
Single-Centre Retrospective Evaluation of Intraoperative Hemoadsorption in Left-Sided Acute Infective Endocarditis

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Patients
2.3. Data Collection
2.4. Statistical Analysis
2.5. Definitions
3. Results
3.1. Operative Characteristics
3.2. Outcomes
3.3. Regression Analyses for Sepsis, Sepsis-Associated Mortality and In-Hospital Mortality
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pettersson, G.B.; Hussain, S.T. Current AATS guidelines on surgical treatment of infective endocarditis. Ann. Cardiothorac. Surg. 2019, 8, 630–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iunget, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC)Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015, 36, 3075–3128. [Google Scholar] [PubMed]
- Farag, M.; Borst, T.; Sabashnikov, A.; Zeriouh, M.; Schmack, B.; Arif, R.; Beller, C.J.; Popov, A.-F.; Kallenbach, K.; Ruhparwar, A.; et al. Surgery for Infective Endocarditis: Outcomes and Predictors of Mortality in 360 Consecutive Patients. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2017, 23, 3617–3626. [Google Scholar] [CrossRef] [PubMed]
- Boss, K.; Jahn, M.; Wendt, D.; Haidari, Z.; Demircioglu, E.; Thielmann, M.; Ruhparwar, A.; Kribben, A.; Tyczynski, B. Extracorporeal cytokine adsorption: Significant reduction of catecholamine requirement in patients with AKI and septic shock after cardiac surgery. PLoS ONE 2021, 16, e0246299. [Google Scholar] [CrossRef]
- Santer, D.; Miazza, J.; Koechlin, L.; Gahl, B.; Rrahmani, B.; Hollinger, A.; Eckstein, F.; Siegemund, M.; Reuthebuch, O. Hemoadsorption during Cardiopulmonary Bypass in Patients with Endocarditis Undergoing Valve Surgery: A Retrospective Single-Center Study. J. Clin. Med. 2021, 10, 564. [Google Scholar] [CrossRef]
- Della Corte, A.; Di Mauro, M.; Dato, G.A.; Barili, F.; Cugola, D.; Gelsomino, S.; Santè, P.; Carozza, A.; della Ratta, E.; Galletti, L. Surgery for prosthetic valve endocarditis a retrospective study of a national registry. Eur. J. Cardiothorac. Surg. 2017, 52, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Pang, P.Y.; Sin, Y.K.; Lim, C.H.; Tan, T.E.; Lim, S.L.; Chao, V.T.; Chua, Y.L. Surgical management of infective endocarditis: An analysis of early and late outcomes. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2015, 47, 826–832. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Warkentin, T.E.; Thachil, J.; van der Poll, T.; Levi, M. the Scientific and Standardization Committee on DIC; the Scientific and Standardization Committee on Perioperative and Critical Care of the International Society on Thrombosis and Haemostasis. Diagnosis and management of sepsis-induced coagulopathy and disseminated intravascular coagulation. J. Thromb. Haemost. 2019, 17, 1989–1994. [Google Scholar]
- Holub, M.; Džupová, O.; Růžková, M.; Stráníková, A.; Bartáková, E.; Máca, J.; Beneš, J.; Herwald, H.; Beran, O. Selected Biomarkers Correlate with the Origin and Severity of Sepsis. Mediat. Inflamm. 2018, 2018, e7028267. [Google Scholar] [CrossRef]
- Buyukasýk, N.S.; Ileri, M.; Alper, A.; Senen, K.; Atak, R.; Hisar, I.; Yetkin, E.; Turhan, H.; Demirkan, D. Increased blood coagulation and platelet activation in patients with infective endocarditis and embolic events. Clin. Cardiol. 2004, 27, 154–158. [Google Scholar] [CrossRef]
- Honore, P.M.; Hoste, E.; Molnár, Z.; Jacobs, R.; Joannes-Boyau, O.; Malbrain, M.L.; Forni, L.G. Cytokine removal in human septic shock: Where are we and where are we going? Ann. Intensive Care 2019, 9, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olmos, C.; Vilacosta, I.; Habib, G.; Maroto, L.; Fernández, C.; López, J.; Sarriá, C.; Salaun, E.; Di Stefano, S.; Carnero, M.; et al. Risk score for cardiac surgery in active left-sided infective endocarditis. Heart Br. Card Soc. 2017, 103, 1435–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tattevin, P.; Fillâtre, P.; Tchamgoué, S.; Lesouhaitier, M.; Nesseler, N.; Tadié, J.M. Should we include microorganisms in scores to predict outcome in candidates for cardiac surgery during the acute phase of endocarditis? J. Thorac. Dis. 2019, 11, E158–E162. [Google Scholar] [CrossRef] [PubMed]
- Träger, K.; Fritzler, D.; Fischer, G.; Schröder, J.; Skrabal, C.; Liebold, A.; Reinelt, H. Treatment of post-cardiopulmonary bypass SIRS by hemoadsorption: A case series. Int. J. Artif. Organs 2016, 39, 141–146. [Google Scholar] [CrossRef]
- Gruda, M.C.; Ruggeberg, K.G.; O’Sullivan, P.; Guliashvili, T.; Scheirer, A.R.; Golobish, T.D.; Capponi, V.J.; Chan, P.P. Broad adsorption of sepsis-related PAMP and DAMP molecules, mycotoxins, and cytokines from whole blood using CytoSorb® sorbent porous polymer beads. PLoS ONE 2018, 13, e0191676. [Google Scholar] [CrossRef]
- Diab, M.; Tasar, R.; Sponholz, C.; Lehmann, T.; Pletz, M.W.; Bauer, M.; Brunkhorst, F.M.; Doenst, T. Changes in inflammatory and vasoactive mediator profiles during valvular surgery with or without infective endocarditis: A case control pilot study. PLoS ONE 2020, 15, e0228286. [Google Scholar] [CrossRef]
- Diab, M.; Lehmann, T.; Bothe, W.; Akhyari, P.; Platzer, S.; Wendt, D.; Deppe, A.-C.; Strauch, J.; Hagel, S.; Günther, A.; et al. Cytokine Hemoadsorption during Cardiac Surgery Versus Standard Surgical Care for Infective Endocarditis (REMOVE): Results from a Multicenter Randomized Controlled Trial. Circulation 2022, 145, 959–968. [Google Scholar] [CrossRef]
- Haidari, Z.; Wendt, D.; Thielmann, M.; Mackowiak, M.; Neuhäuser, M.; Jakob, H.; Ruhparwar, A.; El-Gabry, M. Intraoperative Hemoadsorption in Patients with Native Mitral Valve Infective Endocarditis. Ann. Thorac. Surg. 2020, 110, 890–896. [Google Scholar] [CrossRef]
- Holmén, A.; Corderfeldt, A.; Lannemyr, L.; Dellgren, G.; Hansson, E.C. Whole Blood Adsorber during CPB and Need for Vasoactive Treatment after Valve Surgery in Acute Endocarditis: A Randomized Controlled Study. J. Cardiothorac. Vasc. Anesth. 2022, 36, 3015–3020. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–888. [Google Scholar] [CrossRef] [Green Version]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G., Jr.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2000, 30, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Chu, V.H.; Sexton, D.J.; Cabell, C.H.; Barth, R.L.; Pappas, P.A.; Singh, R.K.; Fowler, V.G.; Ralph, C.G.; Aksoy, O.; Woods, C.W. Repeat Infective Endocarditis: Differentiating Relapse from Reinfection. Clin. Infect. Dis. 2005, 41, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Habib, G.; Erba, P.A.; Iung, B.; Donal, E.; Cosyns, B.; Laroche, C.; Popescu, B.A.; Prendergast, B.; Tornos, P.; Sadeghpour, A.; et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: A prospective cohort study. Eur. Heart J. 2019, 40, 3222–3232. [Google Scholar] [CrossRef] [Green Version]
- Howitt, S.H.; Herring, M.; Malagon, I.; McCollum, C.N.; Grant, S.W. Incidence and outcomes of sepsis after cardiac surgery as defined by the Sepsis-3 guidelines. Br. J. Anaesth. 2018, 120, 509–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kogelmann, K.; Jarczak, D.; Scheller, M.; Drüner, M. Hemoadsorption by CytoSorb in septic patients: A case series. Crit Care. 2017, 21, 74. [Google Scholar] [CrossRef] [Green Version]
- Vahdatpour, C.; Collins, D.; Goldberg, S. Cardiogenic Shock. J. Am. Heart Assoc. 2019, 8, e011991. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Rugg, C.; Klose, R.; Hornung, R.; Innerhofer, N.; Bachler, M.; Schmid, S.; Fries, D.; Ströhle, M. Hemoadsorption with CytoSorb in Septic Shock Reduces Catecholamine Requirements and In-Hospital Mortality: A Single-Center Retrospective “Genetic” Matched Analysis. Biomedicines 2020, 8, 539. [Google Scholar] [CrossRef]
- Lerche, C.J.; Schwartz, F.; Theut, M.; Fosbøl, E.L.; Iversen, K.; Bundgaard, H.; Høiby, N.; Moser, C. Anti-biofilm Approach in Infective Endocarditis Exposes New Treatment Strategies for Improved Outcome. Front. Cell Dev. Biol. 2021, 9, 643335. [Google Scholar] [CrossRef]
- Rowe, S.E.; Wagner, N.J.; Li, L.; Beam, J.E.; Wilkinson, A.D.; Radlinski, L.C.; Zhang, Q.; Miao, E.A.; Conlon, B.P. Reactive oxygen species induce antibiotic tolerance during systemic Staphylococcus aureus infection. Nat. Microbiol. 2020, 5, 282–290. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Preoperative Characteristics | ||||||
|---|---|---|---|---|---|---|
| Unadjusted | Propensity Score Match | |||||
| Control (n = 103) | Hemoadsorption (n = 99) | p Value | Control (n = 99) | Hemoadsorption (n = 99) | p Value | |
| Demographics | ||||||
| Age (years) | 69 [58;77] | 67 [58;75] | 0.612 | 68.0 [56.5;76.0] | 68.0 [56.5;76.0] | 0.745 |
| BMI (kg/m2) | 26.4 [23.8;30.8] | 26.8 [24.0;30.6] | 0.891 | 26.4 [23.9;31.0] | 26.8 [24.0;30.6] | 0.951 |
| Gender (% male) | 83 (80.6%) | 81 (81.8%) | 0.964 | 79 (79.8%) | 81 (81.8%) | 0.857 |
| EuroScore II (%) | 9 [3.6;22.2] | 9.9 [5.5;21.8] | 0.805 | 8.95 [3.58;21.1] | 9.89 [5.5;21.8] | 0.705 |
| Native valve IE | 76 (37.6%) | 49 (24.1%) | 0.106 | 73 (73.7%) | 49 (24.1%) | 0.110 |
| Prosthetic valve IE | 27 (13.3%) | 40 (19.9%) | 0.169 | 27 (27.3%) | 40 (19.9%) | 0.218 |
| CAD | 28 (27.5%) | 28 (28.3%) | 1.000 | 25 (25.5%) | 28 (28.3%) | 0.781 |
| Diabetes Mellitus (II) | 25 (24.3%) | 23 (23.2%) | 0.993 | 25 (25.3%) | 23 (23.2%) | 0.868 |
| pAOD | 6 (5.8%) | 3 (3%) | 0.499 | 4 (4.04%) | 3 (3.03%) | 1.000 |
| History of CVI | 19 (18.4%) | 32 (32.3%) | 0.035 | 19 (19.2%) | 32 (32.3%) | 0.051 |
| Septic embolisms (last 3 weeks) | 19 (18.4%) | 21 (21.2%) | 0.752 | 19 (19.2%) | 21 (21.2%) | 0.860 |
| COPD | 20 (19.4%) | 14 (14.1%) | 0.416 | 18 (18.2%) | 14 (14.1%) | 0.562 |
| Liver cirrhosis | 4 (3.9%) | 6 (6.1%) | 0.533 | 4 (4.08%) | 6 (6.1%) | 0.747 |
| AF preop. | 20 (19.4%) | 27 (27.3%) | 0.248 | 20 (20.2%) | 27 (27.3%) | 0.316 |
| eGFRCKD-EPI (mL/min) | 62 [38;79] | 52 [40;74] | 0.380 | 62.0 [39.5;78.5] | 52.0 [40.0;74.0] | 0.340 |
| RRT preop. | 10 (9.7%) | 8 (8.1%) | 0.874 | 9 (9.09%) | 8 (8.1%) | 1.000 |
| Antiplatelet therapy | 32 (31.1%) | 22 (23.2%) | 0.276 | 30 (30.3%) | 22 (23.2%) | 0.337 |
| Oral anticoagulant therapy | 13 (12.7%) | 10 (10.4%) | 0.772 | 12 (12.2%) | 10 (10.4%) | 0.861 |
| Clinical status | ||||||
| NYHA (III-IV) | 73 (70.9%) | 78 (78.8%) | 0.257 | 72 (72.7%) | 78 (78.8%) | 0.407 |
| Inotropes preop. | 36 (35.0%) | 40 (40.8%) | 0.477 | 35 (35.4%) | 40 (40.8%) | 0.520 |
| Septic shock (within 48 h) | 17 (16.5%) | 19 (19.2%) | 0.753 | 16 (16.2%) | 19 (19.2%) | 0.709 |
| Ventilated preop. | 12 (11.7%) | 9 (9.2%) | 0.733 | 12 (12.1%) | 9 (9.2%) | 0.662 |
| Laboratory Parameters | ||||||
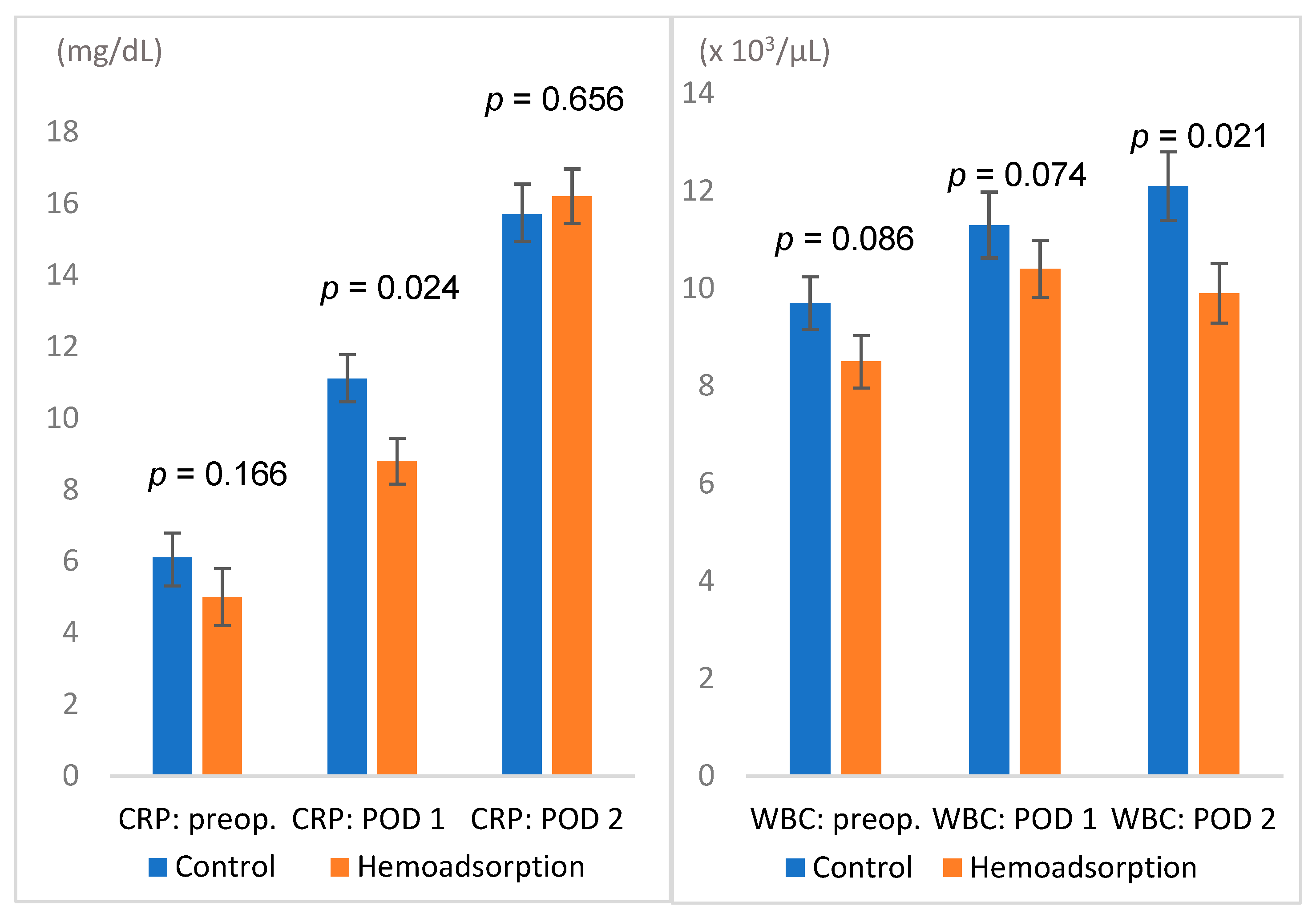
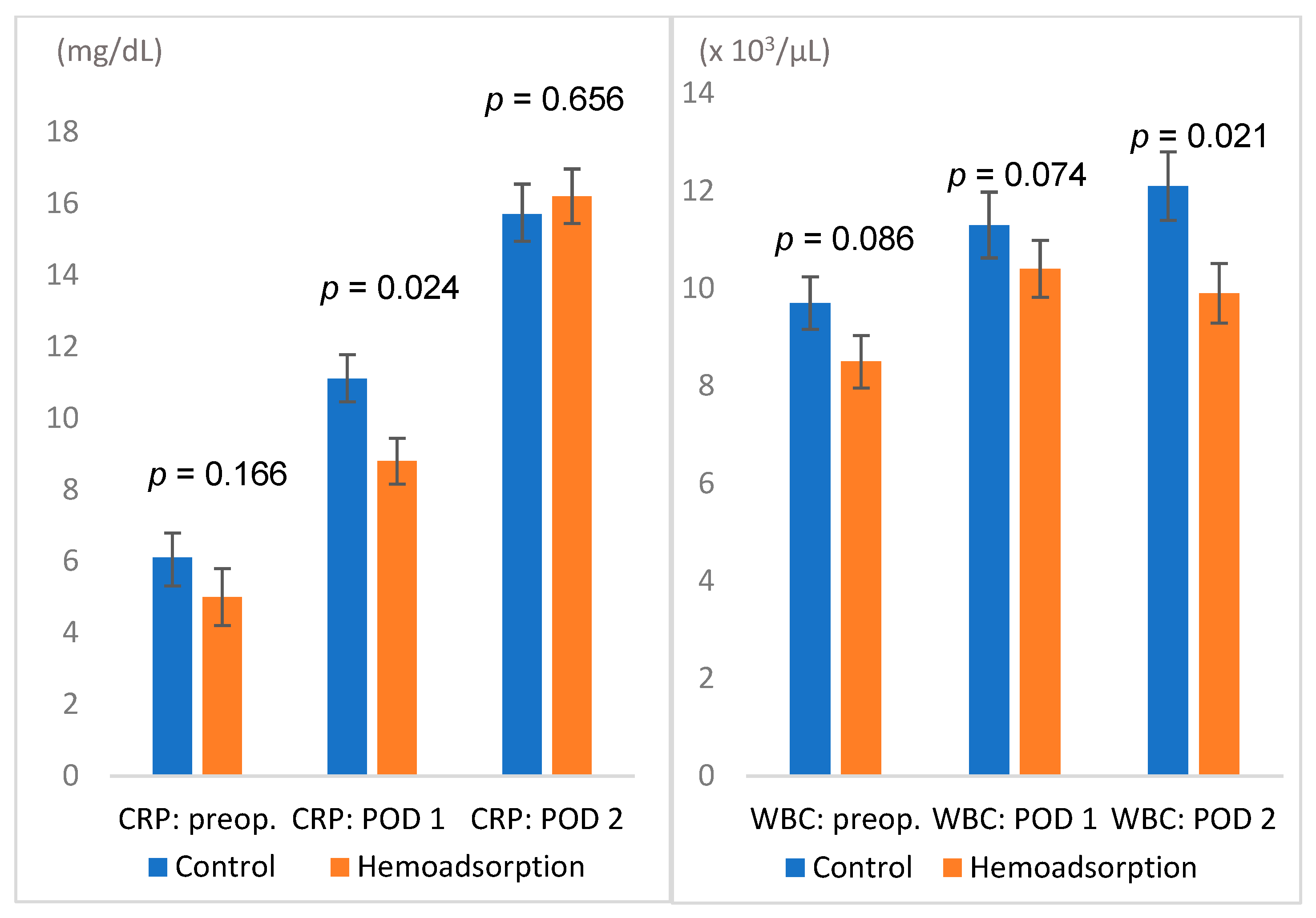
| CRP (mg/dL) preop. | 6 [3;10.9] | 5 [2;10.3] | 0.166 | 6.1 [3.00;11.0] | 5.0 [2.0;10.3] | 0.146 |
| Platelets (×103/µL) preop. | 236 [160;307] | 238 [171;300] | 0.920 | 237 [157;314] | 238 [171;300] | 0.983 |
| WBC (×103/µL) preop. | 9.7 [7.3;14.1] | 8.5 [6.2;12.5] | 0.077 | 9.30 [7.25;14.4] | 8.50 [6.2;12.5] | 0.086 |
| Hb (g/dL) preop. | 10.2 [9.1;11.4] | 10.1 [9.1;11.5] | 0.836 | 10.3 [9.15;11.5] | 10.1 [9.1;11.5] | 0.999 |
| Lactate (mmol/l) at start of surgery | 0.8 [0.6;1.1] | 0.7 [0.5;1] | 0.183 | 0.80 [0.60;1.10] | 0.70 [0.5;1.0] | 0.199 |
| Echocardiographic/Radiologic Characteristics | ||||||
| LV-EF lower than 50% | 29 (28.2%) | 23 (23.2%) | 0.523 | 25 (25.3%) | 23 (23.2%) | 0.868 |
| Vegetations | 98 (95.1%) | 94 (94.9%) | 1.000 | 94 (94.9%) | 94 (94.9%) | 1.000 |
| Paravalvular extension or abscess | 37 (35.9%) | 44 (44.4%) | 0.275 | 36 (36.4%) | 44 (44.4%) | 0.311 |
| Concomitant right-sided endocarditis | 5 (4.9%) | 2 (2.1%) | 0.446 | 5 (5.05%) | 2 (2.1%) | 0.445 |
| Causative infective agent | ||||||
| Staphylococcus spec. | 40 (38.8%) | 31 (32.0%) | 0.385 | 40 (40.4%) | 31 (32.0%) | 0.280 |
| Staphylococcus aureus | 26 (26%) | 19 (21.3%) | 0.563 | 26 (27.1%) | 19 (21.3%) | 0.461 |
| Streptococcus species | 29 (29%) | 18 (20.2%) | 0.221 | 26 (27.1%) | 18 (20.2%) | 0.357 |
| Enterococcus faecalis | 13 (13%) | 15 (16.9%) | 0.590 | 13 (13.5%) | 15 (16.9%) | 0.672 |
| Gram-bacteria | 5 (4.9%) | 5 (5.1%) | 1.000 | 5 (5.10%) | 5 (5.1%) | 1.000 |
| Antibiotic therapy (d) preop. | 6 [2;11] | 5 [3;10.8] | 0.702 | 6 [2;11] | 5 [3;11] | 0.850 |
| Intraoperative Data | ||||||
|---|---|---|---|---|---|---|
| Unadjusted | Propensity Score Match | |||||
| Control (n = 103) | Hemoadsorption (n = 99) | p Value | Control (n = 99) | Hemoadsorption (n = 99) | p Value | |
| Time: diagnosis and surgery (d) | 4 [2;8.3] | 4 [2;9.8] | 0.697 | 4.00 [2.0;7.3] | 4.00 [2.0;9.8] | 0.546 |
| Re-operation | 43 (41.8%) | 46 (46.5%) | 0.769 | 43 (43.4%) | 46 (46.5%) | 0.891 |
| Cardiopulmonary Bypass (min) | 126 [93.0;168] | 134 [108;176] | 0.212 | 126 [93.0;168] | 134 [108;176] | 0.204 |
| Aortic cross-clamp (min) | 82 [59;116] | 91 [72.5;131] | 0.063 | 82.0 [58.0;114] | 91.0 [72.5;131] | 0.058 |
| Selective cerebral perfusion | 2 (1.9%) | 4 (4%) | 0.661 | 2 (2%) | 4 (4%) | 0.697 |
| Isolated aortic valve surgery | 56 (54.4%) | 46 (46.5%) | 0.601 | 56 (56.6%) | 46 (46.5%) | 0.833 |
| Aortic bioprosthesis | 56 (54.4%) | 50 (50.5%) | 0.852 | 50 (50.5%) | 46 (46.5%) | 0.833 |
| Aortic mechanical prosthesis | 8 (7.8%) | 9 (9.1%) | 0.953 | 8 (8.1%) | 9 (9.1%) | 1.000 |
| Complex aortic surgery | 14 (13.6%) | 23 (23.2%) | 0.196 | 10 (10.1%) | 23 (23.2%) | 0.056 |
| Aortic and mitral valve surgery | 9 (8.7%) | 12 (12.1%) | 0.631 | 14 (14.3%) | 8 (8.1%) | 0.248 |
| Isolated mitral valve surgery | 29 (28.2%) | 27 (27.3%) | 1.000 | 25 (25.3%) | 28 (28.3%) | 0.748 |
| Mitral bioprosthesis | 25 (24.3%) | 26 (26.3%) | 0.925 | 21 (21.2%) | 22 (22.2%) | 1.000 |
| Mitral mechanical prosthesis | 8 (7.8%) | 7 (7.1%) | 1.000 | 8 (8.1%) | 7 (7.1%) | 1.000 |
| Mitral valve reconstruction | 5 (4.9%) | 6 (6.1%) | 0.962 | 8 (8.1%) | 5 (5.1%) | 1.000 |
| Concomitant tricuspid valve surgery | 4 (3.9%) | 6 (6.1%) | 0.533 | 4 (4.08%) | 6 (6.1%) | 0.747 |
| Concomitant revascularization | 14 (14.0%) | 14 (14.6%) | 1.000 | 12 (12.1%) | 14 (14.1%) | 0.833 |
| Pericardial patch reconstruction | 36 (35.6%) | 36 (36.4%) | 1.000 | 36 (37.1%) | 36 (36.4%) | 1.000 |
| Postoperative Outcomes | ||||||
|---|---|---|---|---|---|---|
| Unadjusted Data | Propensity Score Matched Data | |||||
| Control (n = 103) | Hemoadsorption (n = 99) | p Value | Control (n = 99) | Hemoadsorption (n = 99) | p Value | |
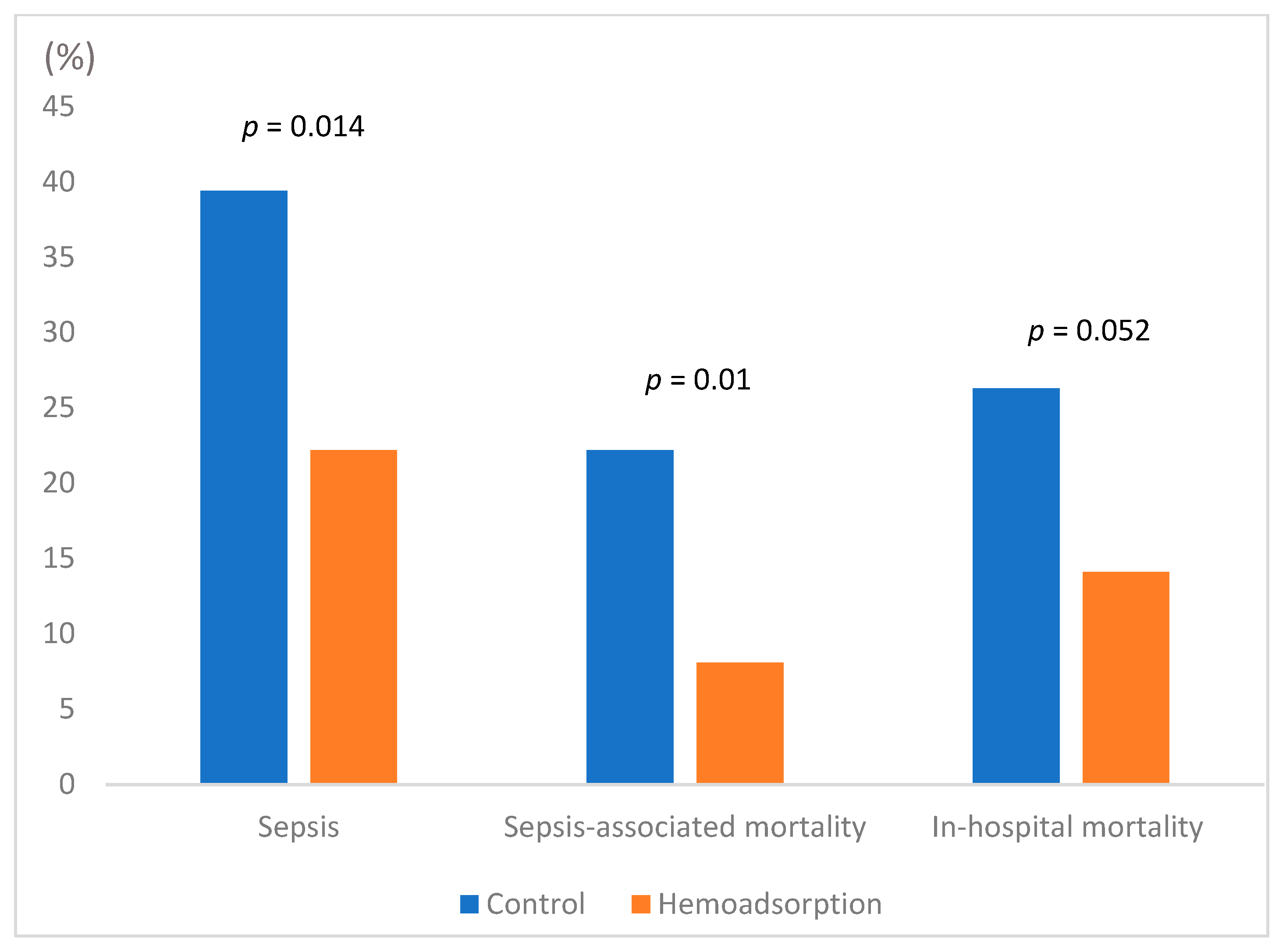
| Sepsis postop. | 39 (37.9%) | 22 (22.2%) | 0.023 | 39 (39.4%) | 22 (22.2%) | 0.014 |
| Sepsis-associated mortality | 22 (21.4%) | 8 (8.1%) | 0.014 | 22 (22.2%) | 8 (8.1%) | 0.010 |
| In-hospital mortality | 26 (25.2%) | 14 (14.1%) | 0.071 | 26 (26.3%) | 14 (14.1%) | 0.052 |
| Re-thoracotomy for bleeding | 17 (16.7%) | 10 (10.2%) | 0.258 | 17 (17.3%) | 10 (10.2%) | 0.214 |
| Mechanical ventilation (h) | 22 [8, 68.2] | 19.0 [10, 65.5] | 0.856 | 22.0 [7.25, 72.0] | 19.0 [10.0, 65.5] | 0.813 |
| Chest tube output (ml) 24 h postop. | 500 [300, 700] | 500 [250, 950] | 0.761 | 500 [300, 700] | 500 [250, 950] | 0.794 |
| New RRT postop. | 25 (24.3%) | 19 (19.2%) | 0.481 | 24 (24.2%) | 19 (19.2%) | 0.491 |
| Central neurological complications | 2 (1.9%) | 8 (8.1%) | 0.055 | 2 (2.02%) | 8 (8.1%) | 0.105 |
| Pneumonia | 10 (9.7%) | 6 (6.1%) | 0.484 | 10 (10.1%) | 6 (6.1%) | 0.434 |
| Deep Sternal Wound Infection | 1 (1.0%) | 0 | 1.000 | 1 (1.01%) | 0 (0.0%) | 1.000 |
| UTI | 2 (1.9%) | 1 (1.0%) | 1.000 | 2 (2.02%) | 1 (1.0%) | 1.000 |
| Cumulative inotropes (mg) POD1 | 12.6 [4.9, 40.1] | 17.8 [7.8, 37.2] | 0.204 | 12.6 [4.85, 40.1] | 17.8 [7.8, 37.2] | 0.227 |
| Cumulative inotropes (mg) POD2 | 5.8 [0.9, 15.2] | 4.9 [1.1, 16.9] | 0.927 | 5.82 [0.86, 16.2] | 4.93 [1.1, 16.9] | 0.877 |
| Lactate (mmol/L) at the end of Surgery | 1.3 [1, 1.7] | 1.2 [0.9, 1.8] | 0.656 | 1.30 [1.00, 1.70] | 1.20 [0., 1.80] | 0.652 |
| Lactate (mmol/L) POD1 | 1.20 [0.90, 1.60] | 1.30 [0.92, 1.75] | 0.191 | 1.20 [0.90, 1.60] | 1.30 [0.9, 1.8] | 0.148 |
| Lactate (mmol/L) POD2 | 1 [0.7, 1.2] | 1 [0.8, 1.3] | 0.142 | 1 [0.7, 1.2] | 1 [0.8, 1.3] | 0.191 |
| WBC (×103/µL) POD1 | 11.4 [9.10, 17.1] | 10.4 [8.10, 15.6] | 0.065 | 11.3 [9.05, 17.1] | 10.4 [8.1, 15.6] | 0.074 |
| WBC (×103/µL) POD2 | 12.1 [8.75, 15.1] | 9.90 [7.40, 14.2] | 0.025 | 12.1 [8.90, 15.3] | 9.90 [7.4, 14.2] | 0.021 |
| CRP (mg/dL) POD1 | 10.0 [7.2, 15.4] | 8.80 [5.0, 12.9] | 0.026 | 11.1 [7.0, 15.8] | 8.8 [5.0, 12.9] | 0.024 |
| CRP (mg/dL) POD2 | 15.4 [11.5, 21.8] | 16.2 [11, 20.6] | 0.824 | 15.7 [11.5, 22.3] | 16.2 [11, 20.6] | 0.656 |
| Hb (g/dL) POD1 | 9.20 [8.4, 9.9] | 9.70 [8.7, 10.3] | 0.011 | 9.2 [8.4, 9.9 | 9.70 [8.7, 10.3] | 0.012 |
| Hb (g/dL) POD2 | 8.75 [8.1, 9.3] | 8.90 [8.4, 9.6] | 0.166 | 8.8 [8.1, 9.3] | 8.90 [8.4, 9.6] | 0.200 |
| Platelets transfused (Units) | 0 [0, 2] | 0 [0, 1] | 0.719 | 0 [0, 1.5] | 0 [0, 1] | 0.801 |
| RBCs transfused | 3.0 [1.0, 6.0] | 1.0 [0.0, 4.0] | 0.016 | 3.0 [1.0, 6.0] | 1.0 [0.0, 4.0] | 0.016 |
| FFPs transfused | 0.0 [0.0, 4.00] | 0.0 [00, 6.00] | 0.014 | 0.0 [0.0, 4.0] | 0.0 [0.0, 6.0] | 0.023 |
| Intensive Care Unit stay (d) | 3 [2, 6] | 4 [2, 8.5] | 0.189 | 3 [2, 6] | 4 [2, 8.5] | 0.238 |
| Hospital stay (d) | 34.5 [24, 46] | 39 [22, 49.2] | 0.312 | 33.5 [24, 46] | 39 [22, 49] | 0.282 |
| Variables Related to Sepsis (Matched Cohort) | ||||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| Variable | OR (ClL, CLU) | p Value | OR (ClL, CLU) | p Value |
| BMI (m2/kg) | 1.098 (1.026, 1.174) | 0.007 | ||
| Hemoadsorption | 0.308 (0.130, 0.730) | 0.008 | 0.42 (0.16, 1.07) | 0.07 |
| Euroscore II | 1.022 (1.003, 1.041) | 0.024 | ||
| Cardiogenic shock in last 48 h | 6.125 (2.616, 14.339) | <0.001 | ||
| Ventilated preop. | 3.326 (1.214, 9.110) | 0.019 | ||
| Staphylococcus spec. | 2.506 (1.126, 5.577) | 0.024 | 2.65 (1.04, 6.75) | 0.041 |
| CRP preop. | 1.104 (1.054, 1.158) | <0.001 | ||
| WBC preop. | 1.18 (1.046, 1.196) | 0.001 | ||
| Lactate preop. | 1.878 (1.114, 3.165) | 0.018 | ||
| Inotropes preop. | 7.266 (2.933, 18.002) | <0.001 | ||
| CPB duration | 1.006 (1.001, 1.011) | 0.011 | ||
| Aortic cros-clamp | 1.007 (1.000, 1.014) | 0.046 | ||
| Lactate end of surgery | 2.207 (1.519, 3.209) | <0.001 | ||
| Inotropes cumulative POD 1 | 1.047 (1.031, 1.065) | <0.001 | ||
| Inotropes cumulative POD2 | 1.05 (1.030, 1.071) | <0.001 | ||
| WBC POD1 | 1.222 (1.131, 1.320) | <0.001 | ||
| WBC POD2 | 1.258 (1.155, 1.370) | <0.001 | 1.28 (1.15, 1.43) | <0.001 |
| Lactate 24 h postop. | 2.644 (1.650, 4.236) | <0.001 | ||
| c-TnT POD1 | 1.351 (1.162, 1.572) | <0.001 | ||
| CK-MB POD 1 | 1.01 (1.004, 1.016) | <0.001 | ||
| CRP POD 1 | 1.088 (1.025, 1.156) | 0.006 | ||
| CRP POD2 | 1.056 (0.998, 1.116) | 0.059 | 1.07 (1.01, 1.14) | 0.021 |
| New RRT postop. | 7.142 (3.101, 16.452) | <0.001 | 4.93 (1.70, 14.26) | 0.003 |
| IABP postop. | 6.308 (1.485, 26.792) | 0.013 | ||
| FFPs transfused | 1.088 (1.020, 1.161) | 0.011 | ||
| Variables Related to Sepsis-Associated Mortality (Matched Cohort) | ||||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| Variable | OR (ClL, CLU) | p Value | OR (ClL, CLU) | p Value |
| BMI | 1.098 (1.026, 1.174) | 0.007 | ||
| Hemoadsorption | 0.308 (0.130, 0.730) | 0.008 | 0.09 (0.01, 0.62) | 0.014 |
| EuroScore II | 1.022 (1.003, 1.041) | 0.024 | ||
| Staphylococcus spec. | 2.506 (1.126, 5.577) | 0.024 | ||
| Inotropes preop. | 7.266 (2.933, 18.002) | <0.001 | ||
| CRP preop. | 1.104 (1.054, 1.158) | <0.001 | ||
| Cardiogenic shock in the last 48 h | 6.125 (2.616, 14.339) | <0.001 | ||
| Ventilated preop. | 3.326 (1.214, 9.110) | 0.019 | ||
| WBC preop. | 1.118 (1.046, 1.196) | 0.001 | ||
| Lactate: start of surgery | 1.878 (1.114, 3.165) | 0.018 | ||
| Concomitant tricuspid valve surgery | 4.32 (1.139, 16.390) | 0.031 | ||
| CPB duration (min.) | 1.006 (1.001, 1.011) | 0.011 | ||
| Aortic cross-clamp (min.) | 1.007 (1.000, 1.014) | 0.046 | ||
| Paravalvular extension or Abscess | 2.179 (0.992, 4.787) | 0.052 | 4.18 (0.73,23.99) | 0.109 |
| Lactate (mmol/L) end of surgery | 2.207 (1.519, 3.209) | <0.001 | ||
| WBC POD1 | 1.222 (1.131, 1.320) | <0.001 | ||
| WBC POD2 | 1.258 (1.155, 1.370) | <0.001 | 1.21 (1.06, 1.38) | 0.006 |
| Lactate at 24 h postop. | 2.644 (1.650, 4.236) | <0.001 | ||
| Inotropes cumulative POD1 | 1.047 (1.030, 1.064) | <0.001 | 1.03 (0.99, 1.06) | 0.068 |
| Inotropes cumulative POD2 | 1.005 (1.002, 1.007) | <0.001 | 1.01 (1.00, 1.01) | 0.015 |
| CRP POD 1 | 1.088 (1.025, 1.156) | 0.006 | 1.15 (1.02, 1.31) | 0.024 |
| CRP POD 2 | 1.056 (0.998, 1.116) | 0.059 | ||
| c-TnT POD 1 | 1.351 (1.162, 1.572) | <0.001 | ||
| CK-MB POD 1 | 1.01 (1.004, 1.016) | 0.001 | ||
| New RRT postop. | 7.142 (3.101, 16.452) | <0.001 | 8.16 (1.49, 44.37) | 0.015 |
| FFPs transfused | 1.088 (1.020, 1.161) | 0.011 | ||
| IABP postop. | 6.308 (1.485, 26.792) | 0.013 | ||
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Variable | OR (ClL, CLU) | p Value | OR (ClL, CLU) | p Value |
| BMI | 1.068 (1.005, 1.135) | 0.034 | ||
| Hemoadsorption therapy | 0.462 (0.225, 0.951) | 0.036 | 0.07 (0.01, 0.79) | 0.032 |
| Staphylococcus spec. | 2.497 (1.223, 5.096) | 0.012 | ||
| Endocarditis of 2 or more valves | 2.654 (1.025, 6.873) | 0.044 | ||
| Cardiogenic chock in the last 48 h | 6.786 (3.047, 15.114) | <0.001 | ||
| Inotropes preop. | 6.362 (2.932, 13.801) | <0.001 | 17.36 (1.77, 170.13) | 0.014 |
| Preop Lactate | 2.147 (1.252, 3.679) | 0.005 | ||
| Ventilated preop. | 5.576 (2.168, 14.338) | <0.001 | ||
| WBC preop. | 1.129 (1.058, 1.204) | <0.001 | ||
| CRP preop. | 1.082 (1.036, 1.130) | <0.001 | ||
| CPB duration | 1.006 (1.002, 1.011) | 0.008 | ||
| Aortic cross-clamp | 1.007 (1.001, 1.014) | 0.026 | ||
| Lactate end of surgery | 2.637 (1.761, 3.948) | <0.001 | ||
| Lactate 24 h postop. | 2.754 (1.712, 4.432) | <0.001 | 4.14 (1.01, 17.01) | 0.049 |
| WBC POD1 | 1.173 (1.100,1.252) | <0.001 | ||
| Inotropes cumulative POD1 | 1.053 (1.035, 1.071) | <0.001 | ||
| Inotropes cumulative POD2 | 1.048 (1.028, 1.069) | <0.001 | 1.02 (1.00, 1.04) | 0.024 |
| WBC POD2 | 1.202 (1.120, 1.289) | <0.001 | ||
| c-TnT POD 1 | 1.365 (1.168, 1.595) | <0.001 | ||
| CK-MB POD 1 | 1.009 (1.003, 1.015) | 0.003 | ||
| eGFRCKD-EPI preop. | 0.984 (0.971, 0.998) | 0.022 | ||
| New RRT postop. | 6.833 (3.174, 14.709) | <0.001 | 14.10 (1.57, 126.67) | 0.018 |
| FFPs transfused | 1.151 (1.076, 1.230) | <0.001 | ||
| RBCs transfused | 1.085 (1.025, 1.149) | 0.005 | 0.9 (0.78, 1.03) | 0.123 |
| Drainage Output (ml) in 24 h | 1.001 (1.000, 1.001) | 0.004 | 1.004 (1.001, 1.006) | 0.002 |
| IABP postop. | 4.278 (1.021, 17.922) | 0.047 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalisnik, J.M.; Leiler, S.; Mamdooh, H.; Zibert, J.; Bertsch, T.; Vogt, F.A.; Bagaev, E.; Fittkau, M.; Fischlein, T. Single-Centre Retrospective Evaluation of Intraoperative Hemoadsorption in Left-Sided Acute Infective Endocarditis. J. Clin. Med. 2022, 11, 3954. https://doi.org/10.3390/jcm11143954
Kalisnik JM, Leiler S, Mamdooh H, Zibert J, Bertsch T, Vogt FA, Bagaev E, Fittkau M, Fischlein T. Single-Centre Retrospective Evaluation of Intraoperative Hemoadsorption in Left-Sided Acute Infective Endocarditis. Journal of Clinical Medicine. 2022; 11(14):3954. https://doi.org/10.3390/jcm11143954
Chicago/Turabian StyleKalisnik, Jurij Matija, Spela Leiler, Hazem Mamdooh, Janez Zibert, Thomas Bertsch, Ferdinand Aurel Vogt, Erik Bagaev, Matthias Fittkau, and Theodor Fischlein. 2022. "Single-Centre Retrospective Evaluation of Intraoperative Hemoadsorption in Left-Sided Acute Infective Endocarditis" Journal of Clinical Medicine 11, no. 14: 3954. https://doi.org/10.3390/jcm11143954
APA StyleKalisnik, J. M., Leiler, S., Mamdooh, H., Zibert, J., Bertsch, T., Vogt, F. A., Bagaev, E., Fittkau, M., & Fischlein, T. (2022). Single-Centre Retrospective Evaluation of Intraoperative Hemoadsorption in Left-Sided Acute Infective Endocarditis. Journal of Clinical Medicine, 11(14), 3954. https://doi.org/10.3390/jcm11143954