
Concomitant Endoscopic Surgery for Bladder Tumors and Prostatic Obstruction: Are We Safely Hitting Two Birds with One Stone? A Systematic Review and Meta-Analysis

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Grading of Evidence, Data Synthesis, and Statistical Analysis
3. Results
3.1. Study Results and Quality Assessment
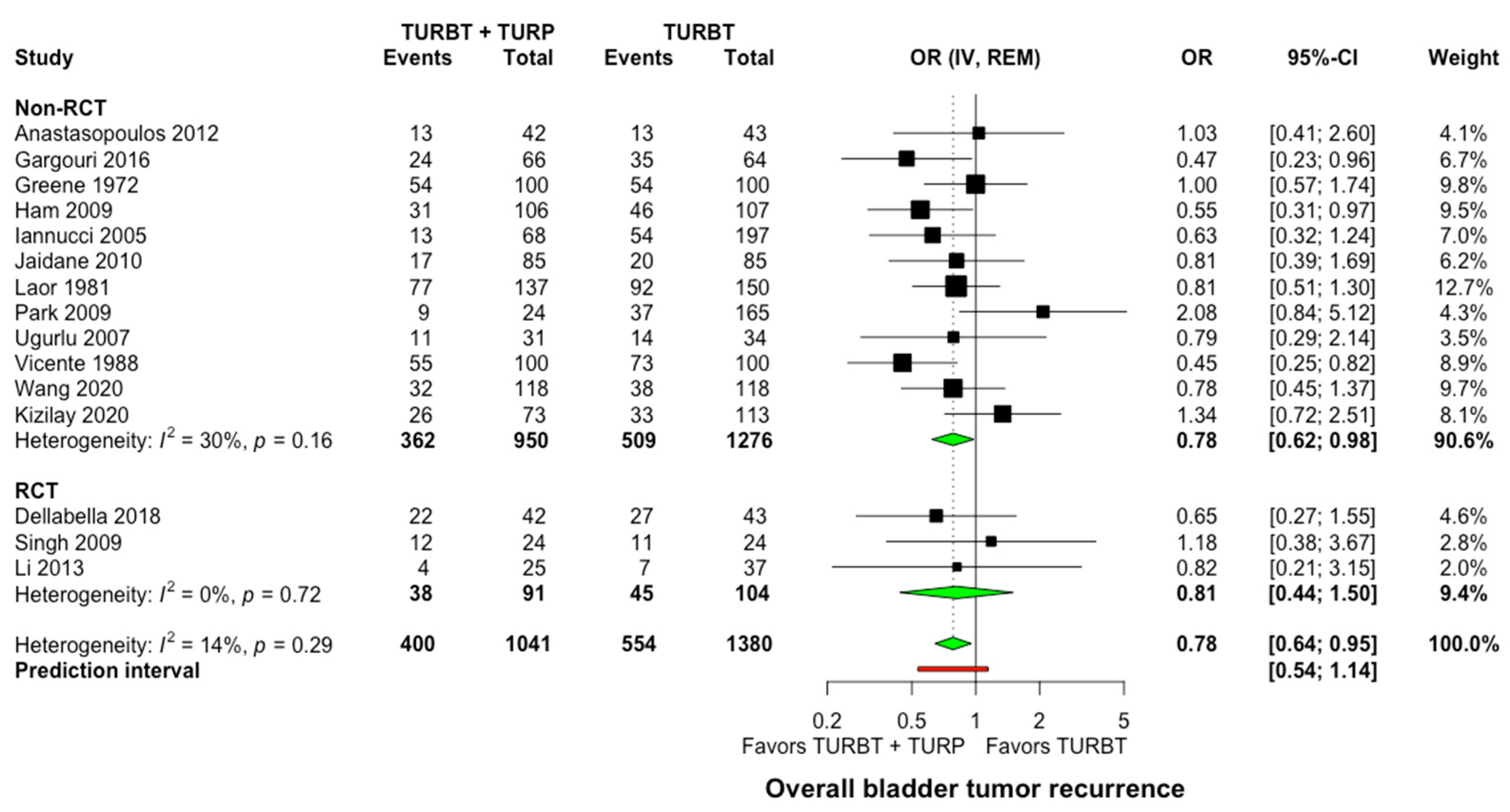
3.2. Bladder Tumor Recurrence
3.3. Bladder Tumor Recurrences Depending on Tumor Grade and Number of Tumors
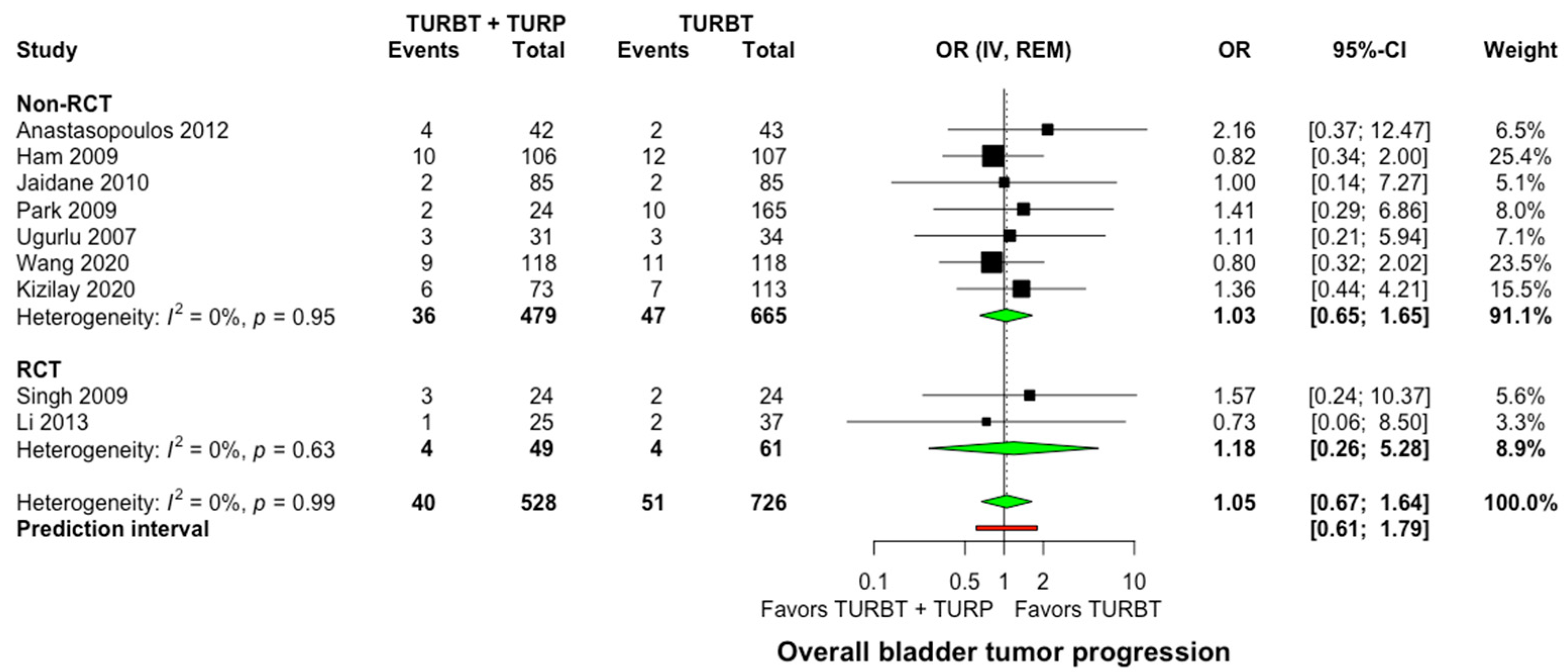
3.4. Bladder Tumor Progression
3.5. Lower Urinary Tract Symptoms
3.6. Quality of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Egan, K.B. The Epidemiology of Benign Prostatic Hyperplasia Associated with Lower Urinary Tract Symptoms: Prevalence and Incident Rates. Urol. Clin. N. Am. 2016, 43, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gonteroe, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef]
- Sylvester, R.J.; van der Meijden, A.P.M.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.W.; Kurthet, K. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: A combined analysis of 2596 patients from seven EORTC trials. Eur. Urol. 2006, 49, 466–467. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, K.; Utsunomiya, N.; Ichioka, K.; Matsui, Y.; Terai, A.; Arai, Y. Impact of superficial bladder cancer and transurethral resection on general health-related quality of life: An SF-36 survey. Urology 2005, 65, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Naslund, M.J.; Gilsenan, A.W.; Midkiff, K.D.; Bown, A.; Wolford, E.T.; Wang, J. Prevalence of lower urinary tract symptoms and prostate enlargement in the primary care setting. Int. J. Clin. Pract. 2007, 61, 1437–1445. [Google Scholar] [CrossRef]
- Speakman, M.; Kirby, R.; Doyle, S.; Ioannou, C. Burden of male lower urinary tract symptoms (LUTS) suggestive of benign prostatic hyperplasia (BPH)—Focus on the UK. BJU Int. 2015, 115, 508–519. [Google Scholar] [CrossRef] [PubMed]
- Braeckman, J.; Denis, L. Management of BPH then 2000 and now 2016—From BPH to BPO. Asian J. Urol. 2017, 4, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Tsivian, A.; Shtricker, A.; Sidi, A.A. Simultaneous transurethral resection of bladder tumor and benign prostatic hyperplasia: Hazardous or a safe timesaver? J. Urol. 2003, 170, 2241–2243. [Google Scholar] [CrossRef]
- Albarran, J.; Imbert, L. Les Tumeurs Du Rein; Masson: Paris, France, 1903. [Google Scholar]
- Hinman, F.J. Recurrence of bladder tumors by surgical implantation. J. Urol. 1956, 75, 695–696. [Google Scholar] [CrossRef]
- Kiefer, J.H. Bladder tumor recurrence in the urethra: A warning. J. Urol. 1953, 69, 652–656. [Google Scholar] [CrossRef]
- Zhou, L.; Liang, X.; Zhang, K. Assessment of the clinical efficacy of simultaneous transurethral resection of both bladder cancer and the prostate: A systematic review and meta-analysis. Aging Male 2020, 23, 1182–1193. [Google Scholar] [CrossRef] [PubMed]
- Sari Motlagh, R.; Mori, K.; Miura, N.; Quhal, F.; Aydh, A.; Laukhtina, E.; Pradere, B.; Karakiewicz, P.I.; Enikeev, D.V.; Deuker, M.; et al. The recurrence and progression risk after simultaneous endoscopic surgery of urothelial bladder tumour and benign prostatic hyperplasia: A systematic review and meta-analysis. BJU Int. 2021, 127, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.; Corbett, M.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Schünemann, H.J.; Brozek, J.; Glasziou, P.; Alonso Coello, P.; Atkins, D.; Kunz, R.; Monteri., V.; Jaescke, R.; et al. GRADE guidelines: 11. Making an overall rating of confidence in effect estimates for a single outcome and for all outcomes. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef]
- Anastasopoulos, P.; Stavropoulos, M.; Bouropoulos, C.; Ferakis, N.; Poulias, I. C26 Long Term Effects of Simultaneous Transurethral Resection of Non-Muscle-Invasive Bladder Tumors and Benign Prostatic Hyperplasia: Analysis of Our Experience. Eur. Urol. Suppl. 2012, 11, 88. [Google Scholar] [CrossRef]
- Dellabella, M.; Branchi, A.; Gasparri, L.; Claudini, R.; Castellani, D. Oncological safety and quality of life in men undergoing simultaneous transurethral resection of bladder tumor and prostate: Results from a randomized controlled trial. World J. Urol. 2018, 36, 1629–1634. [Google Scholar] [CrossRef]
- Gargouri, M.; Jallouli, W.; Ben, C.M.A.; Sellami, A.; Bibi, M.; Ben Rhouma, S.; Nouira, Y. P118—Oncologic results of simultaneous bladder tumor and prostate resection. Eur. Urol. Suppl. 2016, 15, e1709. [Google Scholar] [CrossRef]
- Greene, L.F.; Yalowitz, P.A. The advisability of concomitant transurethral excision of vesical neoplasm and prostatic hyperplasia. J. Urol. 1972, 107, 445–447. [Google Scholar] [CrossRef]
- Ham, W.S.; Kim, W.T.; Jeon, H.J.; Lee, D.; Choi, Y.D. Long-term outcome of simultaneous transurethral resection of bladder tumor and prostate in patients with nonmuscle invasive bladder tumor and bladder outlet obstruction. J. Urol. 2009, 181, 1594–1599. [Google Scholar] [CrossRef] [PubMed]
- Iannucci, M.; Nicolai, M.; Tenaglia, R.L. Resezione simultanea transuretrale di neoplasia vescicale e IPB. Urologia 2005, 72, 115–117. [Google Scholar] [CrossRef]
- Jaidane, M.; Bouicha, T.; Slama, A.; Hmida, W.; Hidoussi, A.; Sorba, N.B.; Mosbah, F. Tumor recurrence in prostatic urethra following simultaneous resection of bladder tumor and prostate: A comparative retrospective study. Urology 2010, 75, 1392–1395. [Google Scholar] [CrossRef] [PubMed]
- Kizilay, F.; Sahin, M.; Turna, B.; Altay, B.; Nazli, O.; Semerci, B. Simultaneous resection of a bladder tumor and prostate is oncologically and functionally safe. Kuwait Med. J. 2020, 52, 268–273. [Google Scholar]
- Li, Z.; Hou, R.; Li, J. The efficacy and safety of simultaneous transurethral GreenLight photoselective vaporization of bladder tumor and prostate in patients with bladder tumor and lower urinary tract symptoms. Int. Urol. Nephrol. 2014, 46, 691–694. [Google Scholar] [CrossRef]
- Laor, E.; Grabstald, H.; Whitmore, W.F. The influence of simultaneous resection of bladder tumors and prostate on the occurrence of prostatic urethral tumors. J. Urol. 1981, 126, 171–175. [Google Scholar] [CrossRef]
- Kim, S.; Park, S.; Kim, S. MP-20.11: Oncologic Results of Simultaneous Transurethral Resection of Superficial Bladder Cancer and Benign Prostatic Hyperplasia. Urology 2009, 74 (Suppl. 4), S144. [Google Scholar] [CrossRef]
- Singh, V.; Sinha, R.J.; Sankhwar, S.N. Outcome of simultaneous transurethral resection of bladder tumor and transurethral resection of the prostate in comparison with the procedures in two separate sittings in patients with bladder tumor and urodynamically proven bladder outflow obstruction. J. Endourol. 2009, 23, 2007–2011. [Google Scholar] [CrossRef]
- Ugurlu, O.; Gonulalan, U.; Adsan, O.; Kosan, M.; Oztekin, V.; Centikaya, M. Effects of simultaneous transurethral resection of prostate and solitary bladder tumors smaller than 3 cm on oncologic results. Urology 2007, 70, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Vicente, J.; Chéchile, G.; Pons, R.; Mendez, G. Tumor recurrence in prostatic urethra following simultaneous resection of bladder tumor and prostate. Eur. Urol. 1988, 15, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Z.; Shao, J.; Lu, Y.; Li, X.; Li, R. Outcome of simultaneous thulium laser enucleation of bladder tumor and prostate in patients with non-muscle invasive bladder tumor and benign prostatic hyperplasia: A matched-pair comparison with a long-term follow-up. World J. Urol. 2021, 39, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Golomb, J.; Gorelik, U.; Keler, T.; Lindner, A. Incidence and pattern of bladder tumor recurrence following combined suprapubic prostatectomy and excision of a bladder tumor. Eur. Urol. 1989, 16, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Sountoulides, P.; Pyrgidis, N.; Brookman-May, S.; Mykoniatis, I.; Karasavvides, T.; Hatzichristou, D. Does Ureteral Stenting Increase the Risk of Metachronous Upper Tract Urothelial Carcinoma in Patients with Bladder Tumors? A Systematic Review and Meta-analysis. J. Urol. 2021, 205, 956–966. [Google Scholar] [CrossRef]
- Silverman, D.T.; Alguacil, J.; Rothman, N.; Real, F.X.; Garcia Closas, M.; Cantor, K.P.; Malats, N.; Tardon, A.; Serra, C.; Garcia Clossas, R.; et al. Does increased urination frequency protect against bladder cancer? Int. J. Cancer 2008, 123, 1644–1648. [Google Scholar] [CrossRef]
- Picozzi, S.C.M.; Ricci, C.; Gaeta, M.; Casellato, S.; Bozzini, G.; Ratti, D.; Carmignani, L. Is it oncologically safe performing simultaneous transurethral resection of the bladder and prostate? A meta-analysis on 1234 patients. Int. Urol. Nephrol. 2012, 44, 1325–1333. [Google Scholar] [CrossRef]
- Kouriefs, C.; Loizides, S.; Mufti, G. Simultaneous Transurethral Resection of Bladder Tumour and Prostate: Is It Safe? Urol. Int. 2008, 81, 125–128. [Google Scholar] [CrossRef]
- Perlis, N.; Zlotta, A.R.; Beyene, J.; Finelli, A.; Fleschner, N.E.; Kulkarni, G.S. Immediate post-transurethral resection of bladder tumor intravesical chemotherapy prevents non-muscle-invasive bladder cancer recurrences: An updated meta-analysis on 2548 patients and quality-of-evidence review. Eur. Urol. 2013, 64, 421–430. [Google Scholar] [CrossRef]
- Sountoulides, P.; Mutomba, W.F.; Bouras, E.; Lim, J.; Bourdoumis, A.; Jain, A. How well do we manage non-muscle invasive bladder tumors? A UK audit of real-life practices. Urol. J. 2020, 87, 142–148. [Google Scholar] [CrossRef]
- Redelma-Sidi, G.; Glickman, M.S.; Bochner, B.H. The mechanism of action of BCG therapy for bladder cancer—A current perspective. Nat. Rev. Urol. 2014, 11, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Laukhtina, E.; Moschini, M.; Krajewski, W.; Teoh, J.Y.; Ploussard, G.; Soria, F.; Roghmann, F.; Muenker, M.A.; Roumiguie, M.; Alvarez-Maestro, M.; et al. Oncological and safety profiles in patients undergoing simultaneous transurethral resection (TUR) of bladder tumour and TUR of the prostate. BJU Int. 2022, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Cox, E.; Saramago, P.; Kelly, J.; Porta, N.; Hall, E.; Tan, W.S.; Sculpher, M.; Soares, M. Effects of Bladder Cancer on UK Healthcare Costs and Patient Health-Related Quality of Life: Evidence from the BOXIT Trial. Clin. Genitourin. Cancer 2020, 18, e418–e442. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.; Nielsen, M.E.; Crandell, J.L.; Palmer, M.H.; Smith, S.K.; Bryant, A.L.; Mayer, D.K. Health-related quality of life among non-muscle-invasive bladder cancer survivors: A population-based study. BJU Int. 2020, 125, 38–48. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year of Publication, Study Design | Sample Size (SG/CG) | Mean Age (Years) (SG/CG) | Prostatic Procedure | BC Stage (SG/CG) | Tumor Grade (SG/CG) | Unifocal Tumor (SG/CG) | Multifocal Tumor (SG/CG) | Mean Follow-Up (Months) (SG/CG) | Adjuvant Therapy (SG/CG) | LUTS Assessment |
|---|---|---|---|---|---|---|---|---|---|---|
| Anastasopoulos, 2012 [20] Non-RCT | 85 (42/43) | 69/69 | Transurethral resection | NA | NA | ΝA | ΝA | 31/27 | ΝA | NA |
| Dellabella, 2018 [21] RCT | 85 (42/43) | 64/63 | Transurethral resection | pTa/pTis: 29/26 pT1: 13/17 | Low: 16/14 High: 26/29 | 21/24 | 21/19 | 37/35 | BCG: 27/26 | IPSS, Qmax, PVR, FACT-BIQ |
| Gargouri, 2016 [22] Non-RCT | 130 (66/64) | 72/64 | Transurethral resection | NA | NA | 38/26 | 28/38 | 41/42 | BCG: 26/40 | NA |
| Greene, 1972 [23] Non-RCT | 200 (100/100) | NA | Transurethral resection | NA | G1: 57/59 G2: 29/23 G3: 14/18 | 81/77 | 19/23 | NA | NA | ΝA |
| Ham, 2009 [24] Non-RCT | 213 (106/107) | 68/66 | Transurethral resection | pTa: 21/19 pT1: 85/88 | Low: 60/59 High: 46/48 | 58/56 | 48/51 | 50/54 | BCG: 49/54 | Qmax, PVR |
| Iannucci, 2005 [25] Non-RCT | 265 (68/197) | NA | Transurethral resection | NA | ΝA | ΝA | ΝA | NA | NA | ΝA |
| Jaidane, 2010 [26] Non-RCT | 170 (85/85) | 71/71 | Transurethral resection | pTa: 9/11 pT1: 76/74 | G1: 32/33 G2: 45/44 G3: 8/8 | 70/65 | 15/20 | 35/33 | BCG: 69/70 | NA |
| Kizilay, 2020 [27] Non-RCT | 186 (73/113) | 62/48 | Transurethral resection | pTa: 49/68 pT1: 24/36 pT2: 0/9 | Low: 51/70 High: 22/43 | 62/89 | 11/24 | NA | ΝA | NA |
| Li, 2013 [28] RCT | 62 (25/37) | 48/66 | Photoselective vaporization | pTa: 3/6 pT1: 17/22 pT2: 5/9 | Low: 20/28 High: 5/9 | 19/25 | 6/12 | NA | BCG: NA, SIIC: all patients | NA |
| Laor, 1981 [29] Non-RCT | 287 (137/150) | 71/60 | Transurethral resection | NA | G1: 51/58 G2: 35/35 G3: 51/57 | 112/124 | 25/26 | 69/96 | NA | ΝA |
| Li, 2013 [28] RCT | 62 (25/37) | 48/66 | Photoselective vaporization | pTa: 3/6 pT1: 17/22 pT2: 5/9 | Low: 20/28 High: 5/9 | 19/25 | 6/12 | NA | BCG: NA, SIIC: all patients | NA |
| Park, 2009 [30] Non-RCT | 189 (24/165) | 70/64 | Transurethral resection | pTa/pTis: 8/56 pT1: 16/109 | Low: 13/81 High: 11/84 | NA | NA | 52/44 | BCG: 22/157 | NA |
| Singh, 2009 [31] RCT | 48 (24/24) | 56/57 | Transurethral resection | pTa: 17/18 pT1: 7/6 | G1: 10/9 G2:11/11 G3: 3/4 | 24/24 | 0/0 | 36/38 | NA | IPSS |
| Ugurlu, 2007 [32] Non-RCT | 65 (31/34) | 68/56 | Transurethral resection | pTa: 25/25 pT1: 6/9 | G1: 26/31 G2: 3/3 G3: 2/0 | 31/34 | 0/0 | 31/27 | NA | ΝA |
| Vicente, 1988 [33] Non-RCT | 200 (100/100) | 69/60 | Transurethral resection | pTa: 21/24 pT1: 79/76 | G1: 4/18 G2: 78/73 G3: 18/9 | 58/52 | 42/48 | 47/46 | None | ΝA |
| Wang, 2020 [34] Non-RCT | 236 (118/118) | 67/65 | Thulium laser enucleation | pTa: 14/21 pT1: 114/97 | Low: 71/79 High: 47/39 | 75/82 | 43/36 | 59/56 | BCG: based on risk, SIIC: 89/93 | Qmax, PVR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savvides, E.; Pyrgidis, N.; Langas, G.; Symeonidis, E.N.; Dimitriadis, G.; Sountoulides, P. Concomitant Endoscopic Surgery for Bladder Tumors and Prostatic Obstruction: Are We Safely Hitting Two Birds with One Stone? A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 6208. https://doi.org/10.3390/jcm11206208
Savvides E, Pyrgidis N, Langas G, Symeonidis EN, Dimitriadis G, Sountoulides P. Concomitant Endoscopic Surgery for Bladder Tumors and Prostatic Obstruction: Are We Safely Hitting Two Birds with One Stone? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(20):6208. https://doi.org/10.3390/jcm11206208
Chicago/Turabian StyleSavvides, Eliophotos, Nikolaos Pyrgidis, Georgios Langas, Evangelos N. Symeonidis, Georgios Dimitriadis, and Petros Sountoulides. 2022. "Concomitant Endoscopic Surgery for Bladder Tumors and Prostatic Obstruction: Are We Safely Hitting Two Birds with One Stone? A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 20: 6208. https://doi.org/10.3390/jcm11206208
APA StyleSavvides, E., Pyrgidis, N., Langas, G., Symeonidis, E. N., Dimitriadis, G., & Sountoulides, P. (2022). Concomitant Endoscopic Surgery for Bladder Tumors and Prostatic Obstruction: Are We Safely Hitting Two Birds with One Stone? A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(20), 6208. https://doi.org/10.3390/jcm11206208