Abstract
Background: High on-clopidogrel platelet reactivity (HPR) following percutaneous coronary intervention (PCI) is associated with increased ischemic risk. It is unclear whether conventional definitions of HPR apply to patients with concomitant oral anticoagulation (OAC). This study aimed to compare the performance of multiple platelet aggregometry (MEA) and thrombelastography (TEG) to detect HPR in patients with atrial fibrillation (AF) and indication for an OAC. Methods: In this observational single-center cohort study, MEA and TEG were performed in patients with AF with an indication for OAC on day 1 to 3 after PCI. The primary outcome was HPR as assessed by MEA (ADP area under the curve ≥ 46 units [U]) or TEG (MAADP ≥ 47 mm), respectively. The secondary exploratory outcomes were a composite of all-cause death, myocardial infarction (MI) or stroke and bleeding, as defined by the International Society on Thrombosis and Hemostasis, at 6 months. Results: Platelet function of 39 patients was analyzed. The median age was 78 (interquartile range [IQR] was 72–82) years. 25 (64%) patients were male, and 19 (49%) presented with acute coronary syndrome. All patients received acetylsalicylic acid and clopidogrel prior to PCI. Median (IQR) ADP-induced aggregation, MAADP, TRAP-induced aggregation, and MAthrombin were 9 (6–15) U, 50 (43–60) mm, 54 (35–77) U and 65 (60–67) mm, respectively. The rate of HPR was significantly higher if assessed by TEG compared with MEA (25 [64%] vs. 1 [3%]; p < 0.001). Within 6 months, four (10%) deaths, one (3%) MI and nine (23%) bleeding events occurred. Conclusion: In patients with AF undergoing PCI, the rates of HPR detected by TEG were significantly higher compared with MEA. Conventional cut-off values for HPR as proposed by consensus documents may need to be re-evaluated for this population at high ischemic and bleeding risk. Further studies are needed to assess the association with outcomes.
1. Introduction
Approximately one-third of patients with atrial fibrillation (AF) have coexisting coronary artery disease often demanding percutaneous coronary intervention (PCI) [1,2]. Guidelines recommend clopidogrel and a direct oral anticoagulant (DOAC) [3,4,5,6] for most patients with AF undergoing PCI [1,7,8]. The omittance of acetylsalicylic acid (ASA) reduces bleeding risk [3]. Still, 6–8% of AF patients experience ischemic events within 6 months after PCI [1,7]. In patients treated with dual antiplatelet therapy (DAPT), high inter-individual variability of response to clopidogrel therapy has been described. High on-clopidogrel platelet reactivity (HPR) was reported in 21% [9] to 39% [10] of patients depending on the assay and patient characteristics. HPR is associated with increased risk for ischemic events [11,12,13]. Guidelines and consensus documents recommend that platelet functions testing (PFT) could be considered for patients as a tool to adapt antiplatelet therapy [7,13]. Viscoelastic tests such as thrombelastography (TEG) have been widely used as tools to assess hemostasis in patients undergoing surgery, obstetrics and trauma patients, but the use in cardiology and the experience in patients treated with oral anticoagulation is limited.
The association of HPR with ischemic risk might be more pronounced in patients with concomitant DOAC, since ASA is often omitted [1]. It is unclear whether conventional definitions of HPR apply to patients with concomitant oral anticoagulation (OAC) and which PFT is most suitable for detecting HPR for risk stratification in these patients.
This study aimed to compare the performance of multiple electrode aggregometry (MEA) and TEG to detect HPR in patients on clopidogrel and OAC.
2. Methods
2.1. Study Design and Clinical Characteristics
Patients were enrolled in an observational prospective single-center cohort study between May 2020 and May 2021. The ethics committee of the University of Freiburg, Germany, approved the protocol and amendments (registry number 194/20). All patients provided written informed consent to participate in the study. MEA and TEG measurements were performed in 39 consecutive patients at the Department of Cardiology and Angiology I at Heart Center Freiburg University. All patients underwent coronary stent implantation and were treated with ASA periprocedurally. Patients were eligible if 18 years or older, had AF with an indication for OAC (CHA2DS2VASC-score ≥ 1 for males, ≥2 for females) and received PCI within the last 3 days. Exclusion criteria were history of stent thrombosis, a platelet count below 50 × 103 platelets per μL blood, therapy with GPIIb/IIIa-inhibitors in the last 24 h and use of prasugrel or ticagrelor in the last 7 days.
2.2. Blood Samples
Venous blood samples were taken using 21 G butterfly needle (Safety-Multifly®-Set, Sarstedt, Nümbrecht, Germany) to a final concentration of >15 μg/mL r-hirudin (SARSTEDT Monovetten, Nümbrecht, Germany) for MEA and 17 IU/mL Li-heparin (Becton, Dickinson and Company, Heidelberg, Germany) for TEG. Blood samples were stored at room temperature, and platelet function was analyzed according to the manufacturer’s instructions.
2.3. Multiple Electrode Aggregometry
Multiple electrode aggregometry (MEA, Roche Diagnostics, Risch-Rotkreuz, Switzerland) was performed on day 1 to 3 after PCI. Whole blood was stimulated with adenosine diphosphate (ADP; final concentration 6.4 μM) or thrombin receptor activating peptide-6 (TRAP; final concentration 32 μM), respectively. HPRMEA was defined as ADP area under the curve [AUC] ≥ 46 U according to the expert consensus on platelet function and genetic testing [13]. For TRAP-induced platelet aggregation, reference values per manufacturer were 94–156 U [13].
2.4. Thrombelastography
Thrombelastography was performed with TEG 6s Hemostasis Analyzer (Haemonetics Corp., Boston, MA, USA). A multichannel cartridge holding dried reagents was used. Approximately 400 μL blood were automatically aspirated into the testing area and mixed with the required reagents. Then, 2 μM ADP was used as a reagent for platelet function, and kaolin with heparinase (concentration > 1800 IU/mL), eliminating the effects of heparin, was used for overall aggregability. The blood was automatically exposed to ultrasound pulses (20–500 Hz frequency), changing during coagulation depending on clot strength. The maximum amplitude (MA, [mm]) was determined to describe the maximum clot strength. HPRTEG was defined as a MAADP ≥ 47 mm after stimulation with ADP. Kaolin-activated channel HKH-channel was used for MAThrombin (reference values per manufacturer: 53–68 mm).
2.5. Study Outcomes and Follow-Up
The primary outcome was the rate of HPR as assessed by TEG and MEA in patients with AF undergoing PCI. The exploratory secondary outcomes were a composite outcome of all-cause death, myocardial infarction (MI) or stroke [14] and bleeding (major or non-major clinically relevant [NMCR]) as defined by the International Society on Thrombosis and Haemostasis (ISTH) [15] at 6 months. Follow-up was assessed by a structured telephone interview at 6 months ±2 weeks after inclusion in the study. Clinical outcome events were adjudicated by two independent physician reviewers blinded to MEA and TEG results. Major discrepancies were resolved by the PI (CBO) who was blinded to MEA and TEG results.
2.6. Statistical Considerations
Data are presented as number with percentage for binomial variables and median with interquartile range for continuous variables. Categorical variables were compared using Fisher’s exact test. Continuous variables were compared with a 2-sided unpaired t-test or Mann–Whitney U test. Pearson’s correlation test was performed to evaluate the correlation between TEG and MEA. A p value of 0.05 or less was considered significant. Data were analyzed with Prism 12.0.13 (GraphPad Software, La Jolla, CA, USA) and SPSS 27.0.0.1 (SPSS Inc., Chicago, IL, USA).
3. Results
3.1. Patient Population and Medication
Thirty-nine patients were enrolled between day 1 and 3 after PCI. Clinical baseline characteristics are shown in Table 1. The median age was 78 (72–82) years and 25 (64%) were male. Median CHA2DS2-VASC score was 5 (4–6) and median HAS-BLED 3 (3–4). Arterial hypertension was reported in 38 (97%) patients, hyperlipidemia in 30 (77%) patients, diabetes mellitus in 15 (38%) patients and family history of coronary artery disease (CAD) in 10 (26%) patients. Median platelet count was 210 (166–297) × 103/μL. Nineteen (49%) patients underwent PCI due to acute coronary syndrome (ACS), 8 (21%) patients had a history of stroke/transient ischemic attack (TIA), and 8 (21%) patients had a history of gastrointestinal or intracranial bleeding.

Table 1.
Clinical baseline characteristics.
The periprocedural antithrombotic therapy and the antithrombotic therapy at discharge are shown in Table 2. Thirty-four (87%) patients received 250 or 300 mg periprocedural ASA, and five (13%) were on 100 mg ASA maintenance therapy. Thirty-six (92%) patients received an initial, periprocedural dose of 300 or 600 mg clopidogrel. Three (8%) patients had 75 mg clopidogrel per day as maintenance therapy. Oral anticoagulation was interrupted before PCI in six (15%) patients. Low-molecular-weight heparin was used in four (10%) patients.
Table 2.
Periprocedural medication and medication at discharge.
At discharge, all patients were prescribed clopidogrel. ASA was discontinued at discharge in 29 (74%) of the patients. OAC therapy at discharge consisted in the vast majority of patients of DOACs: 8 (20%) edoxaban, 10 (26%) apixaban, 16 (41%) rivaroxaban, and 3 (8%) patients received a vitamin K antagonist (VKA). Two (5%) of the patients had no OAC at discharge.
3.2. Platelet Aggregation Assessed by MEA and TEG
Median ADP-induced aggregation AUC was 9 (IQR 6–15) U and median MAADP was 50 (IQR 43–60) mm (Figure 1).
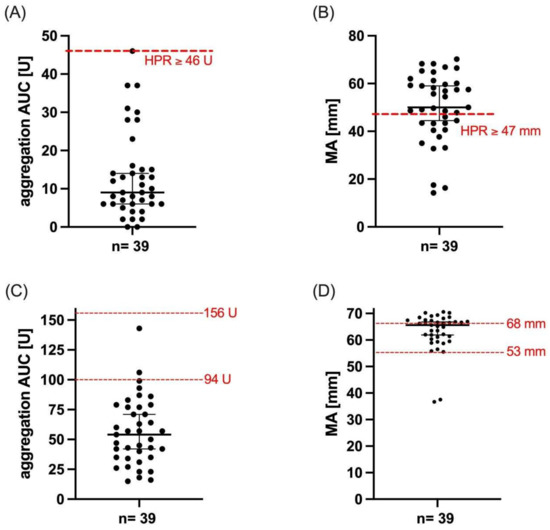
Figure 1.
Platelet reactivity of patients with atrial fibrillation undergoing percutaneous intervention. (A) ADP- and (C) TRAP-induced aggregation as assessed by MEA and MAADP (B) and MAThrombin (D) as assessed by TEG. Median and interquartile range are represented by black lines. Red lines indicate conventional cut-off values (ADP AUC ≥ 46 U and MAADP ≥ 47 mm) or reference values suggested by the manufacturer (TRAP AUC 94-156 U, MAThrombin 53–68 mm), respectively.
The rate of HPR was significantly higher if assessed by TEG compared with MEA 25 (64%) vs. 1 (3%); p < 0.001. Thirty-two (82%) patients received OAC on the day of platelet functioning measurement. No significant difference in ADP-induced aggregation (9 U vs. 11 U; p = 0.09) and MAADP values (59.6 mm vs. 48.5 mm, p = 0.06) were shown when OAC was discontinued at measurement time compared with measurements performed under OAC therapy (Figure 2).
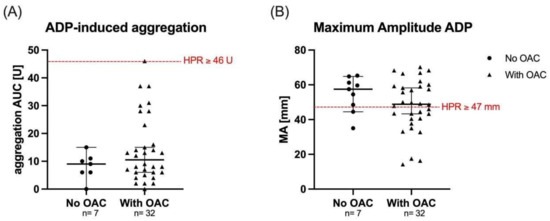
Figure 2.
Platelet reactivity according to oral anticoagulation. Aggregation values for ADP-induced aggregation as assessed by MEA (A) and MAADP as assessed by TEG (B) with and without OAC therapy. Red line represents HPR cut-off and black line median with interquartile range.
Median TRAP-induced aggregation was 54 (IQR 35–77) U and MAThrombin was 66 (IQR 60–67) mm.
ADP-induced aggregation correlated with MAADP (r = 0.45, p < 0.004). TRAP-induced aggregation correlated significantly with MAThrombin (r = 0.36, p = 0.025, Figure 3).
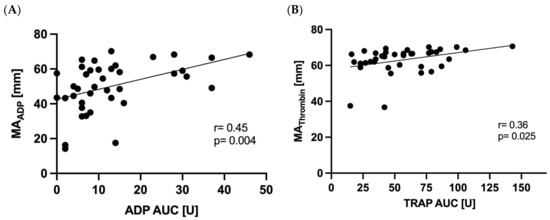
Figure 3.
Correlation of multiple electrode aggregometry with thrombelastography. ADP AUC with MAADP (A) and TRAP AUC with MAThrombin (B).
3.3. Exploratory Clinical Outcomes
The composite exploratory ischemic outcome of death, MI, or stroke occurred in five (13%) patients (five [10%] deaths and one [3%] MI; Table 3). The secondary exploratory outcome NMCR or major bleedings occurred in nine (23%) patients (three [8%] NMCR and six [16%] major bleedings). No significant association of HPR status was observed as assessed by both TEG and MEA with exploratory outcomes. The study had not been powered to detect an association with clinical outcomes.
Table 3.
Exploratory clinical outcomes at 6 months ± 2 weeks according to the presence of HPR and no HPR as assessed by MEA and TEG.
4. Discussion
The main finding of this study is that in patients with AF with an indication for OAC undergoing PCI, the rate of HPR detected by TEG was substantially higher when compared with MEA.
4.1. Multiple Electrode Aggregometry
In patients treated with DAPT, MEA could be considered to assess platelet function and guide antithrombotic therapy [10,13]. The prevalence of HPR as assessed by MEA in patients with DAPT following PCI ranged from 15% up to 39% in patients treated with DAPT after PCI [10,11]. The rate of HPR as assessed by MEA in the present study was low (3%). This might be attributed to the higher rate of AF in the present cohort compared with other studies. AF prevalence increases with age and the presence of comorbidities associated with decreasing platelet reactivity [13]. In a previous study, in patients with AF undergoing PCI, the rate of HPR as assessed by MEA was 15% [11]. However, the majority of these patients were treated with VKA. Studies suggest that VKA attenuates the efficacy of clopidogrel and increases HPR rates [12,16]. In another study in patients with clopidogrel and the DOAC dabigatran, median ADP-induced aggregation was 326 [268–462] (corresponding to 33 [27–46] U as used in the present study) and similar to patients receiving a VKA [17]. Smaller trials investigated platelet aggregation with different assays in patients treated with clopidogrel, ASA and DOAC therapy dabigatran [17,18], edoxaban [19] and low dose rivaroxaban [20]. No effect on clopidogrel-mediated platelet inhibition from different DOACs was observed when platelet aggregation was assessed by MEA or light transmission aggregometry [17,18,19,20]. However, DOAC therapy had been initiated recently in these patients, and it has been stated that alterations in platelet functions may be present when therapy with DOAC is used for a longer period [21]. This might be due to a change in the expression profile of thrombin receptor [21]. Overall, 78% of patients included in the present study were pre-treated with DOAC and not with a VKA. Another study showed that after the first intake of rivaroxaban and dabigatran, ADP-induced aggregation in patients taking clopidogrel was not affected [22]. In the present study, the majority of patients had TRAP-induced aggregation below the reference values. This indicates that the reduced platelet reactivity in these patients might not be exclusively ADP pathway dependent.
4.2. Thrombelastography
Gurbel et al., showed a 10-fold increase in ischemic risk in patients after stenting treated with DAPT when HPR was defined as MAADP ≥47 mm as assessed by TEG [23]. Studies reported HPR rates varying from 21% to nearly 50% in patients undergoing stent implantation after receiving loading with clopidogrel [9,24]. Compared with these rates, in the present study, the rate of HPR assessed by TEG seems high (64%). The patient cohort was elderly and presented with a significant thromboembolic risk. TEG measurements varied significantly between middle-aged and elderly healthy men and women [25]. Others reported a high intra-assay variability of TEG when comparing healthy donors with patients with ASA therapy [26]. These data indicate that reference values might vary according to age.
Smaller trials have evaluated TEG performance in patients treated with triple antithrombotic therapy. Edoxaban prolonged in a dose-dependent manner the speed of thrombin formation when assessed by TEG [19]. Other DOAC such as dabigatran were compared with placebo in patients with coronary artery disease without an indication for oral anticoagulation. Dabigatran affected the parameters related to thrombin formation with no effect on the kaolin-activated clot strength. MAADP was significantly higher in the group treated with dabigatran, showing consistent results with the high median MAADP reported in this study [18].
4.3. Performance of Multiple Electrode Aggregometry and Thrombelastography
In the present study, we identified a significant correlation of TRAP-induced aggregation with MAThrombin as well as ADP-induced aggregation with MAADP. One study performed on 10 healthy volunteers also suggested that linear models could be generated between TEG and MEA [27], but no other studies have compared the performance of TEG with MEA in patients undergoing PCI.
Despite this correlation, the rates of HPR were substantially different between MEA and TEG. This difference might be explained by (1) pre-analytic factors, such as anticoagulant in the blood sampling tube and/or (2) the test principles. Thrombelastography quantifies clot formation, clot strength, and clot stability. MEA principle relies on platelet aggregation and might depend more on isolated platelet function compared with TEG. Consistent with this hypothesis, TEG is less affected by platelet count compared with MEA [28]. TEG, different from other assays, does not bypass other pathways that lead to platelet activation [29].
Most studies evaluating methods that measure platelet aggregation were performed in a setting of only DAPT therapy, have small sample sizes and were not randomized, explaining the conflicting results about the performance of PFT in different patient cohorts.
Further clinical trials are necessary to better explain the mechanisms of these findings.
4.4. Exploratory Outcomes
Death, MI, or stroke occurred in five (13%) patients. Secondary exploratory outcome consisting of NMCR or major bleedings occurred in nine (23%) patients. Different randomized trials compared triple antithrombotic therapy (TAT) with DOAC vs. VKA in patients with AF undergoing PCI and reported lower incidence of ischemic and bleeding events [3,4,5,6].
Chance and the reduced robustness due to the small size of the here presented study might explain the high event rate.
This study was not powered to evaluate the association of HPR with the secondary exploratory outcomes. Further studies need to determine and validate cut-off values to identify patients at risk of ischemic events.
4.5. Study Limitations
The different HPR rates between both methods were observed during exploratory measurements and were not part of a primary study hypothesis. Thus, this current analysis should be considered hypothesis generating. Further studies are necessary to compare these methods and to investigate potential mechanism to explain the observed differences in the assays. Since these findings were part of exploratory analyses, no sample size calculation had been performed regarding the performance of the assays. The low number of events indicates that the study is underpowered to assess association of HPR with ischemic and bleeding outcomes.
5. Conclusions
In patients with AF undergoing PCI, rates of HPR detected by TEG were significantly higher as compared with MEA. These differences indicate that conventional cut-off values for HPR as proposed by consensus documents may need to be re-evaluated for this population at high ischemic and bleeding risk. Further studies will need to investigate the mechanisms of this observation and determine the association of HPR with outcomes according to different definitions.
Author Contributions
Data curation, H.V., D.G., S.S. and V.A.; Formal analysis, D.G., C.B.O., H.V., S.S. and V.A.; Methodology, C.B.O., D.G.; Project administration, C.B.O.; Supervision, D.G. and C.B.O.; Writing—original draft, D.G., H.V., C.B.O.; Writing—review & editing, D.G., H.V., C.B.O., S.L., D.H., D.D. and D.T. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by a grant from the Faculty of Medicine, University of Freiburg to Christoph B. Olivier. Haemonetics® (S.A. Signy-Centre 1274 Signy-Avenex, Switzerland) provided materials to perform thrombelastography.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the University of Freiburg, Germany protocol and amendments were approved in in May 2020 (registry number 194/20).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is not publicly available but can be available on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
Disclosures
CBO received research support from Haemonetics, Deutsche Forschungsgemeinschaft, Faculty of Medicine, Freiburg University; Else Kröner-Fresenius Stiftung; Honoraria: Bayer Vital GmbH; Daiichi Sankyo; Ferrer, Idorsia. DT received within the last 24 months consulting fees/payment for lectures including service on speakers’ bureaus by Alexion Pharma, Amgen, AstraZeneca, Atriva, Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, Daiichi Sankyo, Ferrer, Pfizer and Sanofi.
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Olivier, C.B.; Turakhia, M.P.; Mahaffey, K.W. Anticoagulant and antiplatelet therapy choices for patients with atrial fibrillation one year after coronary stenting or acute coronary syndrome. Expert Opin. Drug Saf. 2018, 17, 251–258. [Google Scholar] [CrossRef]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Ianus, J.; Burton, P.; van Eickels, M.; et al. Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.W.A.; Li, J.; Ten Berg, J.M.; et al. Optimal Antithrombotic Regimens for Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: An Updated Network Meta-analysis. JAMA Cardiol. 2020, 5, 582–589. [Google Scholar] [CrossRef]
- Hou, X.-M.; Han, W.-Z.; Qiu, X.-B.; Fang, W.Y. Clinical characteristics associated with high on-treatment platelet reactivity of patients undergoing PCI after a 300mg loading dose of clopidogrel, measured by thrombelastography. Heart Asia 2013, 5, 66–69. [Google Scholar] [CrossRef][Green Version]
- Sibbing, D.; Aradi, D.; Jacobshagen, C.; Gross, L.; Trenk, D.; Geisler, T.; Orban, M.; Hadamitzky, M.; Merkely, B.; Kiss, R.G.; et al. Guided de-escalation of antiplatelet treatment in patients with acute coronary syndrome undergoing percutaneous coronary intervention (TROPICAL-ACS): A randomised, open-label, multicentre trial. Lancet 2017, 390, 1747–1757. [Google Scholar] [CrossRef]
- Rilinger, J.; Meyer, M.; Schnabel, K.; Weik, P.; Charlet, A.; Esser, J.S.; Zhou, Q.; Bode, C.; Moser, M.; Diehl, P.; et al. High platelet reactivity after P2Y12-inhibition in patients with atrial fibrillation and coronary stenting. J. Thromb. Thrombolysis 2016, 42, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Gruttemeier, J.; Cottin, Y.; Yao, H.; De Maistre, E.; Maza, M.; Bonello, L.; Laine, M.; Resseguier, N.; Zeller, M.; Camoin-Jau, L.; et al. Impact of Platelet Reactivity in ACS Patients on Clinical Outcomes with Triple Antithrombotic Therapy. J. Clin. Med. 2021, 10, 1565. [Google Scholar] [CrossRef] [PubMed]
- Sibbing, D.; Aradi, D.; Alexopoulos, D.; ten Berg, J.; Bhatt, D.L.; Bonello, L.; Collet, J.-P.; Cuisset, T.; Franchi, F.; Gross, L.; et al. Updated Expert Consensus Statement on Platelet Function and Genetic Testing for Guiding P2Y12 Receptor Inhibitor Treatment in Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2019, 12, 1521–1537. [Google Scholar] [CrossRef]
- Hicks, K.A.; Mahaffey, K.W.; Mehran, R.; Nissen, S.E.; Wiviott, S.D.; Dunn, B.; Solomon, S.D.; Marler, J.R.; Teerlink, J.R.; Farb, A.; et al. 2017 Cardiovascular and Stroke Endpoint Definitions for Clinical Trials. Circulation 2018, 137, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C. Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar]
- Sibbing, D.; Von Beckerath, N.; Morath, T.; Stegherr, J.; Mehilli, J.; Sarafoff, N.; Braun, S.; Schulz, S.; Schömig, A.; Kastrati, A. Oral anticoagulation with coumarin derivatives and antiplatelet effects of clopidogrel. Eur. Heart J. 2010, 31, 1205–1211. [Google Scholar] [CrossRef]
- Martischnig, A.M.; Mehilli, J.; Pollak, J.; Petzold, T.; Fiedler, A.K.; Mayer, K.; Schüpke, S.; Sibbing, D.; Massberg, S.; Kastrati, A.; et al. Impact of Dabigatran versus Phenprocoumon on ADP Induced Platelet Aggregation in Patients with Atrial Fibrillation with or without Concomitant Clopidogrel Therapy (the Dabi-ADP-1 and Dabi-ADP-2 Trials). BioMed Res. Int. 2015, 2015, 798486. [Google Scholar] [CrossRef]
- Franchi, F.; Rollini, F.; Cho, J.R.; King, R.; Phoenix, F.; Bhatti, M.; DeGroat, C.; Tello-Montoliu, A.; Zenni, M.M.; Guzman, L.A.; et al. Effects of dabigatran on the cellular and protein phase of coagulation in patients with coronary artery disease on dual antiplatelet therapy with aspirin and clopidogrel: Results from a prospective, randomised, double-blind, placebo-controlled study. Thromb. Haemost. 2016, 115, 622–631. [Google Scholar] [CrossRef]
- Franchi, F.; Rollini, F.; Garcia, E.; Rios, J.R.; Rivas, A.; Agarwal, M.; Kureti, M.; Nagaraju, D.; Wali, M.; Briceno, M.; et al. Effects of Edoxaban on the Cellular and Protein Phase of Coagulation in Patients with Coronary Artery Disease on Dual Antiplatelet Therapy with Aspirin and Clopidogrel: Results of the EDOX-APT Study. Thromb. Haemost. 2020, 120, 83–93. [Google Scholar] [CrossRef]
- Borst, O.; Münzer, P.; Alnaggar, N.; Geue, S.; Tegtmeyer, R.; Rath, D.; Droppa, M.; Seizer, P.; Heitmeier, S.; Heemskerk, J.W.M.; et al. Inhibitory mechanisms of very low–dose rivaroxaban in non–ST-elevation myocardial infarction. Blood Adv. 2018, 2, 715–730. [Google Scholar] [CrossRef]
- Olivier, C.B.; Weik, P.; Meyer, M.; Weber, S.; Anto-Michel, N.; Diehl, P.; Zhou, Q.; Geisen, U.; Bode, C.; Moser, M. TRAP-induced platelet aggregation is enhanced in cardiovascular patients receiving dabigatran. Thromb. Res. 2016, 138, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Olivier, C.B.; Weik, P.; Meyer, M.; Weber, S.; Diehl, P.; Bode, C.; Moser, M.; Zhou, Q. Dabigatran and rivaroxaban do not affect AA- and ADP-induced platelet aggregation in patients receiving concomitant platelet inhibitors. J. Thromb. Thrombolysis 2016, 42, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Gurbel, P.A.; Bliden, K.P.; Navickas, I.A.; Mahla, E.; Dichiara, J.; Suarez, T.A.; Antonino, M.J.; Tantry, U.S.; Cohen, E. Adenosine diphosphate–induced platelet-fibrin clot strength: A new thrombelastographic indicator of long-term poststenting ischemic events. Am. Heart J. 2010, 160, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Chang, H.; Ni, L.; Xue, P.; Li, C.; Yuan, L.; Cui, H.; Yu, C. Analysis of thrombelastogram-guided medication in patients with coronary heart disease after percutaneous coronary intervention. Exp. Ther. Med. 2019, 17, 3047–3052. [Google Scholar] [CrossRef] [PubMed]
- Ni, L.; Xue, P.; An, C.; Yu, X.; Qu, J.; Yao, Y.; Li, Y. Establishment of Normal Range for Thromboelastography in Healthy Middle-Aged and Elderly People of Weihai in China. J. Healthc. Eng. 2021, 2021, 7119779. [Google Scholar] [CrossRef]
- Karon, B.S.; Tolan, N.V.; Koch, C.D.; Wockenfus, A.M.; Miller, R.S.; Lingineni, R.K.; Pruthi, R.K.; Chen, D.; Jaffe, A.S. Precision and Reliability of 5 Platelet Function Tests in Healthy Volunteers and Donors on Daily Antiplatelet Agent Therapy. Clin. Chem. 2014, 60, 1524–1531. [Google Scholar] [CrossRef]
- Dias, J.D.; Pottgiesser, T.; Hartmann, J.; Duerschmied, D.; Bode, C.; Achneck, H.E. Comparison of three common whole blood platelet function tests for in vitro P2Y12 induced platelet inhibition. J. Thromb. Thrombolysis 2020, 50, 135–143. [Google Scholar] [CrossRef]
- Ranucci, M.; Baryshnikova, E. The interaction between preoperative platelet count and function and its relationship with postoperative bleeding in cardiac surgery. Platelets 2017, 28, 794–798. [Google Scholar] [CrossRef]
- Ranucci, M.; Baryshnikova, E. Sensitivity of Viscoelastic Tests to Platelet Function. J. Clin. Med. 2020, 9, 189. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).