
Risk Factors and Surgical Management of Recurrent Herniation after Full-Endoscopic Lumbar Discectomy Using Interlaminar Approach


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Surgical Procedures and Data Collection
2.2.1. Surgical Procedure for Primary FED-IL
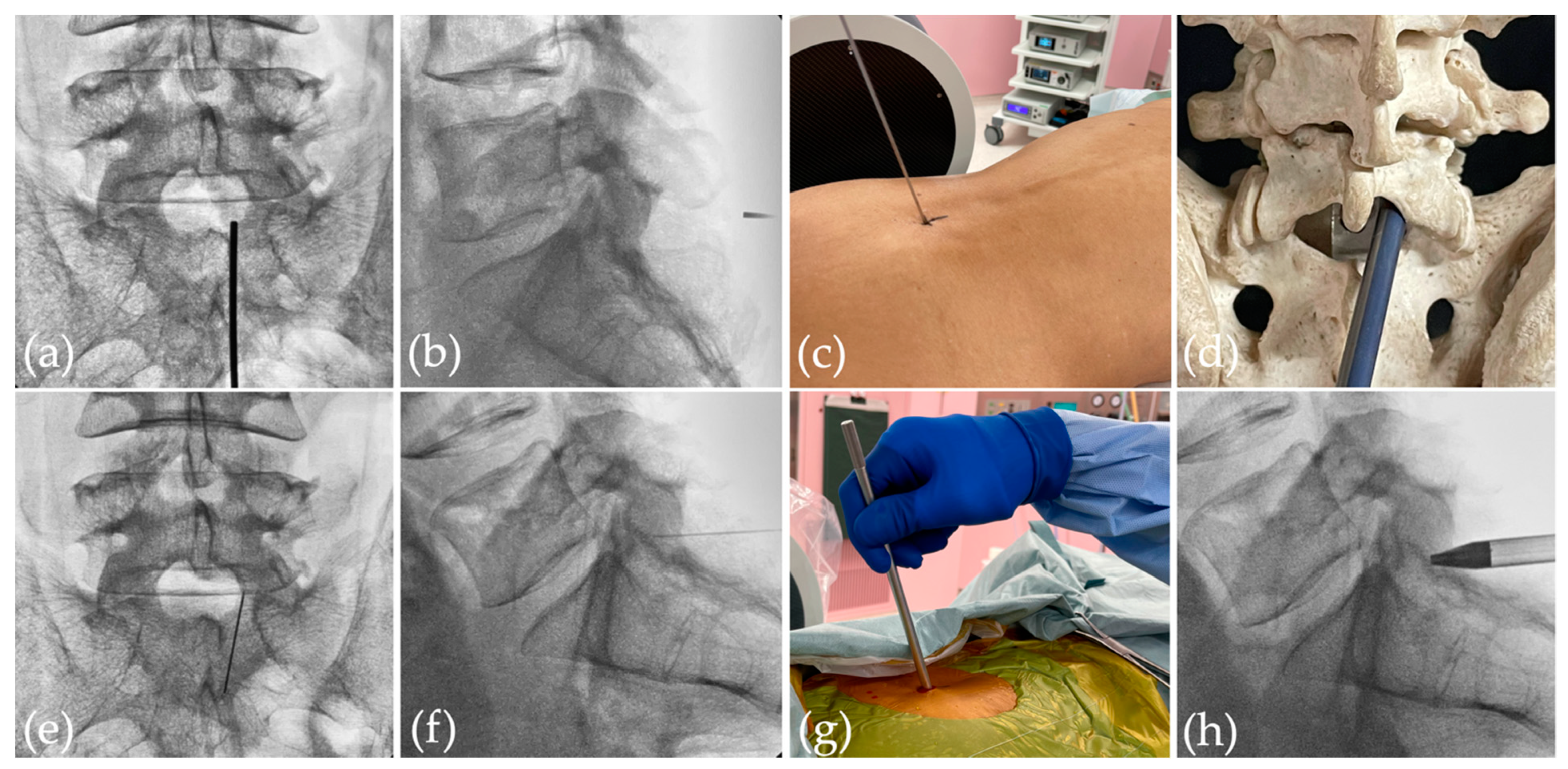
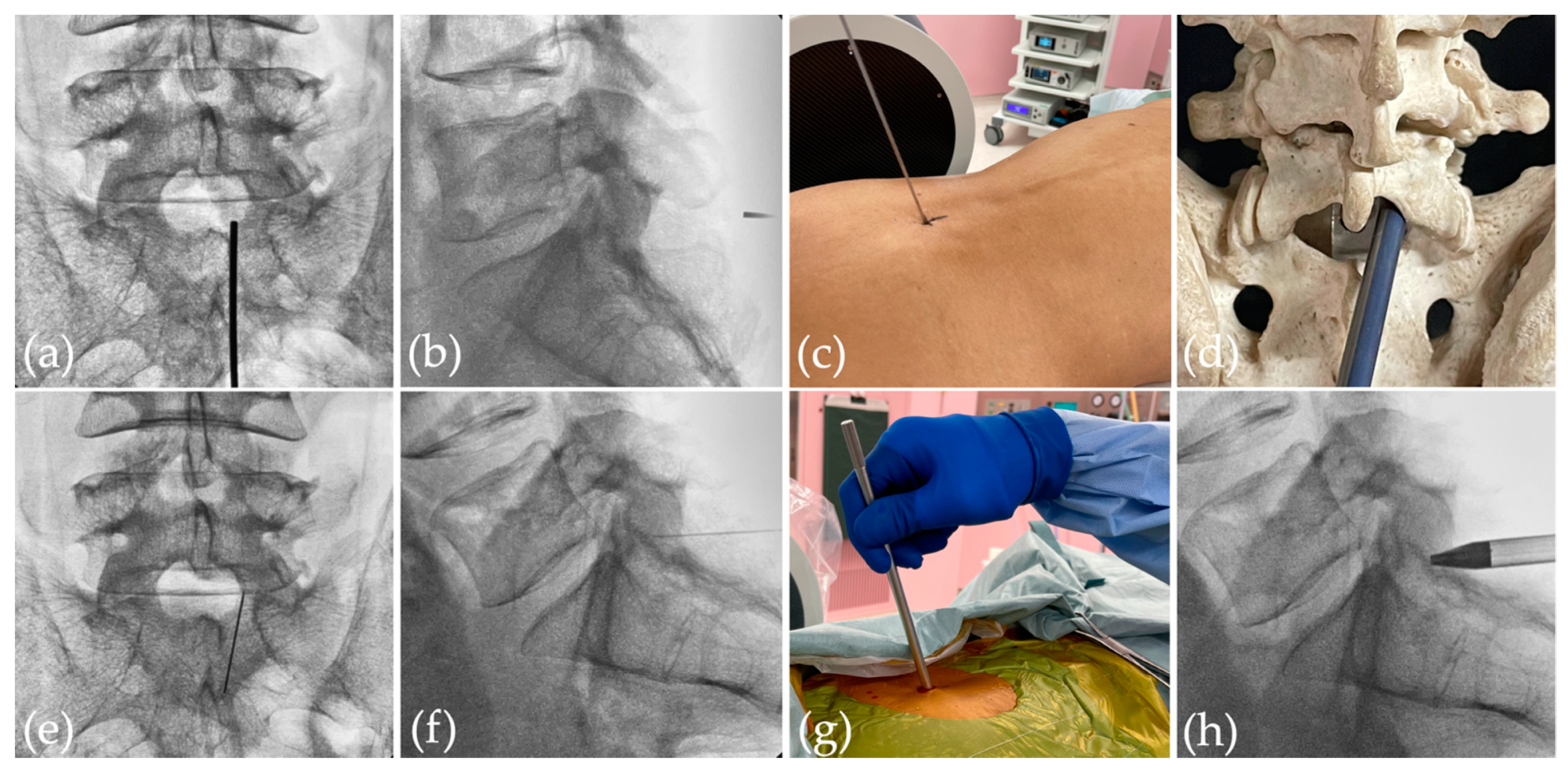
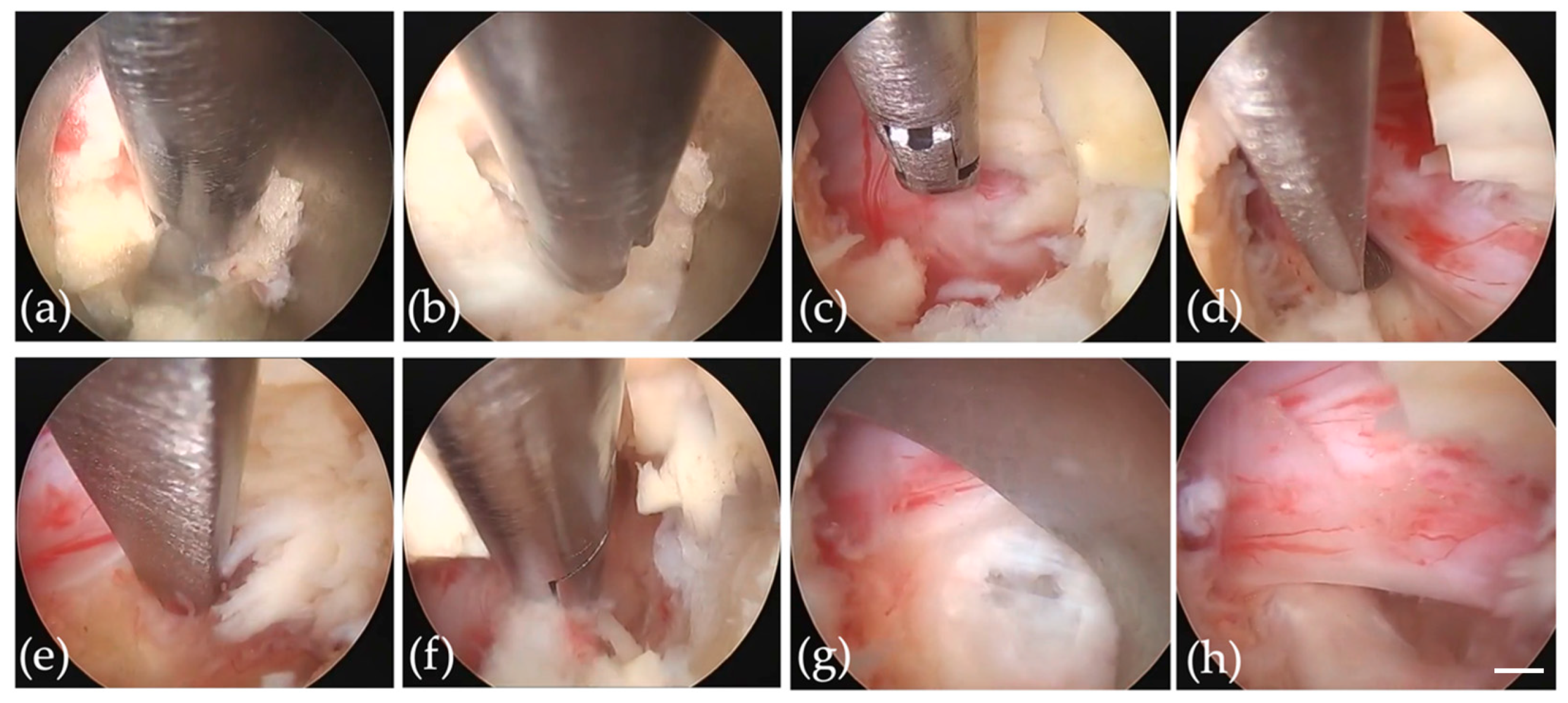
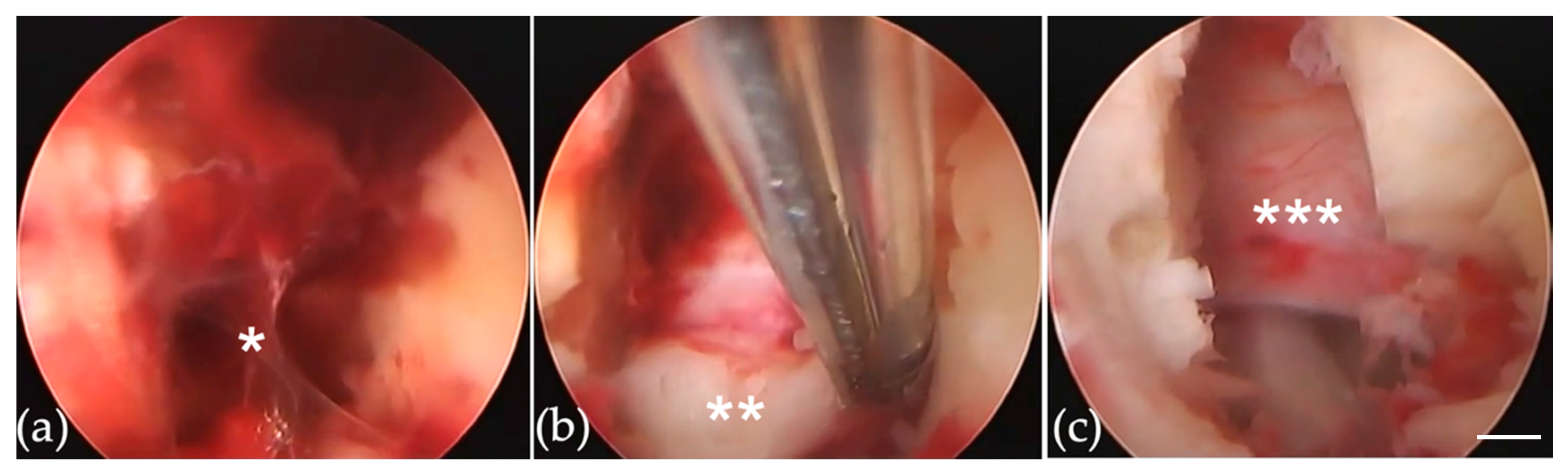
2.2.2. Re-FED-IL for Very Early Recurrent Herniation
2.2.3. Re-FED-IL for Early-to-Late Recurrent Herniation
2.2.4. Minimally Invasive Surgery (MIS) Posterior Lumbar Interbody Fusion (PLIF) for Recurrent Herniation
2.3. Evaluated Data
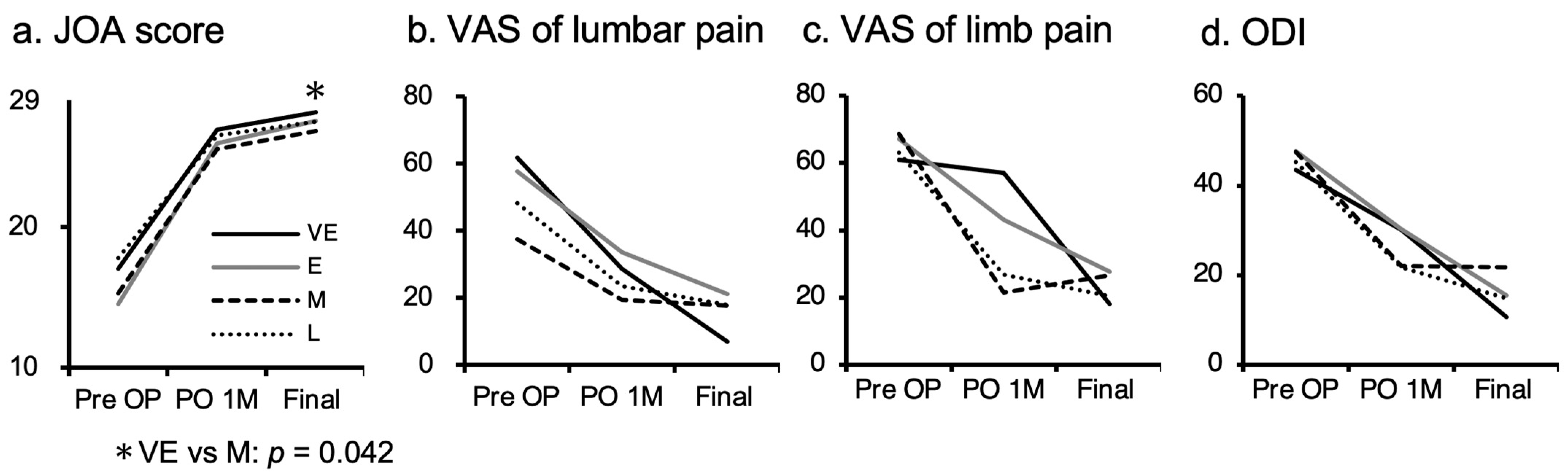
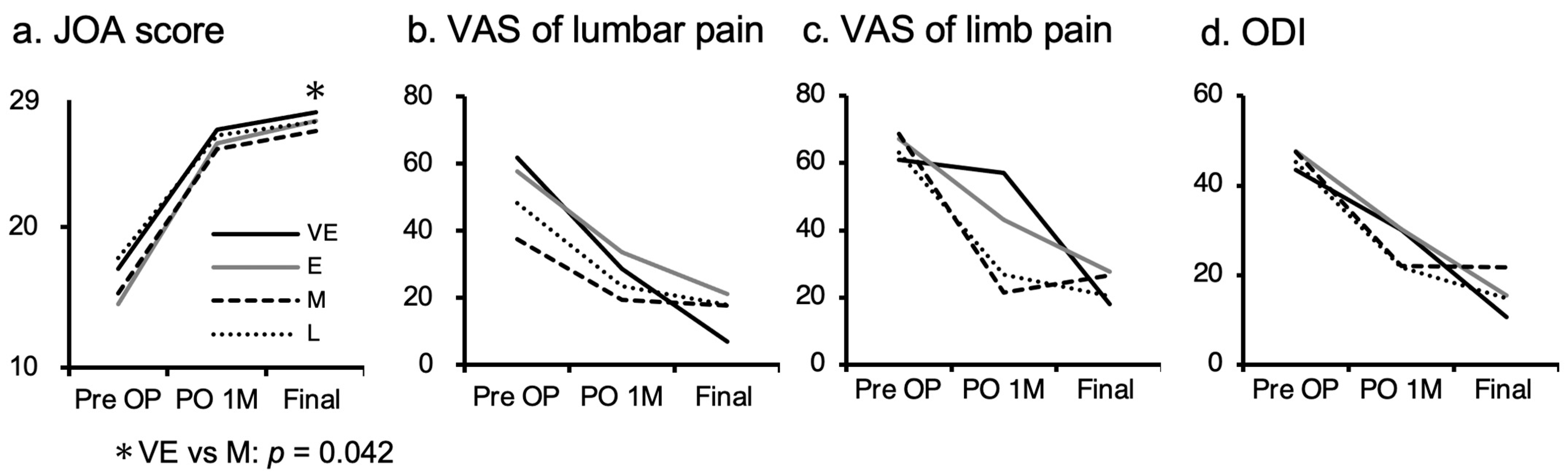
2.4. Clinical Assessment
2.5. Ethics Approval and Consent to Participate
2.6. Data Analysis
3. Results
3.1. Demographics and Clinical Characteristics
3.2. Radiological Characteristics
3.3. Case of Very Early Group
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lurie, J.D.; Tosteson, T.D.; Tosteson, A.N.; Zhao, W.; Morgan, T.S.; Abdu, W.A.; Herkowitz, H.; Weinstein, J.N. Surgical versus nonoperative treatment for lumbar disc herniation: Eight-year results for the spine patient outcomes research trial. Spine 2014, 39, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Ruan, W.; Feng, F.; Liu, Z.; Xie, J.; Cai, L.; Ping, A. Comparison of percutaneous endoscopic lumbar discectomy versus open lumbar microdiscectomy for lumbar disc herniation: A meta-analysis. Int. J. Surg. 2016, 31, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Minamide, A.; Yoshida, M.; Yamada, H.; Nakagawa, Y.; Hashizume, H.; Iwasaki, H.; Tsutsui, S. Clinical outcomes after microendoscopic laminotomy for lumbar spinal stenosis: A 5-year follow-up study. Eur. Spine J. 2015, 24, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: A prospective, randomized, controlled study. Spine 2008, 208, 931–939. [Google Scholar] [CrossRef] [Green Version]
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. Use of newly developed instruments and endoscopes: Full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J. Neurosurg. Spine 2007, 6, 521–530. [Google Scholar] [CrossRef]
- Ruetten, S.; Komp, M.; Godolias, G. A New full-endoscopic technique for the interlaminar operation of lumbar disc herniations using 6-mm endoscopes: Prospective 2-year results of 331 patients. Minim. Invasive Neurosurg. 2006, 49, 80–87. [Google Scholar] [CrossRef]
- Ruetten, S.; Komp, M.; Godolias, G. An extreme lateral access for the surgery of lumbar disc herniations inside the spinal canal using the full-endoscopic uniportal transforaminal approach-technique and prospective results of 463 patients. Spine 2005, 30, 2570–2578. [Google Scholar] [CrossRef]
- Phan, K.; Xu, J.; Schultz, K.; Alvi, M.A.; Lu, V.M.; Kerezoudis, P.; Maloney, P.R.; Murphy, M.E.; Mobbs, R.J.; Bydon, M. Full-endoscopic versus micro-endoscopic and open discectomy: A systematic review and meta-analysis of outcomes and complications. Clin. Neurol. Neurosurg. 2017, 154, 1–12. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Sivabalan, P.; Li, J. Minimally invasive surgery compared to open spinal fusion for the treatment of degenerative lumbar spine pathologies. J. Clin. Neurosci. 2012, 19, 829–835. [Google Scholar] [CrossRef]
- Dabbs, V.M.; Dabbs, L.G. Correlation between disc height narrowing and low back pain. Spine 1990, 15, 1366–1369. [Google Scholar] [CrossRef]
- Pesenti, S.; Lafage, R.; Stein, D.; Elysee, J.C.; Lenke, L.G.; Schwab, F.J.; Kim, H.J.; Lafage, V. The amount of proximal lumbar Lordosis is related to pelvic incidence. Clin. Orthop. Relat. Res. 2018, 476, 1603–1611. [Google Scholar] [CrossRef] [PubMed]
- Fuson, R.L.; Sherman, M.; Vleet, J.V. The conduct of orthopaedic clinical trials. J. Bone Jt. Surg. Am. 1997, 79, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, J.N.; Lurie, J.D.; Tosteson, T.D.; Skinner, J.S.; Hanscom, B.; Tosteson, A.N.; Herkowitz, H.; Fischgrund, J.; Cammisa, F.P.; Albert, T.; et al. Surgical vs. nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006, 296, 2451–2459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atlas, S.J.; Keller, R.B.; Chang, Y.; Deyo, R.A.; Singer, D.E. Surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: Five-year outcomes from the Maine Lumbar Spine Study. Spine 2001, 26, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Peul, W.C.; van Houwelingen, H.C.; van den Hout, W.B.; Brand, R.; Eekhof, J.A.; Tans, J.T.; Thomeer, R.T.; Koes, B.W. Leiden-The Hague Spine Intervention Prognostic Study Group. Surgery versus prolonged conservative treatment for sciatica. N. Engl. J. Med. 2007, 356, 2245–2256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, K.C.; Kim, J.S.; Park, C.K. Percutaneous Endoscopic Lumbar Discectomy as an Alternative to Open Lumbar Microdiscectomy for Large Lumbar Disc Herniation. Pain Physician. 2016, 19, E291–E300. [Google Scholar] [PubMed]
- Choi, G.; Lee, S.H.; Raiturker, P.P.; Lee, S.; Chae, Y.S. Percutaneous endoscopic interlaminar discectomy for intracanalicular disc herniations at L5-S1 using a rigid working channel endoscope. Neurosurgery 2006, 58, ONS59–ONS68. [Google Scholar] [CrossRef] [Green Version]
- Wasinpongwanich, K.; Pongpirul, K.; Lwin, K.M.M.; Kesornsak, W.; Kuansongtham, V.; Ruetten, S. Full-Endoscopic Interlaminar Lumbar Discectomy: Retrospective Review of Clinical Results and Complications in 545 International Patients. World Neurosurg. 2019, 132, e922–e928. [Google Scholar] [CrossRef]
- Xie, T.H.; Zeng, J.C.; Li, Z.H.; Wang, L.; Nie, H.F.; Jiang, H.S.; Song, Y.M.; Kong, Q.Q. Complications of Lumbar Disc Herniation Following Full-endoscopic Interlaminar Lumbar Discectomy: A Large, Single-Center, Retrospective Study. Pain Physician 2017, 20, E379–E387. [Google Scholar]
- Choi, K.C.; Kim, J.S.; Ryu, K.S.; Kang, B.U.; Ahn, Y.; Lee, S.H. Percutaneous endoscopic lumbar discectomy for L5-S1 disc herniation: Transforaminal versus interlaminar approach. Pain Physician 2013, 16, 547–556. [Google Scholar]
- Yin, S.; Du, H.; Yang, W.; Duan, C.; Feng, C.; Tao, H. Prevalence of Recurrent Herniation Following Percutaneous Endoscopic Lumbar Discectomy: A Meta-Analysis. Pain Physician 2018, 21, 337–350. [Google Scholar] [PubMed]
- Kim, J.M.; Lee, S.H.; Ahn, Y.; Yoon, D.H.; Lee, C.D.; Lim, S.T. Recurrence after successful percutaneous endoscopic lumbar discectomy. Minim. Invasive Neurosurg. 2007, 50, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Marković, M.; Živković, N.; Milan, S.; Gavrilović, A.; Stojanović, D.; Aleksić, V.; Ruetten, S. Full-endoscopic interlaminar operations in lumbar compressive lesions surgery: Prospective study of 350 patients—“ENDOS” Study. J. Neurosurg. Sci. 2020, 64, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Passacantilli, E.; Lenzi, J.; Caporlingua, F.; Pescatori, L.; Lapadula, G.; Nardone, A.; Santoro, A. Endoscopic interlaminar approach for intracanal L5-S1 disc herniation: Classification of disc prolapse in relation to learning curve and surgical outcome. Asian J. Endosc. Surg. 2015, 8, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Liu, H.; Zhang, H.; Wang, H.; Zhang, C.; Zhang, Z.; Wu, J.; Tang, Y.; Zhou, Y. Risk Factors for Recurrent Herniation After Percutaneous Endoscopic Lumbar Discectomy. World Neurosurg. 2017, 100, 1–6. [Google Scholar] [CrossRef]
- Shimia, M.; Babaei-Ghazani, A.; Sadat, B.E.; Habibi, B.; Habibzadeh, A. Risk factors of recurrent lumbar disk herniation. Asian J. Neurosurg. 2013, 8, 93–96. [Google Scholar]
- Kim, K.T.; Lee, D.H.; Cho, D.C.; Sung, J.K.; Kim, Y.B. Preoperative Risk Factors for Recurrent Lumbar Disk Herniation in L5-S1. J. Spinal Disord. Tech. 2015, 28, E571–E577. [Google Scholar] [CrossRef]
- Miwa, S.; Yokogawa, A.; Kobayashi, T.; Nishimura, T.; Igarashi, K.; Inatani, H.; Tsuchiya, H. Risk factors of recurrent lumbar disc herniation: A single center study and review of the literature. J. Spinal Disord Tech. 2015, 28, E265–E269. [Google Scholar] [CrossRef]
- Akmal, M.; Kesani, A.; Anand, B.; Singh, A.; Wiseman, M.; Goodship, A. Effect of nicotine on spinal disc cells: A cellular mechanism for disc degeneration. Spine 2004, 29, 568–575. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Newcombe, R.L.; Chandran, K.N. Lumbar discectomy and the diabetic patient: Incidence and outcome. J. Clin. Neurosci. 2001, 8, 10–13. [Google Scholar] [CrossRef] [Green Version]
- Robinson, D.; Mirovsky, Y.; Halperin, N.; Evron, Z.; Nevo, Z. Changes in proteoglycans of intervertebral disc in diabetic patients. A possible cause of increased back pain. Spine 1998, 23, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.T.; Park, S.W.; Kim, Y.B. Disc height and segmental motion as risk factors for recurrent lumbar disc herniation. Spine 2009, 34, 2674–2678. [Google Scholar] [CrossRef] [PubMed]
- Chaojie, Y.; Xinli, Z.; Chong, L.; Shian, L.; Jinming, X.; Tuo, L.; Zide, Z.; Jiarui, C. Risk Factors for Recurrent L5–S1 Disc Herniation After Percutaneous Endoscopic Transforaminal Discectomy: A Retrospective Study. Med. Sci. Monit. 2020, 26, e919888-1–e919888-12. [Google Scholar]
- Carragee, E.J.; Han, M.Y.; Suen, P.W.; Kim, D. Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and annular competence. J. Bone Jt. Surg Am. 2003, 85, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Lu, H.; Shengwen, L.; Junhui, L.; Zhi, S.; Shunwu, F.; Fengdong, Z. Recurrent disc herniation following percutaneous endoscopic lumbar discectomy preferentially occurs when Modic changes are present. J. Orthop. Surg. Res. 2020, 15, 176. [Google Scholar]
- Kim, C.H.; Chung, C.K.; Park, C.S.; Choi, B.; Kim, M.J.; Park, B.J. Reoperation rate after surgery for lumbar herniated intervertebral disc disease: Nationwide cohort study. Spine 2013, 38, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Wang, H.; Zheng, W.; Li, C.; Wang, J.; Zhang, Z.; Huang, B.; Zhou, Y. Reoperation after lumbar disc surgery in two hundred and seven patients. Int. Orthop. 2013, 37, 1511–1517. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.S.; Braybrooke, J.; Newey, M.; Sell, P. A comparative study of the outcomes of primary and revision lumbar discectomy surgery. Bone Jt. J. 2013, 95–B, 90–94. [Google Scholar] [CrossRef]
- Hoogland, T.; van den Brekel-Dijkstra, K.; Schubert, M.; Miklitz, B. Endoscopic transforaminal discectomy for recurrent lumbar disc herniation: A prospective, cohort evaluation of 262 consecutive cases. Spine 2008, 33, 973–978. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.S.; Ogden, A.T.; Shafizadeh, S.; Fessler, R.G. Clinical outcomes after microendoscopic discectomy for recurrent lumbar disc herniation. Clin. Spine Surg. 2010, 23, 30–34. [Google Scholar] [CrossRef]
- El Shazly, A.A.; El Wardany, M.A.; Morsi, A.M. Recurrent lumbar disc herniation: A prospective comparative study of three surgical management procedures. Asian J. Neurosurg. 2013, 8, 139–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dower, A.; Chatterji, R.; Swart, A.; Winder, M.J. Surgical management of recurrent lumbar disc herniation and the role of fusion. J. Clin. Neurosci. 2016, 23, 44–50. [Google Scholar] [CrossRef]
- Shepard, N.; Cho, W. Recurrent Lumbar Disc Herniation: A Review. Glob. Spine J. 2019, 9, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Sun, W.; Fu, D.; Shen, Y.; Chen, Y.Y.; Wang, L.L. Update on biomaterials for prevention of epidural adhesion after lumbar laminectomy. J. Orthop. Translat. 2018, 13, 41–49. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Recurrent | Non-Recurrent | p Value | |
|---|---|---|---|---|
| Cases (total 909) | 65 | 844 | ||
| Mean age (years) | 50.3 | 48.4 | 0.42 | |
| Sex (Male:Female) | 44:21 | 590:254 | 0.71 | |
| Mean BMI (kg/m2) | 24 | 26 | 0.36 | |
| Smoking | + | 31 | 288 | 0.027 |
| − | 34 | 556 | ||
| DM | + | 13 | 84 | 0.011 |
| − | 52 | 760 | ||
| Disc height | 9.6 | 11.9 | <0.01 | |
| Lumbar lordosis (LL) | 32 | 34.5 | 0.16 | |
| Cobb angle | 3.0 | 3.3 | 0.66 | |
| Migration | + | 22 | 362 | 0.15 |
| − | 43 | 482 | ||
| Type | SE | 47 | 517 | 0.076 |
| non-SE (TE or SQ) | 18 | 327 | ||
| Modic | + | 31 | 112 | < 0.01 |
| − | 34 | 732 |
| Groups | Very Early (VE) | Early (E) | Midterm (M) | Long-Term (L) |
|---|---|---|---|---|
| Cases (total 65) | 7 | 14 | 17 | 27 |
| Period from 1st to 2nd OP | 0–14 days | 15 days–3 months | 3 months–1 year | >1 year |
| Mean period from 1st to 2nd OP | 0.3 months | 1.3 months | 6.9 months | 27.7 months |
| Mean age (years) | 42.9 | 49.6 | 47.8 | 54.1 * |
| Sex (Male:Female) | 6:1 | 9:5 | 9:8 | 20:7 |
| Mean BMI (kg/m2) | 23.9 | 22.9 | 24.1 | 24.6 |
| Reoperation procedure (FEDIL/TF/MEL/Open/Fusion) | 7/0/0/0/0 | 9/2/0/1/3 | 12/2/0/0/3 | 15/1/1/0/10 |
| Mean 1st OP time (min) | 59.1 | 61.7 | 71.3 | 72.4 |
| Mean post-1st OP hospitalization days | 7.4 | 3.3 | 3.1 | 4.3 |
| Mean 2nd OP time | 26.4 ** | 66.7 | 74.9 | 73.0 |
| Mean post-2nd OP hospitalization days | 4.0 *** | 7.7 | 6.5 | 10.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ono, K.; Ohmori, K.; Yoneyama, R.; Matsushige, O.; Majima, T. Risk Factors and Surgical Management of Recurrent Herniation after Full-Endoscopic Lumbar Discectomy Using Interlaminar Approach. J. Clin. Med. 2022, 11, 748. https://doi.org/10.3390/jcm11030748
Ono K, Ohmori K, Yoneyama R, Matsushige O, Majima T. Risk Factors and Surgical Management of Recurrent Herniation after Full-Endoscopic Lumbar Discectomy Using Interlaminar Approach. Journal of Clinical Medicine. 2022; 11(3):748. https://doi.org/10.3390/jcm11030748
Chicago/Turabian StyleOno, Koichiro, Kazuo Ohmori, Reiko Yoneyama, Osamu Matsushige, and Tokifumi Majima. 2022. "Risk Factors and Surgical Management of Recurrent Herniation after Full-Endoscopic Lumbar Discectomy Using Interlaminar Approach" Journal of Clinical Medicine 11, no. 3: 748. https://doi.org/10.3390/jcm11030748
APA StyleOno, K., Ohmori, K., Yoneyama, R., Matsushige, O., & Majima, T. (2022). Risk Factors and Surgical Management of Recurrent Herniation after Full-Endoscopic Lumbar Discectomy Using Interlaminar Approach. Journal of Clinical Medicine, 11(3), 748. https://doi.org/10.3390/jcm11030748