
Axillary Web Syndrome in Breast Cancer Women: What Is the Optimal Rehabilitation Strategy after Surgery? A Systematic Review

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
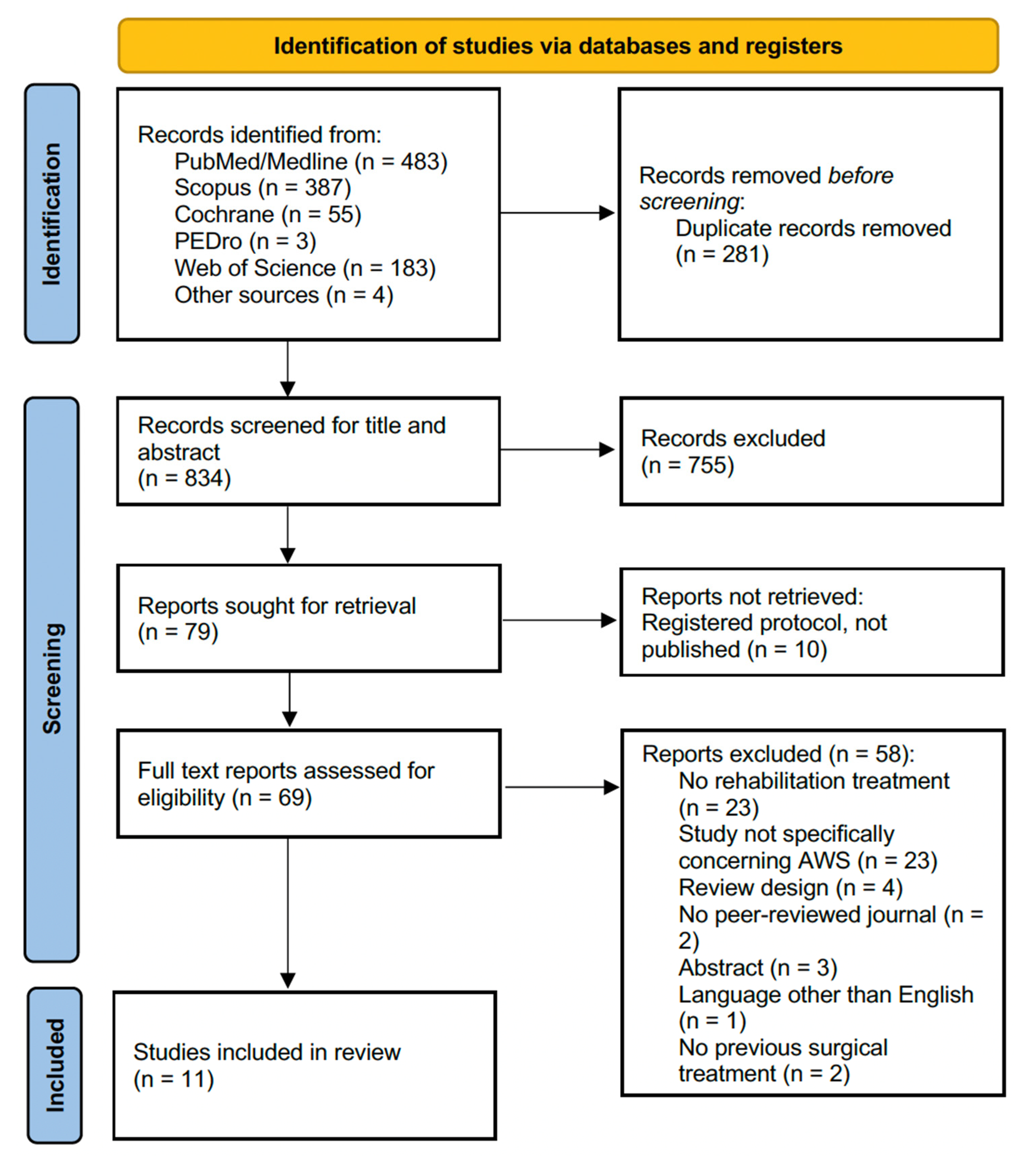
2.1. Search Strategy
2.2. Selection Criteria
- -
- (P) Participants: Adult women suffering from AWS after breast cancer surgery. Studies assessing patients with a diagnosis of AWS by clinical examination or ultrasound assessment were included (without restrictions in terms of AWS diagnosis).
- -
- Intervention: Rehabilitation treatment (education, physiotherapy, therapeutic exercise, myofascial relaxation techniques, scar treatment, manual lymphatic drainage (MLD), and physical therapies). We did not include studies involving pharmacological therapy in AWS management unless it was combined with rehabilitation treatment.
- -
- (C) Comparator: any comparator, including placebo, pharmacological treatment, non-pharmacological treatment, or no treatment.
- -
- (O) Outcome: The primary outcome was self-reported pain. The secondary outcomes were AWS resolution of the clinical presentation, upper limb function, and HR-QoL.
2.3. Data Extraction and Synthesis
2.4. Quality Assessment
3. Results
3.1. Quality Assessment
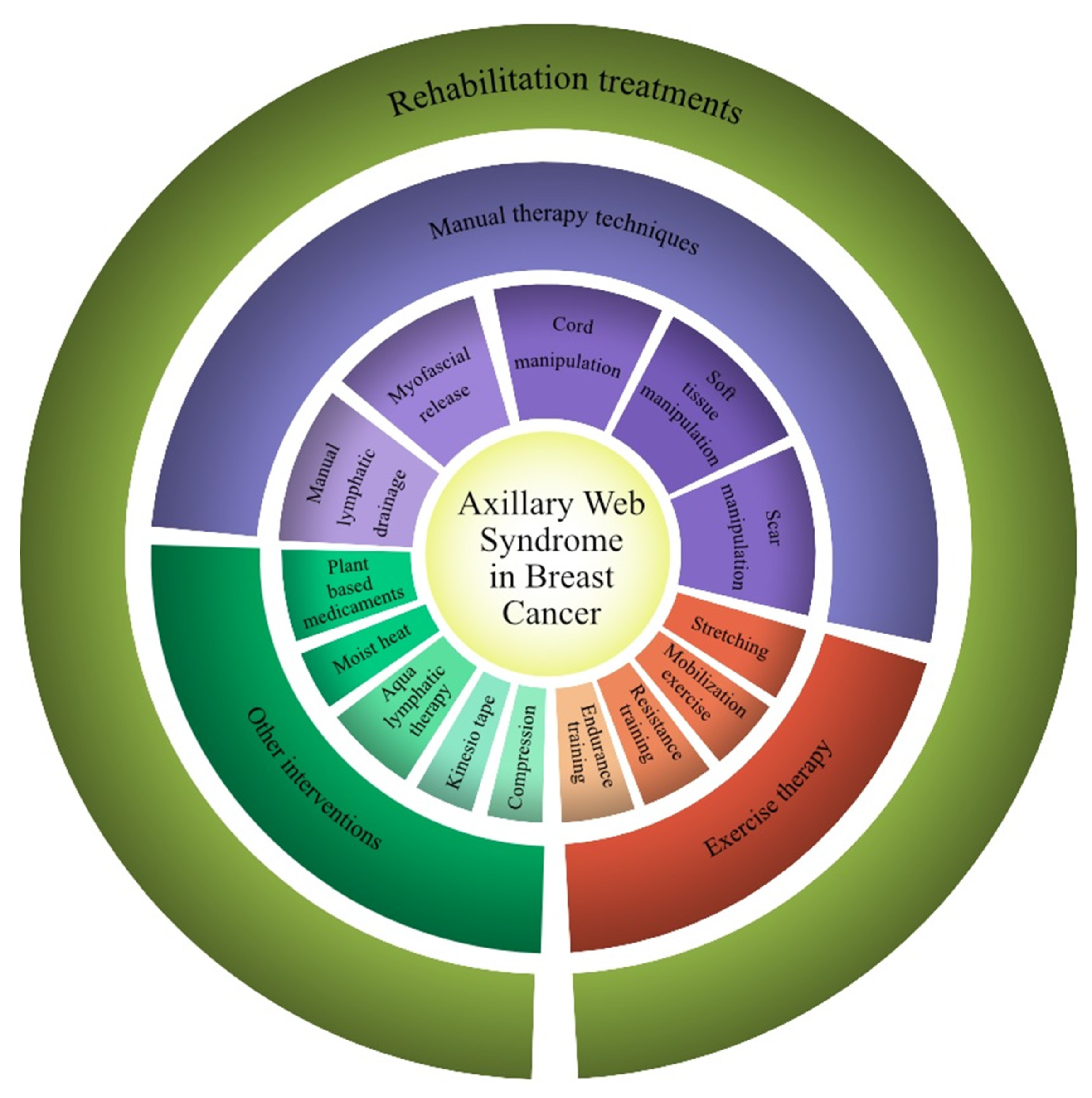
3.2. Rehabilitation Therapy Interventions
3.3. Main Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iacoviello, L.; Bonaccio, M.; de Gaetano, G.; Donati, M.B. Epidemiology of breast cancer, a paradigm of the “common soil” hypothesis. Semin. Cancer Biol. 2020, 72, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Lima, S.M.; Kehm, R.D.; Terry, M.B. Global breast cancer incidence and mortality trends by region, age-groups, and fertility patterns. eClinicalMedicine 2021, 38, 100985. [Google Scholar] [CrossRef]
- Invernizzi, M.; Kim, J.; Fusco, N. Editorial: Quality of Life in Breast Cancer Patients and Survivors. Front. Oncol. 2020, 10, 620574. [Google Scholar] [CrossRef]
- Arnaboldi, P.; Riva, S.; Crico, C.; Pravettoni, G. A systematic literature review exploring the prevalence of post-traumatic stress disorder and the role played by stress and traumatic stress in breast cancer diagnosis and trajectory. Breast Cancer Targets Ther. 2017, 9, 473–485. [Google Scholar] [CrossRef]
- Invernizzi, M.; Corti, C.; Lopez, G.; Michelotti, A.; Despini, L.; Gambini, D.; Lorenzini, D.; Guerini-Rocco, E.; Maggi, S.; Noale, M.; et al. Lymphovascular invasion and extranodal tumour extension are risk indicators of breast cancer related lymphoedema: An observational retrospective study with long-term follow-up. BMC Cancer 2018, 18, 935. [Google Scholar] [CrossRef]
- Invernizzi, M.; de Sire, A.; Lippi, L.; Venetis, K.; Sajjadi, E.; Gimigliano, F.; Gennari, A.; Criscitiello, C.; Cisari, C.; Fusco, N. Impact of Rehabilitation on Breast Cancer Related Fatigue: A Pilot Study. Front. Oncol. 2020, 10, 556718. [Google Scholar] [CrossRef]
- Yang, S.; Chu, S.; Gao, Y.; Ai, Q.; Liu, Y.; Li, X.; Chen, N. A Narrative Review of Cancer-Related Fatigue (CRF) and Its Possible Pathogenesis. Cells 2019, 8, 738. [Google Scholar] [CrossRef]
- de Sire, A.; Lippi, L.; Ammendolia, A.; Cisari, C.; Venetis, K.; Sajjadi, E.; Fusco, N.; Invernizzi, M. Physical Exercise with or without Whole-Body Vibration in Breast Cancer Patients Suffering from Aromatase Inhibitor—Induced Musculoskeletal Symptoms: A Pilot Randomized Clinical Study. J. Pers. Med. 2021, 11, 1369. [Google Scholar] [CrossRef]
- de Sire, A.; Lippi, L.; Venetis, K.; Morganti, S.; Sajjadi, E.; Curci, C.; Ammendolia, A.; Criscitiello, C.; Fusco, N.; Invernizzi, M. Efficacy of Antiresorptive Drugs on Bone Mineral Density in Post-Menopausal Women With Early Breast Cancer Receiving Adjuvant Aromatase Inhibitors: A Systematic Review of Randomized Controlled Trials. Front. Oncol. 2022, 11, 829875. [Google Scholar] [CrossRef]
- Park, S.B.; Tamburin, S.; Schenone, A.; Kleckner, I.R.; Velasco, R.; Alberti, P.; Kanzawa-Lee, G.; Lustberg, M.; Dorsey, S.G.; Mantovani, E.; et al. Optimal outcome measures for assessing exercise and rehabilitation approaches in chemotherapy-induced peripheral-neurotoxicity: Systematic review and consensus expert opinion. Expert Rev. Neurother. 2022, 22, 65–76. [Google Scholar] [CrossRef]
- Moskovitz, A.H.; Anderson, B.O.; Yeung, R.S.; Byrd, D.R.; Lawton, T.J.; Moe, R.E. Axillary web syndrome after axillary dissection. Am. J. Surg. 2001, 181, 434–439. [Google Scholar] [CrossRef]
- de Sire, A.; Invernizzi, M.; Lippi, L.; Cisari, C.; Özçakar, L.; Franchignoni, F. Blurred lines between axillary web syndrome and Mondor’s disease after breast cancer surgery: A case report. Ann. Phys. Rehabil. Med. 2019, 63, 365–367. [Google Scholar] [CrossRef]
- Yeung, W.M.; McPhail, S.; Kuys, S.S. A systematic review of axillary web syndrome (AWS). J. Cancer Surviv. 2015, 9, 576–598. [Google Scholar] [CrossRef]
- Figueira, P.V.; Haddad, C.A.; Rizzi, S.K.; Facina, G.; Nazario, A.C. Diagnosis of Axillary Web Syndrome in Patients After Breast Cancer Surgery. Am. J. Clin. Oncol. 2018, 41, 992–996. [Google Scholar] [CrossRef]
- Koehler, L.A.; Hunter, D.W.; Blaes, A.H.; Haddad, T.C. Function, Shoulder Motion, Pain, and Lymphedema in Breast Cancer With and Without Axillary Web Syndrome: An 18-Month Follow-Up. Phys. Ther. 2018, 98, 518–527. [Google Scholar] [CrossRef]
- Dinas, K.; Kalder, M.; Zepiridis, L.; Mavromatidis, G.; Pratilas, G. Axillary web syndrome: Incidence, pathogenesis, and management. Curr. Probl. Cancer 2019, 43, 100470. [Google Scholar] [CrossRef]
- LeDuc, O.; Sichere, M.; Moreau, A.; Rigolet, J.; Tinlot, A.; Darc, S.; Wilputte, F.; Strapart, J.; Parijs, T.; Clément, A.; et al. Axillary web syndrome: Nature and localization. Lymphology 2009, 42, 176–181. [Google Scholar]
- Jeong, S.; Song, B.J.; Rhu, J.; Kim, C.; Im, S.; Park, G.-Y. A Risk Factor Analysis of Axillary Web Syndrome in Patients After Breast Cancer Surgery: A Single Center Study in Korea. Ann. Rehabil. Med. 2021, 45, 401–409. [Google Scholar] [CrossRef]
- Harris, S.R. Axillary Web Syndrome in Breast Cancer: A Prevalent But Under-Recognized Postoperative Complication. Breast Care 2018, 13, 129–132. [Google Scholar] [CrossRef]
- Marcasciano, M.; Kaciulyte, J.; Mori, F.L.R.; Lo Torto, F.; Barellini, L.; Loreti, A.; Fanelli, B.; De Vita, R.; Redi, U.; Marcasciano, F.; et al. Breast surgeons updating on the thresholds of COVID-19 era: Results of a multicenter collaborative study evaluating the role of online videos and multimedia sources on breast surgeons education and training. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7845–7854. [Google Scholar] [CrossRef]
- Koehler, L.A.; Blaes, A.H.; Haddad, T.C.; Hunter, D.W.; Hirsch, A.T.; Ludewig, P.M. Movement, Function, Pain, and Postoperative Edema in Axillary Web Syndrome. Phys. Ther. 2015, 95, 1345–1353. [Google Scholar] [CrossRef]
- O’Toole, J.; Miller, C.L.; Specht, M.C.; Skolny, M.N.; Jammallo, L.S.; Horick, N.; Elliott, K.; Niemierko, A.; Taghian, A.G. Cording following treatment for breast cancer. Breast Cancer Res. Treat. 2013, 140, 105–111. [Google Scholar] [CrossRef]
- Wernicke, A.G.; Shamis, M.; Sidhu, K.K.; Turner, B.C.; Goltser, Y.; Khan, I.; Christos, P.J.; Komarnicky-Kocher, L.T. Complication Rates in Patients With Negative Axillary Nodes 10 Years After Local Breast Radiotherapy After Either Sentinel Lymph Node Dissection or Axillary Clearance. Am. J. Clin. Oncol. 2013, 36, 12–19. [Google Scholar] [CrossRef]
- de Sire, A.; Losco, L.; Cisari, C.; Gennari, A.; Boldorini, R.; Fusco, N.; Cigna, E.; Invernizzi, M. Axillary web syndrome in women after breast cancer surgery referred to an Oncological Rehabilitation Unit: Which are the main risk factors? A retrospective case-control study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 8028–8035. [Google Scholar] [CrossRef]
- Agostini, F.; Attanasi, C.; Bernetti, A.; Mangone, M.; Paoloni, M.; del Monte, E.; Mammucari, M.; Maggiori, E.; Russo, D.; Di Marzo, R.; et al. Web Axillary Pain Syndrome—Literature Evidence and Novel Rehabilitative Suggestions: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 10383. [Google Scholar] [CrossRef]
- Torres-Lacomba, M.; Prieto-Gómez, V.; Martín, B.-A.; Ferrandez, J.C.; Yuste-Sánchez, M.J.; Navarro-Brazález, B.; Romay-Barrero, H. Manual Lymph Drainage with Progressive Arm Exercises for Axillary Web Syndrome after Breast Cancer Surgery: A Randomized Controlled Trial. Phys. Ther. 2022, 102, pzab314. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a knowledge representation for clinical questions. In AMIA Annual Symposium Proceedings; American Medical Informatics Association: Rockville, MD, USA, 2006; pp. 359–363. [Google Scholar]
- Joanna Briggs Institute Critical Appraisal Checklist for Quasi-Experimental Studies (Non-Randomized Experimental Studies) Checklist. Available online: https://jbi.global/sites/default/files/2019-05/JBI_Quasi-Experimental_Appraisal_Tool2017_0.pdf (accessed on 27 April 2022).
- Cho, Y.; Do, J.; Jung, S.; Kwon, O.; Jeon, J.Y. Effects of a physical therapy program combined with manual lymphatic drainage on shoulder function, quality of life, lymphedema incidence, and pain in breast cancer patients with axillary web syndrome following axillary dissection. Support. Care Cancer 2015, 24, 2047–2057. [Google Scholar] [CrossRef]
- Ibrahim, R.G.A.E.N.; Khalaf, M.M.A.; Elkerm, Y.M.; El Safwany, M.M. Effect of Direct Myofascial Release and Kinesio Tape on Axillary Web Syndrome. J. Med Sci. 2017, 18, 1–10. [Google Scholar] [CrossRef][Green Version]
- Moreau, A.; Leduc, O.; Tinlot, A.; Clement, A.; Parijs, T.; Strappaert, J.; Beckers, F.; Pastouret, F.; Leduc, A. Axillary Web Syndrome (AWS): Its features and the physical treatment plan of care. Eur. J. Lymphology Relat. Probl. 2010, 21, 25–28. [Google Scholar]
- Wyrick, S.L.; Waltke, L.J.; Ng, A.V. Physical Therapy may Promote Resolution of Lymphatic Coding in Breast Cancer Survivors. Rehabil. Oncol. 2006, 24, 29–34. [Google Scholar] [CrossRef]
- Lattanzi, J.B.; Zimmerman, A.; Marshall, L.M. Case Report of Axillary Web Syndrome. Rehabil. Oncol. 2012, 30, 18–21. [Google Scholar] [CrossRef]
- Fourie, W.; Robb, K. Physiotherapy management of axillary web syndrome following breast cancer treatment: Discussing the use of soft tissue techniques. Physiotherapy 2009, 95, 314–320. [Google Scholar] [CrossRef]
- Wei, P.; Zhu, L.; Chen, K.; Jia, W.; Hu, Y.; Su, F. Axillary web syndrome following secondary breast-conserving surgery: A case report. World J. Surg. Oncol. 2013, 11, 8. [Google Scholar] [CrossRef]
- Tilley, A.; Thomas-Maclean, R.; Kwan, W. Lymphatic cording or axillary web syndrome after breast cancer surgery. Can. J. Surg. 2009, 52, E105–E106. [Google Scholar]
- Crane, P.; Ladden, J.; Monica, D. Treatment of axillary web syndrome using instrument assisted soft tissue mobilization and thoracic manipulation for associated thoracic rotation dysfunction. Physiother. Theory Pract. 2017, 34, 74–78. [Google Scholar] [CrossRef]
- Jacob, T.; Bracha, J. Identification of Signs and Symptoms of Axillary Web Syndrome and Breast Seroma During a Course of Physical Therapy 7 Months After Lumpectomy: A Case Report. Phys. Ther. 2019, 99, 229–239. [Google Scholar] [CrossRef]
- Tay, M.R.J.; Wong, C.J.; Aw, H.Z. Prevalence and associations of axillary web syndrome in Asian women after breast cancer surgery undergoing a community-based cancer rehabilitation program. BMC Cancer 2021, 21, 1–7. [Google Scholar] [CrossRef]
- da Luz, C.M.; Deitos, J.; Siqueira, T.C.; Palú, M.; Heck, A.P.F. Management of Axillary Web Syndrome after Breast Cancer: Evidence-Based Practice. Ginecol. Obstet. 2017, 39, 632–639. [Google Scholar] [CrossRef]
- The diagnosis and treatment of peripheral lymphedema: 2020 Consensus Document of the International Society of Lymphology. Lymphology 2020, 53, 3–19.
- Viscuse, P.; Price, K.; Millstine, D.; Bhagra, A.; Bauer, B.; Ruddy, K.J. Integrative medicine in cancer survivors. Curr. Opin. Oncol. 2017, 29, 235–242. [Google Scholar] [CrossRef]
- Bergmann, A.; da Costa Leite Ferreira, M.G.; De Aguiar, S.S.; De Almeida Dias, R.; de Souza Abrahao, K.D.; Paltrinieri, E.M.; Martinez Allende, R.G.; Carvalho de Andrade, M.F. Physiotherapy in upper limb lymphedema after breast cancer treatment: A randomized study. Lymphology 2014, 47, 82–91. [Google Scholar] [PubMed]
- Ha, K.-J.; Lee, S.-Y.; Lee, H.; Choi, S.-J. Synergistic Effects of Proprioceptive Neuromuscular Facilitation and Manual Lymphatic Drainage in Patients with Mastectomy-Related Lymphedema. Front. Physiol. 2017, 8, 959. [Google Scholar] [CrossRef] [PubMed]
- Domenici, L.; Caputo, G.G.; Losco, L.; Di Taranto, G.; Lo Torto, F.; Pierazzi, D.M.; Governa, M.; Benedetti Panici, P.; Ribuffo, D.; Cigna, E. Muscle-Sparing Skin-Reducing Breast Reconstruction with Pre-Pectoral Implants in Breast Cancer Patients: Long-Term Assessment of Patients’ Satisfaction and Quality of Life. J Invest Surg. 2022, 35, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.; Gaitatzis, K.; De Jonge, X.J.; Blackwell, R.; Koelmeyer, L.A. Manual lymphatic drainage treatment for lymphedema: A systematic review of the literature. J. Cancer Surviv. 2021, 15, 244–258. [Google Scholar] [CrossRef]
- Boivin, M.J.; Sikorskii, A.; Haan, P.; Smith, S.S.; Symonds, L.L.; Khattree, R.; Giordani, B.; Blow, A.J.; Osuch, J.R. Health-Related Quality of Life: Longitudinal Analysis From the Time of Breast Biopsy Into the Post-treatment Period. Front. Glob. Womens Health 2021, 2, 608787. [Google Scholar] [CrossRef]
- Chan, R.J.; Nekhlyudov, L.; Duijts, S.F.; Hudson, S.V.; Jones, J.M.; Keogh, J.; Love, B.; Lustberg, M.B.; Mehnert-Theuerkauf, A.; Nathan, P.; et al. Future research in cancer survivorship. J. Cancer Surviv. 2021, 15, 659–667. [Google Scholar] [CrossRef]
- Cheng, K.K.F.; Lim, Y.T.E.; Koh, Z.M.; Tam, W.W.S. Home-based multidimensional survivorship programmes for breast cancer survivors. Cochrane Database Syst. Rev. 2017, 2017, CD011152. [Google Scholar] [CrossRef]
- Galiano-Castillo, N.; Ariza-García, A.; Cantarero-Villanueva, I.; Fernández-Lao, C.; Sánchez-Salado, C.; Arroyo-Morales, M. Agreement between telerehabilitation involving caregivers and face-to-face clinical assessment of lymphedema in breast cancer survivors. Support. Care Cancer 2014, 22, 253–258. [Google Scholar] [CrossRef]
- Invernizzi, M.; de Sire, A.; Venetis, K.; Cigna, E.; Carda, S.; Borg, M.; Cisari, C.; Fusco, N. Quality of Life Interventions in Breast Cancer Survivors: State of the Art in Targeted Rehabilitation Strategies. Anti-Cancer Agents Med. Chem. 2022, 22, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Scarnecchia, E.; Liparulo, V.; Pica, A.; Guarro, G.; Alfano, C.; Puma, F. Multidisciplinary approach to chest wall resection and reconstruction for chest wall tumors, a single center experience. J. Thorac. Dis. 2017, 9, 5093–5100. [Google Scholar] [CrossRef] [PubMed]
- Losco, L.; Cigna, E. Aesthetic Refinements in C-V Flap: Raising a Perfect Cylinder. Aesthet Surg J. 2018, 38, NP26–NP28. [Google Scholar] [CrossRef]
- Chiummariello, S.; Angelisanti, M.; Arleo, S.; Alfano, C. Evaluation of the sensitivity after reduction mammoplasty. Our experience and review of the literature. Ann. Ital. Chir. 2013, 84, 385–388. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| PubMed: ((axillary web syndrome) OR (AWS) OR (cords) OR (cording) OR (webbing) OR (lymphatic cord) OR (axillary web cord) OR (vascular string) OR (lymphatic thrombosis) OR (lymphatic cording) OR (lymphatic cord) OR (axillary string) OR (axillary web) OR (vascular string) OR (mondor disease) OR (axillary web cord) OR (axilla band) OR (axilla cord) OR (fibrous banding) OR (fibrotic bands) OR (string phenomenon) OR (cording lymphoedema) OR (superficial lymphatic thrombosis) OR (vascular ring) OR (fibrous cords) OR (lymph vessel fibrosis) OR (syndrome of the axillary cords)) AND ((breast cancer) OR (breast tumor) OR (breast malignancy) OR (breast neoplasm)) AND ((treatment) OR (therapy) OR (physiotherapy) OR (rehabilitation) OR (exercise) OR (exercises) OR (therapeutic exercise) OR (physical exercise) OR (management)) |
| Scopus: TITLE-ABS-KEY ((((AWS) OR (axillary AND web AND syndrome) OR (lymphatic AND cord) OR (axillary AND web AND cord) OR (vascular AND string) OR (lymphatic AND coding) OR (axillary AND string) OR (axillary AND web) OR (vascular AND string) OR (axilla AND band) OR (axilla AND cord) OR (fibrous AND banding) OR (fibrotic AND band) OR (string AND phenomenon) OR (coding AND lymphoedema) OR (vascular AND ring) OR (fibrous AND cords) OR (lymph AND vessel AND fibrosis) OR (syndrome AND of AND the AND axillary AND cords)) AND ((breast AND cancer) OR (breast AND tumor) OR (breast AND malignancy) OR (breast AND neoplasm)) AND (treatment OR exercise OR (physical AND exercise) OR physiotherapy OR rehabilitation OR management OR (therapeutic AND exercise)))) |
| Cochrane Central Register of Controlled Trials (CENTRAL): ((axillary web syndrome) OR (AWS) OR (cords) OR (cording) OR (webbing) OR (lymphatic cord) OR (axillary web cord) OR (vascular string) OR (lymphatic thrombosis) OR (lymphatic cording) OR (lymphatic cord) OR (axillary string) OR (axillary web) OR (vascular string) OR (mondor disease) OR (axillary web cord) OR (axilla band) OR (axilla cord) OR (fibrous banding) OR (fibrotic bands) OR (string phenomenon) OR (cording lymphoedema) OR (superficial lymphatic thrombosis) OR (vascular ring) OR (fibrous cords) OR (lymph vessel fibrosis) OR (syndrome of the axillary cords)):ti,ab,kw AND ((breast cancer) OR (breast tumor) OR (breast malignancy) OR (breast neoplasm)):ti,ab,kw AND ((treatment) OR (therapy) OR (physiotherapy) OR (rehabilitation) OR (exercise) OR (exercises) OR (therapeutic exercise) OR (physical exercise) OR (management)):ti,ab,kw |
| Physiotherapy Evidence Database (PEDro): axillary web syndrome*treatment |
| Web of Science: TS = (AWS OR (axillary web syndrome) OR (lymphatic cord) OR (axillary web cord) OR (vascular string) OR (lymphatic coding) OR (axillary string) OR (axillary web) OR (vascular string) OR (axilla band) OR (axilla cord) OR (fibrous banding) OR (fibrotic band) OR (string phenomenon) OR (coding lymphoedema) OR (fibrous cords) OR (lymph vessel fibrosis) ) AND (breast cancer OR breast tumor) AND (treatment OR exercise OR (physical exercise) OR physiotherapy OR rehabilitation OR management OR (therapeutic exercise)) |
| Author Year Country | Design | Participants | Time from Surgery | Breast Cancer Treatment | Intervention Modality | Frequency, Volume, Intensity, Protocol Duration | Control | Outcomes | Main Findings | |
|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size (Dropouts) | Mean age (years) BMI (kg/m2) | |||||||||
| Cho et al., 2015 [31] South Korea | RCT | 48 (7) PTMLD: n = 21 PT: n = 20 | PTMLD: 46.6 ± 6.8 PT: 50.7 ± 9.6 PTMLD: ≥25: n = 6; <25: n = 15 PT: ≥25: n = 9; <25: n = 11 | At least 4 weeks | PTMLD: mastectomy (n = 12), lumpectomy (n = 7), breast reconstruction (n = 2). Chemotherapy (n = 9), radiotherapy (n = 21), hormone therapy (n = 14). PT: mastectomy (n = 16), lumpectomy (n = 3), breast reconstruction (n = 1). Chemotherapy (n = 11), radiotherapy (n = 19), hormone therapy (n = 12). | PTMLD: PT consisting of 10 min warm-up (stretching); shoulder flexor, shoulder abductor, and elbow flexor strengthening exercises; 30 min of manual therapy: soft tissue mobilization techniques and stretching for tight tissue cords, shoulder abduction, elbow extension, and wrist supination and extension stretching exercises, shoulder girdle mobilization; and PROM exercises; 10 min cooldown (stretching) + MLD Vodder method 30 min for session. Supervised. | PTMLD: PT 3 times/week (50 min per session) for 4 weeks + MLD 5 times/week (30 min per session) for 4 weeks. PT: PT 3 times/week (50 min per session) for 4 weeks. PT intensity: 60–80% 1RM. MLD intensity: from comfortable to mild discomfort. | PT consisting of 10 min warm-up (stretching); shoulder flexor, shoulder abductor, and elbow flexor strengthening exercises; 30 min of manual therapy: soft tissue mobilization techniques and stretching for tight tissue cords, shoulder abduction, elbow extension, and wrist supination and extension stretching exercises, shoulder girdle mobilization; and PROM exercises; 10 min cooldown (stretching). | Arm volume: circumference measurements; muscular strength: hand-held dynamometer; AROM: digital inclinometer; DASH; EORTC QLQ-C30; EORTC QLQ-BR23; NRS. | This study reports about 48 post-surgical BC AWS patients (mean age PTMLD: 46.6 ± 6.8, PT: 50.7 ± 9.6). They were treated 4 weeks after surgery. The main finding is represented by the improvement observed in QOL (both EORTC QLQ-C30; EORTC QLQ-BR23) including functional and symptom aspects, shoulder flexor strength, and AROM, DASH, and NRS scores that were significantly improved in both groups after the 4-week intervention (p < 0.05). NRS score and arm volume were significantly lower in the PTMLD group than in the PT group (p < 0.05). No lymphedema was observed in the PTMLD group but was observed in the PT group (p < 0.05). Visible cords percentage was not significantly different between the two groups (28.5% PTMLD, 35% PT, p = 0.658). |
| Ibrahim et al., 2018 [32] Egypt | RCT | 60 (NA) Group A: n = 20 Group B: n = 20 Group C: n = 20 | 40–50 NA | 3 months | ALND | Group A: direct myofascial release (in shoulder abduction) and Kinesio tape (in shoulder abduction). Supervised. | All groups: 2 sessions/week for 4 weeks Volume: NR Intensity: NR | Group B: direct myofascial release (in shoulder abduction). Group C: Kinesio tape (in shoulder abduction). | VAS, ultrasound for assessment of AWS cord thickness and disorganization. | This study reports about 60 post-surgical BC AWS patients (aged between 40 and 50 years). They were treated 3 months after surgery. The main finding is represented by the improvement observed in VAS (each group had a significant decrease post-treatment, p = 0.0001, but there was no significant difference between the three groups, p = 0.31); in decrease thickness of the cords (each group had a significant decrease post-treatment, p < 0.05, but there was no significant difference between the three groups, p = 0.39); and in cord disorganization (each group had a significant improvement post-treatment, p < 0.05, and there was a significant difference between groups A and B, p = 0.03, and A and C, p = 0.009, while there was no significant difference between B and C, p = 0.08). |
| Moreau et al., 2010 [33] Belgium | Non-RCT | 28 (NA) Group 1: n = NA Group 2: n = NA | NA NA | NA | BC surgery with axillary clearing in 82.14% of cases (n = 23), and only sentinel node removal in 17.85% of cases (n = 5). | Group 1: MLD (Leduc method) + light adherence stretch (according to ROM, with no pain). Group 2: soft tissue work + adherence stretch (petrissage method, pain could be elicited) + upper extremity mobilization. Supervised. | All groups: at least 13 sessions. Frequency: NR Volume: NR Intensity: NR | NR | Adherence evaluation, upper extremities ROM, VAS. | This study reports about 28 post-surgical BC AWS patients (mean age not specified). The main finding is represented by the improvement observed in adherences, upper extremities ROM, and VAS, which resulted in being significant after 13 sessions of treatment (p < 0.05), while no significant difference was present between groups. |
| Wyrick et al., 2006 [34] United States | Retrospective observational study | 31 (6) | NA NA | From 14 days to 5.8 years; 17% of patients > 1 year. | Lumpectomy (n = 7), double lumpectomy (n = 1), lumpectomy followed by mastectomy (n = 4), mastectomy (n = 8), mastectomy followed by later breast reconstruction (n = 4), mastectomy followed by immediate breast reconstruction (n = 6). One patient was seen twice but had only one surgical procedure. Concomitant cancer therapy (chemotherapy or radiation, n = 12). | Home exercises program with active mobilization; therapeutic exercise, including soft tissue stretching, progressive resistance exercises, Airdyne Bicycle training; if patients had lymphedema or persistent swelling, manual therapy, compression bandages, and intermitting pneumatic compression were also used. Supervision not specified. | Average duration of treatment: 10.1 ± 9.5 weeks. Frequency: NR Volume: NR Intensity: NR | NR | Cording severity (mild, mild to moderate, moderate, moderate to severe, severe), ROM, length of care. | This study reports about 31 post-surgical BC AWS patients (mean age not specified). They were treated from 14 days to 5.8 years after surgery. The main finding is represented by the resolution in lymphatic cording, which was faster with physical therapy. Shoulder ROM improved after 4 weeks of treatment (abduction improved by 52 ± 21° and flexion improved by 39 ± 20°). The difference in treatment duration between regular and irregular patients was statistically significant (p = 0.012): duration of treatment for regular patients (n = 18) was 7.3 ± 3.4 weeks (less than 2 months); duration of treatment for irregular patients (n = 7) was 18.0 ± 17.1 weeks; mean treatment duration for patients with concomitant cancer therapy leading to cancellations (n = 12) was 17.0 ± 14.8 weeks. |
| Lattanzi et al., 2012 [35] United States | Case report | 1 | 44 NA | 10 days. | Lumpectomy and sentinel node dissection. Thirty-five sessions of radiotherapy. | First week: soft tissue mobilization of cords, skin traction techniques, and myofascial release techniques. Second week: + two-person cord traction technique, self-elongation techniques, and skin traction and scar massage. Home stretching program. Supervised. | Physical/occupational therapy 3 times/week for 2 weeks followed by pause during 35 radiotherapy treatments. Then, 2 times/week for 1 week, and then 1 time/week for 2 weeks (total of 5 weeks of protocol duration). Volume: NR Intensity: NR. | NR | ROM, cords evaluation, muscle strength and function, DASH. | This case report presents 1 post-surgical BC AWS patient (44 years old). She was treated 10 days after surgery. The main finding is represented by the improvement in ROM, cords, muscle strength and function, and DASH score (32.5 vs. 7.5). |
| Fourie et al., 2009 [36] South Africa, United Kingdom | Case report | 1 | 47 NA | 22 days. | Left modified radical mastectomy with removal of six axillary lymph nodes. | Manual soft tissue techniques. Home program of gentle stretching and self-mobilization. Supervised. | First week: 2 sessions; Days 8–10: 1 session a day; Up to 26 days: 6 sessions. Total of 11 sessions. 30–45 min each session. Intensity: NR. | NR | AROM, PROM, tissue movement and glide. | This case report presents 1 post-surgical BC AWS patient (47 years old). She was treated 22 days after surgery. The main finding is represented by the improvement in AROM, PROM, tissue movement and glide, until full range of movement with no visible or palpable cording. |
| Wei et al., 2013 [37] China | Case report | 1 | 39 NA | 3 days. | Breast-conserving surgery and axillary lymph node biopsy; 17 days later secondary breast-conserving surgery. | Home program: shoulder exercises and massage to the cord-like structure. Non-supervised. | Plant-based medicament (Aesculus hippocastanum) 300 mg twice a day. Physical program every day in the morning and at bedtime for 30 min, for 3 weeks. Intensity: NR | NR | ROM, VAS, cords evaluation both manual and ultrasound. | This case report presents 1 post-surgical BC AWS patient (39 years old). She was treated 3 days after surgery. The main finding is represented by the improvement after 3 weeks in ROM (90° vs. 170°), VAS (7 vs. 0), cords that became invisible and non-palpable (both manually and by ultrasound). Numbness and tightness were still present but diminished. The plant-based medication Aesculus hippocastanum could have played a role. |
| Tilley et al., 2009 [38] Canada | Case report | 1 | 37 NA | 1 week. | Lumpectomy, sentinel lymph node biopsy, and ALND for a node-positive BC. | Moist heat to the axilla and inner arm for 10 min per session. Shoulder flexion and abduction ROM exercises and gentle stretching. Cord stretching. Home exercises (gentle arm flexion and horizontal abduction). Supervised. | 6 physiotherapy sessions in 3 weeks period. Volume: NR Intensity: NR | NR | ROM, cords evaluation. | This case report presents 1 post-surgical BC AWS patient (37 years old). She was assessed 1 week after surgery. The main finding is represented by the improvement in ROM (135° and 123° vs. 180° and 180°, flexion and abduction, respectively). The cord improved but was still palpable at the end of her treatment sessions, 7 weeks after surgery. |
| de Sire et al., 2020 [13] Italy | Case report | 1 | 66 22 | 1 month. | Left inner upper quadrantectomy with negative sentinel node biopsy. | Manual therapy: myofascial release techniques with soft-tissue mobilization, massage and manipulation of the tight cord and scar tissues, therapeutic shoulder exercises including stretching, and MLD. Supervised. | Fondaparinux 2.5 mg/day for 3 weeks. Rehabilitation program 3 times/week for 3 weeks, 45 min per session. Intensity: NR | NR | ROM, NPRS, Quick DASH, EQ-5D-3L index, EQ-VAS. | This case report presents 1 post-surgical BC AWS + Mondor’s disease patient (66 years old). She was treated 1 month after surgery. The main finding is represented by the improvement after 3 weeks treatment in shoulder ROM (80° and 100° vs. 170° and 170°, flexion and abduction, respectively), NPRS (5 vs. 0), Quick DASH (40 vs. 0), EQ-5D-3L index (0.662 vs. 1.000), EQ-VAS (75 vs. 90). |
| Crane et al., 2017 [39] United States | Case report | 1 | 48 NA | 1 year. | Bilateral mastectomy and negative lymph node dissection. Following surgery, a course of chemotherapy. Three months after completion of chemotherapy, bilateral latissimus dorsi flap reconstruction. | IASTM to the axilla at end range abduction for 5 min, thoracic/thoracolumbar junction manipulation, and flexibility exercise. Home exercise program consisting of shoulder girdle and thoracic stretching. Supervised. | 4 times/week for 4 weeks. Home exercises 3 times/day each day. Volume: NR Intensity: NR | NR | ROM, NPRS, PSFS, thoracic rotation. | This case report presents 1 post-surgical BC AWS patient (48 years old). She was treated 1 year after surgery. The main finding is represented by the improvement in shoulder ROM (140° and 150° vs. 178° and 174°, flexion and abduction, respectively), bilateral thoracic rotation (25% vs. 100%), NPRS (5 vs. 1), and PSFS (19/30 vs. 30/30). |
| Jacob et al., 2019 [40] Israel | Case report | 1 | 65 23.4 | 7 months | Left breast lumpectomy + ALND + intraoperative radiation therapy and whole breast radiation. | MLD, scar tissue techniques, cord stretching, self-massage, supportive bras. Home program: self-lymph-massage, compression garments, stretching exercise, Tidhar method of aqua lymphatic therapy, physical activity program. Supervised. | 1 time/week for 6 weeks, 60 min per session. Intensity: NR | NR | ROM, VAS during shoulder ROM, cording evaluation. | This case report presents 1 post-surgical BC AWS patient (65 years old). She was treated 7 months after surgery. The main finding is represented by the improvement in VAS during shoulder ROM (8 vs. 0), which was never limited, and the disappearance of cording at the end of treatment. |
| Author and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 |
|---|---|---|---|---|---|---|---|---|---|
| de Sire et al., 2020 [13] | Y | N/A | N/A | N/A | Y | Y | N/A | Y | N/A |
| Cho et al., 2015 [31] | Y | Y | Y | Y | N | N | Y | Y | N |
| Ibrahim et al., 2018 [32] | Y | Y | Y | Y | N | N | Y | Y | N |
| Moreau et al., 2010 [33] | Y | Y | Y | Y | Y | Y | Y | Y | N |
| Wyrick et al., 2006 [34] | Y | N/A | N/A | N | N | N | Y | Y | Y |
| Lattanzi et al., 2012 [35] | Y | N/A | N/A | N/A | Y | Y | N/A | Y | N/A |
| Fourie et al., 2009 [36] | Y | N/A | N/A | N/A | Y | N | N/A | Y | N/A |
| Wei et al., 2013 [37] | Y | N/A | N/A | N/A | N | N | N/A | Y | N/A |
| Tilley et al., 2009 [38] | Y | N/A | N/A | N/A | Y | N | N/A | Y | N/A |
| Crane et al., 2017 [39] | Y | N/A | N/A | N/A | N | Y | N/A | Y | N/A |
| Jacob et al., 2019 [40] | Y | N/A | N/A | N/A | Y | N | N/A | Y | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lippi, L.; de Sire, A.; Losco, L.; Mezian, K.; Folli, A.; Ivanova, M.; Zattoni, L.; Moalli, S.; Ammendolia, A.; Alfano, C.; et al. Axillary Web Syndrome in Breast Cancer Women: What Is the Optimal Rehabilitation Strategy after Surgery? A Systematic Review. J. Clin. Med. 2022, 11, 3839. https://doi.org/10.3390/jcm11133839
Lippi L, de Sire A, Losco L, Mezian K, Folli A, Ivanova M, Zattoni L, Moalli S, Ammendolia A, Alfano C, et al. Axillary Web Syndrome in Breast Cancer Women: What Is the Optimal Rehabilitation Strategy after Surgery? A Systematic Review. Journal of Clinical Medicine. 2022; 11(13):3839. https://doi.org/10.3390/jcm11133839
Chicago/Turabian StyleLippi, Lorenzo, Alessandro de Sire, Luigi Losco, Kamal Mezian, Arianna Folli, Mariia Ivanova, Lorenzo Zattoni, Stefano Moalli, Antonio Ammendolia, Carmine Alfano, and et al. 2022. "Axillary Web Syndrome in Breast Cancer Women: What Is the Optimal Rehabilitation Strategy after Surgery? A Systematic Review" Journal of Clinical Medicine 11, no. 13: 3839. https://doi.org/10.3390/jcm11133839
APA StyleLippi, L., de Sire, A., Losco, L., Mezian, K., Folli, A., Ivanova, M., Zattoni, L., Moalli, S., Ammendolia, A., Alfano, C., Fusco, N., & Invernizzi, M. (2022). Axillary Web Syndrome in Breast Cancer Women: What Is the Optimal Rehabilitation Strategy after Surgery? A Systematic Review. Journal of Clinical Medicine, 11(13), 3839. https://doi.org/10.3390/jcm11133839