
Effect of CytoSorb Coupled with Hemodialysis on Interleukin-6 and Hemodynamic Parameters in Patients with Systemic Inflammatory Response Syndrome: A Retrospective Cohort Study
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. CytoSorb Treatment
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Patients’ and Procedures’ Characteristics
3.2. IL-6 and Clinical Outcomes
3.3. Septic Shock Patients
3.4. Predicted vs. Observed Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Newton, K.; Dixit, V.M. Signaling in innate immunity and inflammation. Cold Spring Harb. Perspect. Biol. 2012, 4, a006049. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.K. Pathophysiology of systemic inflammatory response syndrome and multiorgan dysfunction syndrome in acute pancreatitis. In Pancreatitis; Adams, D.B., Cotton, P.B., Zyromski, N.J., Windsor, J., Eds.; John Wiley and Sons: Hoboken, NJ, USA, 2017; pp. 29–37. [Google Scholar] [CrossRef]
- Chousterman, B.G.; Swirski, F.K.; Weber, G.F. Cytokine storm and sepsis disease pathogenesis. Semin. Immunopathol. 2017, 39, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Monard, C.; Rimmele, T.; Ronco, C. Extracorporeal Blood Purification Therapies for Sepsis. Blood Purif. 2019, 47 (Suppl. 3), 2–15. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Kudo, M.; Strober, W. Immunopathogenesis of pancreatitis. Mucosal Immunol. 2017, 10, 283–298. [Google Scholar] [CrossRef]
- Jou, C.; Shah, R.; Figueroa, A.; Patel, J.K. The Role of Inflammatory Cytokines in Cardiac Arrest. J. Intensive Care Med. 2020, 35, 219–224. [Google Scholar] [CrossRef]
- Jozwiak, M.; Bougouin, W.; Geri, G.; Grimaldi, D.; Cariou, A. Post-resuscitation shock: Recent advances in pathophysiology and treatment. Ann. Intensive Care 2020, 10, 170. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef]
- Leppaniemi, A.; Tolonen, M.; Tarasconi, A.; Segovia-Lohse, H.; Gamberini, E.; Kirkpatrick, A.W.; Ball, C.G.; Parry, N.; Sartelli, M.; Woolbrink, D.; et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J. Emerg. Surg. 2019, 14, 27. [Google Scholar] [CrossRef]
- Heering, P.; Morgera, S.; Schmitz, F.J.; Schmitz, G.; Willers, R.; Schultheiss, H.P.; Strauer, B.E.; Grabensee, B. Cytokine removal and cardiovascular hemodynamics in septic patients with continuous venovenous hemofiltration. Intensive Care Med. 1997, 23, 288–296. [Google Scholar] [CrossRef]
- Bellomo, R.; Tipping, P.; Boyce, N. Continuous veno-venous hemofiltration with dialysis removes cytokines from the circulation of septic patients. Crit. Care Med. 1993, 21, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Sander, A.; Armbruster, W.; Sander, B.; Daul, A.E.; Lange, R.; Peters, J. Hemofiltration increases IL-6 clearance in early systemic inflammatory response syndrome but does not alter IL-6 and TNF alpha plasma concentrations. Intensive Care Med. 1997, 23, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Van Deuren, M.; van der Meer, J.W. Hemofiltration in septic patients is not able to alter the plasma concentration of cytokines therapeutically. Intensive Care Med. 2000, 26, 1176–1178. [Google Scholar] [CrossRef]
- Kogelmann, K.; Jarczak, D.; Scheller, M.; Druner, M. Hemoadsorption by CytoSorb in septic patients: A case series. Crit. Care 2017, 21, 74. [Google Scholar] [CrossRef]
- Ankawi, G.; Xie, Y.; Yang, B.; Xie, Y.; Xie, P.; Ronco, C. What Have We Learned about the Use of Cytosorb Adsorption Columns? Blood Purif. 2019, 48, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Friesecke, S.; Stecher, S.S.; Gross, S.; Felix, S.B.; Nierhaus, A. Extracorporeal cytokine elimination as rescue therapy in refractory septic shock: A prospective single-center study. J. Artif. Organs 2017, 20, 252–259. [Google Scholar] [CrossRef]
- Schädler, D.; Pausch, C.; Heise, D.; Meier-Hellmann, A.; Brederlau, J.; Weiler, N.; Marx, G.; Putensen, C.; Spies, C.; Jörres, A.; et al. The effect of a novel extracorporeal cytokine hemoadsorption device on IL-6 elimination in septic patients: A randomized controlled trial. PLoS ONE 2017, 12, e0187015. [Google Scholar] [CrossRef]
- Hawchar, F.; Tomescu, D.; Träger, K.; Joskowiak, D.; Kogelmann, K.; Soukup, J.; Friesecke, S.; Jacob, D.; Gummert, J.; Faltlhauser, A.; et al. Final results of the International CytoSorb Registry. PLoS ONE 2022, 17, e0274315. [Google Scholar] [CrossRef]
- Jeschke, M.G.; van Baar, M.E.; Choudhry, M.A.; Chung, K.K.; Gibran, N.S.; Logsetty, S. Burn injury. Nat. Rev. Dis. Prim. 2020, 6, 11. [Google Scholar] [CrossRef]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Mélot, C.; Vincent, J. Serial Evaluation of the SOFA Score to Predict Outcome in Critically Ill Patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Headley, J.; Theriault, R.; Smith, T.L. Independent validation of APACHE II severity of illness score for predicting mortality in patients with breast cancer admitted to the intensive care unit. Cancer 1992, 70, 497–503. [Google Scholar] [CrossRef] [PubMed]
- R Developpment Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Brouwer, W.P.; Duran, S.; Kuijper, M.; Ince, C. Hemoadsorption with CytoSorb shows a de-creased observed versus expected 28-day all-cause mortality in ICU patients with septic shock: A propensity-score-weighted retrospective study. Crit. Care 2019, 23, 317. [Google Scholar] [CrossRef] [PubMed]
- Schittek, G.A.; Zoidl, P.; Eichinger, M.; Orlob, S.; Simonis, H.; Rief, M.; Metnitz, P.; Fellinger, T.; Soukup, J. Adsorption therapy in critically ill with septic shock and acute kidney injury: A retrospective and prospective cohort study. Ann. Intensive Care 2020, 10, 154. [Google Scholar] [CrossRef]
- Mehta, Y.; Mehta, C.; Kumar, A.; George, J.V.; Gupta, A.; Nanda, S.; Kochhar, G.; Raizada, A. Experience with hemoadsorption (CytoSorb®) in the management of septic shock patients. World J. Crit. Care Med. 2020, 9, 1–12. [Google Scholar] [CrossRef]
- Calabrò, M.G.; Febres, D.; Recca, G.; Lembo, R.; Fominskiy, E.; Scandroglio, A.M.; Zangrillo, A.; Pappalardo, F. Blood Purification with CytoSorb in Critically Ill Patients: Single-Center Preliminary Experience. Artif. Organs 2019, 43, 189–194. [Google Scholar] [CrossRef]
- Zuccari, S.; Damiani, E.; Domizi, R.; Scorcella, C.; D’Arezzo, M.; Carsetti, A.; Pantanetti, S.; Vannicola, S.; Casarotta, E.; Ranghino, A.; et al. Changes in Cytokines, Haemodynamics and Microcirculation in Patients with Sepsis/Septic Shock Under-going Continuous Renal Replacement Therapy and Blood Purification with CytoSorb. Blood Purif. 2020, 49, 107–113. [Google Scholar] [CrossRef]
- Garcia, R.U.; Walters, H.L.; Delius, R.E.; Aggarwal, S. Vasoactive inotropic score (VIS) as biomarker of short-term outcomes in adolescents after cardiothoracic surgery. Pediatr. Cardiol. 2016, 37, 271–277. [Google Scholar] [CrossRef]
- Na, S.J.; Chung, C.R.; Cho, Y.H.; Jeon, K.; Suh, G.Y.; Ahn, J.H.; Carriere, K.C.; Park, T.K.; Lee, G.Y.; Lee, J.M.; et al. Vasoactive Inotropic Score as a Predictor of Mortality in Adult Patients with Cardiogenic Shock: Medical Therapy Versus ECMO. Rev. Esp. Cardiol. 2019, 72, 40–47. [Google Scholar] [CrossRef]
- Koponen, T.; Karttunen, J.; Musialowicz, T.; Pietiläinen, L.; Uusaro, A.; Lahtinen, P. Vasoactive-inotropic score and the prediction of morbidity and mortality after cardiac surgery. Br. J. Anaesth. 2019, 122, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Nogi, K.; Shiraishi, A.; Yamamoto, R.; Sasano, M.; Matsumoto, T.; Karumai, T.; Hayashi, Y. Intermittent Hemodialysis for Managing Metabolic Acidosis During Resuscitation of Septic Shock: A Descriptive Study. Crit. Care Explor. 2019, 1, e0065. [Google Scholar] [CrossRef] [PubMed]
- Prkno, A.; Wacker, C.; Brunkhorst, F.M.; Schlattmann, P. Procalcitonin-guided therapy in intensive care unit patients with severe sepsis and septic shock—A systematic review and meta-analysis. Crit. Care 2013, 17, R291. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.L.; Snider, R.; Nylen, E.S. Procalcitonin in sepsis and systemic inflammation: A harmful biomarker and a therapeutic target. Br. J. Pharmacol. 2010, 159, 253–264. [Google Scholar] [CrossRef]
- Montagnana, M.; Lippi, G.; Tessitore, N.; Salvagno, G.L.; Danese, E.; Targher, G.; Lupo, A.; Guidi, G. Procalcitonin values after dialysis is closely related to type of dialysis membrane. Scand. J. Clin. Lab. Investig. 2009, 69, 703–707. [Google Scholar] [CrossRef]
- Herget-Rosenthal, S.; Marggraf, G.; Pietruck, F.; Hüsing, J.; Strupat, M.; Philipp, T.; Kribben, A. Procalcitonin for accurate detection of infection in haemodialysis. Nephrol. Dial. Transplant. 2001, 16, 975–979. [Google Scholar] [CrossRef]
- Level, C.; Chauveau, P.; Guisset, O.; Cazin, M.C.; Lasseur, C.; Gabinsky, C.; Winnock, S.; Montaudon, D.; Bedry, R.; Nouts, C.; et al. Mass transfer, clearance and plasma concentration of procalcitonin during continuous venovenous hemofiltration in patients with septic shock and acute oliguric renal failure. Crit. Care 2003, 7, R160–R166. [Google Scholar] [CrossRef]
- Mori, K.; Noguchi, M.; Sumino, Y.; Sato, F.; Mimata, H. Use of procalcitonin in patients on chronic hemodialysis: Procalcitonin is not related with increased serum calcitonin. ISRN Urol. 2012, 2012, 431859. [Google Scholar] [CrossRef][Green Version]
- Gruda, M.C.; Ruggeberg, K.G.; O’Sullivan, P.; Guliashvili, T.; Scheirer, A.R.; Golobish, T.D.; Capponi, V.J.; Chan, P.P. Broad adsorption of sepsis-related PAMP and DAMP molecules, mycotoxins, and cytokines from whole blood using CytoSorb® sorbent porous polymer beads. PLoS ONE 2018, 13, e0191676. [Google Scholar] [CrossRef]
- Wagner, D.P.; Knaus, W.A.; Draper, E.A. Statistical validation of a severity of illness measure. Am. J. Public Health 1983, 73, 878–884. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Demographics | |
| N | 118 |
| Age (years) | 63 [51–73] |
| Female gender | 34 (29%) |
| BMI | 27.6 [26.0, 30.4] |
| Comorbidities: | |
| No comorbidities | 30 (25%) |
| Hypertension | 62 (53%) |
| Diabetes mellitus | 26 (22%) |
| Peripheral artery disease | 7 (6%) |
| Heart failure | 8 (7%) |
| COPD | 13 (11%) |
| Indication for CytoSorb treatment: | |
| Septic shock | 81 (69%) |
| SIRS—after OHCA or IHCA | 19 (16%) |
| SIRS—acute pancreatitis | 7 (6%) |
| other | 11 (9%) |
| Vital signs: | |
| MAP (mmHg) | 69.6 ± 12.8 |
| Heart rate (1/min) | 105 ± 22 |
| Organ support: | |
| Mechanical ventilation | 114 (97%) |
| ECMO support | 19 (16%) |
| Renal replacement therapy: | |
| intermittent hemodialysis | 107 (91%) |
| CRRT | 10 (8%) |
| none (pure hemoperfusion) | 1 (1%) |
| Medications: | |
| Vasoactive support | 118 (100%) |
| Hydrocortisone | 90 (76%) |
| Antibiotic treatment | 113 (96%) |
| Immunosuppression * | 15 (13%) |
| Laboratory parameters: | |
| lactate (mmol/L) | 6.3 [3.8–11.9] |
| IL-6 (ng/L) | 5000 [800–5000] |
| pH | 7.3 [7.2–7.4] |
| creatinine (µmol/L) | 200 [139–308] |
| Disease severity scores: | |
| VIS | 70 [43–101] |
| SOFA | 14 [12–16] |
| APACHE II | 33 [28–37] |
| Mortality | |
| 3-day mortality | 30 (25%) |
| 10-day mortality | 47 (40%) |
| 28-day mortality | 66 (56%) |
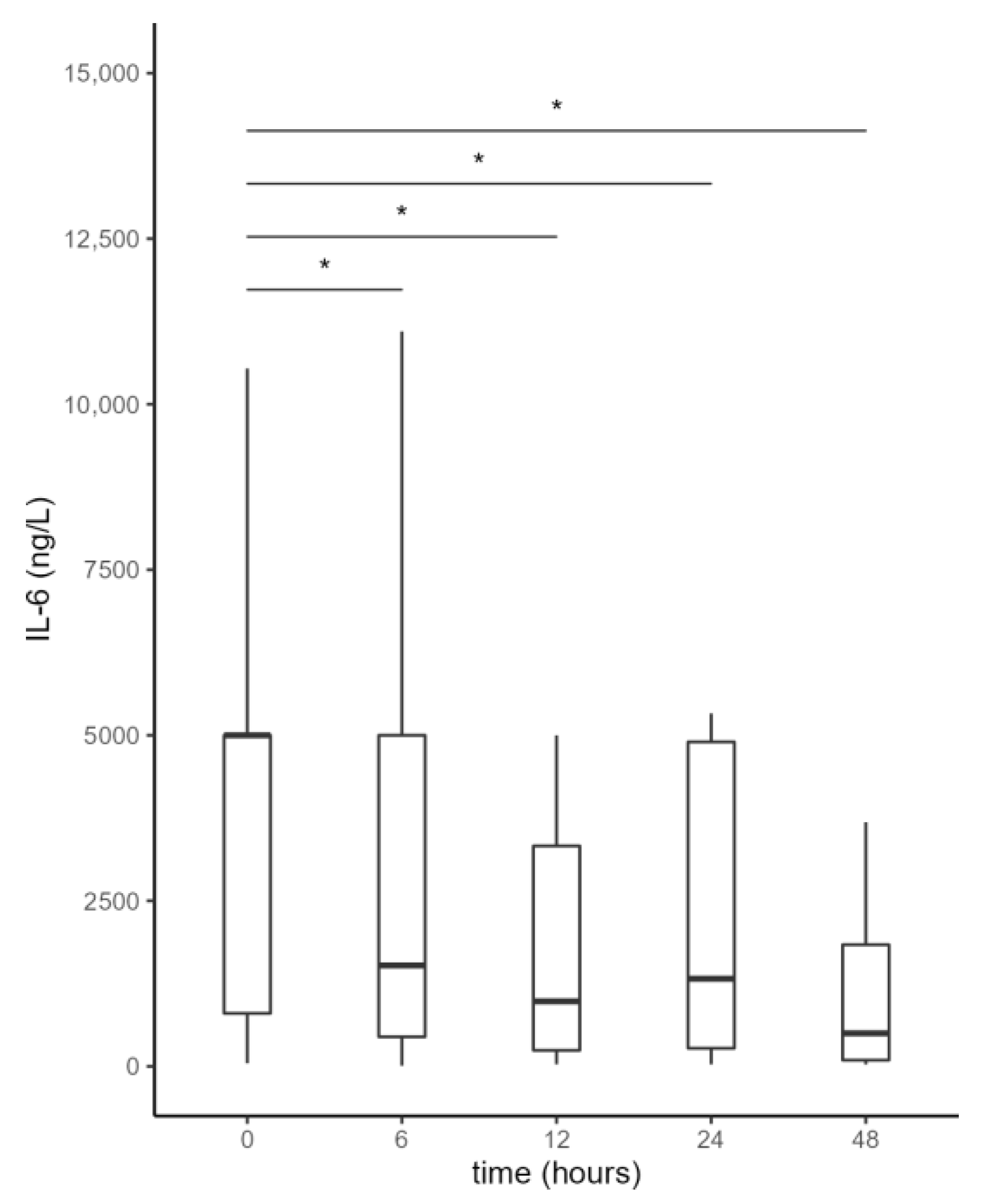
| Time (h) | 0 | 6 | 12 | 24 | 48 |
|---|---|---|---|---|---|
| IL-6 (ng/mL) | 5000 [800–5000] | 1524 [446–5000] | 982 [242–3329] | 1323 [273–4900] | 499 [94–1837] |
| Compared to time 0 (p) | / | <0.001 | <0.001 | <0.001 | <0.001 |
| Compared to previous time category (p) | / | <0.001 | 0.027 | 0.002 | <0.001 |
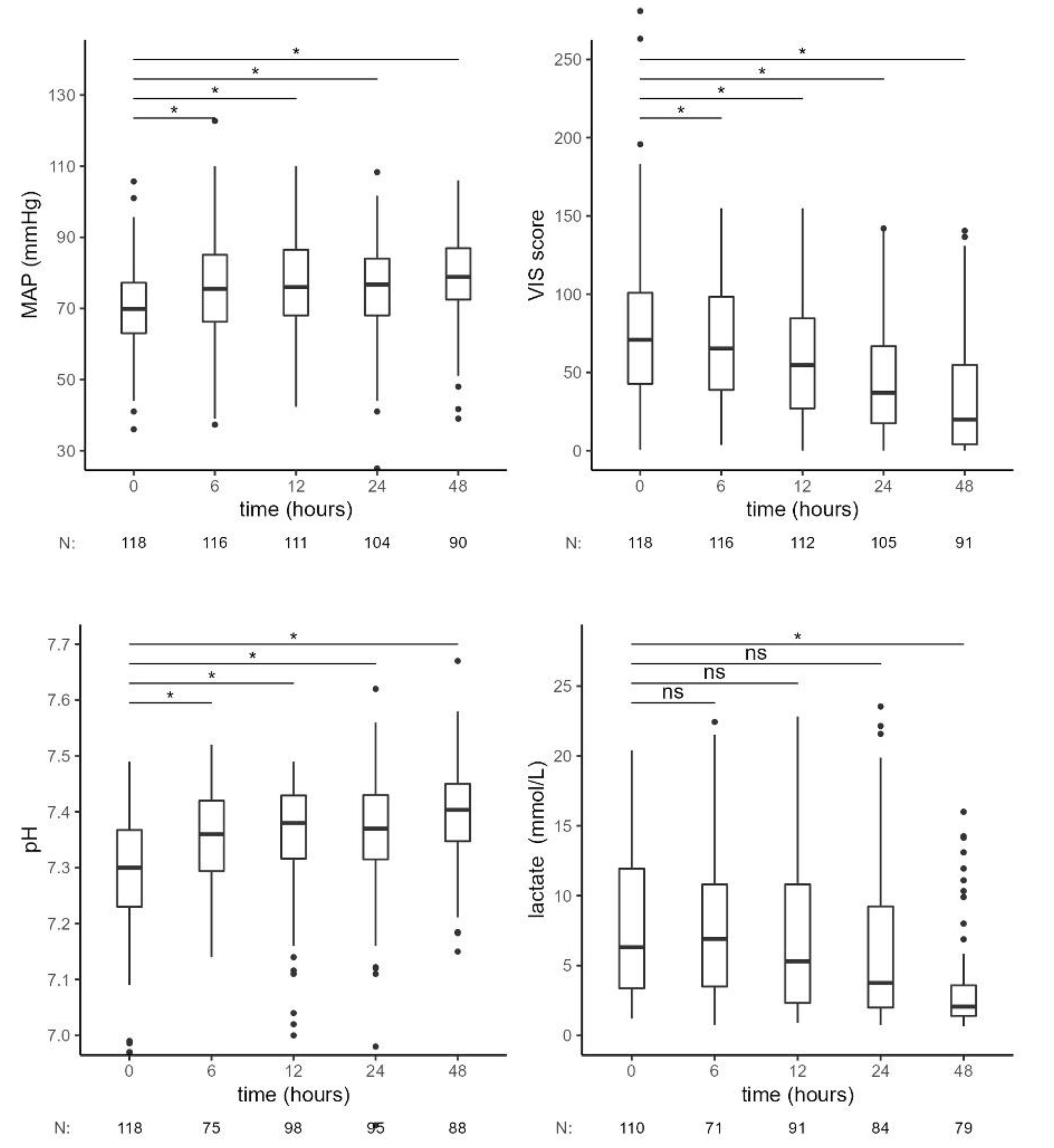
| Time (h) | 0 | 6 | 12 | 24 | 48 |
|---|---|---|---|---|---|
| MAP (mmHg) | 70 [63–77] | 76 [66–85] | 76 [68–87] | 77 [68–84] | 79 [72–87] |
| p-value | / | <0.001 | <0.001 | 0.002 | <0.001 |
| VIS | 71 [43–101] | 65 [39–98] | 55 [27–85] | 37 [18–67] | 20 [4–55] |
| p-value | / | 0.009 | <0.001 | <0.001 | <0.001 |
| pH | 7.30 [7.23–7.37] | 7.36 [7.29–7.42] | 7.38 [7.32–7.43] | 7.37 [7.31–7.43] | 7.40 [7.35–7.45] |
| p-value | / | <0.001 | <0.001 | <0.001 | <0.001 |
| s-lactate (mmol/L) | 6.31 [3.38–11.94] | 6.90 [3.50–10.80] | 5.30 [2.33–10.81] | 3.76 [2.00–9.23] | 2.06 [1.40–3.58] |
| p-value | / | 0.484 | 0.124 | 0.156 | <0.001 |
| Time (h) | 0 | 6 | 12 | 24 | 48 |
|---|---|---|---|---|---|
| IL-6 (ng/mL) | 5000 [1639–5000] | 2804 [885–5000] | 1474 [297–4943] | 2236 [672–4917] | 958 [422–2147] |
| p-value | / | 0.002 | 0.003 | <0.001 | <0.001 |
| MAP (mmHg) | 68 [63–75] | 73 [66–82] | 76 [6–84] | 76 [67–82] | 79 [73–86] |
| p-value | / | <0.001 | <0.001 | 0.003 | <0.001 |
| VIS | 72 [44–100] | 65 [40–95] | 60 [36–88] | 50 [29–75] | 28 [6–59] |
| p-value | / | 0.006 | 0.001 | <0.001 | <0.001 |
| pH | 7.29 [7.22–7.34] | 7.37 [7.30–7.42] | 7.38 [7.32–7.43] | 7.37 [7.32–7.42] | 7.39 [7.34–7.44] |
| p-value | / | <0.001 | <0.001 | <0.001 | <0.001 |
| lactate (mmol/L) | 7.1 [4.0–12.0] | 7.5 [4.3–10.3] | 5.3 [2.5–10.3] | 4.2 [2.3–10.6] | 2.3 [1.7–3.6] |
| p-value | / | 0.271 | 0.025 | 0.162 | <0.001 |
| PCT (µg/L) | 31 [9–89] | 35 [8–71] | 18 [7–68] | 30 [8–66] | 21 [7–55] |
| p-value | / | <0.001 | 0.036 | 0.009 | <0.001 |
| SOFA Group | Mortality—Reference | Mortality—Predicted | Mortality—Observed | p-Value |
|---|---|---|---|---|
| 10–11 | 46% | 8.3/18 | 5/18 (28%) | / |
| 12–14 | 80% | 29.6/37 | 22/37 (59%) | / |
| >14 | 90% | 46.8/52 | 38/52 (73%) | / |
| all | 85/107 (79%) | 65/107 (61%) | 0.005 |
| APACHE II Group | Mortality—Reference | Mortality—Predicted | Mortality Observed | p-Value |
|---|---|---|---|---|
| 15–19 | 27% | 1/2 | 0/2 (0%) | / |
| 20–24 | 50% | 4/8 | 3/8 (38%) | / |
| 25–29 | 65% | 20/31 | 15/31 (48%) | / |
| 30–34 | 80% | 20/25 | 15/25 (60%) | / |
| >34 | 89% | 47/52 | 43/52 (83%) | / |
| all | 92/118 (78%) | 76/118 (64%) | 0.031 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Persic, V.; Jerman, A.; Malgaj Vrecko, M.; Berden, J.; Gorjup, V.; Stecher, A.; Lukic, M.; Jereb, M.; Taleska Stupica, G.; Gubensek, J. Effect of CytoSorb Coupled with Hemodialysis on Interleukin-6 and Hemodynamic Parameters in Patients with Systemic Inflammatory Response Syndrome: A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 7500. https://doi.org/10.3390/jcm11247500
Persic V, Jerman A, Malgaj Vrecko M, Berden J, Gorjup V, Stecher A, Lukic M, Jereb M, Taleska Stupica G, Gubensek J. Effect of CytoSorb Coupled with Hemodialysis on Interleukin-6 and Hemodynamic Parameters in Patients with Systemic Inflammatory Response Syndrome: A Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(24):7500. https://doi.org/10.3390/jcm11247500
Chicago/Turabian StylePersic, Vanja, Alexander Jerman, Marija Malgaj Vrecko, Jernej Berden, Vojka Gorjup, Adela Stecher, Milica Lukic, Matjaz Jereb, Gordana Taleska Stupica, and Jakob Gubensek. 2022. "Effect of CytoSorb Coupled with Hemodialysis on Interleukin-6 and Hemodynamic Parameters in Patients with Systemic Inflammatory Response Syndrome: A Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 24: 7500. https://doi.org/10.3390/jcm11247500
APA StylePersic, V., Jerman, A., Malgaj Vrecko, M., Berden, J., Gorjup, V., Stecher, A., Lukic, M., Jereb, M., Taleska Stupica, G., & Gubensek, J. (2022). Effect of CytoSorb Coupled with Hemodialysis on Interleukin-6 and Hemodynamic Parameters in Patients with Systemic Inflammatory Response Syndrome: A Retrospective Cohort Study. Journal of Clinical Medicine, 11(24), 7500. https://doi.org/10.3390/jcm11247500