
Esophageal Pressure Measurement in Acute Hypercapnic Respiratory Failure Due to Severe COPD Exacerbation Requiring NIV—A Pilot Safety Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Noninvasive Ventilation
2.2. Pes Measurement Procedure
2.3. Analyzed Parameters and Objectives
2.4. Data Analysis
3. Results
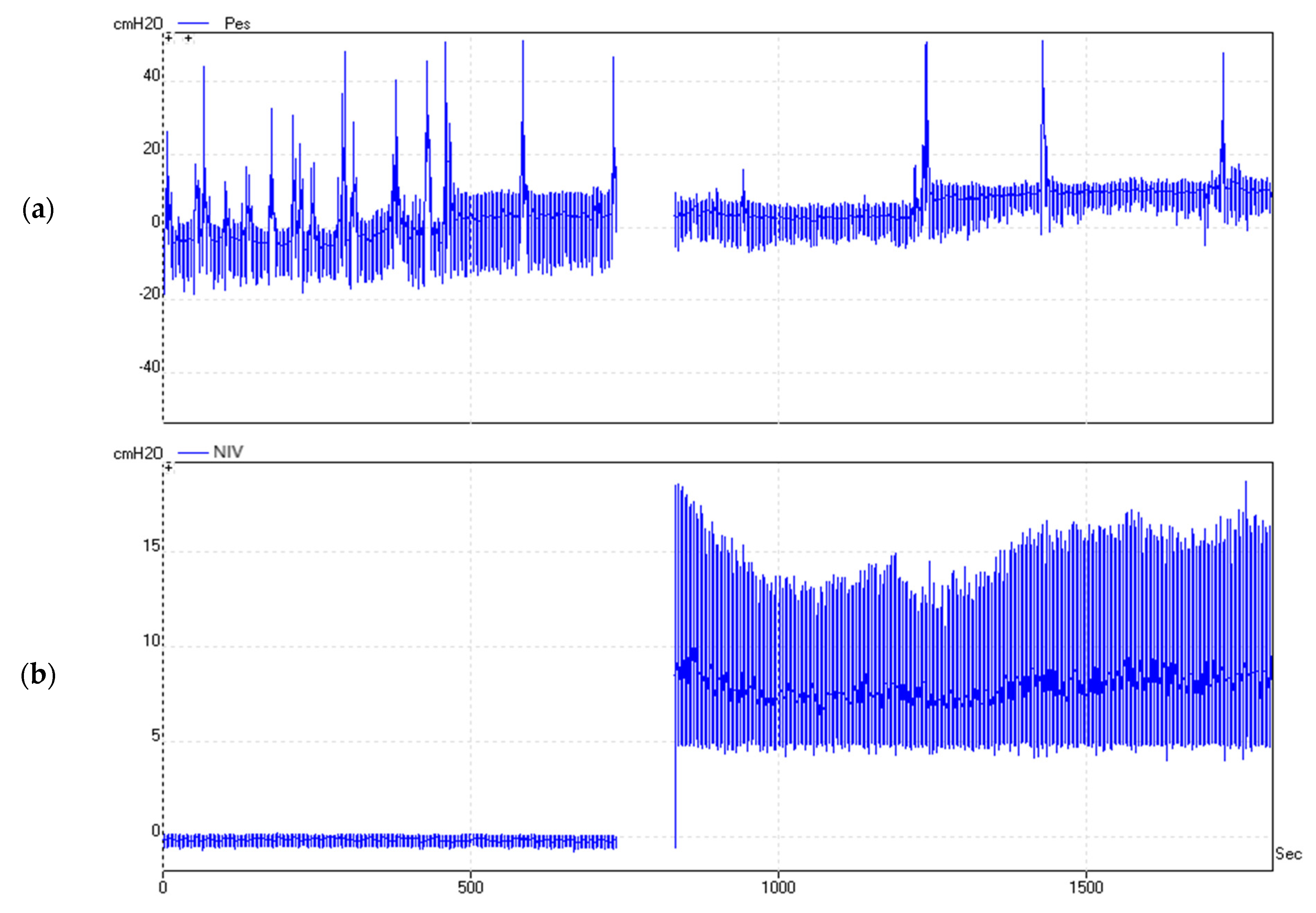
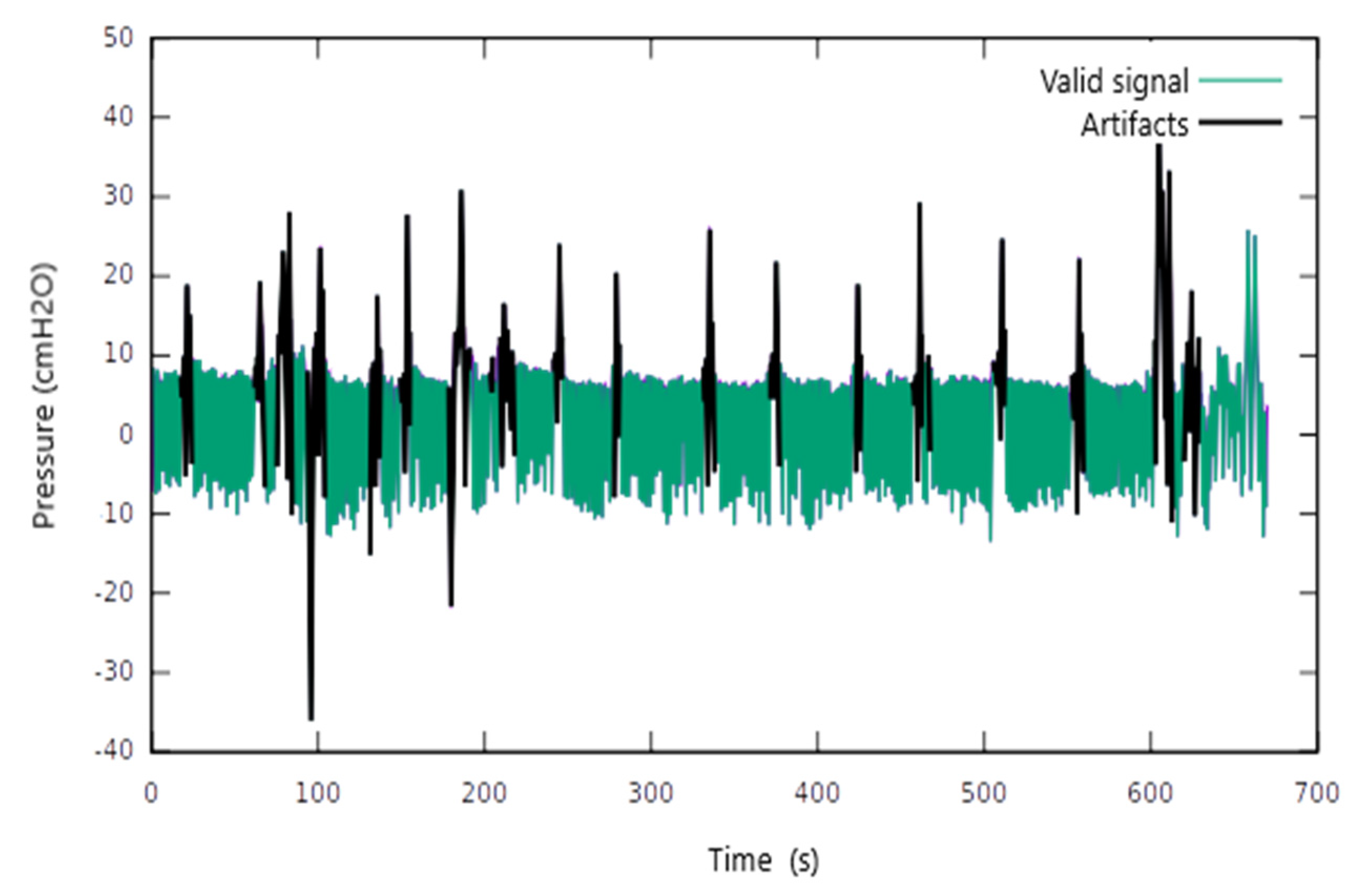
3.1. Pes Measurement: Raw Results and Signal Analysis
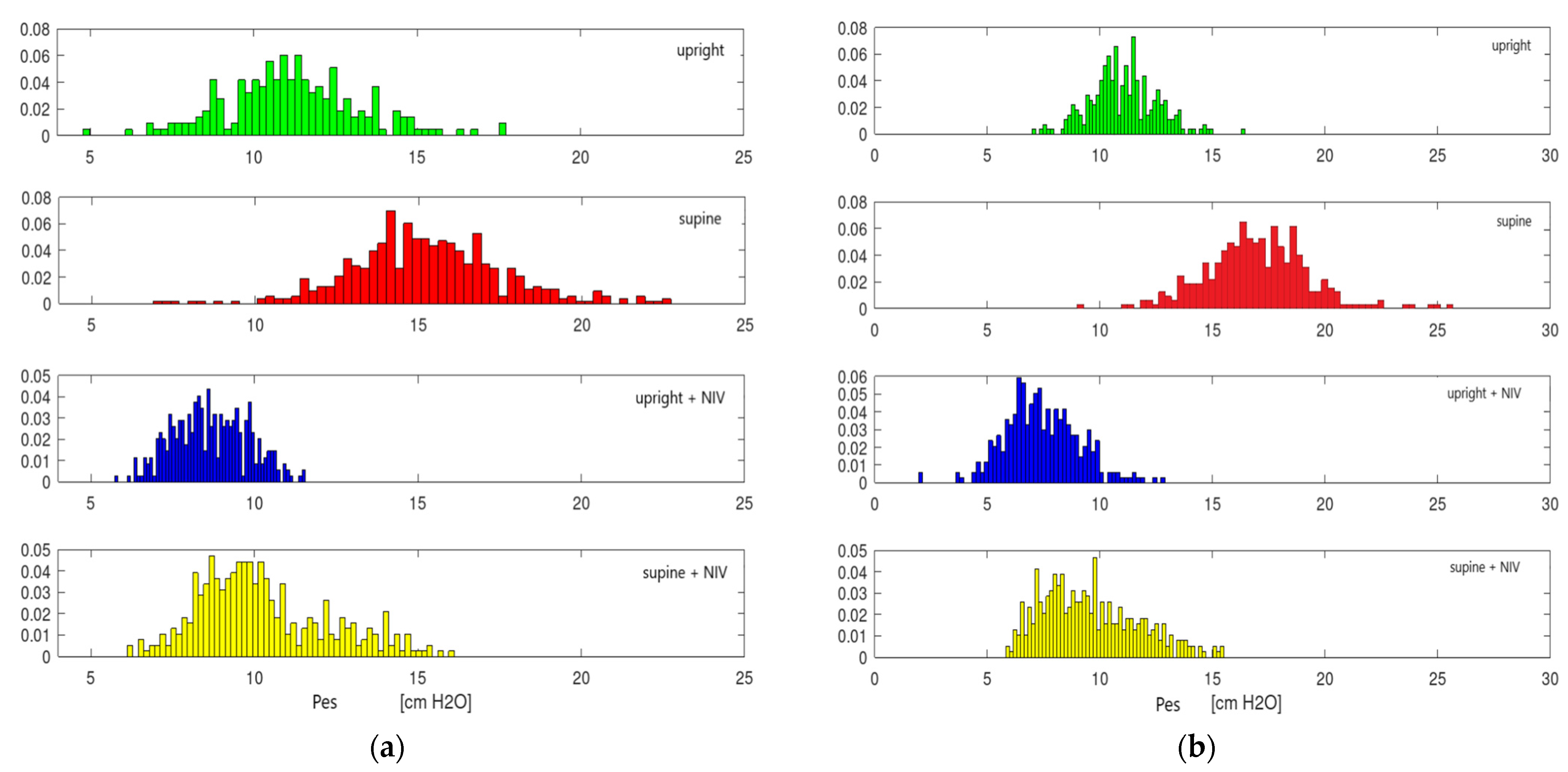
3.2. Measurement Results for ∆Pes
3.3. Influence of Body Position on ∆Pes in the Absence of NIV
3.4. Influence of Ventilatory Support on ∆Pes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akoumianaki, E.; Maggiore, S.M.; Valenza, F.; Bellani, G.; Jubran, A.; Loring, S.H.; Pelosi, P.; Talmor, D.; Grasso, S.; Chiumello, D.; et al. The application of esophageal pressure measurement in patients with respiratory failure. Am. J. Respir. Crit. Care Med. 2014, 189, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Talmor, D.; Sarge, T.; Malhotra, A.; O’Donnell, C.R.; Ritz, R.; Lisbon, A.; Novack, V.; Loring, S.H. Mechanical ventilation guided by esophageal pressure in acute lung injury. N. Engl. J. Med. 2008, 359, 2095–2104. [Google Scholar] [CrossRef] [PubMed]
- Mauri, T.; Yoshida, T.; Bellani, G.; Goligher, E.C.; Carteaux, G.; Rittayamai, N.; Mojoli, F.; Chiumello, D.; Piquilloud, L.; Grasso, S.; et al. Esophageal and transpulmonary pressure in the clinical setting: Meaning, usefulness and perspectives. Intensive Care Med. 2016, 42, 1360–1373. [Google Scholar] [CrossRef]
- Goldberg, P.; Reissmann, H.; Maltais, F.; Ranieri, M.; Gottfried, S.B. Efficacy of noninvasive CPAP in COPD with acute respiratory failure. Eur. Respir. J. 1995, 8, 1894–1900. [Google Scholar] [CrossRef] [PubMed]
- Girault, C.; Richard, J.C.; Chevron, V.; Tamion, F.; Pasquis, P.; Leroy, J.; Bonmarchand, G. Comparative physiologic effects of noninvasive assist-control and pressure support ventilation in acute hypercapnic respiratory failure. Chest 1997, 111, 1639–1648. [Google Scholar] [CrossRef] [PubMed]
- Wysocki, M.; Richard, J.C.; Meshaka, P. Noninvasive proportional assist ventilation compared with noninvasive pressure support ventilation in hypercapnic acute respiratory failure. Crit. Care Med. 2002, 30, 323–329. [Google Scholar] [CrossRef]
- Grieco, D.L.; Menga, L.S.; Cesarano, M.; Rosà, T.; Spadaro, S.; Bitondo, M.M.; Montomoli, J.; Falò, G.; Tonetti, T.; Cutuli, S.L.; et al. Effect of Helmet Noninvasive Ventilation vs High-Flow Nasal Oxygen on Days Free of Respiratory Support in Patients with COVID-19 and Moderate to Severe Hypoxemic Respiratory Failure: The HENIVOT Randomized Clinical Trial. JAMA 2021, 325, 1731–1743. [Google Scholar] [CrossRef]
- Tonelli, R.; Fantini, R.; Tabbì, L.; Castaniere, I.; Pisani, L.; Pellegrino, M.R.; Della Casa, G.; D’Amico, R.; Girardis, M.; Nava, S.; et al. Early Inspiratory Effort Assessment by Esophageal Manometry Predicts Noninvasive Ventilation Outcome in De Novo Respiratory Failure. A Pilot Study. Am. J. Respir. Crit. Care Med. 2020, 202, 558–567. [Google Scholar] [CrossRef]
- Mortamet, G.; Khirani, S.; Amaddeo, A.; Emeriaud, G.; Renolleau, S.; Fauroux, B. Esogastric pressure measurement to assist noninvasive ventilation indication and settings in infants with hypercapnic respiratory failure: A pilot study. Pediatr. Pulmonol. 2017, 52, 1187–1193. [Google Scholar] [CrossRef]
- Yoshida, T.; Brochard, L. Esophageal pressure monitoring: Why, when and how? Curr. Opin. Crit. Care 2018, 24, 216–222. [Google Scholar] [CrossRef]
- Davidson, A.C.; Banham, S.; Elliott, M.; Kennedy, D.; Gelder, C.; Glossop, A.; Church, A.C.; Creagh-Brown, B.; Dodd, J.W.; Felton, T.; et al. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults. Thorax 2016, 71 (Suppl. S2), ii1–ii35. [Google Scholar] [CrossRef] [PubMed]
- Virkkula, P. Diagnosis of Sleep-Related Breathing Disorders: Esophageal Pressure Monitoring, Nasal Resistance and Postural Cephalometry. Ph.D. Thesis, University of Helsinki, Helsinki, Finland, 2003. [Google Scholar]
- Chadda, K.; Annane, D.; Hart, N.; Gajdos, P.; Raphaël, J.C.; Lofaso, F. Cardiac and respiratory effects of continuous positive airway pressure and noninvasive ventilation in acute cardiac pulmonary edema. Crit. Care Med. 2002, 30, 2457–2461. [Google Scholar] [CrossRef] [PubMed]
- Calderini, E.; Confalonieri, M.; Puccio, P.G.; Francavilla, N.; Stella, L.; Gregoretti, C. Patient-ventilator asynchrony during noninvasive ventilation: The role of expiratory trigger. Intensive Care Med. 1999, 25, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Kamerkar, A.; Hotz, J.; Morzov, R.; Newth, C.J.L.; Ross, P.A.; Khemani, R.G. Comparison of Effort of Breathing for Infants on Nasal Modes of Respiratory Support. J. Pediatr. 2017, 185, 26–32.e3. [Google Scholar] [CrossRef]
- Huang, L.; Mendler, M.R.; Waitz, M.; Schmid, M.; Hassan, M.A.; Hummler, H.D. Effects of Synchronisation during Noninvasive Intermittent Mandatory Ventilation in Preterm Infants with Respiratory Distress Syndrome Immediately after Extubation. Neonatology 2015, 108, 108–114. [Google Scholar] [CrossRef]
- Costa, R.; Navalesi, P.; Antonelli, M.; Cavaliere, F.; Craba, A.; Proietti, R.; Conti, G. Physiologic evaluation of different levels of assistance during noninvasive ventilation delivered through a helmet. Chest 2005, 128, 2984–2990. [Google Scholar] [CrossRef][Green Version]
- Mojoli, F.; Iotti, G.A.; Torriglia, F.; Pozzi, M.; Volta, C.A.; Bianzina, S.; Braschi, A.; Brochard, L. In vivo calibration of esophageal pressure in the mechanically ventilated patient makes measurements reliable. Crit. Care 2016, 20, 98. [Google Scholar] [CrossRef]
- Sampath, N.J.; Bhargava, V.; Mittal, R.K. Genesis of multipeaked waves of the esophagus: Repetitive contractions or motion artifact? Am. J. Physiol.-Gastrointest. Liver Physiol. 2010, 298, G927–G933. [Google Scholar] [CrossRef][Green Version]
- Cammarota, G.; Lauro, G.; Santangelo, E.; Sguazzotti, I.; Perucca, R.; Verdina, F.; Boniolo, E.; Tarquini, R.; Bignami, E.; Mongodi, S.; et al. Mechanical Ventilation Guided by Uncalibrated Esophageal Pressure May Be Potentially Harmful. Anesthesiology 2020, 133, 145–153. [Google Scholar] [CrossRef]
- Ozyilmaz, E.; Ugurlu, A.O.; Nava, S. Timing of noninvasive ventilation failure: Causes, risk factors, and potential remedies. BMC Pulm. Med. 2014, 14, 19. [Google Scholar] [CrossRef]
- Knowles, J.H.; Hong, S.K.; Rahn, H. Possible errors using esophageal balloon in determination of pressure-volume characteristics of the lung and thoracic cage. J. Appl. Physiol. 1959, 14, 525–530. [Google Scholar] [CrossRef]
- Hedenstierna, G. Effects of body position on ventilation/perfusion matching. In Anaesthesia, Pain, Intensive Care and Emergency Medicine—APICE; Gullo, A., Ed.; Springer: Milano, Italy, 2005; pp. 3–15. Available online: http://link.springer.com/10.1007/88-470-0351-2_1 (accessed on 11 June 2019).
- Mezidi, M.; Guérin, C. Effects of patient positioning on respiratory mechanics in mechanically ventilated ICU patients. Ann. Transl. Med. 2018, 6, 384. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6212360/ (accessed on 12 June 2019). [CrossRef] [PubMed]
- Kallet, R.H.; Diaz, J.V. The physiologic effects of noninvasive ventilation. Respir. Care 2009, 54, 102–115. [Google Scholar] [PubMed]
- Steriade, A.T.; Johari, S.; Sargarovschi, N.; Necula, D.; Tudose, C.E.; Ionita, D.; Bogdan, M.A.; Bumbacea, D. Predictors of outcome of noninvasive ventilation in severe COPD exacerbation. BMC Pulm. Med. 2019, 19, 131. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.L.; Nzekwu, M.M.U. The effects of body mass index on lung volumes. Chest 2006, 130, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Porta, R.; Vitacca, M.; Clini, E.; Ambrosino, N. Physiological effects of posture on mask ventilation in awake stable chronic hypercapnic COPD patients. Eur. Respir. J. 1999, 14, 517. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Calverley, P.M.A. Respiratory failure in chronic obstructive pulmonary disease. Eur. Respir. J. 2003, 22 (Suppl. S47), 26s–30s. [Google Scholar] [CrossRef] [PubMed]
- Owens, R.L.; Campana, L.M.; Hess, L.; Eckert, D.J.; Loring, S.H.; Malhotra, A. Sitting and supine esophageal pressures in overweight and obese subjects. Obesity 2012, 20, 2354–2360. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | Interval (Min–Max) |
|---|---|---|
| Age | 65.1 | 52–79 |
| BMI | 29.2 | 18–38 |
| mIPAP | 18.2 | 11–27 |
| FEV1 % pred | 28.2 | 19–51 |
| dVNI-72 h (h) | 24.2 | 8–41 |
| Days of NIV | 4.6 | 2–9 |
| LOS | 8 | 4–12 |
| Time | Position ± NIV | ∆Pes | |
|---|---|---|---|
| Mean | Interval | ||
| D1 | Upright | 17.7 | 9.1–28.3 |
| Supine | 23.2 | 15.2–50.8 | |
| Upright + NIV | 12.0 | 5.3–27.2 | |
| Supine + NIV | 13.8 | 6.0–40 | |
| D3 | Upright | 11.7 | 4.0–17.4 |
| Supine | 15.2 | 5.3–24.1 | |
| Upright + NIV | 8.5 | 3.4–15.8 | |
| Supine + NIV | 9.5 | 4.5–22 | |
| DoD | Upright | 13.0 | 6.0–19.5 |
| Supine | 17.3 | 8.1–29.4 | |
| (a) | ||||||||
| Patient’s Position and NIV Support | Mean Difference | Std. Dev. | CI 95% | p * | BMI ** (p) | |||
| Min | Max | |||||||
| D1 | Upright | Supine | −6.30 | 6.11 | −10.41 | −2.20 | <0.01 | 0.07 |
| Upright | Upright NIV | 5.18 | 4.12 | 2.69 | 7.67 | <0.01 | ||
| Supine | Supine NIV | 8.84 | 3.61 | 6.55 | 11.14 | <0.01 | ||
| Upright NIV | Supine NIV | −0.94 | 2.39 | −2.47 | 0.57 | ns | ||
| D3 | Upright | Supine | −3.71 | 3.44 | −6.02 | −1.39 | <0.01 | |
| Upright | Upright NIV | 3.82 | 5.09 | 0.18 | 7.46 | 0.04 | ||
| Supine | Supine NIV | 6.75 | 7.22 | 2.16 | 11.33 | 0.01 | ||
| Upright NIV | Supine NIV | −0.92 | 2.97 | −2.81 | 0.96 | ns | ||
| DoD | Upright | Supine | −3.44 | 3.07 | −6.29 | −0.60 | 0.02 | |
| (b) | ||||||||
| Patient’s Position | Mean Difference | Std. Dev. | CI 95% | p * | BMI **(p) | |||
| Min | Max | |||||||
| D1–D3 | D1 upright | D3 upright | 4.38 | 7.19 | −0.45 | 9.21 | 0.07 | |
| D1 supine | D3 supine | 7.13 | 12.30 | −2.33 | 16.58 | ns | ||
| D1–DoD | D1 upright | DoD upright | 3.47 | 5.09 | −0.45 | 7.38 | 0.02 | <0.01 |
| D1 supine | DoD supine | 2.51 | 5.31 | −2.40 | 7.42 | ns | ||
| D3–DoD | D3 upright | DoD upright | 0.11 | 0.91 | −0.73 | 0.95 | ns | |
| D3 supine | DoD supine | −1.31 | 4.93 | −6.49 | 3.86 | ns | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steriade, A.T.; Gologanu, M.; Bumbacea, R.S.; Bogdan, S.N.; Bumbacea, D. Esophageal Pressure Measurement in Acute Hypercapnic Respiratory Failure Due to Severe COPD Exacerbation Requiring NIV—A Pilot Safety Study. J. Clin. Med. 2022, 11, 6810. https://doi.org/10.3390/jcm11226810
Steriade AT, Gologanu M, Bumbacea RS, Bogdan SN, Bumbacea D. Esophageal Pressure Measurement in Acute Hypercapnic Respiratory Failure Due to Severe COPD Exacerbation Requiring NIV—A Pilot Safety Study. Journal of Clinical Medicine. 2022; 11(22):6810. https://doi.org/10.3390/jcm11226810
Chicago/Turabian StyleSteriade, Alexandru Tudor, Mihai Gologanu, Roxana Silvia Bumbacea, Stefan Nicolae Bogdan, and Dragos Bumbacea. 2022. "Esophageal Pressure Measurement in Acute Hypercapnic Respiratory Failure Due to Severe COPD Exacerbation Requiring NIV—A Pilot Safety Study" Journal of Clinical Medicine 11, no. 22: 6810. https://doi.org/10.3390/jcm11226810
APA StyleSteriade, A. T., Gologanu, M., Bumbacea, R. S., Bogdan, S. N., & Bumbacea, D. (2022). Esophageal Pressure Measurement in Acute Hypercapnic Respiratory Failure Due to Severe COPD Exacerbation Requiring NIV—A Pilot Safety Study. Journal of Clinical Medicine, 11(22), 6810. https://doi.org/10.3390/jcm11226810