
Effectiveness of Therapies Based on Mirror Neuron System to Treat Gait in Patients with Parkinson’s Disease—A Systematic Review



Abstract
:1. Introduction
- -
- Early phase: decrease in speed and stride length, being less automatic.
- -
- Intermediate phase: greater alteration of gait spatiotemporal parameters. Gait festination becomes evident and freezing (“brief episodes of absence or marked reduction of forward progression of the feet, even though there is an intention to walk”) appears [15,16]. Such freezing involves difficulty in initiating walking onset, walking in confined spaces, or walking with time limitation. All of them are related to an increased risk of falls.
- -
- Advanced stage: increase in blockages and the appearance of dyskinesias. Technical aids such as canes or wheelchairs are used to counteract the increased risk of falls.
2. Materials and Methods
2.1. Search Question
2.2. Search Strategy
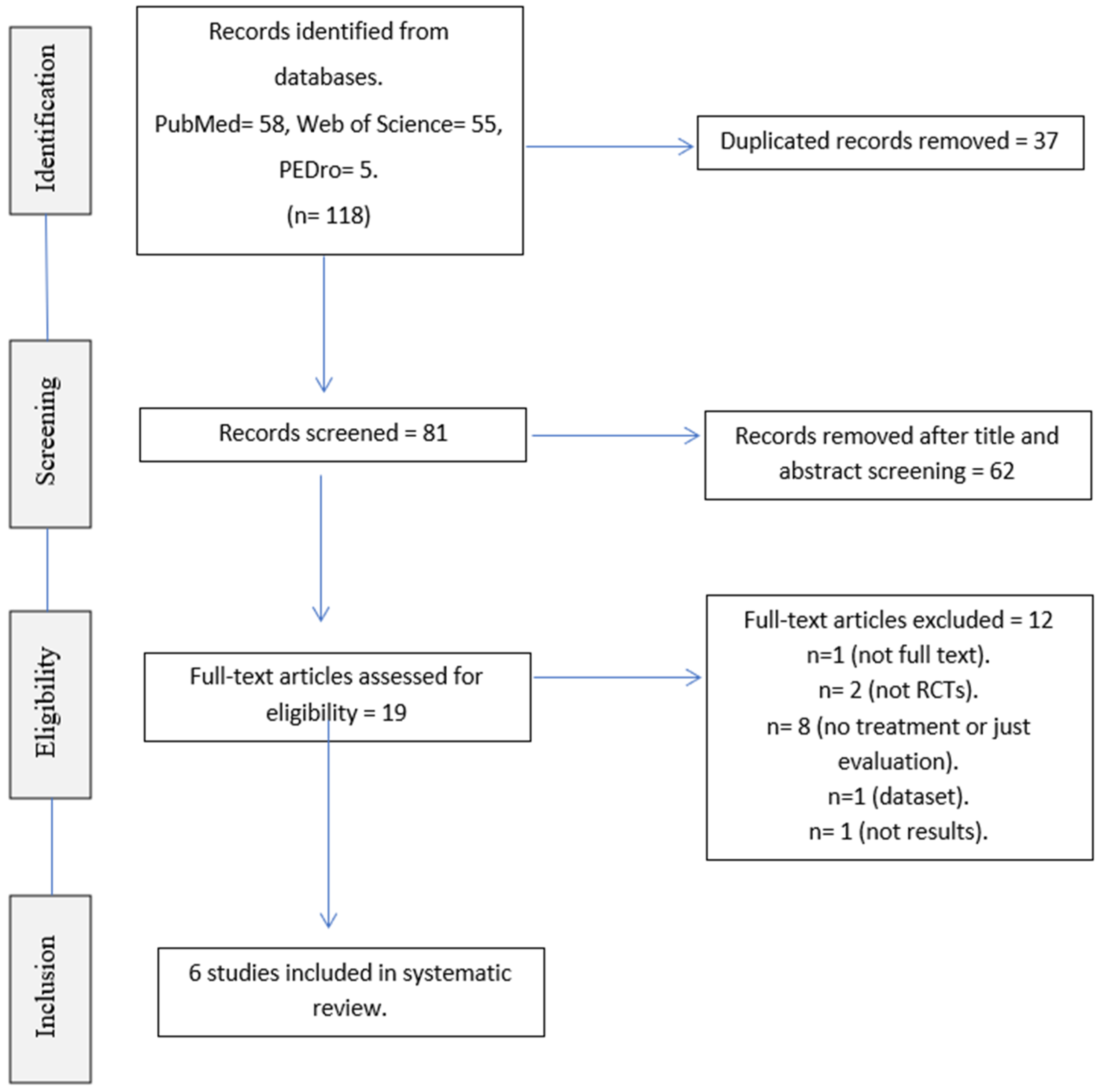
2.3. Study Selection
2.4. Risk of Bias Assessment
3. Results
3.1. Assessment of Risk of Bias
3.2. Results Analysis
- -
- Disease severity.
- -
- Quality of life.
- -
- Balance.
- -
- Gait.
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
References
- Simon, D.K.; Tanner, C.M.; Brundin, P. Parkinson Disease Epidemiology, Pathology, Genetics, and Pathophysiology. Clin. Geriatr. Med. 2019, 36, 1–12. [Google Scholar] [CrossRef]
- Balestrino, R.; Schapira, A.H.V. Parkinson disease. Eur. J. Neurol. 2020, 27, 27–42. [Google Scholar] [CrossRef]
- Bloem, B.R.; Okun, M.S.; Klein, C. Parkinson’s disease. Lancet 2021, 397, 2284–2303. [Google Scholar] [CrossRef]
- Hirsch, L.; Jette, N.; Frolkis, A.; Steeves, T.; Pringsheim, T. The Incidence of Parkinson’s Disease: A Systematic Review and Meta-Analysis. Neuroepidemiology 2016, 46, 292–300. [Google Scholar] [CrossRef]
- Gillies, G.E.; Pienaar, I.S.; Vohra, S.; Qamhawi, Z. Sex differences in Parkinson’s disease. Front. Neuroendocr. 2014, 35, 370–384. [Google Scholar] [CrossRef] [Green Version]
- Tysnes, O.-B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef]
- Conte, A.; Khan, N.; Defazio, G.; Rothwell, J.; Berardelli, A. Pathophysiology of somatosensory abnormalities in Parkinson disease. Nat. Rev. Neurol. 2013, 9, 687–697. [Google Scholar] [CrossRef]
- Pfeiffer, R.F. Non-motor symptoms in Parkinson’s disease. Park. Relat. Disord. 2015, 22, S119–S122. [Google Scholar] [CrossRef]
- Schapira, A.H.V.; Chaudhuri, K.R.; Jenner, P. Non-motor features of Parkinson disease. Nat. Rev. Neurosci. 2017, 18, 435–450, Erratum in Nat. Rev. Neurosci. 2017, 18, 509.. [Google Scholar] [CrossRef]
- Konczak, J.; Corcos, D.M.; Horak, F.; Poizner, H.; Shapiro, M.; Tuite, P.; Volkmann, J.; Maschke, M. Proprioception and Motor Control in Parkinson’s Disease. J. Mot. Behav. 2009, 41, 543–552. [Google Scholar] [CrossRef]
- Chen, Z.; Li, G.; Liu, J. Autonomic dysfunction in Parkinson’s disease: Implications for pathophysiology, diagnosis, and treatment. Neurobiol. Dis. 2019, 134, 104700. [Google Scholar] [CrossRef] [PubMed]
- Debû, B.; De Oliveira Godeiro, C.; Lino, J.C.; Moro, E. Managing Gait, Balance, and Posture in Parkinson’s Disease. Curr. Neurol. Neurosci. Rep. 2018, 18, 23. [Google Scholar] [CrossRef] [PubMed]
- Sveinbjornsdottir, S. The clinical symptoms of Parkinson’s disease. J. Neurochem. 2016, 139, 318–324. [Google Scholar] [CrossRef] [Green Version]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in Parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef]
- Cosentino, C.; Baccini, M.; Putzolu, M.; Ristori, D.; Avanzino, L.; Pelosin, E. Effectiveness of Physiotherapy on Freezing of Gait in Parkinson’s Disease: A Systematic Review and Meta-Analyses. Mov. Disord. 2019, 35, 523–536. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Liu, J.; Tan, Y.; Chen, S. Freezing of gait in Parkinson’s disease: Pathophysiology, risk factors and treatments. Transl. Neurodegener. 2020, 9, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aum, D.J.; Tierney, T.S. Deep brain stimulation foundations and future trends. Front. Biosci. 2018, 23, 162–182. [Google Scholar] [CrossRef] [Green Version]
- Abbruzzese, G.; Marchese, R.; Avanzino, L.; Pelosin, E. Rehabilitation for Parkinson’s disease: Current outlook and future challenges. Park. Relat. Disord. 2016, 22, S60–S64. [Google Scholar] [CrossRef]
- Monteiro-Junior, R.S.; Cevada, T.; Oliveira, B.; Lattari, E.; Portugal, E.M.; Carvalho, A.; Deslandes, A.C. We need to move more: Neurobiological hypotheses of physical exercise as a treatment for Parkinson’s disease. Med. Hypotheses 2015, 85, 537–541. [Google Scholar] [CrossRef]
- McLoughlin, J. Ten guiding principles for movement training in neurorehabilitation. OpenPhysio J. 2020. [Google Scholar] [CrossRef]
- Maier, M.; Ballester, B.R.; Verschure, P.F.M.J. Principles of Neurorehabilitation After Stroke Based on Motor Learning and Brain Plasticity Mechanisms. Front. Syst. Neurosci. 2019, 13, 74. [Google Scholar] [CrossRef] [PubMed]
- Ginis, P.; Nackaerts, E.; Nieuwboer, A.; Heremans, E. Cueing for people with Parkinson’s disease with freezing of gait: A narrative review of the state-of-the-art and novel perspectives. Ann. Phys. Rehabil. Med. 2018, 61, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Horin, A.P.; Harrison, E.C.; Rawson, K.S.; Earhart, G.M. Finger tapping as a proxy for gait: Similar effects on movement variability during external and self-generated cueing in people with Parkinson’s disease and healthy older adults. Ann. Phys. Rehabil. Med. 2020, 64, 101402. [Google Scholar] [CrossRef] [PubMed]
- Muthukrishnan, N.; Abbas, J.J.; Shill, H.A.; Krishnamurthi, N. Cueing Paradigms to Improve Gait and Posture in Parkinson’s Disease: A Narrative Review. Sensors 2019, 19, 5468. [Google Scholar] [CrossRef] [Green Version]
- Cattaneo, L.; Rizzolatti, G. The Mirror Neuron System. Arch. Neurol. 2009, 66, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Rizzolatti, G.; Craighero, L. The mirror-Neuron system. Annu. Rev. Neurosci. 2004, 27, 169–192. [Google Scholar] [CrossRef] [Green Version]
- Cook, R.; Bird, G.; Catmur, C.; Press, C.; Heyes, C. Mirror neurons: From origin to function. Behav. Brain Sci. 2014, 37, 177–192. [Google Scholar] [CrossRef] [Green Version]
- Iacoboni, M.; Molnar-Szakacs, I.; Gallese, V.; Buccino, G.; Mazziotta, J.C.; Rizzolatti, G. Grasping the Intentions of Others with One’s Own Mirror Neuron System. PLoS Biol. 2005, 3, e79. [Google Scholar] [CrossRef] [Green Version]
- Gazzola, V.; Keysers, C. The Observation and Execution of Actions Share Motor and Somatosensory Voxels in all Tested Subjects: Single-Subject Analyses of Unsmoothed fMRI Data. Cereb. Cortex 2008, 19, 1239–1255. [Google Scholar] [CrossRef] [Green Version]
- Small, S.L.; Buccino, G.; Solodkin, A. The mirror neuron system and treatment of stroke. Dev. Psychobiol. 2010, 54, 293–310. [Google Scholar] [CrossRef]
- Mazurek, K.A.; Schieber, M.H. Mirror neurons precede non-mirror neurons during action execution. J. Neurophysiol. 2019, 122, 2630–2635. [Google Scholar] [CrossRef] [PubMed]
- Buccino, G. Action observation treatment: A novel tool in neurorehabilitation. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130185. [Google Scholar] [CrossRef] [PubMed]
- Caligiore, D.; Mustile, M.; Spalletta, G.; Baldassarre, G. Action observation and motor imagery for rehabilitation in Parkinson’s disease: A systematic review and an integrative hypothesis. Neurosci. Biobehav. Rev. 2017, 72, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Bek, J.; Gowen, E.; Vogt, S.; Crawford, T.J.; Poliakoff, E. Combined action observation and motor imagery influences hand movement amplitude in Parkinson’s disease. Park. Relat. Disord. 2018, 61, 126–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbruzzese, G.; Avanzino, L.; Marchese, R.; Pelosin, E. Action Observation and Motor Imagery: Innovative Cognitive Tools in the Rehabilitation of Parkinson’s Disease. Park. Dis. 2015, 2015, 124214. [Google Scholar] [CrossRef] [Green Version]
- Ryan, D.; Fullen, B.; Rio, E.; Segurado, R.; Stokes, D.; O’Sullivan, C. Effect of Action Observation Therapy in the Rehabilitation of Neurologic and Musculoskeletal Conditions: A Systematic Review. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100106. [Google Scholar] [CrossRef]
- Temporiti, F.; Adamo, P.; Cavalli, E.; Gatti, R. Efficacy and Characteristics of the Stimuli of Action Observation Therapy in Subjects With Parkinson’s Disease: A Systematic Review. Front. Neurol. 2020, 11, 808. [Google Scholar] [CrossRef]
- Buchignani, B.; Beani, E.; Pomeroy, V.; Iacono, O.; Sicola, E.; Perazza, S.; Bieber, E.; Feys, H.; Klingels, K.; Cioni, G.; et al. Action observation training for rehabilitation in brain injuries: A systematic review and meta-analysis. BMC Neurol. 2019, 19, 344. [Google Scholar] [CrossRef]
- Ge, S.; Liu, H.; Lin, P.; Gao, J.; Xiao, C.; Li, Z. Neural Basis of Action Observation and Understanding From First- and Third-Person Perspectives: An fMRI Study. Front. Behav. Neurosci. 2018, 12, 283. [Google Scholar] [CrossRef] [Green Version]
- Silva, S.; Borges, L.R.; Santiago, L.; Lucena, L.; Lindquist, A.R.; Ribeiro, T. Motor imagery for gait rehabilitation after stroke. Cochrane Database Syst. Rev. 2020, 9, CD013019. [Google Scholar] [CrossRef]
- Tinaz, S.; Kamel, S.; Aravala, S.S.; Elfil, M.; Bayoumi, A.; Patel, A.; Scheinost, D.; Sinha, R.; Hampson, M. Neurofeedback-guided kinesthetic motor imagery training in Parkinson’s disease: Randomized trial. NeuroImage Clin. 2022, 34, 102980. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, I.A.P.D.S.; Santiago, L.M.D.M.; de Souza, A.A.; Pegado, C.D.L.; Ribeiro, T.S.; Lindquist, A.R.R. Effects of motor imagery training of Parkinson’s disease: A protocol for a randomized clinical trial. Trials 2019, 20, 626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rn, X.Y.; Rn, Y.W.; Shi, T. Effects of motor imagery training on lower limb motor function of patients with chronic stroke: A pilot single-blind randomized controlled trial. Int. J. Nurs. Pract. 2021, 28, e12933. [Google Scholar] [CrossRef]
- Guillot, A.; Hoyek, N.; Louis, M.; Collet, C. Understanding the timing of motor imagery: Recent findings and future directions. Int. Rev. Sport Exerc. Psychol. 2012, 5, 3–22. [Google Scholar] [CrossRef]
- Pinto, T.P.; Ramos, M.M.R.; Lemos, T.; Vargas, C.D.; Imbiriba, L.A. Is heart rate variability affected by distinct motor imagery strategies? Physiol. Behav. 2017, 177, 189–195. [Google Scholar] [CrossRef]
- Guerra, Z.F.; Lucchetti, A.L.G.; Lucchetti, G. Motor Imagery Training After Stroke: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Neurol. Phys. Ther. 2017, 41, 205–214. [Google Scholar] [CrossRef]
- Yepes-Nuñez, J.J.; Urrútia, G.; Romero-García, M.; Alonso-Fernández, S. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. 2021, 74, 790–799, Erratum in Rev. Esp. Cardiol. 2021, 10, 89.. [Google Scholar] [CrossRef]
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Mezzarobba, S.; Grassi, M.; Pellegrini, L.; Catalan, M.; Kruger, B.; Furlanis, G.; Manganotti, P.; Bernardis, P. Action Observation Plus Sonification. A Novel Therapeutic Protocol for Parkinson’s Patient with Freezing of Gait. Front. Neurol. 2018, 8, 723. [Google Scholar] [CrossRef] [Green Version]
- Mezzarobba, S.; Grassi, M.; Pellegrini, L.; Catalan, M.; Krüger, B.; Stragapede, L.; Manganotti, P.; Bernardis, P. Action observation improves sit-to-walk in patients with Parkinson’s disease and freezing of gait. Biomechanical analysis of performance. Park. Relat. Disord. 2020, 80, 133–137. [Google Scholar] [CrossRef]
- Agosta, F.; Gatti, R.; Sarasso, E.; Volonté, M.A.; Canu, E.; Meani, A.G.M.; Sarro, L.; Copetti, M.; Cattrysse, E.; Kerckhofs, E.; et al. Brain plasticity in Parkinson’s disease with freezing of gait induced by action observation training. J. Neurol. 2016, 264, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Abraham, A.; Hart, A.; Andrade, I.; Hackney, M.E. Dynamic Neuro-Cognitive Imagery Improves Mental Imagery Ability, Disease Severity, and Motor and Cognitive Functions in People with Parkinson’s Disease. Neural Plast. 2018, 2018, 6168507. [Google Scholar] [CrossRef] [PubMed]
- Sarasso, E.; Agosta, F.; Piramide, N.; Gardoni, A.; Canu, E.; Leocadi, M.; Msc, V.C.; Basaia, S.; Tettamanti, A.; Volontè, M.A.; et al. Action Observation and Motor Imagery Improve Dual Task in Parkinson’s Disease: A Clinical/fMRI Study. Mov. Disord. 2021, 36, 2569–2582. [Google Scholar] [CrossRef] [PubMed]
- Pelosin, E.; Barella, R.; Bet, C.; Magioncalda, E.; Putzolu, M.; Di Biasio, F.; Cerulli, C.; Casaleggio, M.; Abbruzzese, G.; Avanzino, L. Effect of Group-Based Rehabilitation Combining Action Observation with Physiotherapy on Freezing of Gait in Parkinson’s Disease. Neural Plast. 2018, 2018, 4897276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, S.; Beurskens, A.; Kleynen, M.; Schols, J.; Wade, D. Rehabilitation with mental practice has similar effects on mobility as rehabilitation with relaxation in people with Parkinson’s disease: A multicentre randomised trial. J. Physiother. 2011, 57, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Taximaimaiti, R.; Wang, X.-P. Comparing the Clinical and Neuropsychological Characteristics of Parkinson’s Disease With and Without Freezing of Gait. Front. Neurosci. 2021, 15, 660340. [Google Scholar] [CrossRef]
- Caligiore, D.; Mustile, M.; Fineschi, A.; Romano, L.; Piras, F.; Assogna, F.; Pontieri, F.E.; Spalletta, G.; Baldassarre, G. Action Observation With Dual Task for Improving Cognitive Abilities in Parkinson’s Disease: A Pilot Study. Front. Syst. Neurosci. 2019, 13, 7. [Google Scholar] [CrossRef]
- De Freitas, T.B.; Leite, P.H.W.; Doná, F.; Pompeu, J.E.; Swarowsky, A.; Torriani-Pasin, C. The effects of dual task gait and balance training in Parkinson’s disease: A systematic review. Physiother. Theory Pract. 2018, 36, 1088–1096. [Google Scholar] [CrossRef]

{kind=link}
| Agosta et al. [51] | Abraham et al. [52] | Mezzarobba et al. [49] | Pelosin et al. [54] | Mezzarobba et al. [50] | Sarasso et al. [53] | ||
|---|---|---|---|---|---|---|---|
| Sample size | EG | 12 | 10 | 12 | 33 | 12 | 13 |
| CG | 13 | 10 | 10 | 31 | 10 | 12 | |
| Age | EG | 69.0 ± 8.0 | 66.4 ± 12.5 | 74.67 ± 5.93 | 70.4 ± 4.5 | 74.67± 5.93 | 67.51 ± 6.12 |
| CG | 64.0 ± 7.0 | 65.1 ± 7.5 | 72 ± 5.87 | 72.8 ± 3.1 | 72 ± 5.87 | 63.81 ± 9.23 | |
| Gender | EG | 10 M/2 W | 9 M/1 W | 7 M/5 W | 16 M/17 W | 7 M/5 W | 8 M/5 W |
| CG | 8 M/5 W | 7 M/3 W | 7 M/3 W | 15 M/16 W | 7 M/3 W | 8 M/4 W | |
| Treatment type | AO | DNI | AO + Sonification | AO | AO + Sonification | Dual task + AO − MI | |
| Years of illness | EG | ≥5 | 6.1 ± 3.8 | 10.75 ± 3.44 | 10.7 ± 3.9 | 10.75 ± 3.44 | 8.08 ± 4.13 |
| CG | ≥5 | 8.5 ± 4.5 | 9.4 ± 4.86 | 9.5 ± 4.2 | 9.4 ± 4.86 | 7.92 ± 3.53 | |
| LEDD (mg) | EG | 897 ± 508 | NA | 972.5 ± 253.17 | 435.2 ± 158.5 | 972.5 ± 253.17 | 757.23 ± 480.49 |
| CG | 988 ± 345 | NA | 983.22 ± 379.58 | 383.1 ± 270.2 | 983.22 ± 379.58 | 555 ± 217.25 | |
| FOG | YES | YES | YES | YES | YES | YES | |
| UPDRS III | EG | 27.6 ± 9.7 | 38.4 ± 13.8 | 32.92 ± 8.69 | 31.6 ± 6.1 | 32.92 ± 8.69 | 26.27 ± 9.88 |
| CG | 23.5 ± 7.9 | 32.1 ± 12.2 | 33.2 ± 13.99 | 30.9 ± 7.2 | 33.2 ± 13.99 | 28.83 ± 8.47 | |
| Hoehn and Yahr Scale (mean ± SD) | EG | 2.3 ± 0.4 | 2.0 (1.8, 2.5) * | 2.33 ± 0.49 | 2.4 ± 0.5 | 2.33 ± 0.49 | 2.3 |
| CG | 2.2 ± 0.3 | 2.0 (2.0, 2.5) * | 2.3 ± 0.67 | 2.6 ± 0.3 | 2.3 ± 0.67 | 2.4 | |
| PDQ-39 | EG | 24.7 ± 11.1 | NA | 51.67 ± 26.9 | NA | 51.67 ± 26.9 | 18.19 ± 7.52 |
| CG | 20.2 ± 11.6 | NA | 50.8 ± 29.43 | NA | 50.8 ± 29.43 | 18.95 ± 12.16 |
| Study | Sample and Treatment | Duration | Measurements | Results |
|---|---|---|---|---|
| Agosta et al. [51] | N = 25 EG (12): Observation: 2 videos presenting strategies to avoid FOG episodes with auditory signal associated. Each video lasts 6 min and was repeated twice. Six videos in total. Execution: 8 min after each viewing. Accompanied by auditory signals. CG (13): Observation: static landscape sequences videos. Execution: same actions as EG under physiotherapist instructions. | 60 min/day. 3 sessions/week. 4 weeks. | PRE, POST, and 4 weeks follow-up. (i) Disease severity: HY, UPDRS III. (ii) Freezing severity: FOG-Q, UPDRS II. (iii) Motor function: 10 MWT, BBS. (iv) Quality of life: PDQ-39. (v) fMRI. | EG: POST: p < 0.05 in FOG-Q, UPDRS II ON, UPDRS III ON, PDQ-39, BBS, and 10 MWT. Week 8: p < 0.05 in UPDRS III ON, PDQ-39, BBS, and 10 MWT. CG: POST: p < 0.05 in FOG-Q, PDQ-39, and 10 M WT. Not maintained in 4 weeks follow-up. Groups comparisons p < 0.05 in UPDRS III ON in POST. |
| Abraham et al. [52] | N = 20 EG (10): DNI: DNI warm-up (15 min), DNI concept introduction and practice A (35 min), rest (10 min), DNI concept introduction and practice B (35 min), DNI movement session (20 min), and DNI cool-down (5 min). CG (10): Home intervention: health-related texts reading (1.5 h) and 30-min exercise video target on PD impairments. Telephone follow-up 3 times over the treatment. | 2 h/day. 5 sessions/week. 2 weeks. | PRE and 2–5 days POST intervention. (i) Disease severity: UPDRS, ABC, IPA, BPI, BDI: II. (ii) Motor function: TUG, Fwd gait, 6 MWT, 360° turn test, PRT, 30 s chair stand. (iii) Cognitive function: Trail Making test, BSM, BPST, Reverse Corsi Blocks Visuospatial task. (iv) Imaginary Measures: MIQ-RS, KVIQ-20, VMIQ-2. (v) Satisfaction questionnaire. | EG vs. CG: POST. p < 0.05 in all imaginary measures except for MIQ-RS kinesthetic and VMIQ-2 kinesthetic. (i) IPA p < 0.05. (ii) p < 0.05 in TUG- manual, 360° turn test, PRT. (iii) BPST span p < 0.05. EG is more improved than CG. |
| Mezzarobba et al. [49] | N = 22 EG (12): Observation + sonification: 8 audio-video (1.5 min each one) of 8 specific gait motor gestures related to FOG. Each video twice. Execution: repetition of the same actions (1.5 min each action) after each video observation. CG (10): Execution: same 8 gestures using visual and auditory cues to facilitate the learning of spatial-temporal parameters. Both groups were supervised by a physiotherapist. | 60 min/day. 2 sessions/week. 8 weeks. | PRE, POST, and 1- and 3-month follow-ups. (i) NFOG-Q (main outcome). (ii) Disease severity: UPDRS, HY. (iii) Quality of life: PDQ-39. (iv) Motor function: MPAS, TUG, 6 MWT, BBS. (v) Neuropsychological evaluation. | EG significant improvements compared to CG (p < 0.05) in NFOG-Q, PDQ-39 (mobility and discomfort subscales), and UPDRS III. Results are maintained at 3 months follow-up. BBS significant improvements in EG. |
| Pelosin et al. [54] | N = 64. Group intervention. EG (33): Observation: 2 videos/session (from a total of 6) (6 min/video) with strategies for circumventing FOG. Execution: practice strategies under supervision. Progressive increase in video complexity. CG (31): Observation: 2 videos/session, with sequences of static pictures, with same duration as EG. Execution: same actions and amount of time than EG. | 45 min/day. 2 sessions/week. 5 weeks. | PRE, POST, and 4 weeks follow-up after treatment ends. (i) FOG-Q (ii) TUG (iii) BBS (iv) 10 MWT | PRE vs. POST: significant changes (p < 0.05) in all variables of EG and CG. PRE vs. 4 weeks follow-up: p < 0.05 in all variables of EG and in 10 MWT of CG. |
| Mezzarobba et al. [50] | N = 22 EG (12): Observation + sonification: 8 audio-video/session (1.5 min each one) of 8 specific gait motor gestures, related to FOG. Each video twice. Execution: repetition of the same actions (1.5 min each action) after each video observation. CG (10): Execution: same 8 gestures using visual and auditory cues to facilitate the learning of spatial-temporal parameters. Both groups were supervised by a physiotherapist. | 60 min/day. 2 sessions/week. 8 weeks. | PRE, POST, and 1- and 3-months follow-ups. (i) Postural control: sit-to-walk task (STW). Measured: COM and COP in 6 positions task-specific events. | EG: COM: no significance. COP: significant differences PRE vs. 3 months follow-up in percentiles 10–35 and 63–72. Heel take-off is performed earlier and the STW task is significantly shorter in duration. The COP is significantly lower. CG: COM and COP no significant changes. |
| Sarasso et al. [53] | N = 25 EG (13): Dual task + AO − MI. Four gait/balance exercises each session (2 min observation task + 5 min execution task + 2 min imagination task + 5 min execution task). CG (12): Dual task. Four gait/balance exercises combined with video observation of static landscape instead of observation-imagination. Difficulty increases during the treatment of EG and CG to include dual-task. | 60 min/day. 3 sessions/week. 6 weeks. | PRE, POST, and 8 weeks follow-up. (i) Disease severity: HY, UPDRS, ABC. (ii) Quality of life: PDQ-39. (iii) Gait: TUG, 10 MWT, NFOG-Q (iv) Balance: MiniBESTest. (v) Cognitive evaluation: AST. (vi) Scanner MRI. Motor task (feet dorsiflexion) with eyes closed. Dual task: mentally count from 100 subtracting by 3. | EG: POST and 8 weeks follow-up. p < 0.05 in TUG, TUG-COG, TUG-MAN, its relative peak and rotational speed, DTC during TUG-COG, DTC on the average rotational speed of TUG-COG, MiniBESTest, ABC, 10 MWT, NFOG-Q, and PDQ-39. POST: p < 0.05 in MDS-UPDRS III OFF, HY OFF, and AST. CG: POST: p < 0.05 in TUG, TUG-COG, TUG-MAN, DTC in average rotational speed in TUG-COG, MDS-UPDRS III OFF, and AST. Eight weeks follow-up: p < 0.05 in TUG, TUG-COG, TUG-MAN, MDS-UPDRS III ON, and rotational speed during TUG- COG. EG vs. CG. POST and 8 weeks follow-up: EG significative improvements regarding CG in TUG-COG, average and peak rotational speed in TUG-COG, peak rotational speed in TUG, TUG-MAN, DTC during TUG- COG, MiniBESTest, 10 MWT (normal speed), and ABC. |
| Agosta et al. [51] | Abraham et al. [52] | Mezzarobba et al. [49] | Pelosin et al. [54] | Mezzarobba et al. [50] | Sarasso et al. [53] | |
|---|---|---|---|---|---|---|
| Eligibility criteria | Yes | Yes | Yes | Yes | No | Yes |
| Random participant allocation | Yes | Yes | Yes | Yes | Yes | Yes |
| Concealed allocation | Yes | No | Yes | No | No | Yes |
| Groups similar at baseline | Yes | Yes | Yes | Yes | No | Yes |
| Subjects blinding | No | No | No | No | No | No |
| Therapist blinding | No | No | No | No | No | No |
| Assessor blinding | Yes | No | Yes | No | No | Yes |
| Less than 15% dropouts | No | No | Yes | Yes | No | Yes |
| Intention to treat analysis | No | No | Yes | No | No | No |
| Between groups statistical comparisons | Yes | Yes | Yes | Yes | Yes | Yes |
| Point measures and variability data | Yes | Yes | Yes | Yes | Yes | Yes |
| Total | 6/10 | 4/10 | 8/10 | 5/10 | 3/10 | 7/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lahuerta-Martín, S.; Llamas-Ramos, R.; Llamas-Ramos, I. Effectiveness of Therapies Based on Mirror Neuron System to Treat Gait in Patients with Parkinson’s Disease—A Systematic Review. J. Clin. Med. 2022, 11, 4236. https://doi.org/10.3390/jcm11144236
Lahuerta-Martín S, Llamas-Ramos R, Llamas-Ramos I. Effectiveness of Therapies Based on Mirror Neuron System to Treat Gait in Patients with Parkinson’s Disease—A Systematic Review. Journal of Clinical Medicine. 2022; 11(14):4236. https://doi.org/10.3390/jcm11144236
Chicago/Turabian StyleLahuerta-Martín, Silvia, Rocío Llamas-Ramos, and Inés Llamas-Ramos. 2022. "Effectiveness of Therapies Based on Mirror Neuron System to Treat Gait in Patients with Parkinson’s Disease—A Systematic Review" Journal of Clinical Medicine 11, no. 14: 4236. https://doi.org/10.3390/jcm11144236
APA StyleLahuerta-Martín, S., Llamas-Ramos, R., & Llamas-Ramos, I. (2022). Effectiveness of Therapies Based on Mirror Neuron System to Treat Gait in Patients with Parkinson’s Disease—A Systematic Review. Journal of Clinical Medicine, 11(14), 4236. https://doi.org/10.3390/jcm11144236