
Infection of (Peri-)Pancreatic Necrosis Is Associated with Increased Rates of Adverse Events during Endoscopic Drainage: A Retrospective Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants and Phenotype Data
2.2. Endoscopic Drainage of Pancreatic Necrosis
2.3. Data Analysis
3. Results
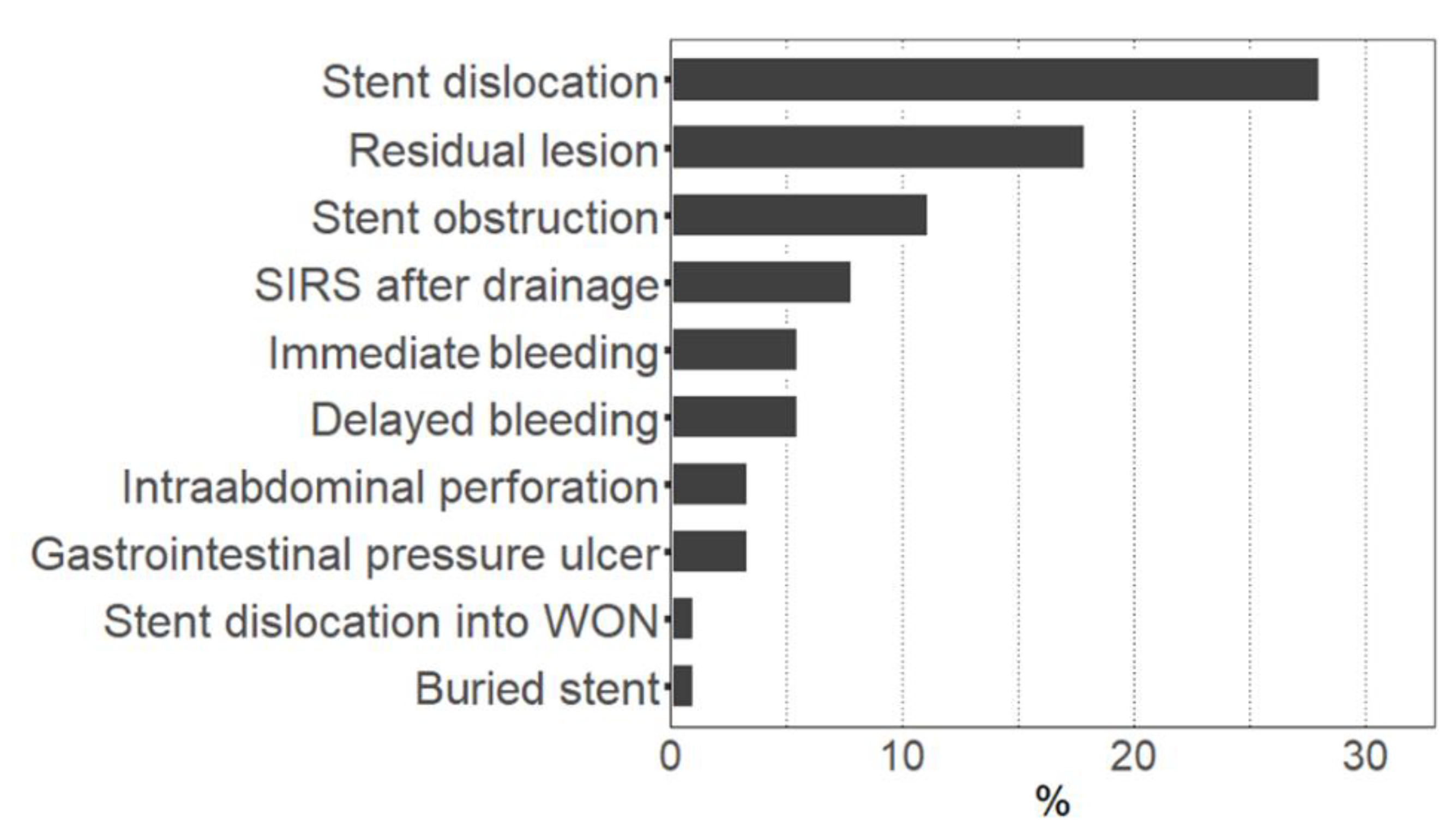
3.1. Rates and Types of Complications during Drainage Therapy
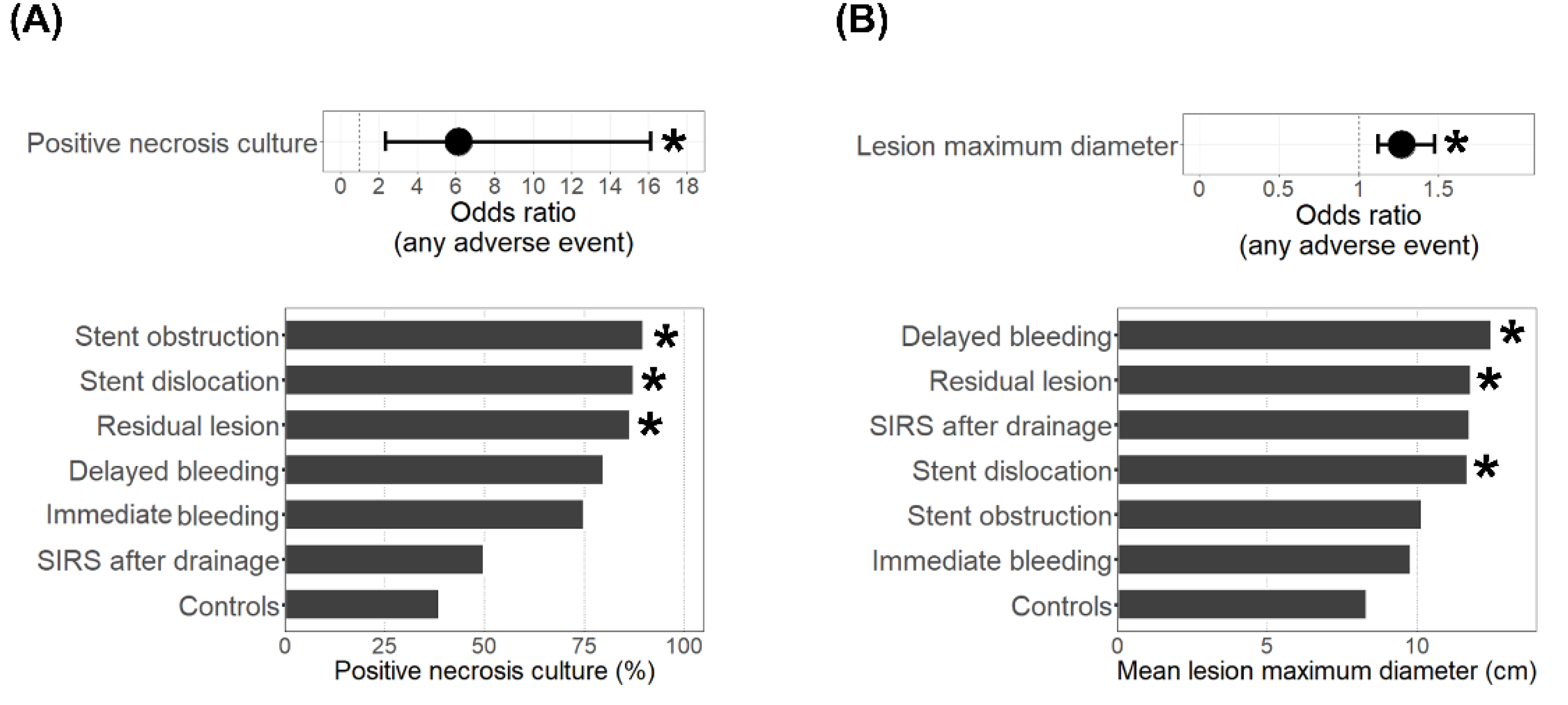
3.2. Treatment Characteristics of Adverse Events Cases and Controls
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peery, A.F.; Crockett, S.D.; Murphy, C.C.; Lund, J.L.; Dellon, E.S.; Williams, J.L.; Jensen, E.T.; Shaheen, N.J.; Barritt, A.S.; Lieber, S.R.; et al. Burden and Cost of Gastrointestinal, Liver, and Pancreatic Diseases in the United States: Update 2018. Gastroenterology 2019, 156, 254–272.e11. [Google Scholar] [CrossRef] [PubMed]
- Weiss, F.U.; Laemmerhirt, F.; Lerch, M.M. Etiology and Risk Factors of Acute and Chronic Pancreatitis. Visc. Med. 2019, 35, 73–81. [Google Scholar] [CrossRef] [PubMed]
- van Santvoort, H.C.; Bakker, O.J.; Bollen, T.L.; Besselink, M.G.; Ali, U.A.; Schrijver, A.M.; Boermeester, M.A.; van Goor, H.; Dejong, C.H.; van Eijck, C.H.; et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology 2011, 141, 1254–1263. [Google Scholar] [CrossRef] [PubMed]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S.; Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis--2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef]
- Aghdassi, A.; Simon, P.; Pickartz, T.; Budde, C.; Skube, M.E.; Lerch, M.M. Endoscopic management of complications of acute pancreatitis: An update on the field. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 1207–1218. [Google Scholar] [CrossRef]
- Van Brunschot, S.; Hollemans, R.A.; Bakker, O.J.; Besselink, M.G.; Baron, T.H.; Beger, H.G.; Boermeester, M.A.; Bollen, T.L.; Bruno, M.J.; Carter, R.; et al. Minimally invasive and endoscopic versus open necrosectomy for necrotising pancreatitis: A pooled analysis of individual data for 1980 patients. Gut 2018, 67, 697–706. [Google Scholar] [CrossRef]
- van Brunschot, S.; van Grinsven, J.; van Santvoort, H.C.; Bakker, O.J.; Besselink, M.G.; A Boermeester, M.; Bollen, T.L.; Bosscha, K.; A Bouwense, S.; Bruno, M.J.; et al. Endoscopic or surgical step-up approach for infected necrotising pancreatitis: A multicentre randomised trial. Lancet 2018, 391, 51–58. [Google Scholar] [CrossRef]
- Bang, J.Y.; Arnoletti, J.P.; Holt, B.A.; Sutton, B.; Hasan, M.K.; Navaneethan, U.; Feranec, N.; Wilcox, C.M.; Tharian, B.; Hawes, R.H.; et al. An Endoscopic Transluminal Approach, Compared With Minimally Invasive Surgery, Reduces Complications and Costs for Patients With Necrotizing Pancreatitis. Gastroenterology 2019, 156, 1027–1040.e3. [Google Scholar] [CrossRef]
- Garg, P.K.; Meena, D.; Babu, D.; Padhan, R.K.; Dhingra, R.; Krishna, A.; Kumar, S.; Misra, M.C.; Bansal, V.K. Endoscopic versus laparoscopic drainage of pseudocyst and walled-off necrosis following acute pancreatitis: A randomized trial. Surg. Endosc. 2020, 34, 1157–1166. [Google Scholar] [CrossRef]
- Angadi, S.; Mahapatra, S.J.; Sethia, R.; Elhence, A.; Krishna, A.; Gunjan, D.; Prajapati, O.P.; Kumar, S.; Bansal, V.K.; Garg, P.K. Endoscopic transmural drainage tailored to quantity of necrotic debris versus laparoscopic transmural internal drainage for walled-off necrosis in acute pancreatitis: A randomized controlled trial. Pancreatology 2021, 21, 1291–1298. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.H.; Sibbald, W.J. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017; Available online: https://www.R-project.org/ (accessed on 14 August 2022).
- Frost, F.; Kacprowski, T.; Rühlemann, M.; Bülow, R.; Kühn, J.-P.; Franke, A.; Heinsen, F.-A.; Pietzner, M.; Nauck, M.; Völker, U.; et al. Impaired Exocrine Pancreatic Function Associates With Changes in Intestinal Microbiota Composition and Diversity. Gastroenterology 2019, 156, 1010–1015. [Google Scholar] [CrossRef] [PubMed]
- Pietzner, M.; Budde, K.; Rühlemann, M.; Völzke, H.; Homuth, G.; Weiss, F.U.; Lerch, M.M.; Frost, F. Exocrine Pancreatic Function Modulates Plasma Metabolites Through Changes in Gut Microbiota Composition. J. Clin. Endocrinol. Metab. 2021, 106, e2290–e2298. [Google Scholar] [CrossRef]
- Frost, F.; Weiss, F.U.; Sendler, M.; Kacprowski, T.; Rühlemann, M.; Bang, C.; Franke, A.; Völker, U.; Völzke, H.; Lamprecht, G.; et al. The Gut Microbiome in Patients With Chronic Pancreatitis Is Characterized by Significant Dysbiosis and Overgrowth by Opportunistic Pathogens. Clin. Transl. Gastroenterol. 2020, 11, e00232. [Google Scholar] [CrossRef]
- Zhu, Y.; He, C.; Li, X.; Cai, Y.; Hu, J.; Liao, Y.; Zhao, J.; Xia, L.; He, W.; Liu, L.; et al. Gut microbiota dysbiosis worsens the severity of acute pancreatitis in patients and mice. J. Gastroenterol. 2019, 54, 347–358. [Google Scholar] [CrossRef]
- Sendler, M.; Wilden, A.; Glaubitz, J.; Frost, F.; Weiss, F.; Lerch, M. Immunosuppression during severe acute pancreatitis is associated with a dramatic shift in intestinal microbiota composition and infected necrosis. Pancreatology 2020, 20, S24. [Google Scholar] [CrossRef]
- Cacopardo, B.; Pinzone, M.; Berretta, S.; Fisichella, R.; Di Vita, M.; Zanghì, G.; Cappellani, A.; Nunnari, G.; Zanghì, A. Localized and systemic bacterial infections in necrotizing pancreatitis submitted to surgical necrosectomy or percutaneous drainage of necrotic secretions. BMC Surg. 2013, 13 (Suppl. 2), S50. [Google Scholar] [CrossRef]
- Mowbray, N.G.; Ben-Ismaeil, B.; Hammoda, M.; Shingler, G.; Al-Sarireh, B. The microbiology of infected pancreatic necrosis. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 456–460. [Google Scholar] [CrossRef]
- Vaishnavi, C.; Samanta, J.; Kochhar, R. Characterization of biofilms in biliary stents and potential factors involved in occlusion. World J. Gastroenterol. 2018, 24, 112–123. [Google Scholar] [CrossRef]
- Li, X.; He, C.; Li, N.; Ding, L.; Chen, H.; Wan, J.; Yang, X.; Xia, L.; He, W.; Xiong, H.; et al. The interplay between the gut microbiota and NLRP3 activation affects the severity of acute pancreatitis in mice. Gut Microbes 2020, 11, 1774–1789. [Google Scholar] [CrossRef] [PubMed]
- Ruhal, R.; Kataria, R. Biofilm patterns in gram-positive and gram-negative bacteria. Microbiol. Res. 2021, 251, 126829. [Google Scholar] [CrossRef] [PubMed]
- Brest, P.; Turchi, L.; Le’Negrate, G.; Berto, F.; Moreilhon, C.; Mari, B.; Ponzio, G.; Hofman, P. Escherichia coli cytotoxic necrotizing factor 1 inhibits intestinal epithelial wound healing in vitro after mechanical injury. Infect. Immun. 2004, 72, 5733–5740. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Konturek, C.; Brzozowski, T.; Konturek, S.J.; Kwiecien, S.; Dembinski, A.; Hahn, E.G. Influence of bacterial lipopolysaccharide on healing of chronic experimental ulcer in rat. Scand. J. Gastroenterol. 2001, 36, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- Brothers, K.M.; Stella, N.A.; Hunt, K.M.; Romanowski, E.G.; Liu, X.; Klarlund, J.K.; Shanks, R.M.Q. Putting on the brakes: Bacterial impediment of wound healing. Sci. Rep. 2015, 5, 14003. [Google Scholar] [CrossRef] [PubMed]
- Chong, K.K.L.; Tay, W.H.; Janela, B.; Yong, A.M.H.; Liew, T.H.; Madden, L.; Keogh, D.; Barkham, T.M.S.; Ginhoux, F.; Becker, D.L.; et al. Enterococcus faecalis Modulates Immune Activation and Slows Healing During Wound Infection. J. Infect. Dis. 2017, 216, 1644–1654. [Google Scholar] [CrossRef]
- Piciucchi, M.; Capurso, G.; Archibugi, L.; Fave, M.M.D.; Capasso, M.; Fave, G.D. Exocrine Pancreatic Insufficiency in Diabetic Patients: Prevalence, Mechanisms, and Treatment. Int. J. Endocrinol. 2015, 2015, 595649. [Google Scholar] [CrossRef]
- Yang, J.; Chen, Y.-I.; Friedland, S.; Holmes, I.; Paiji, C.; Law, R.; Hosmer, A.; Stevens, T.; Matheus, F.; Pawa, R.; et al. Lumen-apposing stents versus plastic stents in the management of pancreatic pseudocysts: A large, comparative, international, multicenter study. Endoscopy 2019, 51, 1035–1043. [Google Scholar] [CrossRef]
- Lang, G.D.; Fritz, C.; Bhat, T.; Das, K.K.; Murad, F.M.; Early, D.S.; Edmundowicz, S.A.; Kushnir, V.M.; Mullady, D.K. EUS-guided drainage of peripancreatic fluid collections with lumen-apposing metal stents and plastic double-pigtail stents: Comparison of efficacy and adverse event rates. Gastrointest. Endosc. 2018, 87, 150–157. [Google Scholar] [CrossRef]
- Bang, J.Y.; Navaneethan, U.; Hasan, M.K.; Sutton, B.; Hawes, R.; Varadarajulu, S. Non-superiority of lumen-apposing metal stents over plastic stents for drainage of walled-off necrosis in a randomised trial. Gut 2019, 68, 1200–1209. [Google Scholar] [CrossRef]
- Chandrasekhara, V.; Barthet, M.; Devière, J.; Bazerbachi, F.; Lakhtakia, S.; Easler, J.J.; Peetermans, J.A.; McMullen, E.; Gjata, O.; Gourlay, M.L.; et al. Safety and efficacy of lumen-apposing metal stents versus plastic stents to treat walled-off pancreatic necrosis: Systematic review and meta-analysis. Endosc. Int. Open 2020, 8, E1639–E1653. [Google Scholar] [CrossRef] [PubMed]
- Yamabe, A.; Irisawa, A.; Wada, I.; Shibukawa, G.; Fujisawa, M.; Sato, A.; Igarashi, R.; Maki, T.; Hoshi, K. Application of a silver coating on plastic biliary stents to prevent biofilm formation: An experimental study using electron microscopy. Endosc. Int. Open 2016, 4, E1090–E1095. [Google Scholar] [CrossRef] [PubMed]
- Obermeier, A.; Würstle, S.; Tuebel, J.; Stolte, P.; Feihl, S.; Lipovcic, N.; Lanzinger, S.; Mühlhofer, H.; Weber, A.; Schmid, R.M.; et al. Novel antimicrobial coatings based on polylactide for plastic biliary stents to prevent post-endoscopic retrograde cholangiography cholangitis. J. Antimicrob. Chemother. 2019, 74, 1911–1920. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Adverse Events Group (n = 52) | No Complication/ Controls (n = 37) | Missing (%) | p-Value | |
|---|---|---|---|---|
| Age (years) | 62.5 (46.8–69.2) | 55.0 (48.0–63.0) | 0 | 0.292 |
| Female sex (%) | 26.9 | 24.3 | 0 | 0.811 |
| Body mass index (kg/m²) | 24.5 (22.5–26.9) | 24.3 (22.3–26.7) | 7.5 | 0.693 |
| Smoking history | 56.1 | 66.7 | 13.5 | 0.361 |
| Etiology of pancreatitis (%) | 0 | 0.763 | ||
| Alcoholic | 40.4 | 48.6 | ||
| Biliary | 34.6 | 24.3 | ||
| Idiopathic | 19.2 | 21.6 | ||
| Other | 5.8 | 5.4 | ||
| Charlson Comorbidity Index | 3.0 (2.0–5.0) | 3.0 (1.0–5.0) | 0 | 0.441 |
| Diabetes mellitus (%) | 19.2 | 40.5 | 0 | 0.033 * |
| PERT (%) | 28.8 | 40.5 | 0 | 0.265 |
| History of non-pancreatic malignancy (%) | 7.7 | 5.4 | 0 | 1.000 |
| History of abdominal surgery (%) | 21.2 | 27.0 | 0 | 0.615 |
| White blood cells (Gpt/L) | 11.4 (8.2–18.1) | 10.5 (9.0–16.0) | 0 | 0.784 |
| Hemoglobin (mmol/L) | 7.6 (6.2–8.6) | 7.5 (6.6–8.2) | 0 | 0.916 |
| Hematocrit (%) | 37.6 (31.8–43.2) | 37.0 (33.6–40.2) | 0 | 0.994 |
| Platelet count (Gpt/L) | 278.5 (208.2–389.5) | 303.0 (197.0–384.0) | 0 | 0.746 |
| eGFR < 60 mL/min (%) | 28.8 | 16.2 | 0 | 0.210 |
| Blood urea nitrogen (mmol/L) | 2.3 (1.8–4.2) | 2.3 (1.6–3.2) | 4.5 | 0.168 |
| Albumin (g/L) | 26.0 (20.0–35.0) | 28.0 (23.2–33.2) | 18.0 | 0.475 |
| Lipase (µkatal/L) | 7.4 (2.7–68.2) | 7.2 (2.1–16.2) | 9.0 | 0.104 |
| ALT (µkatal/L) | 0.5 (0.3–0.8) | 0.4 (0.3–0.6) | 4.5 | 0.130 |
| Bilirubin (µmol/L) | 8.5 (5.7–13.1) | 8.7 (5.7–11.4) | 0 | 0.494 |
| CRP (mg/L) | 111.5 (10.0–196.8) | 114.0 (13.8–210.8) | 1.1 | 0.878 |
| Adverse Events Group (n = 52) | No Complication/ Controls (n = 37) | Missing (%) | p-Value | |
|---|---|---|---|---|
| Indication for drainage (%, multiple possible) | ||||
| Suspected infection | 51.9 | 48.6 | 0 | 0.831 |
| Pain (only) | 19.2 | 18.9 | 0 | 1.000 |
| Continuous enlargement of lesion | 13.5 | 16.2 | 0 | 0.767 |
| Gastric outlet obstruction | 11.5 | 13.5 | 0 | 1.000 |
| Biliary obstruction | 1.9 | 5.4 | 0 | 0.568 |
| Other | 11.5 | 2.7 | 0 | 0.232 |
| Type of stent used for initial treatment (%) | 0 | 0.384 | ||
| Plastic pigtail stent(s) | 46.2 | 35.1 | ||
| LAMS | 53.8 | 64.9 | ||
| Type of lesion (%) | 0.645 | |||
| WON | 96.2 | 91.9 | 0 | |
| ANC | 3.8 | 8.1 | 0 | |
| Location of lesion (%, multiple possible) | ||||
| Head | 30.8 | 27.0 | 0 | 0.814 |
| Body | 59.6 | 45.9 | 0 | 0.281 |
| Tail | 50.0 | 59.5 | 0 | 0.398 |
| Lesion maximum diameter (cm) | 10.9 (8.4–15.1) | 7.6 (6.0–10.0) | 0 | <0.001 * |
| Necrosis culture: positive results (%) | 79.6 | 38.9 | 4.5 | <0.001 * |
| Blood culture: positive results (%) | 26.3 | 21.1 | 36.0 | 0.754 |
| Antibiotic treatment (%) | 100.0 | 97.3 | 0 | 0.416 |
| Highest level of care (%) | 0.054 | |||
| Intensive care unit | 48.1 | 27.0 | 0 | |
| Intermediate care | 26.9 | 24.3 | 0 | |
| Regular ward | 25.0 | 48.6 | 0 | |
| Endoscopic necrosectomy performed (%) | 53.9 | 48.7 | 0 | 0.671 |
| Interval (days) between initial drainage and first necrosectomy | 6.5 (3.8–11.0) | 3.5 (2.2–5.0) | 0 | 0.077 |
| Necessity for repeat interventions (%, multiple possible) | 63.5 | 0 | 0 | <0.001 * |
| Endoscopic | 44.2 | - | ||
| Interventional radiology | 28.8 | - | ||
| Surgical | 9.6 | - | ||
| Duration of initial hospital stay (days) | 21.0 (11.8–63.0) | 14.0 (7.0–31.0) | 0 | 0.003 * |
| Duration of endoscopic drainage (days) | 65.0 (47.8–103.2) | 64.5 (51.2–129.0) | 9.5 | 0.853 |
| Total mortality (%) | 15.4 | 5.4 | 0 | 0.185 |
| Therapy-related mortality (%) | 1.9 | 0 | 0 | 1.000 |
| LAMS (n = 55) | Plastic Stents (n = 48) | p-Value | |
|---|---|---|---|
| Stent dislocation | 21.8 | 29.2 | 0.496 |
| Residual lesion | 10.9 | 22.9 | 0.118 |
| Stent obstruction | 12.7 | 4.2 | 0.170 |
| SIRS after drainage | 3.6 | 10.4 | 0.247 |
| Immediate bleeding | 3.6 | 4.2 | 1.000 |
| Delayed bleeding | 7.3 | 2.1 | 0.369 |
| Other rare complications | 10.9 | 6.2 | 0.498 |
| Complication-associated fatality | 1.8 | 0 | 1.000 |
| Any adverse event | 49.1 | 54.2 | 0.694 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frost, F.; Schlesinger, L.; Wiese, M.L.; Urban, S.; von Rheinbaben, S.; Tran, Q.T.; Budde, C.; Lerch, M.M.; Pickartz, T.; Aghdassi, A.A. Infection of (Peri-)Pancreatic Necrosis Is Associated with Increased Rates of Adverse Events during Endoscopic Drainage: A Retrospective Study. J. Clin. Med. 2022, 11, 5851. https://doi.org/10.3390/jcm11195851
Frost F, Schlesinger L, Wiese ML, Urban S, von Rheinbaben S, Tran QT, Budde C, Lerch MM, Pickartz T, Aghdassi AA. Infection of (Peri-)Pancreatic Necrosis Is Associated with Increased Rates of Adverse Events during Endoscopic Drainage: A Retrospective Study. Journal of Clinical Medicine. 2022; 11(19):5851. https://doi.org/10.3390/jcm11195851
Chicago/Turabian StyleFrost, Fabian, Laura Schlesinger, Mats L. Wiese, Steffi Urban, Sabrina von Rheinbaben, Quang Trung Tran, Christoph Budde, Markus M. Lerch, Tilman Pickartz, and Ali A. Aghdassi. 2022. "Infection of (Peri-)Pancreatic Necrosis Is Associated with Increased Rates of Adverse Events during Endoscopic Drainage: A Retrospective Study" Journal of Clinical Medicine 11, no. 19: 5851. https://doi.org/10.3390/jcm11195851
APA StyleFrost, F., Schlesinger, L., Wiese, M. L., Urban, S., von Rheinbaben, S., Tran, Q. T., Budde, C., Lerch, M. M., Pickartz, T., & Aghdassi, A. A. (2022). Infection of (Peri-)Pancreatic Necrosis Is Associated with Increased Rates of Adverse Events during Endoscopic Drainage: A Retrospective Study. Journal of Clinical Medicine, 11(19), 5851. https://doi.org/10.3390/jcm11195851