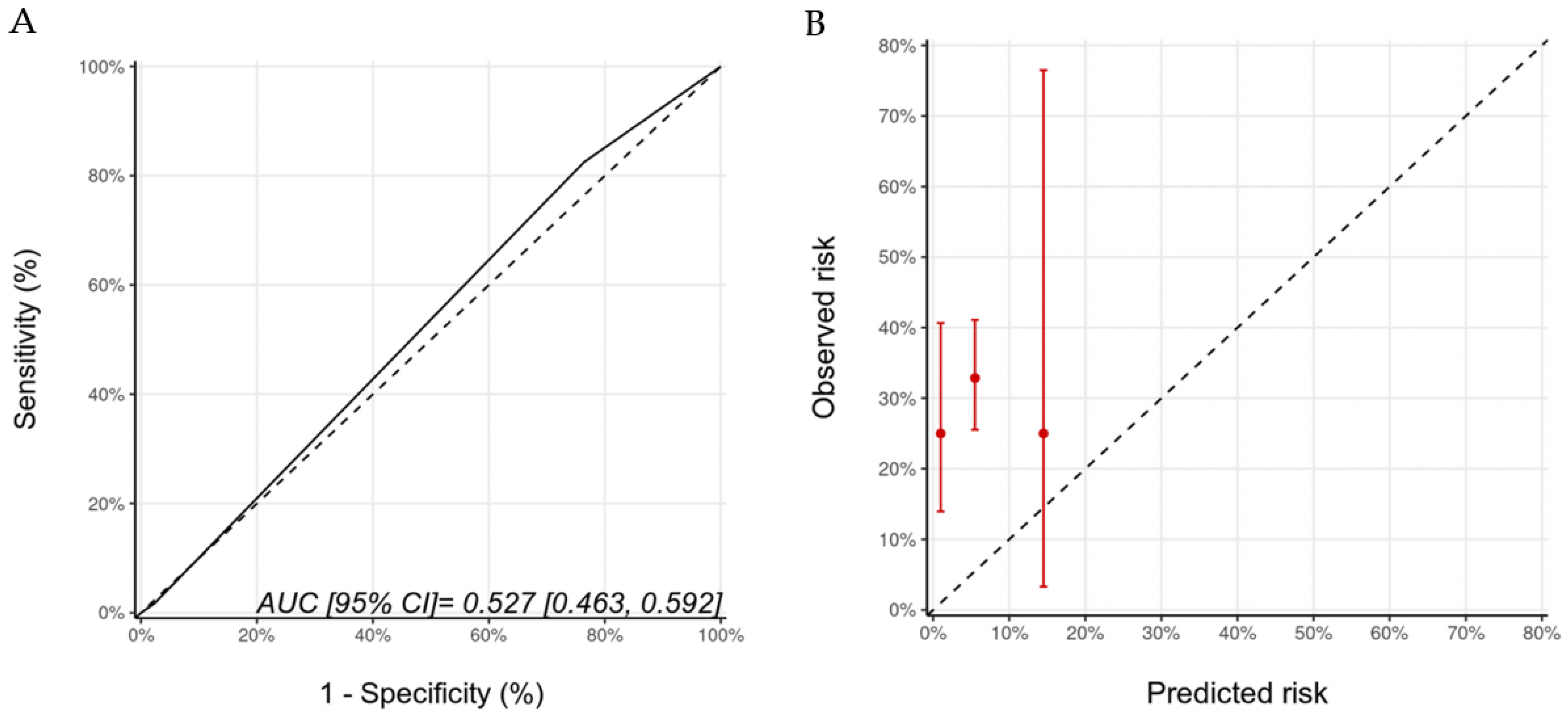
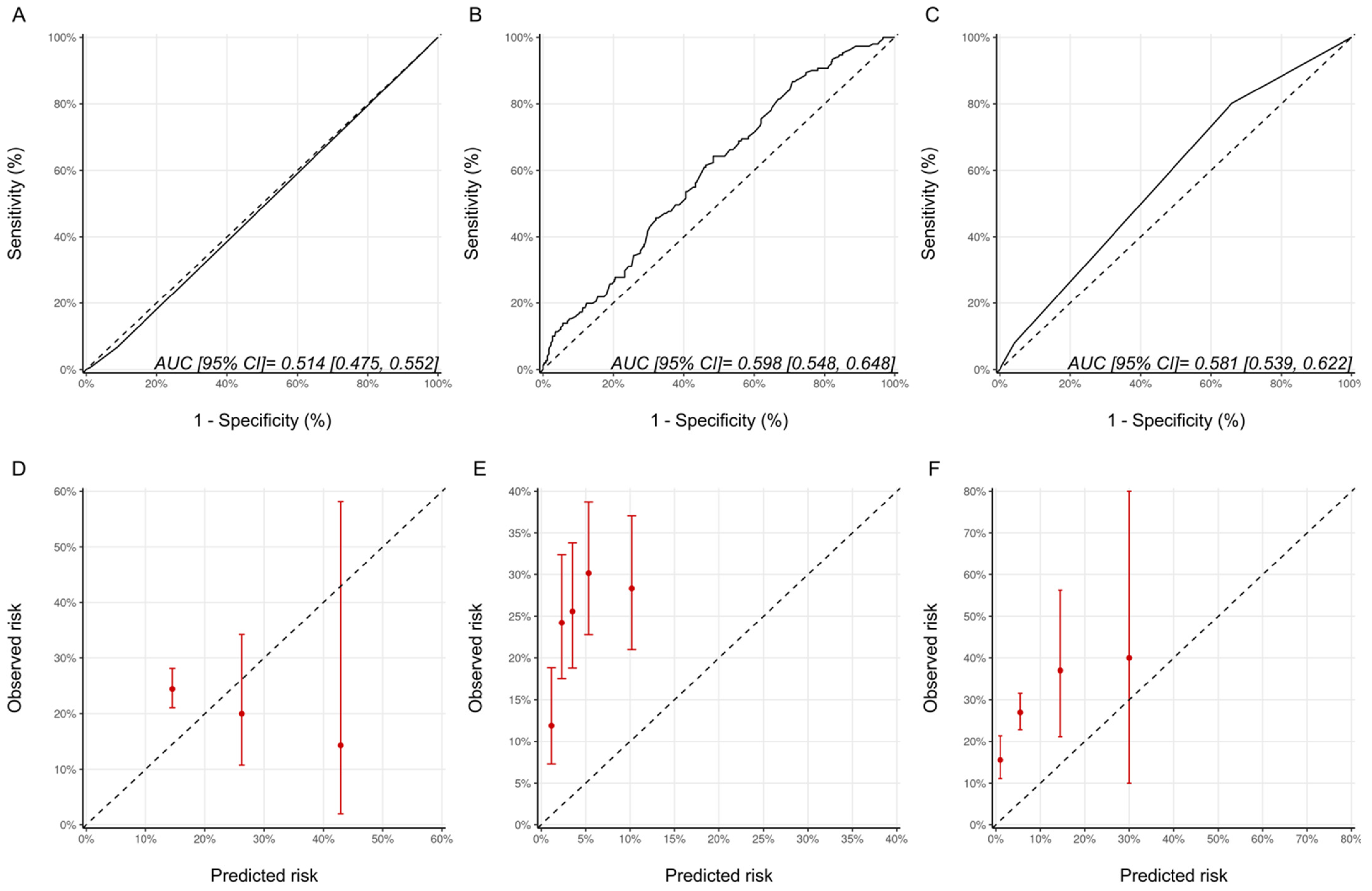
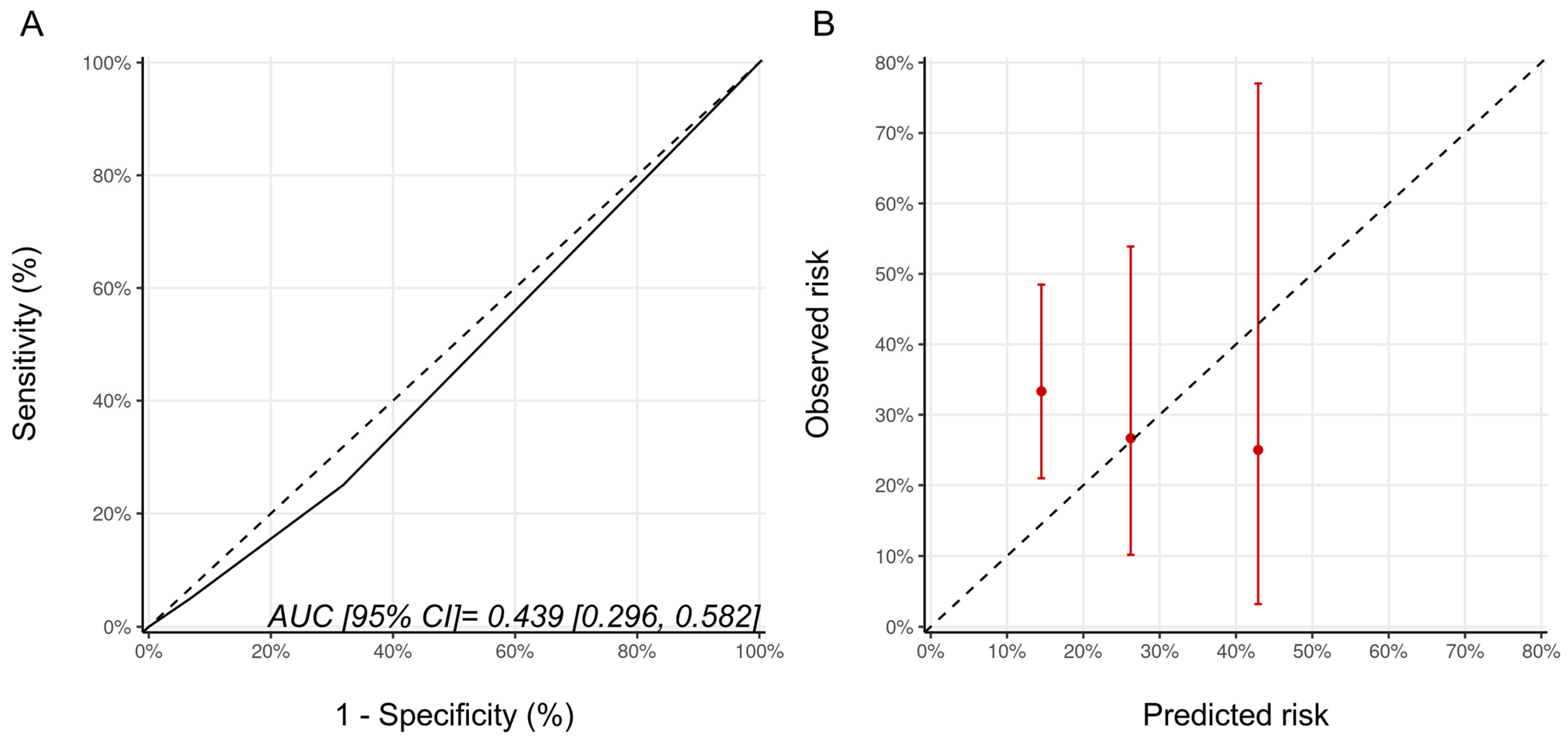
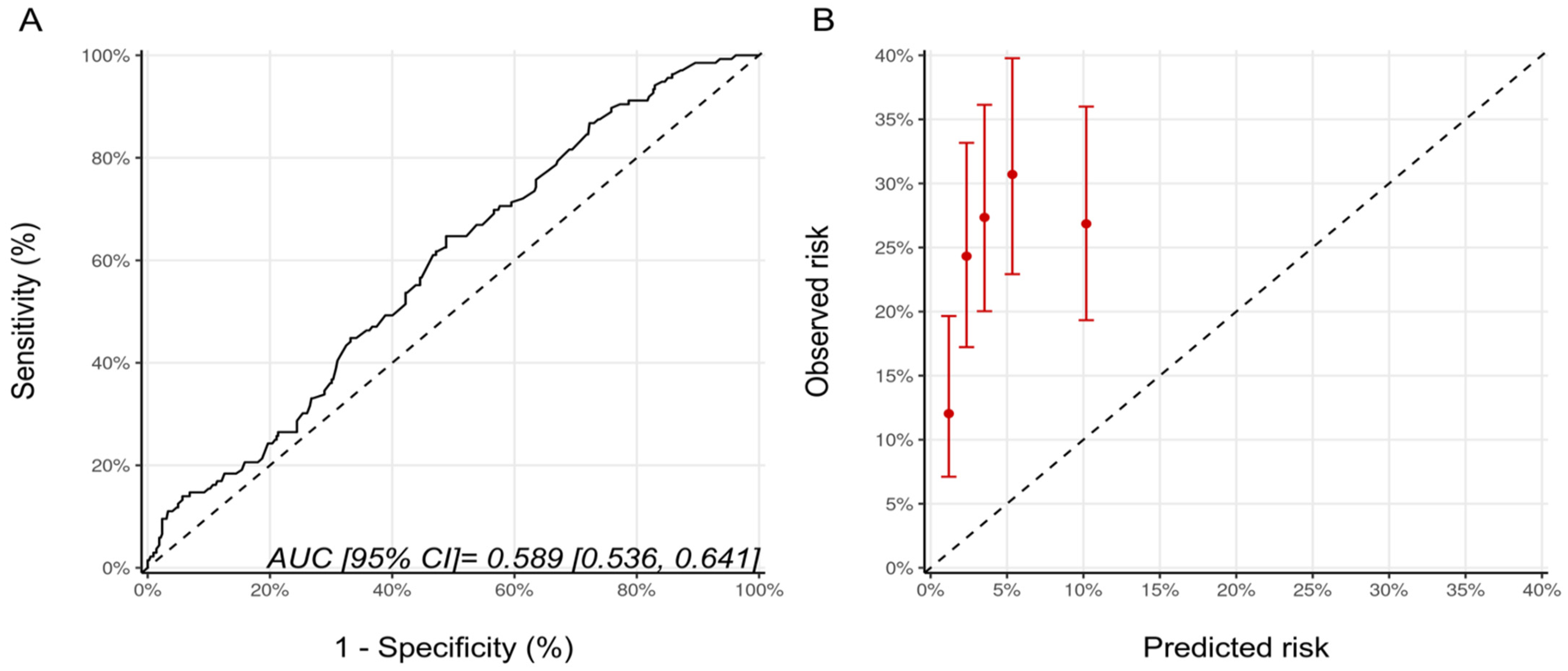
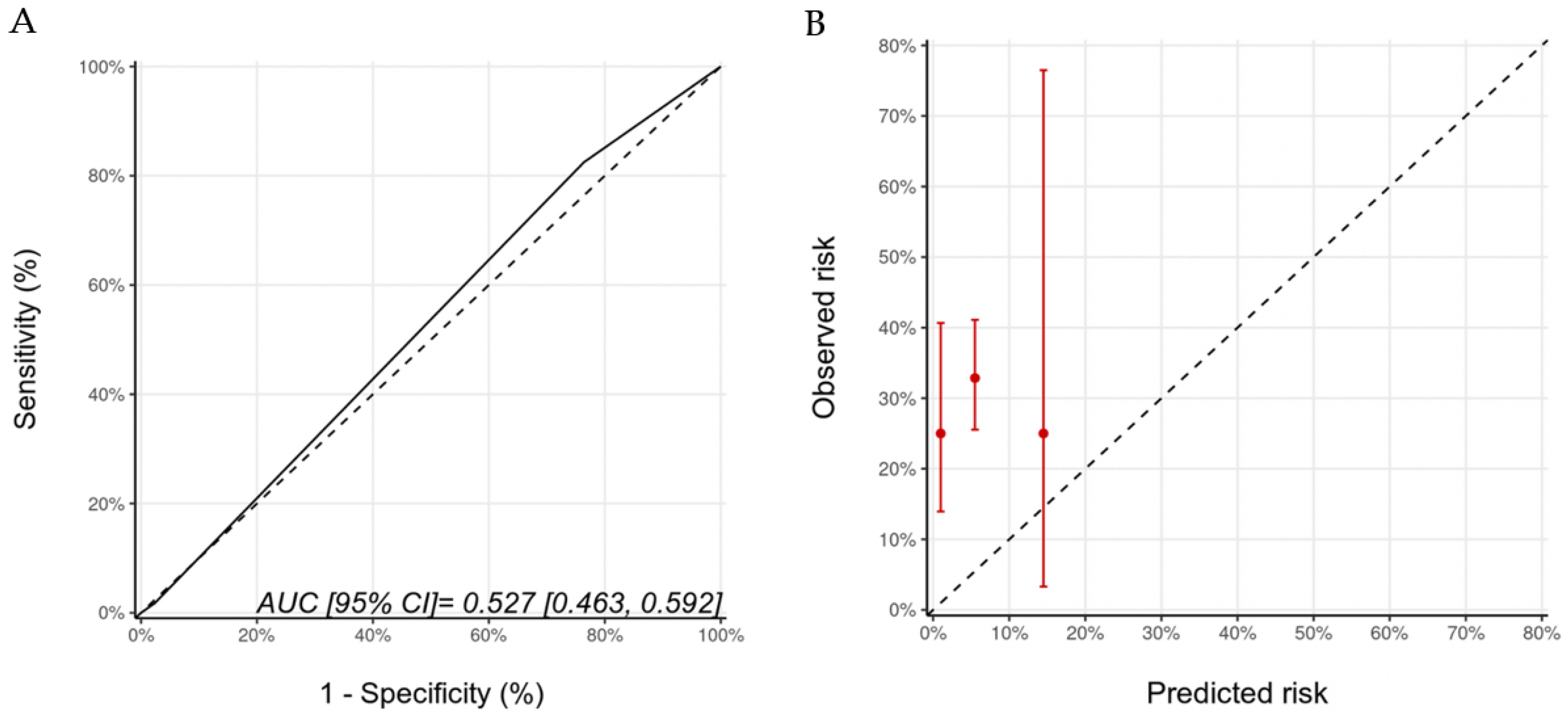
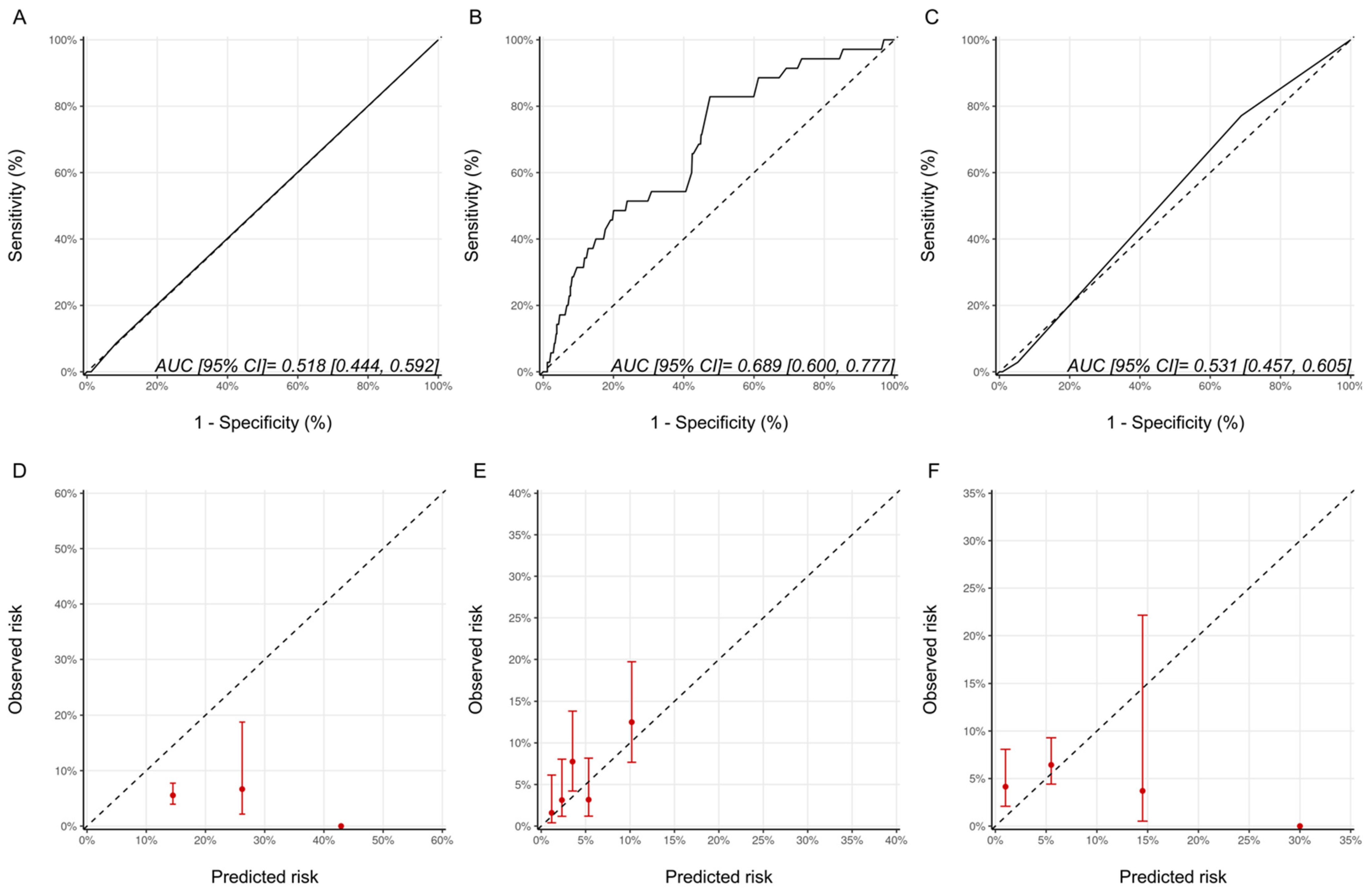
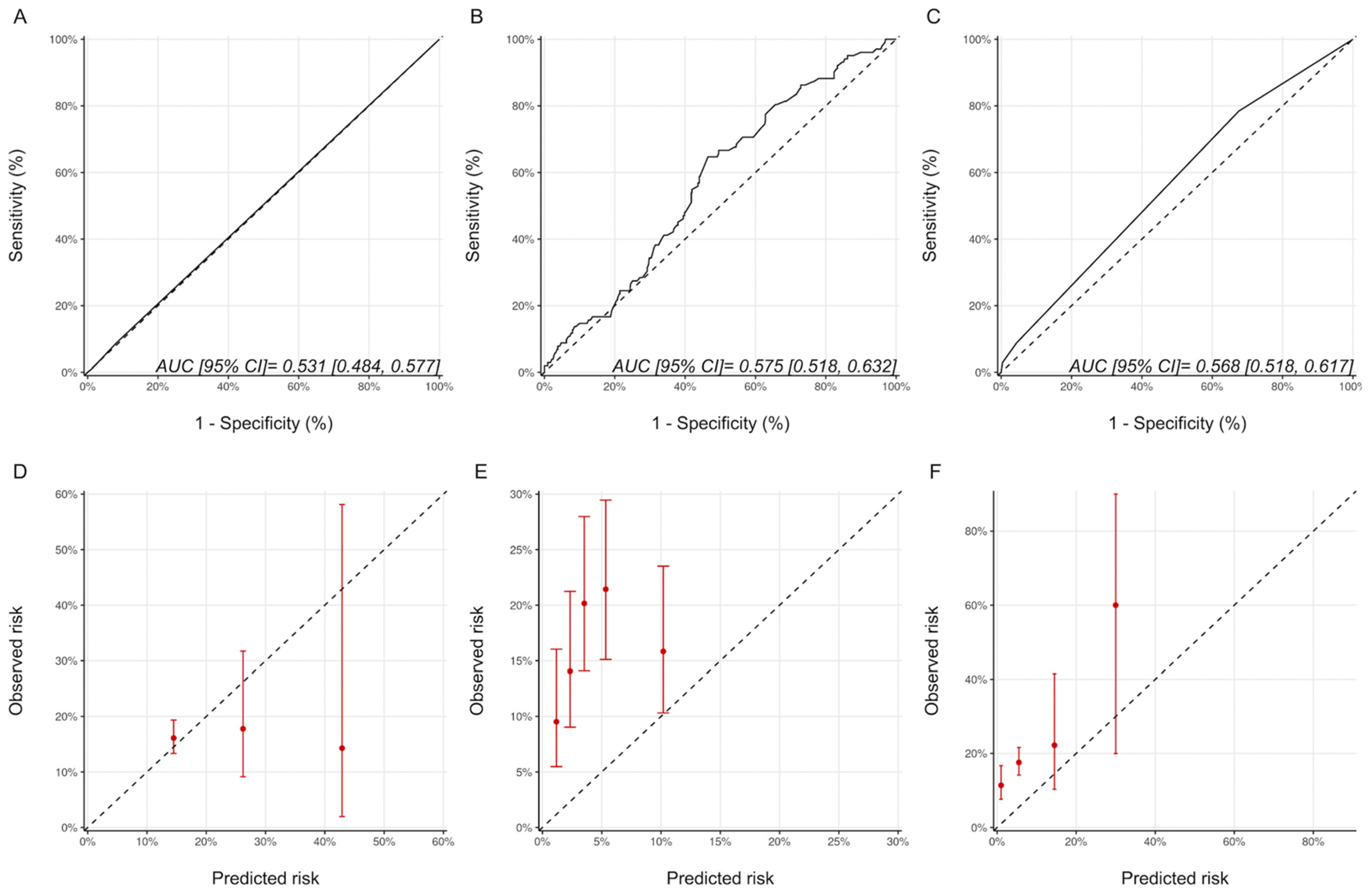
3.3. Discrimination and Calibration of the Risk Models
3.4. Sensitivity Analyses
4. Discussion
4.1. CTRCD Risk Assessment
4.2. Existing Risk Prediction Models
4.3. CTRCD Definition and Model Performance
4.4. Limitations of Existing Models
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guglin, M.; Krischer, J.; Tamura, R.; Fink, A.; Bello-Matricaria, L.; McCaskill-Stevens, W.; Munster, P.N. Randomized Trial of Lisinopril Versus Carvedilol to Prevent Trastuzumab Cardiotoxicity in Patients With Breast Cancer. J. Am. Coll. Cardiol. 2019, 73, 2859–2868. [Google Scholar] [CrossRef]
- Narayan, H.K.; French, B.; Khan, A.M.; Plappert, T.; Hyman, D.; Bajulaiye, A.; Domchek, S.; DeMichele, A.; Clark, A.; Matro, J.; et al. Noninvasive Measures of Ventricular-Arterial Coupling and Circumferential Strain Predict Cancer Therapeutics–Related Cardiac Dysfunction. JACC Cardiovasc. Imaging 2016, 9, 1131–1141. [Google Scholar] [CrossRef]
- Houbois, C.P.; Nolan, M.; Somerset, E.; Shalmon, T.; Esmaeilzadeh, M.; Lamacie, M.M.; Amir, E.; Brezden-Masley, C.; Koch, C.A.; Thevakumaran, Y.; et al. Serial Cardiovascular Magnetic Resonance Strain Measurements to Identify Cardiotoxicity in Breast Cancer. JACC Cardiovasc. Imaging 2020, 14, 962. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Abdel-Qadir, H.; Fischer, H.D.; Liu, Y.; Camacho, X.; Amir, E.; Austin, P.C.; Lee, D.S. Risk-Imaging Mismatch in Cardiac Imaging Practices for Women Receiving Systemic Therapy for Early-Stage Breast Cancer: A Population-Based Cohort Study. J. Clin. Oncol. 2018, 36, 2980–2987. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Abdel-Qadir, H.; Fischer, H.D.; Camacho, X.; Amir, E.; Austin, P.C.; Lee, D.S. Breast Cancer Therapy–Related Cardiac Dysfunction in Adult Women Treated in Routine Clinical Practice: A Population-Based Cohort Study. J. Clin. Oncol. 2016, 34, 2239–2246. [Google Scholar] [CrossRef]
- Copeland-Halperin, R.S.; Al-Sadawi, M.; Patil, S.; Liu, J.E.; Steingart, R.M.; Dang, C.T.; Yu, A.F. Early Trastuzumab Interruption and Recurrence-Free Survival in ERBB2 -Positive Breast Cancer. JAMA Oncol. 2020, 6, 1971. [Google Scholar] [CrossRef]
- Rushton, M.; Lima, I.; Tuna, M.; Johnson, C.; Ivars, J.; Pritchard, K.; Hawken, S.; Dent, S. Impact of Stopping Trastuzumab in Early Breast Cancer: A Population-Based Study in Ontario, Canada. JNCI J. Natl. Cancer Inst. 2020, 112, 1222–1230. [Google Scholar] [CrossRef]
- Curigliano, G.; Lenihan, D.; Fradley, M.; Ganatra, S.; Barac, A.; Blaes, A.; Herrmann, J.; Porter, C.; Lyon, A.R.; Lancellotti, P.; et al. Management of Cardiac Disease in Cancer Patients throughout Oncological Treatment: ESMO Consensus Recommendations. Ann. Oncol. 2020, 31, 171–190. [Google Scholar] [CrossRef] [Green Version]
- Armenian, S.H.; Lacchetti, C.; Barac, A.; Carver, J.; Constine, L.S.; Denduluri, N.; Dent, S.; Douglas, P.S.; Durand, J.-B.; Ewer, M.; et al. Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2017, 35, 893–911. [Google Scholar] [CrossRef]
- Ezaz, G.; Long, J.B.; Gross, C.P.; Chen, J. Risk Prediction Model for Heart Failure and Cardiomyopathy After Adjuvant Trastuzumab Therapy for Breast Cancer. J. Am. Heart Assoc. 2014, 3, e000472. [Google Scholar] [CrossRef] [Green Version]
- Romond, E.H.; Jeong, J.-H.; Rastogi, P.; Swain, S.M.; Geyer, C.E.; Ewer, M.S.; Rathi, V.; Fehrenbacher, L.; Brufsky, A.; Azar, C.A.; et al. Seven-Year Follow-Up Assessment of Cardiac Function in NSABP B-31, a Randomized Trial Comparing Doxorubicin and Cyclophosphamide Followed by Paclitaxel (ACP) With ACP Plus Trastuzumab As Adjuvant Therapy for Patients With Node-Positive, Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer. J. Clin. Oncol. 2012, 30, 3792–3799. [Google Scholar] [CrossRef]
- Rushton, M.; Johnson, C.; Dent, S. Trastuzumab-Induced Cardiotoxicity: Testing a Clinical Risk Score in a Real-World Cardio-Oncology Population. Curr. Oncol. 2017, 24, 176–180. [Google Scholar] [CrossRef] [Green Version]
- Lyon, A.R.; Dent, S.; Stanway, S.; Earl, H.; Brezden-Masley, C.; Cohen-Solal, A.; Tocchetti, C.G.; Moslehi, J.J.; Groarke, J.D.; Bergler-Klein, J.; et al. Baseline Cardiovascular Risk Assessment in Cancer Patients Scheduled to Receive Cardiotoxic Cancer Therapies: A Position Statement and New Risk Assessment Tools from the C Ardio- O Ncology S Tudy G Roup of the H Eart F Ailure A Ssociation of the E Uropean S Ociety of C Ardiology in Collaboration with the I Nternational C Ardio- O Ncology S Ociety. Eur. J. Heart Fail. 2020, 22, 1945–1960. [Google Scholar] [CrossRef]
- Battisti, N.M.L.; Andres, M.S.; Lee, K.A.; Ramalingam, S.; Nash, T.; Mappouridou, S.; Senthivel, N.; Asavisanu, K.; Obeid, M.; Tripodaki, E.-S.; et al. Incidence of Cardiotoxicity and Validation of the Heart Failure Association-International Cardio-Oncology Society Risk Stratification Tool in Patients Treated with Trastuzumab for HER2-Positive Early Breast Cancer. Breast Cancer Res. Treat. 2021, 188, 149–163. [Google Scholar] [CrossRef]
- Seidman, A.; Hudis, C.; Pierri, M.K.; Shak, S.; Paton, V.; Ashby, M.; Murphy, M.; Stewart, S.J.; Keefe, D. Cardiac Dysfunction in the Trastuzumab Clinical Trials Experience. J. Clin. Oncol. 2002, 20, 1215–1221. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on Cancer Treatments and Cardiovascular Toxicity Developed under the Auspices of the ESC Committee for Practice Guidelines: The Task Force for Cancer Treatments and Cardiovascular Toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert Consensus for Multimodality Imaging Evaluation of Adult Patients during and after Cancer Therapy: A Report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2014, 27, 911–939. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Qadir, H.; Tai, F.; Croxford, R.; Austin, P.C.; Amir, E.; Calvillo-Argüelles, O.; Ross, H.; Lee, D.S.; Thavendiranathan, P. Characteristics and Outcomes of Women Developing Heart Failure After Early Stage Breast Cancer Chemotherapy: A Population-Based Matched Cohort Study. Circ. Heart Fail. 2021, 14, e008110. [Google Scholar] [CrossRef]
- Abdel-Qadir, H.; Fang, J.; Lee, D.S.; Tu, J.V.; Amir, E.; Austin, P.C.; Anderson, G.M. Importance of Considering Competing Risks in Time-to-Event Analyses: Application to Stroke Risk in a Retrospective Cohort Study of Elderly Patients With Atrial Fibrillation. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004580. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Qadir, H.; Thavendiranathan, P.; Austin, P.C.; Lee, D.S.; Amir, E.; Tu, J.V.; Fung, K.; Anderson, G.M. The Risk of Heart Failure and Other Cardiovascular Hospitalizations After Early Stage Breast Cancer: A Matched Cohort Study. JNCI J. Natl. Cancer Inst. 2019, 111, 854–862. [Google Scholar] [CrossRef] [Green Version]
- Slamon, D.; Wolfgang, E.; Nicholas, R.; Tadeusz, P.; Miguel, M.; Michael, P.; John, M.; John, G.; Arlene, C.; Marek, P.; et al. Adjuvant Trastuzumab in HER2-Positive Breast Cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar]
- Bobrowski, D.; Suntheralingam, S.; Calvillo-Argüelles, O.; Michalowska, M.; Amir, E.; Sacha Bhatia, R.; Thavendiranathan, P.; Abdel-Qadir, H. The Yield of Routine Cardiac Imaging in Breast Cancer Patients Receiving Trastuzumab-Based Treatment: A Retrospective Cohort Study. Can. J. Cardiol. 2020, 36, 1658–1666. [Google Scholar] [CrossRef] [PubMed]
- Heck, S.L.; Mecinaj, A.; Ree, A.H.; Hoffmann, P.; Schulz-Menger, J.; Fagerland, M.W.; Gravdehaug, B.; Røsjø, H.; Steine, K.; Geisler, J.; et al. Prevention of Cardiac Dysfunction During Adjuvant Breast Cancer Therapy (PRADA): Extended Follow-Up of a 2 × 2 Factorial, Randomized, Placebo-Controlled, Double-Blind Clinical Trial of Candesartan and Metoprolol. Circulation 2021, 143, 2431–2440. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Colombo, A.; Torrisi, R.; Sandri, M.T.; Civelli, M.; Salvatici, M.; Lamantia, G.; Colombo, N.; Cortinovis, S.; Dessanai, M.A.; et al. Trastuzumab-Induced Cardiotoxicity: Clinical and Prognostic Implications of Troponin I Evaluation. J. Clin. Oncol. 2010, 28, 3910–3916. [Google Scholar] [CrossRef]
- de Azambuja, E.; Procter, M.J.; van Veldhuisen, D.J.; Agbor-Tarh, D.; Metzger-Filho, O.; Steinseifer, J.; Untch, M.; Smith, I.E.; Gianni, L.; Baselga, J.; et al. Trastuzumab-Associated Cardiac Events at 8 Years of Median Follow-Up in the Herceptin Adjuvant Trial (BIG 1-01). J. Clin. Oncol. 2014, 32, 2159–2165. [Google Scholar] [CrossRef]
- Yu, A.F.; Flynn, J.R.; Moskowitz, C.S.; Scott, J.M.; Oeffinger, K.C.; Dang, C.T.; Liu, J.E.; Jones, L.W.; Steingart, R.M. Long-Term Cardiopulmonary Consequences of Treatment-Induced Cardiotoxicity in Survivors of ERBB2 -Positive Breast Cancer. JAMA Cardiol. 2020, 5, 309. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients N = 629 | CTRCD N = 151 | No CTRCD N = 478 | p Value | |
|---|---|---|---|---|
| Age, years ± SD | 52.4 ± 10.9 | 52.7 ± 10.9 | 52.4 ± 10.9 | 0.827 |
| Tumor laterality, n (%) | 0.689 | |||
| Left | 341 (54) | 79 (52) | 262 (55) | |
| Right | 268 (43) | 68 (45) | 200 (42) | |
| Bilateral | 21 (3) | 4 (3) | 17 (4) | |
| Stage, n (%) | 0.152 | |||
| 1 | 127 (20) | 23 (15) | 104 (22) | |
| 2 | 329 (52) | 80 (53) | 249 (52) | |
| 3 | 173 (28) | 48 (32) | 125 (26) | |
| Hormone receptor positive (either ER/PR), n (%) | 413 (66) | 98 (65) | 315 (66) | 0.821 |
| Post-menopausal status, n (%) | 309 (49) | 72 (48) | 237 (50) | 0.709 |
| Surgery (mastectomy or lumpectomy), n (%) | 622 (99) | 149 (99) | 473 (99) | 0.776 |
| Anthracycline received, n (%) | 568 (90) | 138 (91) | 430 (90) | 0.604 |
| Cumulative anthracycline, mg/m2 ± SD | 272.4 ± 76 | 275.6 ± 80 | 260 ± 75 | 0.061 |
| Radiotherapy, n (%) | 493 (78) | 127 (84) | 366 (77) | 0.499 |
| Diabetes, n (%) | 44 (7) | 11 (7) | 33 (7) | 0.856 |
| Hypertension, n (%) | 110 (18) | 30 (20) | 80 (17) | 0.391 |
| Dyslipidemia, n (%) | 83 (13) | 25 (17) | 58 (12) | 0.169 |
| Smoker (current), n (%) | 46 (7) | 13 (9) | 33 (7) | 0.476 |
| Smoker (Ex), n (%) | 122 (19) | 31 (21) | 91 (19) | 0.723 |
| At least 1 CVRF, n (%) | 402 (64) | 106 (70) | 296 (62) | 0.065 |
| Coronary artery disease, n (%) | 16 (3) | 3 (2) | 13 (3) | 0.618 |
| Heart failure, n (%) | 5 (1) | 1 (1) | 4 (1) | 0.833 |
| Atrial fibrillation, n (%) | 12 (2) | 5 (3) | 7 (2) | 0.148 |
| Baseline LVEF, % ± SD | 64 ± 7 | 62 ± 7 | 65 ± 7 | 0.001 |
| Imaging modality, n (%) | 0.010 | |||
| MUGA | 440 (70) | 93 (62) | 347 (73) | |
| Echo | 189 (30) | 58 (38) | 131 (27) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suntheralingam, S.; Fan, C.-P.S.; Calvillo-Argüelles, O.; Abdel-Qadir, H.; Amir, E.; Thavendiranathan, P. Evaluation of Risk Prediction Models to Identify Cancer Therapeutics Related Cardiac Dysfunction in Women with HER2+ Breast Cancer. J. Clin. Med. 2022, 11, 847. https://doi.org/10.3390/jcm11030847
Suntheralingam S, Fan C-PS, Calvillo-Argüelles O, Abdel-Qadir H, Amir E, Thavendiranathan P. Evaluation of Risk Prediction Models to Identify Cancer Therapeutics Related Cardiac Dysfunction in Women with HER2+ Breast Cancer. Journal of Clinical Medicine. 2022; 11(3):847. https://doi.org/10.3390/jcm11030847
Chicago/Turabian StyleSuntheralingam, Sivisan, Chun-Po Steve Fan, Oscar Calvillo-Argüelles, Husam Abdel-Qadir, Eitan Amir, and Paaladinesh Thavendiranathan. 2022. "Evaluation of Risk Prediction Models to Identify Cancer Therapeutics Related Cardiac Dysfunction in Women with HER2+ Breast Cancer" Journal of Clinical Medicine 11, no. 3: 847. https://doi.org/10.3390/jcm11030847
APA StyleSuntheralingam, S., Fan, C.-P. S., Calvillo-Argüelles, O., Abdel-Qadir, H., Amir, E., & Thavendiranathan, P. (2022). Evaluation of Risk Prediction Models to Identify Cancer Therapeutics Related Cardiac Dysfunction in Women with HER2+ Breast Cancer. Journal of Clinical Medicine, 11(3), 847. https://doi.org/10.3390/jcm11030847